slides - UCSF CME
advertisement

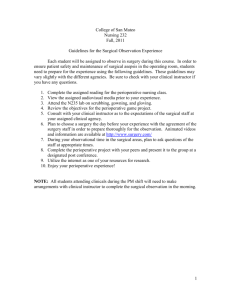
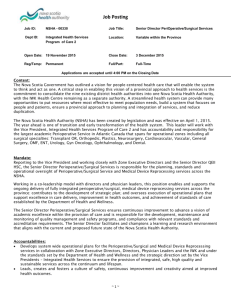
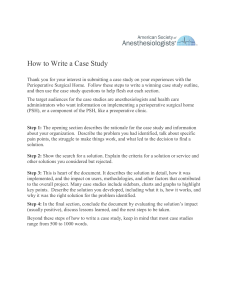
THE PERIOPERATIVE SURGICAL HOME: WHY EVERYONE WINS Thomas R. Vetter, MD, MPH Maurice S. Albin Professor of Anesthesiology and Perioperative Medicine Professor of Gerontology, Geriatrics and Palliative Care Professor of Pediatrics Professor of Health Care Organization and Policy University of Alabama at Birmingham © Thomas R. Vetter 2015 MY PRESENTATION OBJECTIVES Describe the details of a prototypic Perioperative Surgical Home model Foster the conversation about the various topics central to the rationale, implementation, and validation of a Perioperative Surgical Home model My Conflicts of Interest: I have nothing to disclose. WHAT IS VALUE IN HEALTH CARE? HEALTH CARE VALUE EQUATION QUALITY SAFETY SATISFACTION VALUE $ TOTAL COSTS OF CARE “Burning Platform” of Changing Reimbursement Models Goal of the Department of Health and Human Services is to increase the proportion of federal payments related to value to 30% by the end of 2016 and to 50% by the end 2018. Porter ME. What is Value in Health Care? N Engl J Med 2010;363:2477-81. Vetter TR, Jones KA: Perioperative Surgical Home: Perspective II. In Value-Based Care, Anesthesiology Clinics (Fleisher LA, Guest Editor) 2015 [In press]. 1 THE DRIVERS OF VALUE-BASED HEALTHCARE Centers for Medicare & Medicaid Services (CMS) Accountable Care Organizations (ACOs) Pay‐for‐Performance and Quality Incentives Population Health Management Commercial Insurers Regional Care Organizations (RCOs) Specialty Care Programs Large Employers Centers of Excellence Medicaid Opt‐Out States Increased Value Patients Greater Out‐of‐ Pocket Expenses Vetter TR, Jones KA: Perioperative Surgical Home: Perspective II. In Value-Based Care, Anesthesiology Clinics (Fleisher LA, Guest Editor) 2015 [In press]. MEDICARE ACCESS AND CHIP REAUTHORIZATION ACT OF 2015 (MACRA) • Eliminated the Sustainable Growth Rate (SGR) formula • Consolidates and expands pay-for-performance (P4P) incentives within the fee-for-service system, creating the new Merit-Based Incentive Payment System (MIPS) that combines the current: – Physician Quality Reporting System (PQRS) – Value-Based Modifier (VBM) – Electronic Health Record (EHR) Meaningful Use (MU) • Applies to physicians, nurse practitioners, clinical nurse specialists, physician assistants, and certified registered nurse anesthetists MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) FEE-FOR-SERVICE ADJUSTMENTS • Adjusts Medicare payments based on performance on a single budget-neutral payment beginning in 2019 • Losers Negative Adjustments to Payments – 2019: Up to ‒ 4% – 2020: Up to ‒ 5% – 2021: Up to ‒ 7% – 2022: Up to ‒ 9% • Winners Positive Adjustments to Payments – 2019: Up to + 12% – 2020: Up to + 15% – 2021: Up to + 21% – 2022: Up to + 27% 2 THE IOM’S CEO CHECKLIST FOR HIGHVALUE HEALTH CARE: 5 SELECTED ITEMS • Infrastructure Fundamentals Information technology best practices: automated, reliable information to and from the point of care Evidence protocols: effective, efficient, and consistent care • Care Delivery Priorities Integrated care: right care, right setting, right providers, right teamwork Shared decision making: patient–clinician collaboration on care plans Targeted services: tailored community and clinic interventions for resource-intensive patients Cosgrove D, Fisher M, Gabow P, Gottlieb G, Halvorson G, James B, Kaplan G, Perlin J, Petzel R, Steele G, Toussaint J. A CEO Checklist for High-Value Health Care. Washington, DC: Institute of Medicine, 2012. INCREASING THE VALUE OF SURGICAL CARE Perioperative Surgical Home must translate, implement, sustain, and document quality, safety, and satisfaction improvement and cost reduction strategies: – Decrease practice variability – including unit of service cost for anesthesia services – Increase practice efficiency – including the maximum use of advanced practice nurses – Patient risk stratification and mitigation – including open dialogue about futile surgery – Perioperative optimization of patient co-morbidities – including optimal timing of surgery – Patient education and counseling – including “What can I do to improve the outcomes that are most important to me?” Vetter TR, Jones KA: Perioperative Surgical Home: Perspective II. In Value-Based Care, Anesthesiology Clinics 2015 [In press]. ONE DEFINITION OF THE PERIOPERATIVE SURGICAL HOME Patient-centered, institution-led, interdisciplinary, team-based, coordinated, standardized care model Guides the patient through the entire surgical continuum, from the decision for surgery to posthospital discharge care Seeks to enhance surgical experience and outcomes and to add measurable value to the highest cost segment of healthcare Multiple effective variants based upon institutional infrastructure, resources, and internal/external forces Vetter TR, Goeddel LA, Boudreaux AM, Hunt TR, Jones KA, Pittet JF. The Perioperative Surgical Home: How Can It Make the Case so Everyone Wins? BMC Anesthesiol 2013 Mar 14;13:6. 3 IDEALLY, A HIGHLY COLLABORATIVE AND THUS SYMBIOTIC RELATIONSHIP… American Society of Anesthesiologists American College of Surgeons Society of Hospital Medicine American College of Physicians American Academy of Family Physicians Anesthesiologist and CRNA Surgeon Hospitalist THE PATIENT Can we all play nice in the sandbox? and Intensivist Let’s hope so… For everyone‘s sake Primary Care Physician and Medical Specialists American Association of Nurse Practitioners American Association of Nurse Anesthetists ROBUST INTEGRATION OF THE ENTIRE PERIOPERATIVE CONTINUUM OF CARE Preoperative Phase Intraoperative Phase Postoperative Phase PostDischarge Phase Three Key Design Elements 1. Strong Patient and Family Centeredness and Shared Decision-Making 2. Robust Team Member Collaboration Across the Continuum 3. Seamless Health Information Exchange and Shared Care Plans Service Line or Procedure‐Specific Integrated Care Pathways Enhanced Recovery after Surgery (ERAS®) Protocols Perioperative Risk Optimization and Management Planning Tools Reduce Practice Variation, Optimize Patient Outcomes, Maximize Value 4 INTEGRATED CARE PATHWAY (ICP) • ICP = Task-orientated care plan that details all the essential steps or elements in the care of all patients undergoing a specific surgical procedure • Toyota Production System (TPS) approach to making cars and LEAN Six Sigma methodology are rigorously applied to surgical patient care. • Collect and analyze data to highlight and address any lack of process standardization and resulting inefficiencies, rework, and waste Kain ZN, Vakharia S, Garson L, Engwall S, Schwarzkopf R, Gupta R, Cannesson M. The Perioperative Surgical Home as a Future Perioperative Practice Model. Anesth Analg 2014 May;118(5):1126-30. EXAMPLES OF INTEGRATED CARE PATHWAYS Campbell H, Hotchkiss R, Bradshaw N, Porteous M. Integrated Care Pathways. BMJ. 1998 Jan 10;316(7125):133-7. PERIOPERATIVE RISK OPTIMIZATION AND MANAGEMENT PLANNING TOOL • Conventional national clinical practice guidelines can have limited local clinician buy-in and adoption • PROMPT™ local clinician-designed/driven approach: – Accommodates patients' individual differences – Respects and seeks local providers' clinical acumen – Keeps pace with the rapid growth of medical knowledge • PROMPT™ is not prescriptive “cook-book” medicine but a local best practices-based decision support tool • Some examples of PROMPTs (55+ in pipeline at UAB): – PONV, postoperative delirium; patient-centered blood management; perioperative anticoagulant therapy Vetter TR, Jones KA: Perioperative Surgical Home: Perspective II. In Value-Based Care, Anesthesiology Clinics (Fleisher LA, Guest Editor) 2015 [In press]. Vetter TR, Barman J, Boudreaux AM, Jones KA: Developing, Prioritizing and Implementing the Use of the Perioperative Risk Optimization and Management Planning Tool (PROMPT™). Anesth Analg Case Management Report 2015 [In preparation]. 