External cephalic version for breech presentation at term (Review)
advertisement
")
External cephalic version for breech presentation at term
(Review)
Hofmeyr GJ, Kulier R
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2011, Issue 1
http://www.thecochranelibrary.com
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
TABLE OF CONTENTS
HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . .
BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . .
ACKNOWLEDGEMENTS
. . . . . . . . . . . . . . . . . . . . . . . . . . .
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . .
DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 External cephalic version at term, Outcome 1 Non-cephalic births. . . .
Analysis 1.2. Comparison 1 External cephalic version at term, Outcome 2 Caesarean section.
. . .
Analysis 1.3. Comparison 1 External cephalic version at term, Outcome 3 Apgar score < 7 at 1 minute.
Analysis 1.4. Comparison 1 External cephalic version at term, Outcome 4 Apgar score < 7 at 5 minutes.
Analysis 1.5. Comparison 1 External cephalic version at term, Outcome 5 Umbilical vein pH < 7.20. .
Analysis 1.6. Comparison 1 External cephalic version at term, Outcome 6 Neonatal admission. . . .
Analysis 1.7. Comparison 1 External cephalic version at term, Outcome 7 Perinatal death. . . . .
Analysis 1.8. Comparison 1 External cephalic version at term, Outcome 8 Enrolment-delivery interval.
APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . .
DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . .
SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . .
INDEX TERMS
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
1
1
2
2
3
3
5
7
7
8
8
8
11
19
19
20
20
21
21
22
22
23
23
24
24
24
25
25
25
i
[Intervention Review]
External cephalic version for breech presentation at term
G Justus Hofmeyr1 , Regina Kulier2
1 Department of Obstetrics and Gynaecology, East London Hospital Complex, University of the Witwatersrand, University of Fort
Hare, Eastern Cape Department of Health, East London, South Africa. 2 Geneva Foundation for Medical Education and Research,
Geneva, Switzerland
Contact address: G Justus Hofmeyr, Department of Obstetrics and Gynaecology, East London Hospital Complex, University of the
Witwatersrand, University of Fort Hare, Eastern Cape Department of Health, Frere and Cecilia Makiwane Hospitals, Private Bag X
9047, East London, Eastern Cape, 5200, South Africa. justhof@gmail.com.
Editorial group: Cochrane Pregnancy and Childbirth Group.
Publication status and date: New search for studies and content updated (no change to conclusions), published in Issue 1, 2011.
Review content assessed as up-to-date: 7 December 2010.
Citation: Hofmeyr GJ, Kulier R. External cephalic version for breech presentation at term. Cochrane Database of Systematic Reviews
1996, Issue 1. Art. No.: CD000083. DOI: 10.1002/14651858.CD000083.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACT
Background
Management of breech presentation is controversial, particularly in regard to manipulation of the position of the fetus by external
cephalic version (ECV). ECV may reduce the number of breech presentations and caesarean sections, but there also have been reports
of complications with the procedure.
Objectives
The objective of this review was to assess the effects of ECV at or near term on measures of pregnancy outcome. Methods of facilitating
ECV, and ECV before term are reviewed separately.
Search strategy
We searched the Cochrane Pregnancy and Childbirth Trials Register (September 2010), the Cochrane Central Register of Controlled
Trials (2010, Issue 3) and PubMed (1966 to September 2010).
Selection criteria
Randomised trials of ECV at or near term (with or without tocolysis) compared with no attempt at ECV in women with breech
presentation.
Data collection and analysis
Two reviewers assessed eligibility and trial quality, and extracted the data.
Main results
We included seven studies. The pooled data from these studies show a statistically significant and clinically meaningful reduction in
non-cephalic birth (seven trials, 1245 women; risk ratio (RR) 0.46, 95% confidence interval (CI) 0.31 to 0.66; and caesarean section
(seven trials, 1245 women; RR 0.63, 95% CI 0.44 to 0.90) when ECV was attempted. There were no significant differences in the
incidence of Apgar score ratings below seven at one minute (two trials, 108 women; RR 0.95, 95% CI 0.47 to 1.89) or five minutes
(four trials, 368 women; RR 0.76, 95% CI 0.32 to 1.77), low umbilical artery pH levels (one trial, 52 women; RR 0.65, 95% CI 0.17
to 2.44), neonatal admission (one trial, 52 women; RR 0.36, 95% CI 0.04 to 3.24), perinatal death (six trials, 1053 women; RR 0.34,
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
1
95% CI 0.05 to 2.12), nor time from enrolment to delivery (2 trials, 256 women; weighted mean difference -0.25 days, 95% CI -2.81
to 2.31).
