DIAGNOSTIC METHODS
MYOCARDIAL INFARCTION
Quantitative assessment of myocardial ischemia and
necrosis by continuous vectorcardiography and
measurement of creatine kinase release in patients
MAGNUS SEDERHOLM, M.D., PER GRT-rTUM, M.D., LEIF ERHARDT, M.D.,
AND JOHN KJEKSHUS, M.D.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
ABSTRACT The accuracy of the use of the maximal QRS vector difference to estimate myocardial
infarct size irrespective of infarct location was compared with that of measurement of cumulative
creatine kinase (CK) release. Sixty patients with acute myocardial infarction and a history of symptoms
of less than 4 hr duration were followed for 24 to 72 hr with orthogonal vectorcardiography and CK
release analysis. Spatial QRS vector differences were calculated between the first QRS complex
recorded and subsequent QRS complexes at timed intervals. The QRS vector difference increased
rapidly and reached a plateau at an average 12.1 hr after onset of symptoms, as compared with 34.0 hr
for the cumulated CK release. In 42% of the patients a stepwise progression of infarct evolution was
observed. Irrespective of infarct location the maximal spatial ST vector magnitude was related to the
ultimate QRS vector difference (r = .80) and to the cumulative amount of CK released (r
.64).
Furthermore, maximal QRS vector difference correlated well with the maximal cumulative CK release
(r - .64) Ten patients had possible infarct expansion, as indicated by recurrent QRS changes without
concomitant CK release. Fifteen patients had infarct extension that was indicated by secondary CK
release and that in seven patients was associated with further QRS changes. Infarct extension caused an
approximate 25% increase in infarct size. Spatial ST vector magnitude, QRS vector difference, and
cumulative CK release are complementary measures in the quantification of evolving myocardial injury
after acute coronary occlusion and in the determination of sequels to therapeutic interventions.
Circulation 68, No. 5, 1006-1012, 1983.
=
ACUTE MYOCARDIAL ISCHEMIA and infarction
are dynamic processes and information on the size and
progression of infarction with time is potentially important in coronary care. The use of continuous vectorcardiography (VCG) to monitor patients was suggested by Hodges et al.,' and has been further adapted for
the evaluation of acute myocardial infarction (AMI). 2-5
Serial analysis of spatial VCGs permits a simple and
convenient determination of temporal and quantitative
changes in the QRS complex and ST segment. In contrast to precordial electrocardiographic mapping,
which applies quantitatively only to anterior myocardial infarcts, spatial VCG can be used irrespective of
infarct location since the electromotive forces are reduced to three equipotential orthogonal leads.
ST segment deviations vary markedly during the
From the Cardiology Section, Danderyds Hospital, Danderyd, Swe-
den, Institute of Informatics, University of Oslo, Oslo, Norway, and
Cardiology Section, Barum Hospital, Sandvika, Norway.
Address for correspondence: John Kjekshus, M.D., Berum Hospital, 1316, Sandvika, Norway.
Received April 4, 1983; revision accepted July 14, 1983.
1006
early phase of an AMI and continuous recording is
necessary to capture the maximum deviation. In animal experiments this value defines the area of the reversible injury and predicts the ultimate infarct size.6'7
QRS changes closely reflect myocardial cell death8 and
serial analysis of VCGs may provide important information about the rate and extent of infarction. The
vectorial deviations of the QRS complex from preinfarction values theoretically reflect the loss of electrically active myocardium due to irreversible damage.9 10 This vector difference has been shown to
correlate with morphometric measurements of infarct
size in animal experiments."' 12 In the clinical setting
the premorbid reference VCG is rarely available.
However, the onset of symptoms does not necessarily
mean that the necrotic process has started but simply
that the patient has ongoing myocardial ischemia. Necrosis, as reflected by changes in the QRS complex,
may develop after various time intervals, but usually
begins developing after 1 to 2 hr.'3 Thus, when obtained early, the first QRS complex may prove valid as
a reference value.