5 PERIOPERATIVE PERSONALIZED PATIENT CARE MATRIX PROMPT 1 PROMPT 2 PROMPT 3 • ICP Element 1 • ICP Element 2 • ICP Element 3 • ICP Element 4 Preoperative Phase PROMPT 1 PROMPT 2 PROMPT 3 Intraoperative Phase • ICP Element 5 • ICP Element 6 • ICP Element 7 • ICP Element 8 • ICP Element 9 • ICP Element 10 • ICP Element 11 • ICP Element 12 Postoperative Phase Post‐Discharge Phase • ICP Element 13 • ICP Element 14 • ICP Element 15 • ICP Element 16 PROMPT 1 PROMPT 2 PROMPT 3 PROMPT 1 PROMPT 2 PROMPT 3 In this example, the Integrated Care Pathway (ICP) (e.g., for pancreatectomy) contains 16 specific, standardized elements, and the patient’s co-morbidities warrant 3 Perioperative Risk Optimization and Management Planning Tools (PROMPT 1, PROMPT 2, PROMPT 3) (e.g., for preoperative anemia, diabetes mellitus, and postoperative cognitive dysfunction/delirium) Vetter TR, Boudreaux AM, Jones KA, Hunter JM Jr, Pittet JF. The Perioperative Surgical Home: How Anesthesiology Can Collaboratively Achieve and Leverage the Triple Aim in Health Care. Anesth Analg. 2014 May;118(5):1131-6. WHAT PROBLEMS ARE WE TRYING TO FIX? • Incomplete & inconsistent patient preparation for surgery • Incomplete documentation of patient co-morbidities • Incomplete & inaccurate medication reconciliation • Irregular & inefficient patient scheduling and throughput • Persistent case delays and cancellations • Continued failure to rescue and never events • Greater than desired morbidity and mortality • Higher than desired hospital readmission rates • Difficulty with compliance with key performance measures • Lower than desired patient and family satisfaction • Excessive and variable cost per episode of surgical care BY THE WAY, DOCTOR…WHAT IS YOUR RISK-ADJUSTED MORTALITY? • Observed-to-expected (O:E) mortality ratio is an increasingly important health care quality metric. • Allows quantification/comparison of survival outcomes among different providers/institutions • Hospital revenue will be directly affected by its risk-adjusted mortality rate. • As hospital performance data circulate ever more widely to the public, the O:E ratio is quite prominent. Shine D. Risk-Adjusted Mortality: Problems and Possibilities. Computational and Mathematical Methods in Medicine 2012, 2012:5. 6 UHC TOP PERFORMERS (123 MEMBERS) Rank October 2014 UHC Quality Leadership Awards October 2013 UHC Quality Leadership Awards 1 NYU Langone Medical Center NYU Langone Medical Center 2 Emory University Hospital Mayo Clinic – Rochester 3 Emory Hospital Midtown Ohio State University Wexner Medical Center 4 Mayo Clinic – Rochester Beaumont Health System, Royal Oak, MI 5 Rush University Medical Center Rush University Medical Center 6 Beaumont Health System, Royal Oak, MI University of Utah Health Care 7 Fletcher Allen Health Center, Vermont Emory University Hospital 8 Ohio State University Wexner Medical Center University of Kansas Medical Center, Kansas City, KS 9 University of Utah Health Care University of Missouri Health Care 10 University of Colorado Hospital Cleveland Clinic 11 Houston Methodist Hospital 12 Memorial Hermann-Texas Medical Center https://www.uhc.edu/news/Twelve-academic-medical-centers-receive THE AGING UNITED STATES POPULATION “THE SILVER TSUNAMI” Number of Americans > 65 years (millions) 80 70 60 50 54.8 25% of all Medicare spending occurs in the last year of life 40 25.5 30 31.2 40.3 35 16.6 20 10 72.1 An estimated 32% of older Americans undergo surgery in the year before their death…and 9 4.9 3.1 0 1900 1920 1940 1960 1980 1990 2000 2010 2020 2030 