Authors’ conclusions
Attempting cephalic version at term reduces the chance of non-cephalic births and caesarean section. There is not enough evidence from
randomised trials to assess complications of external cephalic version at term. Large observational studies suggest that complications
are rare.
PLAIN LANGUAGE SUMMARY
External cephalic version for breech presentation at term
External cephalic version from 36 weeks reduces the chance of breech presentation at birth and caesarean section.
There is less risk to the baby and mother when the baby is head-down at the time of birth. External cephalic version (ECV) is a procedure
by which the baby, who is lying bottom first, is manipulated through the mother’s abdominal wall to the head-down position. The
review of seven studies, 1245 women, found that If the baby is not head down after about 36 weeks of pregnancy, ECV reduces the
chance that the baby will present as breech at the time of birth, and reduces the chance of caesarean birth.
BACKGROUND
Considerable disagreement surrounds the management of breech
presentation, particularly with respect to the place of external
cephalic version (ECV). ECV is a procedure in which the baby
is manipulated by pressure through the mother’s abdominal wall
into a cephalic (head-down) position. The interpretation of nonrandomised trials is confounded by the fact that breech presentation per se appears to be a marker for poor perinatal outcome. For
example, the incidence of minor childhood handicap following
breech presentation has been found to be high (19.4%) and similar for those delivered following trial of labour and those following
an elective caesarean section (Danielian 1996).
Breech presentation may be caused by an underlying fetal or maternal abnormality, or may be an apparently chance occurrence,
or related to an otherwise benign variant such as cornual placental position (the placenta in a lateral position near the top of the
uterus). In the latter instances, breech presentation places a healthy
fetus and mother at increased risk of a complicated vaginal delivery or caesarean section. It is not surprising that, over the years,
the possibility of manipulating the baby from the breech to the
cephalic presentation has intrigued obstetric caregivers.
ECV before term (usually before 34 weeks’ gestation) came into
routine obstetric practice on the basis of the self-evident immediate effectiveness of the procedure as well as reassuring results
from several non-randomised trials, and in spite of the negative
results of the only randomised trial reported prior to 1980 (Brosset
1956). The popularity of ECV before term waned after the mid1970s, partly because of reports of a substantial perinatal mortality associated with the procedure (Bradley-Watson 1975), and the
increasing perception of caesarean section as a safer option than
ECV or breech delivery.
Prior to the mid-1970s, ECV was usually attempted before term
because of the belief that the procedure would seldom be successful at term. Subsequent studies showed that with the use of tocolysis (medication to relax the uterus), ECV could be achieved
in a substantial proportion of women with breech presentation at
term. ECV at term differs in many fundamental ways from that
performed before term. These include the fact that the fetus is
mature and may be delivered more readily in the event of complications, and that spontaneous versions without ECV attempt, or
reversion after successful ECV, are less common at term. ECV before term is therefore evaluated as a separate procedure (see ’External cephalic version for breech presentation before term’ (Hutton
2006)). Rust 2005 randomly allocated at or near term participants
into two groups for late versus early ECV and found no difference
in success rate or mode of delivery. This review includes studies
in which the intention was to include pregnant women at or near
term (i.e. from 36 weeks’ gestation).
External cephalic version at term has been shown to be feasible in
two small uncontrolled trials in women with previous caesarean
section (Flamm 1991; Schachter 1994), and in two in women in
labour (Ferguson 1985; Fortunato 1988). El-Muzaini 2008a and
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
2
El-Muzaini 2008b are abstract reports of prospective controlled
studies of ECV in labour and with previous caesarean section respectively, with results in favour of ECV, but it is not clear whether
these studies were randomised. To our knowledge, no randomised
trials of these interventions have been reported.
External cephalic version may be of particular importance in resource-poor situations in which women may be unable to reach
health services during labour, and caesarean sections are unavailable or unsafe (Hofmeyr 2004a).