CIRCULATION
DIAGNOSTIC METHODS-MYOCARDIAL
INFARCTION
In this study we have examined the possible usefulof continuous recordings of spatial ST and QRS
vectors in the assessment of the evolution of ischemia
and necrosis in AMI and compared these indices with
the cumulative release of myocardial creatine kinase
(CK).
represent the Cartesian coordinates of the summation vector for
each beat. The reproducibility of this procedure was tested and
gave a coefficient of variation of 4% for repeated measurements. The first recording obtained was chosen as the reference
and all subsequent recordings were vectorially subtracted from
this to give the QRS vector difference (QRS-VD) according to
the formula
Patients and methods
QRS-VD (gV sec) = V(XXr XX2)2 + (EYr<Yi) + ($ZrXZi)
ness
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Sixty patients (45 men and 15 women, age range 37 to 78
years) with AMI completed this study. All patients fulfilled the
following inclusion criteria: (1) no previous history or past
electrocardiographic sign of myocardial infarction, (2) admitted
within 4 hr after onset of symptoms, (3) no intraventricular
conduction defects (QRS duration S 0.11 sec), (4) typical
symptoms for more than 30 min and ST segment elevation > 1
mm in leads I, II, III, aVL, and aVF or > 2 mm in V3 through
V6, (5) no pericardial friction rub on admission. None of the
patients received intramuscular injections or required cardioversion during the study period, and no patients showed severe
electrolyte disturbances. Twelve patients were excluded from
the study, five because they did not survive long enough for
adequate CK and VCG analysis and seven because they developed bundle branch block or QRS duration >0.11 sec.
Blood samples for CK analysis were drawn every second
hour until the twelfth hour and thereafter every fourth through
sixth hour up to 72 hr. The enzyme concentration was measured
by a standard Autoanalyzer technique.'4 Accumulated CK release was computed from the time-activity curves assuming a
first-order elimination from one compartment. If the descending
limb of the time-activity curve was smoothly declining over at
least five consecutive observations, an individual elimination
rate constant, kD, was calculated by exponential curve fitting of
these segments. Otherwise a standard kD of 0.0576 hr-', equivalent to the mean value of all individual kDS, was used for
calculating the cumulative CK release curves. This procedure
was chosen to avoid spuriously low kDS due to recurrent or
continuous CK release. A polyphasic CK release was defined as
two or more distinct plateaus in the cumulative CK curve, each
differing more than 10% from the previous one. CK plateau
levels (CKmax) and the corresponding time from onset of symptoms to plateau level (CK release time) were determined from
each curve.
As soon as possible after admission, electrodes were attached
to the patients according to the Frank orthogonal lead system. '5
The X, Y, and Z lead tracings were continuously recorded for
24 hr with an ICR vectorcardiograph connected to an analog
tape recorder running at 15/16 inch/sec (2.38 cm/sec). Sequential analysis of the ST and QRS vectors were done hourly and
plotted as a function of time.
The spatial ST vector magnitude (ST-VM) was calculated
with the formula
ST-VM (mV)
=
VX2
+ y2 + Z2
where X, Y, and Z represents the coordinates of the ST projections on the three orthogonal axes: X, right to left; Y, head to
foot; and Z, anterior to posterior. ST-VM was calculated 20
msec after the termination of the QRS complex (J point) and the
isoelectric baseline was drawn between adjacent PQ segments.
All scalar QRS complexes were digitized on a microcomputer
system. The horizontal resolution corresponded to 2 msec and
the vertical resolution to 2.5 ,uV. The onset and offset of the
QRS complex was visually determined. For each lead the QRS
complex was summed between onset and offset. These sums
Vol. 68, No. 5, November 1983
where XX,XY, and EZ denote lead sums from onset to offset of
QRS complex, r is the reference beat, and i is the current beat.
The QRS-VD and ST-VM were plotted as a function of time
from onset of symptoms. From these graphs the following parameters were determined: maximal ST-VM recorded during
the registration period (ST-VMmax), maximal QRS-VD (QRSVDmax), and the duration of the QRS vector evolution from
onset of symptoms to plateau level (QRS evolution time). Polyphasic evolution of the QRS vector changes was arbitrarily
defined as a new permanent change of at least 10%, preceded by
a plateau of more than 2 hr duration.
Statistical computations were performed with the BMDP-8 1
package (Biomedical Computer Programs, Health Sciences
Computing Facility, UCLA). Comparison of group means was
by Wilcoxon nonparametric statistical analysis. All values are
given as mean and range.
Results
The sampling of CK and recording of VCGs began
on average 2.55 (0 to 4.0) hr after onset of symptoms.
Monophasic infarct evolution. Monophasic infarct
evolution as reflected by the cumulative CK release
and the QRS-VD was found in 35 of the 60 patients.
Figure 1, A, illustrates a typical monophasic infarct
evolution. Average CKmax for the monophasic infarcts
was 3197 (I 10 to 7900) IU/1 and QRS-VDmax was 25.0
(2.6 to 68.9) ,uV sec. The average CK release time
was 27.4 (8.0 to 50.0) hr and was considerably longer
than the QRS evolution time of 9.7 (1.0 to 19.0) hr
(p < .001).