4.1% 13.1% 19.3% Administration on Aging: A Profile of Older Americans: 2011. Washington, DC: U.S. Department of Health and Human Services; 2011: 1-16. Kwok AC, Semel ME, Lipsitz SR, Bader AM, Barnato AE, Gawande AA, Jha AK. The Intensity and Variation of Surgical Care at the End of Life: A Retrospective Cohort Study. The Lancet 2011;378:1408-13. PROJECTED RISE IN CHRONIC DISEASE BURDEN BETWEEN 2003 AND 2023 Percentage Increase in Prevalence 70% 62% 54% 60% 56% 50% By 2020, 157 million Americans will have one chronic disease, and 81 million will have multiple such conditions. 41% 39% 40% 31% 29% 30% 20% 10% 0% Cancers Mental Disorders Diabetes Heart Disease Hypertension Pulmonary Conditions Stroke Versus a Projected 19% Population Growth DeVol R., Bedroussian A. An Unhealthy America: The Economic Burden of Chronic Disease. Santa Monica, CA: Miliken Institute; 2007: 1-38. 7 ANESTHESIA-RELATED SAFETY • Modern death rate from complications/adverse events associated with anesthesia has decreased by 97%: – 64 deaths per 100,000 anesthetics in late 1940’s – By 2005, only 0.82 deaths per 100,000 anesthetics • Both increased age and prevalence of chronic diseases have been independently associated with increased surgical mortality. Maintaining or improving on the 20th century gains in anesthesia-related mortality will be challenging. • The Perioperative Surgical Home offers the needed more comprehensive and coordinated approach to the management of our older and sicker surgical patients. Li G, Warner M, Lang BH, Huang L, Sun LS. Epidemiology of Anesthesia-Related Mortality in the United States, 1999–2005. Anesthesiology 2009, 110(4):759-765. Turrentine FE, Wang H, Simpson VB, Jones RS. Surgical Risk Factors, Morbidity, and Mortality in Elderly Patients. J Am Coll Surg 2006, 203(6):865-877. WHEREVER YOU GO – THERE YOU ARE Surgical death rates vary widely across US hospitals ─ from 3.5% in very-low-mortality hospitals to 6.9% in very-high-mortality hospitals. • Despite similar rates of overall complications and of major complications ─ • MORTALITY in patients with major complications was significantly greater in hospitals with very high overall mortality compared with those with very low overall mortality. BUT WHY? Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in Hospital Mortality Associated with Inpatient Surgery. N Engl J Med 2009, 361(14):1368-1375. FAILURE-TO-RESCUE (FTR) • Silber et al. (1992) = Hospital deaths after adverse occurrences such as postsurgical complications • Contributors to FTR have been broadly categorized: 1) Lack of a timely response prompt recognition of the complication 2) Lack of an appropriate response correct management and treatment • An abundance of retrospective data supports that adverse events in general ward (non-ICU) patients are preceded by a significant period — on the order of hours — of physiologic deterioration • Most common causes in the surgical population 1) Respiratory complications (38%) 2) Infection complications (28%) 3) Cardiovascular complications (23%) Taenzer, AH, Pyke JB, McGrath SP. A Review of Current and Emerging Approaches to Address Failure-to-Rescue. Anesthesiology 2011 Aug,115(2):421-431. Helling TS, Martin LC, Martin M, et al. Failure Events in Transition of Care for Surgical Patients. J Am Coll Surg 2014 Apr;218(4):723-31. 