Several authors have investigated which factors are associated
with an increased chance of successful external cephalic version
(Boucher 2003; Fortunato 1988; Guyer 2001; Lau 1997; Le Bret
2004). Factors which have been found to predict failure of ECV attempt include engagement of the presenting part, difficulty in palpating the fetal head and a tense uterus on palpation (Lau 1997),
and increased amniotic fluid volume (Boucher 2003). However,
a prediction model based on clinical parameters was found to be
insufficiently accurate to be useful in predicting the outcome of
ECV attempts (Chan 2004).
The preferences of women with breech presentation regarding
their care appear to have changed in recent years. In an Israeli
study in 1995, 54% were willing to consider ECV and 65% preferred planned caesarean section if the breech presentation persisted, compared with 24% and 97% respectively in 2001 (Yogev
2002). In an Australian study in 2001, 39% of women attending
antenatal clinic would choose ECV if needed, and 22% were undecided (Raynes-Greenow 2004).
Complications reported following ECV at term include fracture of
the baby’s femur (Papp 2004), prolonged tachycardia (rapid heartbeat) of the baby (Nzewi 1999), sinusoidal baby’s heart rate pattern
(a fluctuating pattern sometimes indicating compromise) (Ferber
1999), and fetal-maternal haemorrhage (bleeding from the baby’s
to the mother’s circulation in the placenta) (Shankar 2004). The
rate of caesarean section during labour has been found to be greater
following successful ECV than in spontaneous cephalic presentation: 20% versus 6.3%, risk ratio (RR) 3.2 (Ben-Haroush 2002);
27.6% versus 12.5%, RR 2.04; 95% confidence interval 1.43 to
2.91 (Chan 2004b); odds ratio 2.04 for nulliparous women, 4.30
for multiparous (Vezina 2004). This is not surprising, given that
women with persistent breech presentation in the first instance are
a high-risk group. Cord blood gases at delivery were no different
(Chan 2004c).
However, reported series of cases have reported very low complication rates with ECV (Boucher 2003; Impey 1999; Impey
2005). A review of 44 studies of ECV (7377 participants) from
1990 to 2002 found the most frequently reported complication
to be transient abnormal baby’s heart rate patterns (5.7%). Less
frequent complications were persisting pathological baby’s heart
rate patterns (0.37%); vaginal bleeding (0.47%); placental abruption (0.12%); emergency caesarean section (0.43%); and perina-
tal mortality (0.16%) (Collaris 2004). Because of the risk of allo
immunisation, anti-D prophylaxis is recommended for non-sensitised D-negative women following ECV attempts (Fung Kee Fung
2003).
Contra-indications to ECV include: multiple pregnancy, severe
abnormality, unsatisfactory condition or death of the baby, caesarean section necessary irrespective of the presentation (e.g. major
placenta praevia), and ruptured membranes. Relative contraindications include previous caesarean section, poor growth of the
baby, and bleeding from the uterus.
The question of whether ECV might increase the risk of motherto-child transmission of viral infections such as HIV is important
and, in the absence of direct evidence, we have reviewed the relevant biological evidence and concluded that, unlike fetal-maternal transfusion (bleeding from the baby’s to the mother’s circulation in the placenta), maternal-fetal transfusion is extremely rare,
and unlikely to be precipitated by ECV (Holmes 2004). It is also
reassuring that in a randomised trial of fundal pressure to expel
the baby during caesarean section, no evidence of maternal-fetal
transfusion was found (Owens 2003).
Several authors have reported success rates for external cephalic
version at term in routine clinical practice in the region of
40% to 50%: 53% (Hughes 1997); 39% (Williams 1999); 55%
(Guyer 2001); 45% (Devendra 2002); 43% (Lojacono 2003);
51% (Skupski 2003); 42% to 65% (depending on amniotic fluid
volume (Boucher 2003)); and 51% (Le Bret 2004).
Readers are referred to previous reviews of the topic (Hofmeyr
1989; Hofmeyr 1991; Hofmeyr 1992; Hofmeyr 1993; Zhang
1993). See also related Cochrane systematic reviews: ’External
cephalic version for breech presentation before term’, ’Cephalic
version by postural management for breech presentation’ and ’Interventions to help external cephalic version for breech presentation at term’ (Hutton 2006; Hofmeyr 2000; Hofmeyr 2004b).
