ORIGINAL CONTRIBUTION
Perioperative N-acetylcysteine to Prevent
Renal Dysfunction in High-Risk Patients
Undergoing CABG Surgery
A Randomized Controlled Trial
Karen E. A. Burns, MD, MSc, FRCPC
Michael W. A. Chu, MD, MEd
Richard J. Novick, MD, MSc, FRCSC
Stephanie A. Fox, BA, RRT
Kerri Gallo, RN
Claudio M. Martin, MD, MSc, FRCPC
Larry W. Stitt, MSc
A. Paul Heidenheim, MA
M. Lee Myers, MD, FRCSC
Louise Moist, MD, MSc, FRCPC
C
ORONARY ARTERY BYPASS
graft (CABG) surgery is being
performed on a broader range
of surgical candidates at increased surgical risk.1,2 Patients with advanced age, more diffuse coronary artery disease, and an increased number
of comorbidities are frequently referred for CABG surgery.3 These patients are at higher risk for fatal and
nonfatal postoperative complications
following CABG surgery, especially
with cardiopulmonary bypass (CPB) exposure.4-6 Renal dysfunction is an important postoperative complication,
with associated increased morbidity and
mortality.
The incidence of acute renal failure
requiring renal replacement therapy
(RRT) following CPB is estimated to occur in up to 3.7% of patients, while azotemia, not necessitating RRT, occurs in
approximately 11.4% of operative candidates.7 Prolonged intensive care unit
(ICU) and hospital stay, increased 30day mortality, hospital mortality, and
Context Renal dysfunction is a complication of coronary artery bypass graft (CABG)
surgery performed with cardiopulmonary bypass (CPB) that is associated with increased morbidity and mortality. N-acetylcysteine, an antioxidant and vasodilator, counteracts renal ischemia and hypoxia.
Objective To determine whether perioperative intravenous (IV) N-acetylcysteine preserves renal function in high-risk patients undergoing CABG surgery with CPB compared with placebo.
Design, Setting, and Patients Randomized, quadruple blind, placebo-controlled
trial (October 2003-September 2004) in operating rooms and general intensive care
units (ICUs) of 2 Ontario tertiary care centers. The 295 patients required elective or
urgent CABG and had at least 1 of the following: preexisting renal dysfunction, at least
70 years old, diabetes mellitus, impaired left ventricular function, or undergoing concomitant valve or redo surgery.
Interventions Patients received 4 (2 intraoperative and 2 postoperative) doses of
IV N-acetylcysteine (600 mg) (n=148) or placebo (n=147) over 24 hours.
Main Outcome Measures The primary outcome was the proportion of patients
developing postoperative renal dysfunction, defined by an increase in serum creatinine level greater than 0.5 mg/dL (44 µmol/L) or a 25% increase from baseline within
the first 5 postoperative days. Secondary outcomes included postoperative interventions and complications, the requirement for renal replacement therapy (RRT), adverse events, hospital mortality, and ICU and hospital length of stay.
Results There was no difference in the proportion of patients with postoperative renal dysfunction (29.7% vs 29.0%, P =.89; relative risk [RR], 1.03 [95% confidence
interval {CI}, 0.72-1.46]) in the N-acetylcysteine and placebo groups, respectively. We
noted nonsignificant differences in postoperative interventions and complications, the
need for RRT (0.7% vs 2.1%; P =.37), total (6.1% vs 9.6%; P=.26) and serious adverse events, hospital mortality (3.4% vs 2.7%; P⬎.99), and ICU and hospital length
of stay between the N-acetylcysteine and placebo groups. A post hoc subgroup analysis of patients (baseline creatinine level ⬎1.4 mg/dL [120 µmol/L]) showed a nonsignificant trend toward fewer patients experiencing postoperative renal dysfunction in
the N-acetylcysteine group compared with the placebo group (25.0% vs 37.1%; P=.29).
Conclusions N-acetylcysteine did not prevent postoperative renal dysfunction, interventions, complications, or mortality in high-risk patients undergoing CABG surgery with CPB. Further research is required to identify CABG patients at risk for postoperative renal events, valid markers of renal dysfunction, and to establish renal thresholds
associated with important clinical outcomes.
www.jama.com
JAMA. 2005;294:342-350
Author Affiliations are listed at the end of this article.
Corresponding Author: Karen Burns, MD, MSc, FRCPC, Interdepartmental Division of Critical Care,
342 JAMA, July 20, 2005—Vol 294, No. 3 (Reprinted)
University of Toronto, St Michael’s Hospital, 30 Bond
St, c/o 4-012 Bond Wing, Toronto, Ontario, Canada
M5B 1W8 (burnske2@yahoo.ca).
©2005 American Medical Association. All rights reserved.
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
tioxidant. Several meta-analyses20-24 and
randomized controlled trials (RCTs)
have demonstrated that N-acetylcysteine attenuates contrast-associated declines in renal function. The total dose
of N-acetylcysteine received was variable in the RCTs with N-acetylcysteine
first administered approximately 24
hours orally and over 30 minutes intravenously immediately before contrast
exposure in some beneficial studies .25,26
While inexpensive and infrequently associated with toxicity, N-acetylcysteine is a medication with which many clinicians have considerable clinical
experience. If N-acetylcysteine was demonstrated to be beneficial in reducing
morbidity in CABG patients exposed to
CPB, it may represent a cost-saving preventive strategy.
Because CPB in CABG patients is associated with renal dysfunction, we
conducted an RCT to test the hypothesis that perioperative administration
of intravenous N-acetylcysteine would
preserve renal function in high-risk patients undergoing on-pump CABG surgery compared with placebo.