8 COMPLICATIONS, FAILURE TO RESCUE AND MORTALITY RATES Michigan Surgical Collaborative for Outcomes Research and Evaluation (M-SCORE) • Medicare Provider Analysis and Review (MEDPAR) data from 2005 and 2006 for pancreatectomy, esophagectomy, AAA repair, CABG, AVR, and MVR • 8 major postoperative complications: pulmonary failure, pneumonia, myocardial infarction, deep venous thrombosis/ pulmonary embolism, acute renal failure, hemorrhage, surgical site infection, and gastrointestinal bleeding • Failure to rescue (FTR) was defined as death in a patient with one or more of these 8 defined complications. Ghaferi AA, Birkmeyer JD, Dimick JB. Complications, Failure to Rescue, and Mortality with Major Inpatient Surgery in Medicare Patients. Ann Surg 2009 Jun, 250(6):1029-1034. Ghaferi AA, Birkmeyer JD, Dimick JB. Hospital Volume and Failure to Rescue with High-Risk Surgery. Med Care 2011 Dec;49(12):1076-81. COMPLICATIONS, FAILURE TO RESCUE AND MORTALITY RATES 40% 35% 36.4% 32.7% 30% Failure to Rescue Rates (subgroups) 5.7% versus 56.9% for esophagectomy 4.0% versus 50.8% for pancreatectomy 25% 20% 16.7% 15% 10% 6.8% 5% 8.0% 3.0% 0% Complications Failure to Rescue Mortality Best Hospital Mortality Worst Hospital Mortality NNH = 20 for MORTALITY at worst versus best hospitals Ghaferi AA, Birkmeyer JD, Dimick JB. Complications, Failure to Rescue, and Mortality with Major Inpatient Surgery in Medicare Patients. Ann Surg 2009, 250(6):1029-1034. Ghaferi AA, Birkmeyer JD, Dimick JB. Hospital Volume and Failure to Rescue with High-Risk Surgery. Med Care 2011 Dec;49(12):1076-81. PREOPERATIVE TARGETS TO PREVENT FTR AND IMPROVE SURGICAL MORTALITY • “Failure to rescue is an emerging quality metric.” • 2007 to 2011 Nationwide Inpatient Sample • Lowest mortality quintile: N = 282 hospitals; 56,893 patients • Highest mortality quintile: N = 282 hospitals; 45,784 patients • Small bowel resection, pancreatectomy, colorectal resection, open abdominal aortic aneurysm repair, lower extremity arterial bypass, and nephrectomy • FTR population (+) Qualifying postoperative complication • High-mortality risk population High risk predicted via logistic regression model based upon age & co-morbidities Hyder JA, Wakeam E, Adler JT, DeBord Smith A, Lipsitz SR, Nguyen LL. Comparing Preoperative Targets to Failure-to-Rescue for Surgical Mortality Improvement. J Am Coll Surg 2015 Jun;220(6):1096-106. 9 PREOPERATIVE TARGETS TO PREVENT FTR AND IMPROVE SURGICAL MORTALITY FTR: 20.2% vs 22.4% p = 0.002 Variation in mortality rates across lowest-mortality hospitals (gray bars) and highest-mortality hospitals (black bars) 1) FTR population 18.9% vs 7.8%, p < 0.0001, NNH = 9 2) High-risk 20.2% vs 7.5%, p < 0.0001, NNH = 8 3) Emergency surgery 11.1% vs 4.1%, p < 0.0001, NNH = 14 4) Elderly (> 75 years) 10.7% vs 3.7%, p < 0.0001, NNH = 14 Postoperative FTR = A potential way to reduce mortality Hyder JA, Wakeam E, Adler JT, DeBord Smith A, Lipsitz SR, Nguyen LL. Comparing Preoperative Targets to Failure-to-Rescue for Surgical Mortality Improvement. J Am Coll Surg 2015 Jun;220(6):1096-106. ASSOCIATION BETWEEN POSTOPERATIVE TROPONIN LEVELS AND 30-DAY MORTALITY AMONG PATIENTS UNDERGOING NONCARDIAC SURGERY • 15,133 patients; sequential 4th generation troponin T levels at 6-12 hours postoperatively, POD 1, 2, 3 peak value of… • TnT of 0.02 ng/mL: – 4% mortality with adjusted hazard ratio [aHR] = 2.41 • TnT of 0.03 to 0.29 ng/mL: – 9.3% mortality & aHR = 5.00 • TnT of 0.30 ng/mL or greater: – 16.9% mortality & aHR = 10.48 Myocardial Injury after Non-Cardiac Surgery (MINS) How do we risk stratify patients and prevent MINS? Kaplan-Meier Estimates of 30-Day Mortality Based on Peak Troponin T Values Association between Postoperative Troponin Levels and 30-day Mortality among Patients Undergoing Noncardiac Surgery. Vascular Events In Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators. JAMA. 2012 Jun 6;307(21):2295-304. PYRAMID OF PRACTICE CHANGE Practice Change 3 BUILDING BLOCKS Decision Support Analytics Informatics (Data) Vetter TR, Jones KA: Perioperative Surgical Home: Perspective II. In Value-Based Care, Anesthesiology Clinics 2015 [In press]. 