OBJECTIVES
To assess, using the best available evidence, the effects of external
cephalic version (ECV) at or near term for breech presentation on:
presentation at and method of delivery; and perinatal and maternal
morbidity and mortality.
METHODS
Criteria for considering studies for this review
Types of studies
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
3
Clinical trials comparing the effects of ECV at or near term, with
or without tocolysis, with a control group (no ECV attempt), on
clinically meaningful outcomes; random allocation to treatment
and control groups, with adequate allocation concealment; violations of allocated management and exclusions after allocation not
sufficient to materially affect outcomes.
Types of participants
Pregnant women with babies in the breech presentation at or near
term and no contraindications to ECV.
Types of interventions
Details of the search strategies for CENTRAL and MEDLINE,
the list of handsearched journals and conference proceedings, and
the list of journals reviewed via the current awareness service can
be found in the ‘Specialized Register’ section within the editorial information about the Cochrane Pregnancy and Childbirth
Group.
Trials identified through the searching activities described above
are each assigned to a review topic (or topics). The Trials Search
Co-ordinator searches the register for each review using the topic
list rather than keywords.
In addition, we searched CENTRAL (The Cochrane Library, 2010,
Issue 3) and PubMed (1966 to September 2010) using the terms
external cephalic version OR ECV.
We did not apply any language restrictions.
ECV attempt at term, with or without the use of tocolysis, compared with no ECV attempt.
Data collection and analysis
Types of outcome measures
Perinatal outcomes including non-cephalic presentation at delivery, method of delivery and perinatal and maternal morbidity and
mortality. Outcomes included if clinically meaningful; reasonable
measures taken to minimise observer bias; missing data insufficient
to materially influence conclusions; data available for analysis according to original allocation, irrespective of protocol violations;
data available in format suitable for analysis.
Search methods for identification of studies
For methods used when assessing the trials identified in the previous version of this review see Appendix 1. For this update we used
the following methods when assessing the trials identified by the
updated search (Dafallah 2004; El-Muzaini 2008a; El-Muzaini
2008b; Hindawi 2005; Rust 2005).
Selection of studies
The first author (GJH) and a supporting researcher (TL) (see
Acknowledgements) independently assessed for inclusion all the
potential studies identified as a result of the search strategy. We
resolved any disagreement through discussion and, if required,
would have consulted RK.
Electronic searches
Data extraction and management
We searched the Cochrane Pregnancy and Childbirth Group’s
Trials Register by contacting the Trials Search Co-ordinator (10
September 2010).
The Cochrane Pregnancy and Childbirth Group’s Trials Register
is maintained by the Trials Search Co-ordinator and contains trials
identified from:
1. quarterly searches of the Cochrane Central Register of
Controlled Trials (CENTRAL);
2. weekly searches of MEDLINE;
3. handsearches of 30 journals and the proceedings of major
conferences;
4. weekly current awareness alerts for a further 44 journals
plus monthly BioMed Central email alerts.
We designed a form to extract data. For eligible studies, GJH and
TL extracted the data using the agreed form. We entered data
into Review Manager software (RevMan 2008) and checked for
accuracy. When information was unclear, we attempted to contact
authors of the original reports to provide further details.
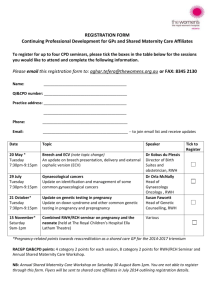
Assessment of risk of bias in included studies
GJH and TL independently assessed the risk of bias for each study
using the criteria outlined in the Cochrane Handbook for Systematic
Reviews of Interventions (Higgins 2009; see Figure 1). We resolved
any disagreement through discussion and, if required, would have
consulted RK.
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
4
Figure 1. Risk of bias graph: review authors’ judgements about each risk of bias item presented as
percentages across all included studies
(1) Sequence generation (checking for possible selection
bias)
We described for each included study the method used to generate
the allocation sequence in sufficient detail to allow an assessment
of whether it should produce comparable groups.
We assessed the method as:
• adequate (any truly random process, e.g. random number
table; computer random number generator);
• inadequate (any non-random process, e.g. odd or even date
of birth; hospital or clinic record number); or
• unclear.