Box. Inclusion and Exclusion Criteria
Inclusion Criteria
All adult patients admitted for elective or urgent coronary artery bypass graft (CABG)
surgery necessitating exposure to cardiopulmonary bypass and deemed high risk
for postoperative renal dysfunction
High-risk patients were defined by the presence of 1 or more of the following
criteria at the time of preoperative assessment:
Preexisting renal impairment (baseline serum creatinine level ⬎1.4 mg/dL [120
µmol/L])
Ejection fraction ⬍35% or grade 3 or 4 left ventricular function
Age ⱖ70 years
Diabetes mellitus treated with insulin or oral hypoglycemic agents
Concomitant valve or redo surgery
Exclusion Criteria
Emergent CABG, cardiac transplantation, or insertion of left ventricular assist
device
Known allergy or hypersensitivity to N-acetylcysteine
Acute renal failure (⬎1.1 mg/dL [100 µmol/L] increase in serum creatinine level
from preadmission to operation)
Enrolled in conflicting research study
Prior renal transplantation
Serum creatinine level ⬎4.5 mg/dL (400 µmol/L)
N-acetylcysteine within 5 days of planned operation
Planned off-pump CABG surgery
METHODS
discharges to extended-care facilities
have been attributed to renal dysfunction following CPB exposure.8-11 While
some authors have demonstrated a high
incidence of acute renal failure following CPB exposure in the absence of significant perioperative cardiac failure or
renal insults,12 others have suggested
that advanced age,7,8,11,13 preexisting renal dysfunction,8,11,14 and conditions
that compromise renal blood flow (including diabetes,8,13 poor left ventricular function,13,14 valve procedures,13,14
or repeat revascularization8,13,14) place
patients at increased risk for postoperative renal dysfunction. Age, diabetes, and impaired left ventricular function are more frequently associated with
prolonged ICU stay, although the use
of off-pump coronary artery bypass
(OPCAB) or minimally invasive direct
coronary artery bypass (MIDCAB) surgery may be more appropriate in this
regard.15
The renal dysfunction that occurs after cardiac surgery is multifactorial. Potential causes of renal dysfunction include cardiovascular compromise,
prolonged CPB exposure, increased catecholamine level, nonpulsatile flow, hypothermia, renal hypoperfusion, and the
induction of inflammatory mediators.
These factors may collectively contribute to renal hypoxia and ischemia. Hypoxic-ischemic insults result in direct
toxic effects within renal tubular epithelial cells with depletion of local antioxidants and the formation of reactive oxygen species. In addition, hypoxia
induces perturbations in renal hemodynamics resulting in enhanced sensitivity to vasoconstrictive stimuli and
attenuated responsiveness to nitric
oxide–dependent vasodilation. 16-19
N-acetylcysteine has been shown to attenuate ischemic renal failure through
nitric oxide–independent arteriolar vasodilation while functioning as an an-
©2005 American Medical Association. All rights reserved.
Patients
Between October 2003 and September
2004, we enrolled high-risk patients
(BOX) scheduled for elective or urgent
CABG surgery at 2 sites of the London
Health Sciences Centre in a quadrupleblind (patients, clinicians, data collectors, and the data analyst), placebocontrolled RCT. We identified elective
and urgent patients at the time of surgical consultation in preadmission clinics and hospital wards, respectively. The
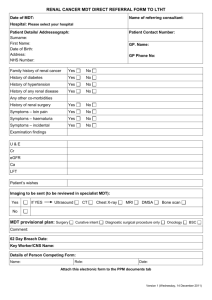
flow of patients through the study and
reasons for exclusion are detailed in the
FIGURE. This study was approved by the
Research Ethics Board at the University of Western Ontario. Approval to use
N-acetylcysteine for this indication and
in the CABG population was obtained
from the Therapeutics Product Directorate of Health Canada. We obtained
written informed consent for study participation from all patients or their legal representatives.
(Reprinted) JAMA, July 20, 2005—Vol 294, No. 3
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
343
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
operative complications (myocardial infarction, stroke, mediastinitis, and
bloodstream infections). We recorded
the requirement for RRT during hospitalization, hospital mortality, and ICU
and hospital length of stay. In addition,
we collected information on total and serious drug-related adverse events and
their impact on study medication discontinuation. A data and safety monitoring committee comprising an independent nephrologist, cardiologist, and
intensivist conducted a blinded interim analysis at 50% of targeted enrollment for safety and efficacy end points.
Figure. Patient Flow Through the Study
471 Patients Assessed for Eligibility
176 Excluded
41 Patients Refused Participation
8 Clinicians Refused Participation
82 Met Exclusion Criteria
37 Patients Missed
8 No Consent
295 Randomized
148 Assigned to Receive N-acetylcysteine
147 Received N-acetylcysteine as Assigned
1 Did Not Receive N-acetylcysteine
(Patient Missed)
147 Assigned to Receive Placebo
144 Received Placebo as Assigned
3 Did Not Receive Placebo
1 Preoperative Death
2 Patients Missed
Operative Management
0 Lost to Follow-up
0 Immediate Postoperative Death
4 Underwent Off-Pump Surgery
1 Did Not Receive N-acetylcysteine∗
3 Received N-acetylcysteine
1 Underwent Valve Only Surgery On-Pump
0
1
0
1
148 Included in Primary Analyses
148 Had Postoperative Creatinine Level
143 Included in Per-Protocol Analyses
143 Had Postoperative Creatinine Level
Lost to Follow-up
Immediate Postoperative Death
Underwent Off-Pump Surgery
Underwent Valve Only Surgery On-Pump
147 Included in Primary Analyses
145 Had Postoperative Creatinine Level
143 Included in Per-Protocol Analyses
142 Had Postoperative Creatinine Level
*One patient who did not receive N-acetylcysteine also underwent off-pump surgery. See Footnote to Table 3.
Interventions
At each site, patients underwent delayed randomization on the morning of
the scheduled surgery to receive either
4 doses of intravenous N-acetylcysteine (n=148) or placebo (n = 147) over
a 24-hour period. Randomization was
performed by a pharmacy trials coordinator using a permuted block strategy with alternating blocks of 4 and 6.
Allocation was concealed using central randomization with drugs prepared by the pharmacy. Patients, health
care clinicians, and individuals participating in the data collection and data
analysis were blinded to treatment
assignment.
Four premixed, prepackaged bags
containing either liquid N-acetylcysteine or a color- and consistencymatched placebo were prepared and
dispensed by a site pharmacist. Each
of the 4 bags contained either
N-acetylcysteine (600 mg) or placebo
(5% dextrose in water). The first 2 doses
of N-acetylcysteine or placebo were administered in the operating room im-
mediately following induction of anesthesia and on successful weaning
from CPB. The third and fourth doses
were administered in the ICU, 12 and
24 hours after administration of the first
dose. Patients requiring reoperation
within the first 24 hours remained in
the same group to which they were
originally randomized and received the
2 postoperative doses at 12 and 24
hours after the initial dose.
Outcome Measures
The primary end point was the proportion of patients developing postoperative renal dysfunction defined as an absolute increase in serum creatinine level
of greater than 0.5 mg/dL (44 µmol/L)
or a 25% increase from baseline at any
time within the first 5 postoperative days.
Secondary end points included the requirement for postoperative interventions (vasoactive medications, intraaortic balloon pump insertion, renal dose
dopamine, mechanical ventilation for at
least 48 hours, or reintubation and reoperation within 24 hours) and post-
344 JAMA, July 20, 2005—Vol 294, No. 3 (Reprinted)
All patients underwent general anesthesia with a single lumen endotracheal
tube. Patients were monitored using a
central venous catheter, Swan-Ganz
catheter, radial arterial line, Foley catheter, electrocardiography, transesophageal echocardiography, and nasopharangeal and rectal temperature probes.