10 PERIOPERATIVE MEDICAL INFORMATICS Perioperative epidemiology is an area of growth – ultimately enabling the perioperative care team to translate precise real‐time information into improved outcomes. Proposed Model of the Flow of Data Throughout the Perioperative Period Outcomes Decision Support Bartels K, Barbeito A, Mackensen GB. The Anesthesia Team of the Future. Curr Opin Anaesthesiol 2011, 24(6):687-692. MEMORIAL SLOAN KETTERING CANCER CENTER DIRECTOR OF PERIOPERATIVE INFORMATICS AND INNOVATION • The Director of Perioperative Informatics and Innovation (“Director”) will be a key leader in the transformation of care across the pre-operative, intra-operative, and post-operative care, leading a team in the implementation of systems across the new 14 story Josie Robertson Surgery Center. • The Director will be a leader in the development of system-wide analytics initiatives that will transform care for MSK patients. • The qualified candidate will have experience overseeing the design, build and implementation of clinical systems combining informatics and clinical process, data analytics and the ability to optimize the interoperability of clinical information systems to enhance patient safety and clinical outcomes. www.wittkieffer.com/position/memorial-sloankettering-cancer-center/director-of-perioperative-informatics-and-innovation/12005 WHAT’S IN IT FOR THE SURGEON? • The Perioperative Surgical Home is not intended to replace the surgeon’s primary patient care responsibility… • Rather aligns and leverages the talents and abilities of the entire perioperative care team in the service of the patient • From a surgeon’s perspective, the Perioperative Surgical Home model can create value in four primary ways: 1) Takes advantage of the well-established relationships among the surgeon/anesthesiologist/intensivist/hospitalist 2) Expands upon the existing pre-, intra-, and post-operative relationship between the anesthesiologist and the patient 3) Increases the quality of surgical care by increasing the scope and depth of the perioperative team 4) Improves the surgeon’s efficiency and productivity Vetter TR, Goeddel LA, Boudreaux AM, Hunt TR, Jones KA, Pittet JF. The Perioperative Surgical Home: How Can It Make the Case so Everyone Wins? BMC Anesthesiol 2013 Mar 14;13:6. 11 ENHANCED RECOVERY AFTER SURGERY (ERAS) • Pioneered in Scandinavia and UK by surgeons • Evidence-based “fast-track” approach to surgery • Multifaceted perioperative care pathway designed to attenuate the stress response during all three phases of the perioperative period and the patient’s surgical journey • Facilitate the maintenance of bodily composition and organ function and to achieve early recovery Varadhan KK, Lobo DN, Ljungqvist O. Enhanced Recovery After Surgery: The Future of Improving Surgical Care. Crit Care Clin 2010;26(3):527-47. Ljungqvist O. ERAS-Enhanced Recovery After Surgery: Moving Evidence-Based Perioperative Care to Practice. J Parenter Enteral Nutr 2014;38(5):559-66. ENHANCED RECOVERY AFTER SURGERY (ERAS) • Preadmission patient counseling and education, including anxiety reduction techniques • Prehabilitation of nutritional (protein) status, cardiopulmonary reserve, and muscle strength • No prolonged fasting • No or selective bowel preparation • Oral fluid and carbohydrate loading immediately prior to surgery • Antibiotic and thromboembolism prophylaxis • Oral adjuvant analgesics but no sedative premedication • Single subarachnoid dose of a moderately hydrophilic opioid for laparoscopic surgery • Short‐acting anesthetic agents and medications • No surgical drains • Avoidance of salt and water overload • Goal‐directed fluid therapy • Restrictive blood transfusion triggers • Maintenance of normothermia via body warmer and intravenous fluid warmer • Anesthetic depth monitoring in patients at risk for delirium and cognitive dysfunction • Mid‐thoracic epidural analgesia with local anesthetic but no opioid for open laparotomy • No nasogastric tube • Prevention of postoperative nausea and vomiting • Avoidance of salt and water overload • Restrictive blood transfusion triggers • Early oral nutrition • Early mobilization • Non‐opioid intravenous and oral analgesics Hunter JM, Vetter TR: Major General Surgery in the Elderly Patient. In Barnett SR (Ed). Perioperative Care of the Elderly Patient. Cambridge, UK: Cambridge University Press, 2015/2016 [In press]; www.erassociety.org/ PREOPERATIVE PREHABILITATION • “Prehabilitation” is an intervention to enhance functional capacity in anticipation of a forthcoming physiological stressor. • Preoperative prehabilitation aims to enhance functional capacity preoperatively for better tolerance of surgery and to facilitate recovery. • Also accurately predict and then reduce need for prolonged postoperative, post-discharge institutional rehabilitation and convalescence Carli F, Charlebois P, Stein B, Feldman L, Zavorsky G, Kim DJ et al. Randomized Clinical Trial of Prehabilitation in Colorectal Surgery. Br J Surg 2010;97(8):1187-97. Li C, Carli F, Lee L, Charlebois P, Stein B, Liberman AS et al. Impact of a Trimodal Prehabilitation Program on Functional Recovery After Colorectal Cancer Surgery: A Pilot Study. Surg Endosc 2013;27(4):1072-82. Biffl WL, Biffl SE. Rehabilitation of the Geriatric Surgical Patient: Predicting Needs and Optimizing Outcomes. Surg Clin North Am 2015;95(1):173-90. 12 PREOPERATIVE TRIMODAL PREHABILITATION • Home-based, approximately one month program: 1) Moderate aerobic and resistance exercises 2) Nutritional counseling + whey protein supplementation 3) Relaxation exercises (anxiety reduction) P = 0.016 But no changes were observed in SF-36 or Hospital Anxiety and Depression Scale (HADS) scores and post-operative complication rates and the hospital length of stay were similar in the prehabilitation versus the postoperative rehabilitation patients. Li C, Carli F, Lee L, Charlebois P, Stein B, Liberman AS et al. Impact of a Trimodal Prehabilitation Program on Functional Recovery After Colorectal Cancer Surgery: A Pilot Study. Surg Endosc 2013;27(4):1072-82. Gillis C, Li C, Lee L, Awasthi R, Augustin B, Gamsa A et al. Prehabilitation Versus Rehabilitation: A Randomized Control Trial in Patients Undergoing Colorectal Resection for Cancer. Anesthesiology 2014 May;121(5):937-47. ANESTHESIOLOGY AND OUR NEEDED MORE COMPETITIVE STRATEGY • Anesthesiology is facing strong economic pressures that require a broader competitive strategy. • Looming austere, constrained economic landscape and need to provide a more effective and efficient product • To strengthen the future viability of our specialty: Urgent need for anesthesiologists to challenge our current, historically successful business model and our assumptions about the market forces, mission, and core competencies of our specialty Gross WL, Gold B. Anesthesiology and Competitive Strategy. Anesth Clin 2009, 27(1):167-174. Seim AR, Sandberg WS. Shaping the Operating Room and Perioperative Systems of the Future: Innovating for Improved Competitiveness. Curr Opin Anaesth 2010, 23(6):765-771. Martin J, Cheng D. Role of the Anesthesiologist in the Wider Governance of Healthcare and Health Economics. Can J Anaesth 2013;60:918-28 THE ANESTHESIOLOGIST AND PERIOPERATIVE MEDICINE • Necessary to expand the core knowledge, skills, and experience expected of the anesthesiologist • Need to view the “Perioperative Medicine” as an expansion of the specialty, rather than an abdication of the traditional and still vital intraoperative role • Not all anesthesiologists will be able or willing to play a role in this new activity. • But just as with the seminal development within anesthesia of the subspecialties of critical care medicine and pain medicine, a subset will need to do so and be supported by colleagues in their efforts Van Aken H, Thomson D., Smith G, Zorab J. 150 Years of Anaesthesia -- A Long Way to Perioperative Medicine: The Modern Role of the Anaesthesiologist. Eur J Anaesthesiol 1998, 15(5):520-523. Grocott MPW, Pearse RM. Perioperative Medicine: The Future of Anaesthesia? Br J of Anaesth 2012, 108(5):723-726. 