(2) Allocation concealment (checking for possible selection
bias)
We described for each included study the method used to conceal
the allocation sequence in sufficient detail and determined whether
intervention allocation could have been foreseen in advance of, or
during recruitment, or changed after assignment.
We assessed the methods as:
• adequate (e.g. telephone or central randomisation;
consecutively numbered sealed opaque envelopes);
• inadequate (open random allocation; unsealed or nonopaque envelopes, alternation; date of birth);
• unclear.
intervention a participant received. We judged studies at low risk
of bias if they were blinded, or if we judged that the lack of blinding
could not have affected the results. We assessed blinding separately
for different outcomes or classes of outcomes.
We assessed the methods as:
• adequate, inadequate or unclear for participants;
• adequate, inadequate or unclear for personnel;
• adequate, inadequate or unclear for outcome assessors.
(4) Incomplete outcome data (checking for possible attrition
bias through withdrawals, dropouts, protocol deviations)
We described for each included study, and for each outcome or
class of outcomes, the completeness of data including attrition
and exclusions from the analysis. We stated whether attrition and
exclusions were reported, the numbers included in the analysis at
each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes.
Where sufficient information was reported, or could be supplied
by the trial authors, we re-included missing data in the analyses
which we undertook. We assessed methods as:
• adequate;
• inadequate (20% or more data missing);
• unclear.
(3) Blinding (checking for possible performance bias)
We described for each included study the methods used, if any, to
blind study participants and personnel from knowledge of which
(5) Selective reporting bias
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
5
We described for each included study how we investigated the
possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
• adequate (where it was clear that all of the study’s prespecified outcomes and all expected outcomes of interest to the
review had been reported);
• inadequate (where not all the study’s pre-specified outcomes
had been reported; one or more reported primary outcomes were
not pre-specified; outcomes of interest were reported
incompletely and so could not be used; study failed to include
results of a key outcome that would have been expected to have
been reported);
• unclear.
We would have included cluster-randomised trials in the analyses
along with individually randomised trials had there been any, and
would have adjusted their sample sizes or standard errors using the
methods described in the Handbook in Section 16.3.4 and 16.3.6
(Higgins 2009). If we identified both cluster-randomised trials
and individually-randomised trials, we planned to synthesise the
relevant information. We would consider it reasonable to combine
the results from both if there was little heterogeneity between the
study designs and the interaction between the effect of intervention
and the choice of randomisation unit was considered to be unlikely.
We would also acknowledge heterogeneity in the randomisation
unit and perform a separate meta-analysis.
Crossover trials
(6) Other sources of bias
We described for each included study any important concerns we
had about other possible sources of bias. We assessed whether each
study was free of other problems that could put it at risk of bias:
• yes;
• no;
• unclear.
(7) Overall risk of bias
We made explicit judgements about whether studies were at high
risk of bias, according to the criteria given in the Handbook (
Higgins 2009). With reference to (1) to (6) above, we assessed
the likely magnitude and direction of the bias and whether we
considered it likely to impact on the findings. We explored the
impact of the level of bias through undertaking sensitivity analyses
- see Sensitivity analysis.
Measures of treatment effect
We identified no crossover trials on this topic for the update, but
if such trials were identified and deemed eligible for inclusion, we
would include them in the analyses with parallel group trials, using
methods described by Elbourne 2002.
Dealing with missing data
For included studies, we noted levels of attrition. We explored the
impact of including studies with high levels of missing data in the
overall assessment of treatment effect by using sensitivity analysis.
For all outcomes we have carried out analyses, as far as possible, on
an intention-to-treat basis, i.e. we attempted to include all participants randomised to each group in the analyses. The denominator
for each outcome in each trial was the number randomised minus
any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We used the I² statistic to measure heterogeneity among the trials
in each analysis. If we identified substantial heterogeneity (I² >
30%) we explored it by pre-specified subgroup analysis.
Dichotomous data
For dichotomous data, we present results as summary risk ratio
with 95% confidence intervals.
Continuous data
For continuous data, we used the mean difference if outcomes were
measured in the same way between trials. We used the standardised
mean difference to combine trials that measure the same outcome,
but used different methods.