A median sternotomy incision was performed in all patients. Patients received heparin with an initial dose of 300
to 400 U per kg of body weight, and
maintenance doses were administered to
maintain the activated clotting time of
more than 480 seconds. The ascending
aorta and right atrium were cannulated
in all patients. The CPB circuit consisted of a roller pump (Jostra HL-20,
Jostra AG Maquet Cardiopulmonary,
Hirrlingen, Germany), a nonheparincoated polyvinylchloride circuit
(Terumo Cardiovascular Systems Inc,
Ashland, Maine), a membrane oxygenator (Capiox SX 18, Terumo Cardiovascular Systems Inc, Elkton, Md), a micron arterial filter (Medtronic 38,
Medtronic, Minneapolis, Minn), and an
open venous reservoir system. The
pump prime solution (1 L lactated Ringer’s solution, 500 mL pentastarch, and
1 ampule sodium bicarbonate) and antifibrinolytic agents were administered
according to site-specific protocols and
surgeon preference, respectively. A lowvolume prime, miniaturized, centrifugal pump circuit (Medtronic Resting
Heart Bypass Circuit, Medtronic) was
used in 3 patients. Flow rates were ti-
©2005 American Medical Association. All rights reserved.
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
trated to maintain perfusion pressures
between 60 and 80 mm Hg and a cardiac index of at least 2.4 L/min/m2. Intermittent boluses or infusions of phenylepherine, norepinephrine, and
vasopressin were administered to treat
low intraoperative perfusion pressures
at the discretion of the surgical team. The
most common myocardial protection
strategy used was an antegrade, intermittent, cold blood cardioplegia technique using a cardioplegia delivery system (Medtronic MYOtherm XP,
Medtronic). After successfully weaning from CPB, protamine sulfate and vasoactive medications were administered to reverse systemic heparinization
and optimize systemic perfusion pressures and cardiac output, respectively.
Patients were transferred to the ICU, intubated, and sedated.
Study Definitions
A myocardial infarction was defined by
a new 40-ms Q wave in at least 2 contiguous leads on an electrocardiogram, the development of a new dominant R wave in lead V1, or a new left
bundle-branch block or the presence of
a total creatine kinase (CK) level exceeding 1500 U/L (or CK-MB level ⬎5%
of the total) at any time postoperatively. We defined a stroke by the presence of new focal neurological deficit
persisting for at least 24 hours or by a
new defect on a computed tomogram
or magnetic resonance imaging. Mediastinitis was defined by the requirement for reoperation for deep sternal
wound infection, while the presence of
a postoperative fever in association with
2 positive blood cultures defined bloodstream infection. We defined serious
drug-related adverse events to include
bronchospasm, hypotension, and anaphylaxis. Additionally, we documented the occurrence of other adverse events including nausea,
vomiting, stomatitis, cutaneous rash,
urticaria, and facial edema.
Data Collection
We collected baseline data including patient weight and serum creatinine level
(defined as the serum creatinine level
at the time of enrollment in the preoperative clinic [elective cases] or in hospital [urgent cases]). We noted the presence of comorbidities including the
following: (1) congestive heart failure
(CHF) (defined by an episode within
the 30 days of acceptance for surgery); (2) peripheral vascular disease
(history of intermittent claudication, decreased pedal pulses, or previous vascular surgery); (3) cerebrovascular disease (history of a stroke or transient
ischemic attack); (4) myocardial infarction (within 30 days of acceptance
of surgery); (5) diabetes (managed by
diet, oral hypoglycemic agents, or insulin); (6) chronic obstructive lung disease (requiring inhaled corticosteroids or bronchodilators or spirometry
demonstrating obstructive physiology); and (7) hypertension (active treatment for elevated blood pressure). We
documented preoperative use of (1) angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers,
(2) platelet antiaggregation therapies,
and (3) nonsteroidal anti-inflammatory drugs (NSAIDs) and cyclooxygenase 2 (COX-2) inhibitors. In addition,
we collected intraoperative data on the
procedure performed, number of vessels bypassed, conversions to OPCAB,
and the total cross-clamp and CPB time.
Statistical Analyses
We used the 2 test (or alternatively, the
Fisher exact test when the expected
value was <5) for comparing 2 proportions. We compared differences in logtransformed ICU and hospital length of
stay in survivors using the unpaired t
test and compared ICU and hospital
length of stay between groups using
time-to-event analysis with censoring
of deaths and application of the logrank test. Intention-to-treat and perprotocol analyses for all primary and
secondary outcomes were conducted.
In addition, we performed adjusted
analyses for clinically important baseline imbalances (CHF and procedure
performed [CABG vs other]) using logistic regression and proportional hazards regression for dichotomous and
continuous outcomes, respectively. Post
©2005 American Medical Association. All rights reserved.
hoc we conducted a subgroup analysis to assess for treatment effect in patients with a baseline serum creatinine level greater than 1.4 mg/dL (120
µmol /L). Continuous data are expressed as mean (SD) or median (minimum, maximum). We did not impute
missing data. All analyses were conducted using SAS 8.2 (SAS Institute Inc,
Cary, NC). We considered P values
ⱕ.05 to be statistically significant.
We used the formula for 2 independent proportions for dichotomous outcomes to estimate the sample size
required for the primary outcome: attenuation of postoperative increase in serum
creatinine level of greater than 0.5 mg/dL
(44 µmol/L) or a 25% increase from baseline within the first 5 postoperative days.
Anticipating a 50% reduction in the primary outcome25 and assuming a baseline event rate of 30%, with a 2-sided ␣
of .05, 1:1 allocation, and assuming a 10%
loss to follow-up, a total of 296 patients
would result in 80% power to detect a
50% reduction in the proportion of
patients with the primary end point.
RESULTS
Participants
We randomized 295 patients to receive
N-acetylcysteine (n = 148) or placebo
(n=147). At the discretion of the attending surgeon, 4 patients randomized to receive N-acetylcysteine underwent
OPCAB surgery and 2 patients (1 in the
N-acetylcysteine group and 1 in the placebo group) underwent valve surgery
only. One N-acetylcysteine patient who
underwent OPCAB and 3 placebo patients did not receive any study medication. Whereas all participants were included in the intention-to-treat analyses,
only patients undergoing CABG with
CPB and receiving at least 1 dose of study
medication were included in the perprotocol analyses. Two placebo patients, including 1 patient who died preoperatively prior to receiving study
medication, and 1 patient who died postoperatively had no postoperative creatinine measurement. The Figure depicts
patient flow through the study.