The relationship between CKmax and QRSVDmax is
shown in figure 2, and suggests an association between
the two independent indices of myocardial necrosis (r
= .65). The average ST-VMmaX for monophasic infarcts was 0.264 (0.050 to 0.590) mV and was reduced
by 27% after 1 hr (p < .001). A close correlation was
obtained between ST-VMmax and QRS-VDmax (r = .80;
figure 3, closed circles) and between ST-VMmaX and
CKm, (r = .69; figure 4, closed circles). Separate
examination of 13 patients admitted within 2 hr of
onset of symptoms showed no significant differences
in the regressions between ST-VMmaX and QRS-VDmax,
ST-VMmax and CKmaxW and QRS-VDmax and CKmW, but
the dispersions were smaller for the early admissions.
Biphasic infarct evolution. Biphasic infarct evolution
was found in 25 patients (42%); in 15 patients it was
evident from the CK release curves and in 17 patients it
1007
SEDERHOLM et al.
QRS-VD ST-VM
mV
PVs
0.3
20 -
infarcts. Phase II was normally preceded by a recurrent
rise in ST-VM. To define the importance of
3000
as a determinant of ultimate infarct size in biphasic
infarcts, regressions of ST-VMmax vs QRS-VDmax and
CKmax were performed for phase I and phase II. The
best relationships were obtained for phase II and they
conformed to the corresponding monophasic regressions (figures 3 and 4, open circles; r = .81 and .59 for
ST-VMmax vs QRS-VDmax and CKmax, respectively).
The relationship between CKmax and QRS-VDmax for
phase II closely matched that for monophasic infarcts
(figure 2, open circles; r = .62) and the combined
regression was CKmax = 75.5 X QRS-VDmax + 1330
(r = .64). In further analysis terminal values for CK
release and QRS-VD were used irrespective of monophasic or biphasic infarct course.
Infarct location. There were 28 anterior and 32 inferior infarcts. Salient data are listed in table 2. Inferior
infarcts tended to have somewhat longer CK release
and QRS evolution times and to be smaller, as reflected by the CK release, the QRS-VD evolution, and STsegment changes, when compared with anterior infarcts. However, only the difference in QRS-VDmax
values reached significance (p = .034). Infarct location did not influence the relationship between STVMmax and QRS-VDmax, ST-VMmaX and CKmax, or between QRS-VDmax and CKmax. Seven patients had left
anterior hemiblock and two patients had left posterior
hemiblock. The relationships between ST-VMmax and
QRS-VDmax and between QRS-VDmax and CKmax ob-
-0.2
2000
10 -
-0.1
0
A
1000
50
10
40
20
30
Hours after onset of symptoms
QRS-VD ST-VM
iVs I mV
20 -
Cwr. CK
U/L
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
1500
io0
10 -
500
0
B
10
30
40
50
20
Hours after onset of symptoms
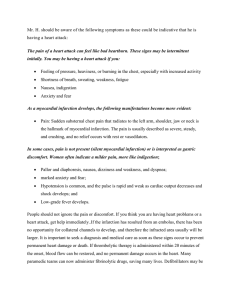
FIGURE 1. A, Monophasic infarct evolution as reflected by the temporal changes in cumulative CK release, spatial ST-VM, anci QRS-VD.
The recordings were started 3.5 hr after onset of symptoms. 'ST-VM was
maximal after 6 hr, the QRS-VD reached a plateau level afte r 17 hr, and
the CK release was complete after 31 hr. B, Biphasic infarc I evolution.
Recordings were started 3 hr after onset of symptoms. S;T-VM was
maximal at start of recording, with a second rise after 10 hi,r. QRS-VD
in5al nlntpnjl
leveled off after 8 hr, followed by a recurrent increase to a f111a1
plateau
after 17 hr. Similar but markedly delayed biphasic evolutiion was observed for cumulative CK, with plateau levels after 27 an d 38 hr.
was evident from the QRS-VD curves. In on ly seven
of these patients was a biphasic course obse-rved for
both parameters. Figure 1, B, illustrates a biphasic
infarct evolution pattern. Details on CK relf ease and
QRS-VD evolution for monophasic and bip]hasic infarcts are given in table 1.