Unit of analysis issues
Cluster-randomised trials
Assessment of reporting biases
Where we suspected reporting bias (see ‘Selective reporting bias’
above), we attempted to contact study authors, asking them to
provide missing outcome data. Where this was not possible, and
the missing data were thought to introduce serious bias, we explored the impact of including such studies in the overall assessment of results by a sensitivity analysis.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2008). We used fixed-effect inverse variance metaanalysis for combining data where trials were examining the same
intervention, and the trials’ populations and methods were judged
sufficiently similar. Where we suspected clinical or methodological
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
6
heterogeneity between studies sufficient to suggest that treatment
effects may differ between trials, we used random-effects metaanalysis. If substantial heterogeneity was identified in a fixed-effect meta-analysis, we noted this and repeated the analysis using a
random-effects method.
Subgroup analysis and investigation of heterogeneity
We performed no subgroup analyses in the original review or the
update. If we identified substantial heterogeneity in a fixed-effect
meta-analysis, we noted this and repeated the analysis using a
random-effects method.
Sensitivity analysis
Due to the potentially high risk of bias in two of the studies
(Dafallah 2004; Hindawi 2005) and our lack of success in contacting the respective trial authors, we undertook the meta-analyses of included studies twice: first, including all the studies and
second, excluding the high risk of bias studies. When sensitivity
analyses showed that the overall results and conclusions were not
affected by their inclusion, we regarded the results of the review
with a higher degree of certainty. If both or either of these studies
had greatly influenced the findings of the review, we would have
recommended an appropriate degree of caution.
RESULTS
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
See Characteristics of included studies.
Risk of bias in included studies
See Characteristics of included studies, particularly the ’Methods’
and ’Notes’ sections.
In three trials, randomly ordered sealed envelopes or cards were
used for allocation, but only one (Mahomed 1991) specified
that the cards were sequentially numbered. Van Dorsten 1981
and Brocks 1984 used ’random’ allocation without specifying the
mechanism. Concealment of allocation was thus not optimal.
Dafallah 2004 and Hindawi 2005 do not describe the methods
of randomisation and allocation concealment at all. In addition,
group sizes differ by 13% and outcomes are not clearly prespecified
in Hindawi 2005. Attempts to contact the respective authors for
more information failed. See Sensitivity analysis.
The exclusion of three women after enrolment in Van Dorsten
1981 is unlikely to have affected the results materially.
Brocks 1984 studied 65 women who agreed to randomisation and
a further 65 who either specifically requested or refused external
cephalic version (ECV) attempt. Because factors which may have
a bearing on the outcome of pregnancy may influence the decision
to accept ECV, we have limited this review to an analysis of the
65 randomised cases.
Van de Pavert 1990 attempted ECV without tocolysis in 21/25 of
the study group, and with tocolysis in 16/20 initial failures. Thus
8/25 (32%) received no ECV attempt (4) or incomplete ECV
protocol (4). ECV was attempted on request in 5/27 of the control
group, tocolysis being used in the three which were successful.
While the analysis was appropriate according to intention-to-treat,
the rate of non-compliance with the allocated treatment reduces
the power of the study to detect differences resulting from ECV
attempt.
Effects of interventions
Because of significant heterogeneity, results for the first two outcomes were pooled using the random-effects model. For all other
data we used the fixed-effect model. Sensitivity analyses showed
overall results not to be greatly influenced by the inclusion of the
two high risk of bias studies and so they are included in the results.
Overall, the pooled data from included studies show a statistically
significant and clinically meaningful reduction in non-cephalic
birth (seven trials, 1245 women; risk ratio (RR) 0.46, 95% confidence interval (CI) 0.31 to 0.66); and caesarean section (seven
trials, 1245 women; RR 0.63, 95% CI 0.44 to 0.90) when ECV
was attempted. Data were not available from all the trials for the
remaining outcomes. There were no significant differences in the
incidence of Apgar score ratings below seven at one minute (two
trials, 108 women; RR 0.95, 95% 0.47 to 1.89) or five minutes
(four trials, 368 women; RR 0.76, 95% 32 to 1.77), low umbilical
artery pH levels (one trial, 52 women RR 0.65; 0.17 to 2.44),
neonatal admission (one trial, 52 women; RR 0.36, 95% 0.04
to 3.24), perinatal death (six trials, 1053 women; RR 0.34, 95%
CI 0.05 to 2.12), nor time from enrolment to delivery (2 trials,
256 women; weighted mean difference -0.25 days, 95% -2.81 to
2.31).