We present the baseline characteristics and intraoperative data for the study
(Reprinted) JAMA, July 20, 2005—Vol 294, No. 3
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
345
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
Table 1. Baseline Characteristics
No. (%)
Characteristic
Age, mean (SD), y
N-acetylcysteine Group
(n = 148)
68.9 (8.9)
Placebo Group
(n = 147)
69.2 (9.7)
116.0 (78.4)
87.5 (16.6)
117.0 (79.6)
84.8 (19.0)
1.1 (0.3)
1.2 (0.4)
32 (21.6)
34 (23.0)
36 (24.5)
29 (19.7)
92 (62.2)
66 (44.6)
15 (10.1)
88 (59.9)
63 (42.9)
29 (19.7)
2 (1.4)
10 (6.8)
71 (48.0)
43 (29.1)
29 (19.6)
5 (3.4)
73 (49.7)
44 (29.9)
25 (17.0)
5 (3.4)
112 (75.7)
36 (24.3)
32 (21.6)
24 (16.2)
20 (13.5)
13 (8.8)
106 (72.1)
31 (21.1)
27 (18.4)
26 (17.7)
23 (15.7)
30 (20.4)
84 (56.8)
70 (47.3)
16 (10.8)
80 (54.4)
66 (44.9)
7 (4.8)
Men
Weight, mean (SD), kg
Serum creatinine, mean (SD), mg/dL
Inclusion criteria
Renal dysfunction (creatinine ⬎1.4 mg/dL)
EF ⬍35% or grade 3-4 LV
Age ⱖ70 y
Diabetes
Planned concomitant valve
Redo CABG surgery
Ventricle grade
I
II
III
IV
Comorbidities
Hypertension
Recent myocardial infarction
COPD
Peripheral vascular disease
Cerebrovascular accident
Congestive heart failure
Preoperative medications
Platelet inhibitors
ACE inhibitors or angiotensin blockers
NSAIDs or COX-2 inhibitors
Abbreviations: ACE, angiotensin-converting enzyme; CABG, coronary artery bypass graft; COPD, chronic obstructive
pulmonary disease; COX-2, cyclooxygenase 2; EF, ejection fraction; LV, left ventricle; NSAIDs, nonsteroidal antiinflammatory drugs.
SI conversion: To convert serum creatinine to µmol/L, multiply by 88.4.
Table 2. Intraoperative Data
No. (%)
N-acetylcysteine Group
(n = 148)
Placebo Group
(n = 147)*
Procedure
CABG
CABG ⫹ valve
Other (valve only)
133 (89.9)
14 (9.5)
1 (0.7)
117 (80.1)
28 (19.2)
1 (0.7)
No. of vessels bypassed
0
1
2
3
4
5
6
Pump time, mean (SD), min†
1 (0.7)
11 (7.4)
32 (21.6)
62 (41.9)
39 (26.4)
2 (1.4)
1 (0.7)
90.4 (28.6)
1 (0.7)
16 (11.0)
26 (17.8)
66 (45.2)
29 (19.9)
7 (4.8)
1 (0.7)
101.1 (35.6)
Cross-clamp time, mean (SD), min‡
59.2 (23.9)
65.3 (28.0)
Abbreviation: CABG, coronary artery bypass graft surgery.
*Does not include data from 1 placebo patient who died preoperatively.
†Total pump time in 144 N-acetylcysteine and 146 placebo patients.
‡Aortic cross-clamp time available for 142 N-acetylcysteine and 144 placebo patients.
346 JAMA, July 20, 2005—Vol 294, No. 3 (Reprinted)
participants in TABLE 1 and TABLE 2, respectively. The groups were similar with
regard to age, sex, weight, baseline serum creatinine level, proportion with renal dysfunction at baseline, ventricular
grade, ejection fraction less than 35% or
grade 3 or 4 left ventricular function, at
least 70 years old, and diabetes mellitus. By chance, compared with the Nacetylcysteine group, more patients in the
placebo group had a history of CHF and
underwent concomitant valve surgery.
Correspondingly, we observed increased pump time in the placebo group
compared with the N-acetylcysteine
group. Conversely, more patients in the
N-acetylcysteine group were treated at
the time of initial assessment with
NSAIDs or COX-2 inhibitors. While the
former imbalances would be expected to
bias against placebo, the latter imbalance would be expected to bias against
N-acetylcysteine.
Primary Outcome
We observed nonsignificant differences in the proportion of patients developing postoperative renal dysfunction (44/148 [29.7%] vs 42/145
[29.0%]; relative risk [RR], 1.03 [95%
confidence interval {CI}, 0.72-1.46]);
unadjusted P=.89; adjusted P ⬎.99) in
the N-acetylcysteine and placebo
groups, respectively. Adjusted and perprotocol (43/143 [30.1%] vs 40/142
[28.2%]) analyses confirmed that this
result was robust.
Secondary Outcomes
Postoperative Interventions. We found
nonsignificant differences between Nacetylcysteine and placebo patients with
regard to the requirement for vasoactive medications, intra-aortic balloon
pump insertion, renal dose dopamine,
mechanical ventilation of at least 48
hours, or reintubation and reoperation (TABLE 3).
Postoperative Complications. We
noted nonsignificant differences in the
proportion of patients in the Nacetylcysteine and placebo groups experiencing myocardial infarction,
stroke, mediastinitis, or bloodstream infections (Table 3).
©2005 American Medical Association. All rights reserved.
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
Hospital Outcomes and Length of
Stay. The requirement for RRT during
hospitalization (0.7% vs 2.1%; P=.37)
was infrequent and did not differ significantly between the N-acetylcysteine and
placebo groups, respectively. We found
nonsignificant differences in hospital
mortality (3.4% vs 2.7%; P⬎.99) between patients treated with N-acetylcysteine and placebo, respectively (Table 3).
We noted similar median ICU (2.0 days
[1, 42] vs 2.0 days [2, 53]; P=.57) and
hospital length of stay (7.0 days [5, 64]
vs 8.0 days [5, 372]; P=.31) between Nacetylcysteine and placebo survivors.
Time-to-event analysis confirmed nonsignificant differences in ICU (2.0 days
vs 2.0 days; P=.82) and hospital (7.0 days
vs 8.0 days; P=.52) length of stay in the
N-acetylcysteine and placebo groups, respectively. Per-protocol and adjusted
analyses remained nonsignificant for all
secondary outcomes.
Adverse Events. Nonsignificant differences were also noted between patients treated with N-acetylcysteine and
placebo with respect to the incidence of
total (6.1% vs 9.6%; P=.26) and serious
(0.7% vs 0%; P ⬎.99) adverse events
(TABLE 4). The single serious adverse
event, an episode of intraoperative hypotension treated with epinephrine and
norepinephrine, was possibly related to
N-acetylcysteine but other potential
causes were present and subsequent
doses of N-acetylcysteine were tolerated. No patient discontinued medication as a consequence of an adverse event.