CK release time and QRS evolution time tc) the first
plateau of biphasic infarcts (phase I) were s ,imilar to
times to first plateau of monophasic infarcts. The time
to the second plateau of biphasic infarcts (phasse II) was
about 80% longer than that to the plateau of nrionophasic infarcts (p < .001) and to phase I of biphasic
infarcts (p < .001). The magnitudes of C]Km.I and
QRS-VDmax both increased by 25% from plhase I to
phase II. Neither of these measures were stattistically
different from CKmax and QRS-VDmax of mo ,nophasic
1008
l~
Cum. CK
U/L
U/L
Io
8000 -
ST-VM.ax
.
.
.
X 6000S
0
* O
0
0
0
0 9, O
0 0
0
0
O
00
coo
2000-
.
0
0 0 0
0
0
0
0
Smonophasic
Ibiphasic
20
40
QRS-VD max
r=0.64
60
pVsec
FIGURE 2. The relationship between the ultimate CKmax and QRSVDmax (n = 5 1). The r value given is for all patients. For monophasic
infarcts alone r = .65 and for biphasic infarcts r = .62. The regression
equation for all patients is CKmax = 75.5 x QRS-VDmax + 1330.
CIRCULATION
DIAGNOSTIC METHODS-MYOCARDIAL INFARCTION
pVsec
0
0
60
0
40x
E
0
0
0
0
0
U)
0
0
O
A
0 0
*
S
20 1 0
00
00
0*
0
0
0
*
0
*0
00
0
00
0
0
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
r =0.80
0
* monophasic
o biphasic
0:3
0.6
mV
ST-VM max
FIGURE 3. The relationship between the initial spatial ST-VM and the
final maximal QRS-VD (n = 56). The r value given is for all patients.
For monophasic infarcts alone r = .80 and for biphasic infarcts r = .81.
The regression equation for all patients is QRS-VDmax = 72.8 x STVMmax + 7.0.
U-ooservec
servecu in: 4-ttnese patients contormec tO+ tnose
overall.
Elimination rate of CK. Individual k0 was calculated
in 44 patients and averaged 0.0576 (0.0276 to 0.08 10)
hr-'. Correlation analysis suggested that kD was not
related to CKmax, QRS-VDmax, or QRS evolution time.
-
4--
tivation may further reduce this fraction in patients
with large infarcts.2' Accordingly, large infarcts may
be underestimated by CK analysis.
Incorrect estimates of kD due to continuing CK release, fluctuations in blood volume, and drug effects
may impair estimates of infarct size.22 23 The mean
value and range of kD observed in this study was comparable to that obtained in a previous study23 and was
unrelated to the infarct size reflected by CK release and
the independent QRS-VD. Furthermore, kD was unrelated to infarct duration and infarct location.
Electrocardiographic changes have been used as
complements to enzyme analysis to describe acute
ischemic injury and ultimate myocardial necrosis. The
use of precordial ST-QRS mapping, as described by
Maroko et al. ,6, 24 is restricted to estimation of anterior
infarcts. In contrast, VCG can be used irrespective of
infarct location and a spatial vector can be constructed
assuming that the electrical activity of the heart can be
represented by dipoles and that the orthogonal leads
are equipotential. These assumptions have been criticized.25' 26
Regional intramyocardial conduction delays may
2
occur with myocardial infarction.27
If true vectorial
summation of the different regional dipoles can be
performed, conduction delays should not interfere
U/L
0
0
.
0
Discussion
Assessment of myocardial necrosis by measurement
of cumulated CK release is an empirical method that
has been well documented in experimental animals'6
and patients and correlations of .75 to .93 have been
found between cumulated CK release and morphometrically measured infarct size in man.'7-'9 The method
has several limitations, however.
Myocardial enzyme release reflects cell membrane
permeability changes rather than the occurrence of cell
death and will not correctly define the temporal progression of infarction. Furthermore, the appearance of
enzymes in circulating blood is delayed by the lag
phase between the different enzyme compartments.
The fraction of CK retrieved from the blood volume
is probably about 20% of the total myocardial CK
depletion.20 Impaired washout of CK from areas with
severely reduced blood flow leading to prolonged exposure to the myocardial lymph with subsequent inacVol. 68, No. 5, November 1983
0
0
0
0
A.
'U
4)
0
0
s0 0
0
0
4)
0
0
0
00
SOD
0.
0
S
*
0
0
.
0
0
0
0
*
*00
S
0
0
0
0
0
0
r=0.64
0
S
* monophasic
o biphasic
0.3
ST-VM max
6
mv
FIGURE 4. The relationship between the initial spatial ST-VM and the
final cumulative CK release (n = 58). The r value indicated is for all
patients. For monophasic infarcts alone r = .69 and for biphasic infarcts
r = .59. The regression equation for all patients is CKmax = 7180 x
ST-VMmax + 1530.