DISCUSSION
The absolute numbers of non-cephalic births and caesarean sections vary considerably between trials. This probably reflects differences in study populations and caesarean section policies. The
direction of effects is, however, consistent, with the exception of
the rates of caesarean section in the study of Van de Pavert 1990.
Considerable crossover between groups in the latter study may
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
7
have reduced the power of the study to show differences related to
external cephalic version (ECV). The study authors suggest that
against a background of low caesarean section rates for breech presentation, the negative experience of failed ECV may render the
woman or doctors more likely to opt for caesarean section.
It has been suggested that ECV may be more successful (and spontaneous version more common) in black African than Caucasian
women, possibly because of the tendency for the presenting part
to remain high until the onset of labour (Hofmeyr 1986). Ethnicity was not a pre-defined sub-group analysis for this review.
However, post-hoc sensitivity analysis excluding the two studies
in black African women (Hofmeyr 1983; Mahomed 1991) eliminated the significant heterogeneity, with the following risk ratios (fixed-effect model): non-cephalic presentation at birth: 0.61
(0.51 to 0.73); caesarean section: 0.65 (0.44 to 0.97).
The recent trend to routine caesarean section for persistent breech
presentation may result in a greater impact of ECV on caesarean
section rates than was apparent in the studies reviewed.
The trials reviewed do not give information on women’s views.
are reassuring. There is sound reason for the clinical use of ECV at
term, with the appropriate precautions, in any woman in whom
the value of an improved chance of a cephalic birth outweighs the
risk of the procedure.
Implications for research
Future research should be directed towards refining the selection of
women suitable for ECV attempt at term. For example, previous
caesarean section has been regarded as a contraindication to ECV.
In an uncontrolled series ECV was found to be successful in 82%
of 56 women with one or two previous caesarean sections (Flamm
1991).
The place of ECV during labour requires further study. This procedure was reported to be successful in 11 (73%) out of 15 women
in labour considered unsuitable for vaginal breech delivery. Caesarean section was avoided in 10 (67%) of the women (Ferguson
1985).
Further research is needed to define more accurately the effect
of ECV on perinatal outcome, and the place of ECV in nonlongitudinal lies.
Future studies should include an assessment of women’s views.
AUTHORS’ CONCLUSIONS
Implications for practice
The studies in this review provide convincing evidence that the
chance of breech birth and caesarean section may be substantially
reduced by attempting external cephalic version (ECV) at or near
term. The numbers studied are too small to give an accurate assessment of the risks of ECV, though data from observation studies
ACKNOWLEDGEMENTS
Tess Lawrie for assistance with study selection, data extraction and
help preparing this update; Sonja Henderson and Denise Atherton
for administrative support; Lynn Hampson and Jill Hampson for
the literature search.
REFERENCES
References to studies included in this review
rate: a controlled trial. British Journal of Obstetrics and
Gynaecology 1983;90:392–9.
Brocks 1984 {published data only}
Brocks V, Philipsen T, Secher NJ. A randomized trial of
external cephalic version with tocolysis in late pregnancy.
British Journal of Obstetrics and Gynaecology 1984;91:653–6.
Mahomed 1991 {published data only}
Mahomed K, Seeras R, Coulson R. External cephalic version
at term. A randomised controlled trial using tocolysis.
British Journal of Obstetrics and Gynaecology 1991;98:8–13.
Dafallah 2004 {published data only}
Dafallah SE, Elhag SM. The role of external cephalic version
on the presentation at delivery. Saudi Medical Journal 2004;
25(3):386–8.
Van de Pavert 1990 {published data only}
Van de Pavert R, Gravenhorst JB, Keirse MJNC. Value of
external version in breech presentation at term. Nederlands
Tijdschrift voor Geneeskunde 1990;134:2245–8.
Hindawi 2005 {published data only}
Hindawi I. Value and pregnancy outcome of external
cephalic version. Eastern Mediterranean Health Journal
2005;11(4):633–9.