Protocol Compliance. Four Nacetylcysteine (2.7%) and 8 placebo
(5.5%) (P = .23) patients did not receive all 4 doses of medication.
Subgroup Analysis. A post hoc subgroup analysis of patients with a baseline creatinine level greater than 1.4
mg/dL (120 µmol/L) demonstrated a
nonsignificant trend toward fewer patients experiencing postoperative renal dysfunction in the N-acetylcysteine group compared with the placebo
group (25.0% vs 37.1%; P = .29).
COMMENT
We conducted an RCT to investigate
whether perioperative intravenous
N-acetylcysteine or placebo could attenuate postoperative declines in renal
function in high-risk CABG surgery patients exposed to CPB. We found nonsignificant between-group difference in
the proportion of patients experiencing an increase in serum creatinine level
of greater than 0.5 mg/dL (44 µmol/L)
or a 25% increase from baseline within
the first 5 postoperative days. We also
found nonsignificant between-group differences in the requirement for postoperative interventions, postoperative complications, RRT, total and serious adverse
events, hospital deaths, and in ICU and
hospital length of stay.
Our study has several strengths. First,
to our knowledge, this is the largest
RCT investigating a prophylactic intervention in a high-risk population undergoing CABG surgery. During study
implementation, we enrolled 62.6%
(295/471) of patients assessed for eligibility. Our results are therefore generalizable to a frequently encountered
subset of patients undergoing a commonly performed surgery. Second, it is
the first RCT to investigate the effect
of prophylactic N-acetylcysteine administration on postoperative renal
function in elective and urgent CABG
patients exposed to CPB. Third, the internal validity of our trial was strengthened by use of central randomization,
allocation concealment, and multilevel blinding (patients, physicians, data
collectors, and data analysts). Fourth,
we used a strategy of delayed randomization to minimize the potential for patients to be exposed to study medication in the event of cancelled, altered,
or postponed surgery. Fifth, we admin-
Table 3. Postoperative Outcomes*
No. (%)
N-acetylcysteine Group
(n = 148)
Primary outcome
Increase in serum creatinine level†
Secondary outcomes
Interventions
Vasoactive drugs
Renal dose dopamine
MV ⱖ48 h
IABP insertion
Reoperation within 24 h
Complications
Myocardial infarction
Stroke
Bloodstream infection
Mediastinitis
Hospital outcomes
RRT during hospital stay
Hospital deaths
Adverse events
Serious adverse events
All adverse events
Placebo Group
(n = 147*)
Unadjusted
P Value
44 (29.7)
42 (29.0)
.89
36 (24.3)
16 (10.8)
8 (5.4)
6 (4.1)
2 (1.4)
41 (28.1)
9 (6.2)
12 (8.2)
8 (5.5)
3 (2.1)
.47
.15
.34
.57
.68‡
5 (3.4)
3 (2.0)
4 (2.7)
7 (4.8)
6 (4.1)
2 (1.4)
.54
.33‡
.68‡
2 (1.4)
1 (0.7)
⬎.99‡
1 (0.7)
5 (3.4)
3 (2.1)
4 (2.7)
.37‡
⬎.99‡
1 (0.7)
9 (6.1)
0 (0)
14 (9.6)
⬎.99‡
.26
Abbreviations: IABP, intra-aortic balloon pump; MV, mechanical ventilation; RRT, renal replacement therapy.
*While 148 and 147 patients in the N-acetylcysteine and placebo groups, respectively, were eligible for the intentionto-treat analysis of the primary outcome, serum creatinine measurements were not available for 2 placebo patients
who died perioperatively (1 preoperative and 1 postoperative death; comparison, 148 N-acetylcysteine vs 145 placebo). While the number of patients meeting the per-protocol definition for the primary outcome was 143 and 143 in
the N-acetylcysteine and placebo groups, respectively, the numbers with serum creatinine measurements available
were 143 and 142, respectively. The per-protocol analysis of the primary outcome does not include measurements
for 4 off-pump coronary artery bypass graft surgery patients (including 1 patient who did not receive medication) and
1 valve surgery patient in the N-acetylcysteine group. Similarly, it does not include data for 1 patient who underwent
valve surgery, 3 patients who did not receive medication (including 1 preoperative death), and 1 postoperative death
in the placebo group. Secondary outcomes were not available for 1 patient who died prior to surgery in the placebo
group.
†An absolute increase in serum creatinine level greater than 0.5 mg/dL (44 µmol/L) or a 25% increase from baseline at
any time within the first 5 postoperative days.
‡Fisher exact P value.
©2005 American Medical Association. All rights reserved.
(Reprinted) JAMA, July 20, 2005—Vol 294, No. 3
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
347
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
Table 4. Adverse Events*
N-acetylcysteine Placebo
Group
Group
(n = 148)
(n = 147)*
All adverse events
Nausea
Vomiting
Nausea and
vomiting
Serious adverse
events
Hypotension
Total adverse
events
3
4
8
3
1
3
1
0
9
14
*Number of patients experiencing adverse events in the Nacetylcysteine and placebo groups. See footnote to Table
3 pertaining to secondary outcomes.
istered the study intervention intravenously prior to and following CPB
exposure to maximize renal exposure
to N-acetylcysteine. Finally, we identified a high-risk cohort of CABG
surgery patients using the study inclusion criteria. This assertion is supported by the fact that 29% of participants developed the primary outcome,
and approximately one quarter of
participants required vasoactive medications.
Our study also has limitations. First,
despite randomization, we noted potentially important imbalances in the proportion of patients with preoperative
CHF and planned CABG plus valve surgery between the N-acetylcysteine and
placebo groups. These imbalances
occurred by chance alone. To address
the potential for these imbalances to bias
study results, we conducted adjusted
analyses. The adjusted analyses remained nonsignificant for all primary
and secondary outcomes. Second,
despite efforts to minimize the potential for ineligible patients to be randomized through preoperative screening and implementation of delayed
randomization, 2 patients underwent
valve surgery alone and 4 underwent
OPCAB. Ultimately, the decision of
whether CABG surgery can be performed or whether it should be performed without CPB rests with the cardiac surgeon and is dependent on
anatomic and clinical considerations at
the time of surgery. Notwithstanding,
per-protocol analyses supported that
N-acetylcysteine did not prevent postoperative renal dysfunction.