1009
SEDERHOLM et al.
TABLE 1
VCG and cumulative CK changes in monophasic and biphasic infarcts
Biphasic infarcts
(n = 25)
Monophasic infarcts
(n =35)
ST-VM
First phase
0.264 (0.050-0.590)
25.5 (2.6-68.9)
3197 (110-7900)
9.7 (1.0-19.0)
27.4 (8.0-50.0)
(mV)
QRS-VDma, (,uV sec)
CK .. (lU/l)
QRS evolution time (hr)
CK release time (hr)
21.1
3103
9.2
27.4
Second phase
0.276 (0.010-0.760)
26.3 (11.5-52.4)
(9.5-39.2)
3886 (900-8100)
(190-7100)
17.6 (8.0-30.0)
(3.0-15.0)
49.6 (28.0-70.0)
(9.0-39.5)
ST-VM at start of recording. Plateau values of QRS-VD and cumulative CK release are given for monophasic and for the first
and second levels of biphasic infarcts. QRS evolution and CK release times from onset of pain to each plateau are given. All
values are expressed as mean and range.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
with the QRS integrals since these are computed over
the entire QRS complex, thereby eliminating effects of
altered activation sequence. However, the present
study was not designed to evaluate effects of major
changes in ventricular conduction and patients developing bundle branch blocks were excluded. The relationships between QRS-VDmaX, ST-VMmaX, and CKmax
observed in patients presenting with left ventricular
hemiblocks conformed to those observed overall. During AMI early R wave changes unrelated to tissue
necrosis may cause erroneous estimates of infarct evolution.28 The changes have been attributed to reduced
conductivity, displacement of the isoelectric baseline,
or increased volume of the ventricles.29 They were,
however, of a very transient nature and subsided within 1 to 2 hr of onset of symptoms.30
Despite these objections, good correlations between
VCG estimates and postmortem examinations of infarct size in baboons"I and dogs2231 have been shown.
A close relationship between morphometric infarct
size and the integral of initial spatial vector magnitude
(r = .90) in patients has recently been reported32 and a
QRS score derived from the standard 12-lead electrocardiogram has been shown to relate to morphometric
assessments of anterior (r = 80)3 and inferior infarcts
(r = .74).34 Although the QRS-VD and cumulated CK
.
release are indirect measures of infarct size, the correlation between these indices obtained in the present study conforms well to results reported previously7-19. 32-34 and suggests that the QRS-VDs provide an
estimate of infarct size. This result is in contrast to that
of Wikswo et al. ,35 who found no relationship between
CK release and QRS changes. The discrepancy may be
explained by the small number of subjects in their
study and their inclusion of patients with previous
myocardial infarction or a history of symptoms of up to
6 hr. The use of a constant kD for calculating cumulated
CK release may also have adversely affected the relationship between CK release and QRS changes. Studies with precordial mapping support an association
between CK release and QRS changes in anterior infarcts.36-3 The present study extends these findings to
inferior infarcts.
One problem associated with infarct sizing from
QRS changes is the lack of a preinfarction reference.
In dog experiments Hillis et al. 13 found that the size of
the Q wave at 2 hr after occlusion was about a seventh
of the final Q wave at 24 hr. However, myocardial
infarction evolves more rapidly in dogs than in humans. Separate examination of the patients admitted
within or after 2 hr of onset of symptoms did not show
any significant differences in the regression of QRS-
TABLE 2
VCG and cumulative CK changes with respect to infarct location
Anterior infarcts
(n = 28)
ST-VMm.X (mV)
QRS-VDm. (/AV-sec)
CKmax (lU/l)
QRS evolution time (hr)
CK release time (hr)
0.318 (0.050-0.640)
32.3 (8.8-68.9)
3851 (110-8100)
11.0 (1.0-23.0)
30.7 (8.0-55.0)
Inferior infarcts
(n =- 32)
0.232
21.0
3052
13.3
37.2
(0.010-0.760)
(5.7-49.6)
(380-6200)
(3.0-30.0)
(13.0-70.0)
Total
n 60)
=
0.269
25.7
3410
12.1
34.0
(0.010-0.760)
(5.7-68.9)
(110-8100)
(1.0-30.0)
(8.0-70.0)
ST-VM at start of recording. Ultimate values for QRS-VD and cumulative CK release are given. QRS evolution and CK
release times are relative to onset of symptoms.