13 UAB PREOPERATIVE ASSESSMENT, CONSULTATION, AND TREATMENT CLINIC • Semantic and clinical evolution has occurred at UAB – PAT = Pre-Admission Testing (1990) – PAC = Pre-Anesthesia Assessment Clinic (1995) – PACT Clinic = Preoperative Assessment, Consultation, and Treatment Clinic (2010) • Road trips to Johns Hopkins, Brigham and Women’s, Cleveland Clinic (Cleveland), and Mayo Clinic (Rochester) • PACT Clinic moniker intentionally chosen to communicate our comprehensive scope of practice and services • Frankly, we continue to grow into its full potential… VALUE STREAM MAPPING: PSH PREOPERATIVE PROCESS ACTIVITY MAPPING • Preoperative patient risk screening tool • Formal E&M code-based preoperative consultation • Robust patient-centered shared decision-making • Therapeutic interventions • Post-discharge care planning before surgery • Preoperative clearance Vetter TR, Jones KA: Perioperative Surgical Home: Perspective II. In Value-Based Care, Anesthesiology Clinics 2015 [In press]. A COMPREHENSIVE REVIEW OF THE PERIOPERATIVE SURGICAL HOME LITERATURE “The PSH model may have significant implications for policymakers, payers, administrators, clinicians, and patients. The potential for policy-relevant cost savings and quality improvement is apparent across the perioperative continuum of care, especially for integrated care organizations, bundled payment, and value-based purchasing.” Kash BA, Zhang Y, Cline KM, Menser T, Miller TR. The Perioperative Surgical Home (PSH): A Comprehensive Review of US and Non-US Studies Shows Predominantly Positive Quality and Cost Outcomes. Milbank Q 2014 Dec;92(4):796-821. 14 A COMPREHENSIVE REVIEW OF THE PERIOPERATIVE SURGICAL HOME LITERATURE • 152 peer-reviewed articles between 1980 and 2013 • History and evolution of PSH and PSH-like models • Summary of the results of studies of PSH elements in the United States and in other countries Phase of Perioperative Care Significantly Positive Cost & Efficiency Significantly Positive Clinical Outcomes Preoperative Initiatives 82% 82% Intraoperative Initiatives 77% 86% Postoperative Initiatives 75% 87% Kash BA, Zhang Y, Cline KM, Menser T, Miller TR. The Perioperative Surgical Home (PSH): A Comprehensive Review of US and Non-US Studies Shows Predominantly Positive Quality and Cost Outcomes. Milbank Q 2014 Dec;92(4):796-821. INTEGRATED CARE PATHWAYS • Task-orientated care plans that detail the essential steps or elements in the care of all patients on a specific service line or undergoing a specific surgical procedure • Lean or Six Sigma: Collect data to highlight and address any lack of process standardization and resulting inefficiencies, rework, and waste • UC Irvine Health “Total Joint Perioperative Surgical Home” Outcome LOS 30 Day RA Transfusion Complications Mortality SCIP UCI Health 3 days 0.7% 6.2% 0% 0% 100% Group Benchmark THA UCI THA Benchmark TKA UCI TKA Per Diem Cost $16,267 $9,952 $17,588 $10,042 Implementation of a Total Joint Replacement-Focused Perioperative Surgical Home: A Management Case Report. Garson L, Schwarzkopf R, Vakharia S, Alexander B, Stead S, Cannesson M, Kain Z. Anesth Analg. 2014 May;118(5):1081-9. Total joint Perioperative Surgical Home: An Observational Financial Review. Raphael DR, Cannesson M, Schwarzkopf R, Garson LM, Vakharia SB, Gupta R, Kain ZN. Perioper Med (Lond). 2014 Aug 27;3:6. FEW FINAL OBSERVATIONS… There is no limit to what can be accomplished if it doesn't matter who gets the credit. Ralph Waldo Emerson (1803 – 1882) Health care must be a business — But medicine remains an art and a science, and the successful practice of medicine is all about strong relationships with one’s patients and one’s colleagues. 15