Compared with placebo, RCTs investigating single-dose, preoperative ␣2-adrenergic agonists,27 infusions of intraoperative nifedipine28 or prostaglandin
E129 and intraoperative and postoperative fenoldopam30 or diltiazem 31 in
usual-risk patients undergoing CABG
surgery with CPB demonstrated that the
experimental interventions prevented
deterioration in postoperative renal
function, 27,28 urine N-acetyl--Dglucosamine,29 urine 2-microglobulin, 29 free water clearance, 29 and
improved creatinine clearance30 and glomerular filtration rate.31 Conversely, a
cohort study and RCTs investigating
prophylactic intraoperative and postoperative interventions in high-risk
patients undergoing on-pump CABG
surgery produced variable results. In a
multicenter, prospective cohort study,
Ranucci and colleagues32 evaluated
fenoldopam in 216 patients with serum
creatinine levels of at least 1.8 mg/dL
(160 µmol/L) and an additional entry
criterion (age, diabetes, decreased ejection fraction). The authors found significant reductions in the incidence of
acute renal failure and death and attenuation of postoperative decrements in
creatinine clearance. Investigators also
compared the prophylactic administration of pentoxifylline33 and enoximone (a phosphodiesterase III inhibitor)34 with placebo in separate studies
each involving 40 elderly elective CABG
patients. These trials demonstrated
reductions in bypass-induced inflammatory mediators and significantly
smaller increases in ␣-1 microglobulin
in the intervention groups compared
with controls, with no demonstrable
effect on serum creatinine level. Conversely, an RCT investigating low- and
high-dose diltiazem infusions in 24 elective cardiac surgery patients with
elevated preoperative serum creatinine
levels found no differences in serum creatinine level and glomerular filtration
rate, measured by iohexol, in the first 5
postoperative days, but a higher glomerular filtration rate 3 weeks after surgery
in the diltiazem group compared with
348 JAMA, July 20, 2005—Vol 294, No. 3 (Reprinted)
the placebo group.35 A further RCT compared esmolol plus enoximone with placebo in 42 patients older than 65 years
and demonstrated significantly decreased
creatinine clearance in patients treated
with placebo on the first postoperative
day.36 Important differences in the populations studied, interventions applied,
and outcomes measured may have
resulted in discordant findings between
studies investigating usual- and highrisk patients and among studies involving high-risk patients.
While 29% of participants in both
groups developed laboratory evidence
of renal dysfunction in our study, few
patients experienced clinically important morbidity or mortality. It is conceivable that a treatment effect may have
been missed as a result of the population studied or the primary outcome
selected. Preoperative renal dysfunction8,11,14 and age8,11,13 are important
baseline determinants of postoperative renal function and outcomes. Two
RCTs investigating high-risk CABG candidates made baseline renal dysfunction (serum creatinine ⱖ1.8 mg/dL [160
µmol/L]32 or between 1.4 mg/dL and 3.4
mg/dL [120 and 300 µmol/L35]) a compulsory inclusion criterion. Similar to
other studies,33,34,36 we included renal
dysfunction (serum creatinine ⬎1.4
mg/dL [120 µmol/L]) as one of several
inclusion criteria. As a result, we
observed a mean pooled baseline creatinine level of 1.2 mg/dL (103.7 µmol/
L), which was lower than studies including elevated baseline creatinine as a
compulsory criterion (2.4 mg/dL [216
µmol/L32] and 1.8 mg/dL [155 µmol/
L35]) but higher than studies including it as one of many criteria (1.2 mg/dL
[102 µmol/L],33 0.9 mg/dL [79.6 µmol/
L]34 and approximately 0.7 mg/dL [60
µmol/L36]). Consequently, only 23.0%
of our participants had a baseline serum
creatinine level greater than 1.4 mg/dL
(120 µmol/L). A post hoc subgroup
analysis of patients with baseline creatinine level greater than 1.4 mg/dL (120
µmol/L) demonstrated a nonsignificant trend toward fewer patients experiencing renal dysfunction in the N-acetylcysteine group compared with the
©2005 American Medical Association. All rights reserved.
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
placebo group. While of interest, this
post hoc analysis is underpowered,
exploratory in nature, and potentially
confounded by other factors influencing postoperative renal function. Similarly, while age of at least 70 years was
one of our inclusion criteria, 3 RCTs
investigating high-risk patients limited enrollment to patients older than
80 years33,34 or older than 65 years.36 The
pooled age in our study was 69.0 years,
with 61.1% of our participants at least
70 years old. Therefore, while similar,
our cohort was younger than those
investigated by the other authors (69.5
years,32 83.5 years,33 81.5 years,34 72.5
years, 35 and 70.5 years 36 ). In summary, compared with other high-risk
studies, we identified a slightly younger
population with mild to moderate renal
dysfunction. Consequently, our population, while at risk for experiencing
postoperative renal dysfunction, may
not have been at appreciable risk for
developing clinically important morbidity or mortality.
The definition and selection of the
primary outcome warrant consideration in interpreting our results. We
selected a surrogate outcome, commonly used in studies of contrastinduced nephropathy, as the primary
outcome. Since the serum creatinine
level typically peaks after CABG surgery with CPB on the second postoperative day and returns to baseline by
the fourth and fifth postoperative days,37
we expected to capture postoperative
renal dysfunction with our definition.
Notwithstanding, while we identified
laboratory evidence of renal dysfunction at the thresholds adopted, few patients experienced important clinical
events, suggesting that the threshold
may be too low for this population. Two
observational studies examining renal
dysfunction following CABG surgery
and demonstrating effects on clinical
outcomes used higher thresholds (⬎0.7
mg/dL [62 µmol] increase from baseline or a serum creatinine level ⬎2.0
mg/dL [177 µmol/L] and ⬎0.9 mg/dL
[80 µmol/L] increase with a serum creatinine level ⬎2.1 mg/dL [185 µmol/
L]).8,11 A higher threshold may aid in
identifying a subset of patients at risk
for important sequelae and in differentiating responses to interventions. Conversely, a lower threshold may have
captured unimportant events associated with the effects of volume shifts
and pressure changes on the kidney. Finally, compared with cystatin C, some
authors have recently suggested that serum creatinine may not be a valid
marker of postoperative renal dysfunction.38,39
Regardless of the entry criteria or outcome measure selected, there are several possible reasons why we did not
observe a treatment effect. First, Nacetylcysteine may be ineffective in preventing postoperative renal dysfunction following CPB exposure. Second,
the dose, while being well studied for
prevention of contrast-induced nephropathy, may be inadequate to counteract the hypoxic-ischemic insults to
the renal tubular epithelial cells induced by CPB. Third, the timing of administration of the initial dose may be
important. We administered the initial dose of N-acetylcysteine at induction of anesthesia leaving marginal time
for N-acetylcysteine to interfere with expression of adhesion molecules, Nacetylcysteinetivate nuclear factorkappa  in mesangial cells, and exert
its vasodilatory effect. Fourth, the activity of N-acetylcysteine may be overwhelmed by the formation of reactive
oxygen species with concurrent depletion of antioxidants during and after
CPB.40-42 Fifth, the multifactorial renal
dysfunction observed following CABG
surgery may not be amenable to the antioxidant and vasodilatory effects of Nacetylcysteine. Alternatively, postoperative renal insults may be additive,
and N-acetylcysteine may only counteract CPB-induced hypoxemicischemic insults.