1010
CIRCULATION
DIAGNOSTIC METHODS-MYOCARDIAL INFARCTION
VDmax vs CKmx, although the correlation coefficients
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
were higher for those admitted early. These results
indicate that a VCG obtained within 4 hr of onset of
symptoms may be a valid reference for infarct size
estimation.
The use of ST segment changes as an indicator of
ischemia and predictor of ultimate myocardial necrosis
has been well established, despite theoretical limitations.39 ST segment changes are maximal within minutes after onset of myocardial ischemia and are subsequently reduced as infarction evolves or the ischemia is
reversed. This implies that the true ST-VMmaX may be
underestimated in many patients. The reduction in STVM of 27% after 1 hr emphasizes the importance of
early and continuous recording in obtaining the STVmm that, indirectly, is the tissue at risk of necrosis.
In the present study the ST-VMmI related equally well
to the ultimate QRS-VD and cumulated CK release.
Recordings obtained later than 4 hr after onset of pain
are probably less representative of the ST-VMmax and
therefore are not very useful as a predictor of the final
QRS vector changes.
About 40% of the patients showed electrocardiographic or enzymatic evidence of biphasic infarct evolution. Different pathophysiologic mechanisms may be
reflected by the stepwise changes in the respective
curves. Short-term changes in left ventricular volume
or thinning of the infarcted area without extension of
the actual necrosis have been shown to produce change
in the QRS complex.40'4' In the present study, 10 patients (17%) had a second permanent change in the
QRS-VD that was not accompanied by further CK
release, and this presumably reflected infarct expansion. Seven patients (12%) demonstrated a recurrent
rise in QRS-VD and cumulative CK release that
strongly suggested infarct extension. In eight patients
(13%) secondary CK release was observed without
associated QRS changes. This may be explained by
insufficient VCG observation time or increase in plasma CK independent of infarct extension caused by
changes in plasma volume or increased washout of
extravascular CK. Thus, between 12% and 25% of the
patients in this study showed infarct extension. This is
close to the incidence reported in previous studies 30 40, 42
The observation that ST-VMmax correlated better
with QRS-VDmax and CKma of the second plateau than
of the first plateau indicates that the ultimate size of the
necrosis is defined by the ischemia early after coronary
occlusion. However, part of the jeopardized myocardium will not be irreversibly injured until much later, as
indicated by the QRS evolution time of 9.2 hr to the
Vol. 68, No. 5, November 1983
first plateau vs 17.6 hr to the second plateau. This may
be due to nonuniform residual flow that results in different capacity for survival. This has considerable
bearing on the use of early intervention to limit infarct
size.
Patients with anterior wall infarcts tended to have a
higher ST-VMma, QRS-VDm ,,,, and CKmax than inferior
infarcts. This is probably due to the fact that in humans
a larger myocardial mass is supplied by the left anterior
descending artery than by the right circumflex artery.
The QRS evolution time was not related to infarct size,
but the time to complete the infarction was shorter in
anterior than in inferior infarcts (table 2), confirming
the results of a previous study.2
No single index presently available can accurately
assess the progression of the ischemic injury and the
ultimate infarct size. The changes in the VCG and the
enzyme release therefore have to be used as complementary indices. The present study shows that these
indices may be particularly valuable in trials of treatment aimed at limiting infarct size. Continuous analysis of the VCG permits semiquantitative assessment of
the evolving myocardial ischemia and infarction. Because infarct size varies over a wide range a large
patient group is needed to detect infarct reduction. The
group size can be reduced if the method of comparing
the infarct size predicted from initial ST-VM with the
observed size as measured by CK release and QRS-VD
is used. From this study it may be calculated that to
detect a 30% reduction of infarct size predicted from
the ST-VMmax obtained early, a minimum of 60 patients per group will be required to show a statistical
difference at a = .05 and 1-13 (power) = .80.
Since the QRS-VD on average evolves in less than
10 hr early intervention has to be started within 4 to 6
hr after onset of symptoms in order to prove effective.