CONCLUSION
In this study, perioperative, intravenous intermittent-dose N-acetylcysteine did not prevent postoperative renal
dysfunction, interventions, or complications compared with placebo in highrisk patients undergoing on-pump
©2005 American Medical Association. All rights reserved.
CABG surgery. Before additional prophylaxis trials are initiated to investigate alternative N-acetylcysteine dosing regimens, further research is required
to identify CABG patients at risk for
postoperative renal events, valid markers of renal dysfunction, and to establish renal thresholds associated with important clinical outcomes.
Author Affiliations: Divisions of Critical Care Medicine (Drs Burns and Martin), Nephrology (Dr Moist,
Ms Gallo, Mr Heidenheim), Cardiac Surgery (Drs Chu,
Novick, and Myers and Ms Fox) and the Department
of Biostatistics (Mr Stitt) at the University of Western
Ontario, London, Ontario.
Author Contributions: Drs Burns and Moist had full
access to all of the data in the study and take responsibility for the integrity of the data and the accuracy
of the data analysis.
Study concept and design: Burns, Chu, Novick, Martin,
Stitt, Moist.
Acquisition of data: Burns, Chu, Novick, Fox, Gallo,
Heidenheim, Myers, Moist.
Analysis and interpretation of data: Burns, Chu, Fox,
Martin, Stitt, Heidenheim, Moist.
Drafting of the manuscript: Burns, Moist.
Critical revision of the manuscript for important intellectual content: Burns, Chu, Novick, Fox, Gallo,
Martin, Stitt, Heidenheim, Myers, Moist.
Statistical analysis: Stitt, Heidenheim.
Obtained funding: Burns, Chu, Novick, Martin, Moist.
Administrative, technical, or material support: Burns,
Chu, Novick, Fox, Gallo, Heidenheim, Myers, Moist.
Study supervision: Burns, Novick, Martin, Myers, Moist.
Financial Disclosures: None reported.
Funding/Support: This study was funded by research grants obtained from the Lawson Health Research Institute and Physician Services Incorporated.
Dr Burns holds a postdoctoral fellowship from the Canadian Institutes for Health Research. Dr Chu is the
recipient of the William T. MacEachern Research Fellowship.
Role of the Sponsor: The funding sources had no influence in study design and conduct; data collection,
analysis, and interpretation; manuscript preparation;
or in the decision to submit the manuscript for publication.
Acknowledgment: We are indebted to the pharmacists, anesthetists, cardiac surgeons, intensivists, and
intensive care nursing staff of both hospitals for their
cooperation in this study.
REFERENCES
1. Abramov D, Tamariz MG, Fremes SE, et al. Trends
in coronary artery bypass surgery results: a recent,
9-year study. Ann Thorac Surg. 2000;70:84-90.
2. Katz NM, Wolfe-Pearce JL, Chase GA. Comparison of results and risk factors of cardiac surgery in two
3-year time periods in the 1990’s. Am J Cardiol. 1998;
81:1400-1404.
3. Ferguson TB, Hammill BG, Peterson ED, De Long
ER, Grover FL; the STS National Database Committee.
A decade of change—risk profiles and outcomes for
isolated coronary artery bypass grafting procedures,
1990-1999: a report from the STS National Database
Committee and the Duke Clinical Research Institute.
Ann Thorac Surg. 2002;73:480-490.
4. Ivanov J, Weisel RD, David TE, Naylor CD. Fifteen
year trends in risk severity and operative mortality in
elderly patients undergoing coronary artery bypass graft
surgery. Circulation. 1998;97:673-680.
5. McGrath LB, Laub GW, Graf D, Gonzalez-Lavin L.
(Reprinted) JAMA, July 20, 2005—Vol 294, No. 3
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007
349
N-ACETYLCYSTEINE IN CORONARY ARTERY BYPASS GRAFT PATIENTS
Hospital death on a cardiac surgical service: negative
influence of changing practice patterns. Ann Thorac
Surg. 1990;49:410-412.
6. Moshkovitz Y, Paz Y, Shabtai E, et al. Predictors
of early and overall outcome in coronary artery bypass without cardiopulmonary bypass. Eur J Cardiothorac Surg. 1997;12:31-39.
7. Zanardo G, Michielon P, Paccagnella A, et al. Acute
renal failure in the patient undergoing cardiac operation: prevalence, mortality rate and main risk factors.
J Thorac Cardiovasc Surg. 1994;107:1489-1495.
8. Mangano CM, Diamondstone LS, Ramsay JG, Aggarwal A, Herskowitz A, Mangano DT. Renal dysfunction after myocardial revascularization: risk factors, adverse outcomes and hospital resource utilization.
Ann Intern Med. 1998;128:194-203.
9. Chertow GM, Levy EM, Hammermeister KE, Grover
F, Daley J. Independent association between acute renal failure and mortality following cardiac surgery. Am
J Med. 1998;104:343-348.
10. Naylor CD, Rothwell DM, Tu JV, Austin P; the
Steering Committee of the Cardiac Care Network of
Ontario. Outcomes of coronary artery bypass surgery in Ontario. In: Naylor CD, Slaughter PM, eds. Cardiovascular Health and Services in Ontario: An ICES
Atlas. Toronto, Ontario: Institute for Clinical Evaluative Sciences; 1999:189-197.
11. Antunes PE, Prieto D, Ferrao de Oliveira J, Antunes MJ. Renal dysfunction after myocardial
revascularization. Eur J Cardiothorac Surg. 2004;
25:597-604.
12. Chattas MA, Sethna DH, Rezkana H, et al. Patterns of acute renal failure requiring dialysis after open
heart surgery. Anesth Analg. 1986;65:S57.
13. Bove T, Grazia Calabro M, Landoni G, et al. The
incidence and risk of acute renal failure after cardiac
surgery. J Cardiothorac Vasc Anesth. 2004;18:442-445.
14. Chertow GM, Lazarus JM, Christensen CL, et al.
Preoperative renal risk stratification. Circulation. 1997;
95:878-884.
15. Bucerius J, Gummert JF, Walther T, et al. Predictors of prolonged ICU stay after on-pump versus offpump coronary artery bypass grafting. Intensive Care
Med. 2004;30:88-95.
16. Yoshioka T, Fogo A, Beckman JK. Reduced activity of antioxidant enzymes underlies contrast mediainduced renal injury in volume depletion. Kidney Int.
1992;41:1008-1015.
17. Baliga R, Ueda N, Walker PD, Shaw SW. Oxidant mechanisms in toxic acute renal failure. Am J Kidney Dis. 1997;29:465-477.
18. Bakris GL, Lass M, Gaber AO, et al. Radiocontrast medium induced declines in renal function: a role
for oxygen free radicals. Am J Physiol. 1990;258:F115F120.
19. Perrella MA, Edell ES, Krowka MJ, Cortese DA,
Burnett JC Jr. Endothelium-derived relaxant factor in
pulmonary and renal circulation during hypoxia. Am
J Physiol. 1992;263:R45-R50.
20. Birck R, Krzossok S, Markowetz F, Schnulle P, van
der Woude FJ, Braun C. Acetylcysteine for prevention of contrast nephropathy: meta-analysis. Lancet.
2003;362:598-603.
21. Isenbarger DW, Kent SM, O’Malley PG. Metaanalysis of randomized clinical trials on the usefulness of acetylcysteine for prevention of contrast
nephropathy. Am J Cardiol. 2003;92:1454-1458.
22. Alonso A, Lau J, Jaber BL, Weintraub A, Sarnak
MJ. Prevention of radiocontrast nephropathy with Nacetylcysteine in patients with chronic kidney disease: a meta-analysis of randomized, controlled trials.
Am J Kidney Dis. 2004;43:1-9.
23. Guru V, Fremes SE. The role of N-acetylcysteine
in preventing radiographic contrast-induced
nephropathy. Clin Nephrol. 2004;62:77-83.
24. Misra D, Leibowitz K, Gowda RM, Shapiro M, Khan
IA. Role of N-acetylcysteine in prevention of contrastinduced nephropathy after cardiovascular procedures: a meta-analysis. Clin Cardiol. 2004;27:607-610.
25. Tepel M, van der Giet M, Schwarzfeld C, Laufer
U, Liermann D, Zidek W. Prevention of radiographiccontrast agent induced reductions in renal function by
acetylcysteine. N Engl J Med. 2000;343:180-184.
26. Baker CSR, Wragg A, Kumar S, DePalma R, Baker
LRI. A rapid protocol for the prevention of contrastinduced renal dysfunction: the RAPPID study. J Am
Coll Cardiol. 2003;41:2114-2118.
27. Kulka PJ, Tryba M, Zenz M. Preoperative alpha2adrenergic receptor agonists prevent the deterioraton of renal function after cardiac surgery: results of
a randomized, controlled trial. Crit Care Med. 1996;
24:947-952.
28. Bertolissi M, Antonucci F, De Monte A, Padovani R, Giordano F. Effects on renal function of a
continuous infusion of nifedipine during cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 1996;10:
238-242.
29. Abe K, Sakakiara T, Yoshiya L. The effect of prostaglandin E1 on renal function after cardiac surgery
involving cardiopulmonary bypass. Prostaglandins Leukot Essent Fatty Acids. 1993;49:627-631.
30. Caimmi PP, Pagani L, Micalizzi E, et al. Fenoldopam for renal protection in patients undergoing cardiopulmonary bypass. J Cardiothorac Vasc Anesth.
2003;17:491-494.
31. Zanardo G, Michielon P, Rosi P, et al. Effects of a
350 JAMA, July 20, 2005—Vol 294, No. 3 (Reprinted)
continuous diltiazem infusion on renal function during cardiac surgery. J Cardiothorac Vasc Anesth. 1993;
7:711-716.
32. Ranucci M, Soro G, Barzaghi N, et al. Fenoldopam prophylaxis of postoperative acute renal failure
in high-risk cardiac surgery patients. Ann Thorac Surg.
2004;78:1332-1338.
33. Boldt J, Brosch C, Piper SN, Suttner S, Lehmann
A, Werling C. Influence of prophylactic use of pentoxifylline on postoperative organ dysfunction in elderly cardiac surgery patients. Crit Care Med. 2001;29:
952-958.
34. Boldt J, Brosch C, Suttner S, Piper SN, Lehmann
A, Werling C. Prophylactic use of the phosphodiesterase III inhibitor enoximone in elderly cardiac surgery patients: effect on hemodynamics, inflammation and markers of organ function. Intensive Care
Med. 2002;28:1462-1469.
35. Bergman AS, Odar-Cederlof I, Westman L,
Bjellerup P, Hoglund P, Ohqvist G. Diltiazem infusion
for renal protection in cardiac surgical patients with
preexisting renal dysfunction. J Cardiothorac Vasc
Anesth. 2002;16:294-299.
36. Boldt J, Brosch C, Lehmann A, Suttner S, Isgro F.
The prophylactic use of the -blocker esmolol in combination with phosphodiesterase III inhibitor enoximone in elderly cardiac surgery patients. Anesth Analg.
2004;99:1009-1017.
37. Stafford Smith M. Perioperative renal dysfunction: implications and strategies for protection. In: Newman MF, ed. Perioperative Organ Protection. Richmond, Va: Society of Cardiovascular Anesthesiologists;
2003:89-124.
38. Hoffmann U, Fischereder M, Kruger B, Drobnik
W, Kramer BK. The value of N-acetylcysteine in the
prevention of radiocontrast agent-induced nephropathy seems questionable. J Am Soc Nephrol. 2004;15:
407-410.
39. Dharnidharka VR, Kwon C, Stevens G. Serum cystatin C is superior to serum creatinine as a marker of
kidney function: a meta-analysis. Am J Kidney Dis.
2002;40:221-226.
40. Zhang H, Spapen H, Nugyen DN, Rogiers P, Bakker J, Vincent JL. Effects of N-acetylcysteine on regional blood glow during endotoxic shock. Eur Surg
Res. 1995;27:292-300.
41. DiMari J, Megyesi J, Udvarhelyi N, Price P, Davis
R, Safirstein R. N-acetylcysteine ameliorates ischemic
renal failure. Am J Physiol. 1997;272:F292-F298.
42. Khachigian LM, Collins T, Fries JW. Nacetylcysteine blocks mesangial VCAM-1 and NFkappa B expression in vivo. Am J Pathol. 1997;151:
1225-1229.
©2005 American Medical Association. All rights reserved.
Downloaded from www.jama.com at Medical Library of the PLA, on August 22, 2007