References
1. Hodges M, Akiyama T, Biddle TL, Clarke WB, Roberts DL,
Kronenberg MW: Continuous recording of the vectorcardiogram in
acutely ill patients. Am Heart J 88: 593, 1974
2. Sederholm M, Erhardt L, Sj0gren A: Continuous vectorcardiography in acute myocardial infarction. Natural course of ST and
QRS-vectors. Int J Cardiol 4: 53, 1983
3. Kjekshus JK, Gr0ttum P: Modification of acute myocardial infarction by intravenous beta-pyridylcarbinol. In Hjalmarson A, Wilhelmsen L, editors: Proceedings of a conference on acute and long
term medical management of myocardial ischemia, Copenhagen,
September 8-9, 1977. M0lndal, 1978, Astra, p 373
4. Kronenberg MW, Hodges M, Akiyama T, Roberts DL, Ehrich
DA, Biddle TL, Yu PN: ST-segment variations after acute myocardial infarction. Relationship to clinical status. Circulation 54: 756,
1976
5. Akiyama T, Hodges M, Biddle TL, Zawrotny B, Vangellow C:
Measurements of ST segment elevation in acute myocardial infarction in man. Comparison of a precordial mapping technique and the
Frank vector system. Am J Cardiol 36: 155, 1975
1011
SEDERHOLM et al.
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
6. Maroko PR, Kjekshus JK, Sobel BE, Watanabe T, Covell JW,
Ross J Jr, Braunwald E: Factors influencing infarct size following
experimental coronary artery occlusions. Circulation 43: 67, 1971
7. Kjekshus JK, Maroko PR, Sobel BE: Distribution of myocardial
injury and its relation to epicardial ST-segment changes after coronary artery occlusion in the dog. Cardiovasc Res 6: 490, 1972
8. Abildskov JA, Boyle RS: Further studies of the electrocardiographic effects of experimental myocardial lesions. Am Heart J 69:
49, 1965
9. Bayley RH: Biophysical principles of electrocardiography. New
York, 1958, Paul B. Hoeber Inc
10. Nelson CV, Hodgkin BC, Bonner RA, Angelakos ET: The difference vector: assessment of effects of changes or interventions. Am
Heart J 95: 220, 1978
11. Wickline S, McNamara J: Vectorcardiographic quantification of
infarct size in baboons. Circulation 57: 910, 1978
12. Flowers N, Hand C, Sridharan MR, Horan L, Sohi GS: Surface
reflections of cardiac exitation and the assessment of infarct volume in dogs. Circ Res 43: 406, 1978
13. Hillis LD, Askenazi J, Braunwald E, Radvany P, Muller JE, Fishbein MC, Maroko PR: Use of changes in epicardial QRS complex
to assess interventions which modify the extent of myocardial
necrosis following coronary artery occlusion. Circulation 54: 591,
1976
14. H0rder M, Magid E, Pitkanen E, Harkonen M, Str0mme JH,
Theodorsen L, Gerhardt W, Waldenstr0m J: Recommended method for the determination of creatine kinase in blood modified by the
inclusion of EDTA. Sand J Clin Lab Invest 39: 1, 1979
15. Frank E: Accurate, clinically practical system for spatial vectorcardiography. Circ Res 13: 737, 1956
16. Shell WE, Kjekshus JK, Sobel BE: Quantitative assessment of the
extent of myocardial infarction in the conscious dog by means of
analysis of serial changes in serum creatine phosphokinase activity.
J Clin Invest 50: 2614, 1971
17. Bleifeld W, Mathey D, Hanrath P, Buss H, Effert S: Infarct size
estimated from serial serum creatine phosphokinase in relation to
left ventricular hemodynamics. Circulation 55: 303, 1977
18. Grande P, Fisher Hansen B, Christiansen C, Naestoft J: Acute
myocardial infarct size estimated by serum CK-MB determinations: clinical accuracy and prognostic relevance utilizing a practical modification of the isoenzyme approach. Am Heart J 101: 582,
1981
19. Schuster EH, Kallman C, Bulkley BH: Sizing human myocardial
infarcts from creatine kinase curves: The effects of reperfusion.
Circulation 62 (suppl III): 111-216, 1980 (abst)
20. Roberts R, Henry PD, Sobel BE: An improved basis for enzymatic
estimation of infarct size. Circulation 52: 713, 1975
21. Cairms JA, Missirlis E, Fallen EL: Myocardial infarction size from
serial CPK: variability of CPK serum entry ratio with size and
model of infarction. Circulation 58: 1143, 1978
22. Cairms JA, Klassen GA: The effect of propranolol on canine myocardial CPK distribution space and rate of disappearance. Circulation 56: 284, 1977
23. Sobel BE, Kjekshus JK, Roberts R: Enzymatic estimation of infarct size. In Hearse DJ, de Leiris J, editors: Enzymes in cardiology: diagnosis and research. New York, 1979, John Wiley and
Sons, pp 257-289
24. Maroko PR, Libby P, Covell JW, Sobel BE, Ross J Jr, Braunwald
E: Precordial ST segment elevation mapping: an atraumatic method
1012
for assessing alterations in the extent of myocardial ischemic injury. Am J Cardiol 29: 223, 1972
25. Flowers NC, Johnsson JC, Horan LG: Effect of VCG sensitivity to
dipole content in detecting infarctional changes. J Electrocardiol 5:
211, 1972
26. Mailloux GE, Gulrajani RM: Theoretical evaluation of the McFee
and Frank vectorcardiographic lead system using a numerical inhomogeneous torso model. IEEE Trans Biomed Eng 29: 322, 1982
27. Grant RP: Peri-infarction block. Prog Cardiovasc Dis 2: 237, 1959
28. Ribeiro LGT, Louie EK, Hillis D, Davis MA, Maroko PR: Early
augmentation of R wave voltage after coronary artery occlusion: a
useful index of myocardial injury. J Electrocardiol 12: 89, 1979
29. Samson WE, Scher AM: Mechanism of ST-segment alterations
during acute myocardial injury. Circ Res 8: 780, 1960
30. Madias JE: The earliest electrocardiographic sign of acute transmural myocardial infarction. J Electrocardiol 10: 193, 1977
31. Kjekshus JK, Mohr B, Gr0ttum P: Infarct evolution determined by
temporal changes of QRS infarct vectors. Trans Eur Soc Cardiol 1:
62, 1979 (abst)
32. Cowan MJ, Reichenbach DD, Bruce RA, Fisher L: Estimation of
myocardial infarct size by digital computer analysis of the VCG. J
Electrocardiol 15: 307, 1982
33. Ideker RE, Wagner GS, Ruth WK, Alonso DR, Bishop SP, Bloor
CM, Fallon JT, Gottlieb GJ, Hackel DB, Phillips HR, Reimer KA,
Roark SF, Rogers WJ, Savage RM, White RD, Selvester RII:
Evaluation of a QRS scoring system for estimating myocardial
infarct size. II. Correlation with quantitative anatomic findings for
anterior infarcts. Am J Cardiol 49: 1604, 1982
34. Roark SF, Ideker RE, Wagner GS, Alonso DR, Bishop SP, Bloor
CM, Bramlet DA, Edwards JE, Fallon JT, Gottlieb GJ, Hackel
DB, Phillips HR, Reimer KA, Rogers WJ, Ruth WK, Savage RM,
White RD, Selvester RH: Evaluation of a QRS scoring system for
estimating myocardial infarct size. III. Correlation with quantitative anatomic findings for inferior infarcts. Am J Cardiol 51: 382,
1983
35. Wikswo J Jr, Gundersen S, Murphy A, Dawson A, Smith R:
Sequential QRS vector subtractions in acute myocardial infarction
in humans. Circ Res 49: 1055, 1981
36. Muller JE, Maroko PR, Braunwald E: Evaluation of precordial
electrocardiographic mapping as a mean of assessing changes in
myocardial injury. Circulation 52: 16, 1975
37. Yusuf S, Lopez R, Maddison A, Maw P, Ray N, McMillan S,
Sleight P: Value of electrocardiogram in predicting and estimating
infarct size in man. Br Heart J 42: 286, 1979
38. Henning H, Hardarson T, Francis G, O'Rourke RA, Ryan W, Ross
J Jr: Approach to the estimation of myocardial infarct size by
analysis of precordial ST-segment and R-wave maps. Am J Cardiol
41: 1, 1978
39. Holland RP, Brooks H: Precordial and epicardial surface potentials
during myocardial ischemia in the pig. A theoretical and experimental analysis of the TQ and ST-segment. Circ Res 37: 471, 1975
40. Hutchins GM, Bulkley BH: Infarct expansion versus extension:
Two different complications of acute myocardial infarction. Am J
Cardiol 41: 1127, 1978
41. Battler A, Froelicher VF, Gallagher KP, Kennada T, McKown D,
Kemper WS, Ross J Jr: Effects of changes in ventricular size on
regional and surface QRS amplitudes in the conscious dog. Circulation 62: 174, 1980
42. Marmor A, Sobel BE, Roberts R: Factors presaging early recurrent
myocardial infarction ("extension"). Am J Cardiol 48: 603, 1981
CIRCULATION
Quantitative assessment of myocardial ischemia and necrosis by continuous
vectorcardiography and measurement of creatine kinase release in patients.
M Sederholm, P Grøttum, L Erhardt and J Kjekshus
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2016
Circulation. 1983;68:1006-1012
doi: 10.1161/01.CIR.68.5.1006
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1983 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/68/5/1006
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/