Van Dorsten 1981 {published data only}
Van Dorsten JP, Schifrin BS, Wallace RL. Randomized
control trial of external cephalic version with tocolysis in late
pregnancy. American Journal of Obstetrics and Gynecology
1981;141:417–24.
Hofmeyr 1983 {published data only}
Hofmeyr GJ. Effect of external cephalic version in late
pregnancy on breech presentation and caesarean section
References to studies excluded from this review
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
8
Besio 1994 {published data only}
Besio M, Coto M. Evaluation of the external cephalic version
in the management of dystocia (published erratum appears
in Revista Chilena de Obstetricia y Ginecologia 1995;60(2):
145). Revista Chilena de Obstetricia y Ginecologia 1994;59:
422–7.
El-Muzaini 2008a {published data only}
El-Muzaini MF, Felimban HM, Al-Hazmi NM, Shabaan
LA, Namankani FY, Fathudein MA. Breech in labor, to turn
or not to turn?. BJOG: an international journal of obstetrics
and gynaecology 2008;115(s1):77.
El-Muzaini 2008b {published data only}
El-Muzaini MF, Felimban HM, Al-Hazmi NM, Shabaan
LA, Namankani FY, Fathudein MA. Breech with previous
scar, is ECV a good option?. BJOG: an international journal
of obstetrics and gynaecology 2008;115(s1):77–8.
Rust 2005 {published data only}
Rust O, Atlas R, Gersbach E, Roberts W, Larkin R, Hess
LW. A randomized trial of late versus early external cephalic
version for the treatment of abnormal presentation at term
[abstract]. American Journal of Obstetrics and Gynecology
2005;193(6 Suppl):S129.
Stine 1985 {published data only}
Stine LE, Phelan JP, Wallace R, Eglinton GS, Van Dorsten
JP, Schifrin BS. Update on external cephalic version
performed at term. Obstetrics & Gynecology 1985;65:642–6.
Van Veelen 1989 {published data only}
Van Veelen AJ, Van Cappellen AW, Flu PK, Straub MJPF,
Wallenburg HCS. Effect of external cephalic version in
late pregnancy on presentation at delivery: a randomized
controlled trial. British Journal of Obstetrics and Gynaecology
1989;96:916–21.
Additional references
Alderson 2004
Alderson P, Green S, Higgins JPT, editors. Cochrane
Reviewers’ Handbook 4.2.2 [updated December 2003]. In:
The Cochrane Library, Issue 1, 2004. Chichester, UK: John
Wiley & Sons, Ltd.
Ben-Haroush 2002
Ben-Haroush A, Perri T, Bar J, Yogev Y, Bar-Hava I, Hod
M, et al.Mode of delivery following successful external
cephalic version. American Journal of Perinatology 2002;19:
355–60.
Boucher 2003
Boucher M, Bujold E, Marquette GP, Vezina Y. The
relationship between amniotic fluid index and successful
external cephalic version: a 14-year experience. American
Journal of Obstetrics and Gynecology 2003;189:751–4.
Bradley-Watson 1975
Bradley-Watson PJ. The decreasing value of external
cephalic version in modern obstetric practice. American
Journal of Obstetrics and Gynecology 1975;123:237–40.
Brosset 1956
Brosset A. The value of prophylactic external version in
cases of breech presentation. Acta Obstetricia et Gynecologica
Scandinavica 1956;35:555–62.
Chan 2004
Chan LY, Leung TY, Fok WY, Chan LW, Lau TK. Prediction
of successful vaginal delivery in women undergoing external
cephalic version at term for breech presentation. European
Journal of Obstetrics & Gynecology and Reproductive Biology
2004;116:39–42.
Chan 2004b
Chan LY, Tang JL, Tsoi KF, Fok WY, Chan LW, Lau TK.
Intrapartum cesarean delivery after successful external
cephalic version: a meta-analysis. Obstetrics & Gynecology
2004;104:155–60.
Chan 2004c
Chan LY, Leung TY, Fok WY, Chan LW, Lau TK.
Cord blood acid-base status at delivery after successful
external cephalic version. Acta Obstetricia et Gynecologica
Scandinavica 2004;83:436–9.
Collaris 2004
Collaris RJ, Oei SG. External cephalic version: a safe
procedure? A systematic review of version-related risks. Acta
Obstetricia et Gynecologica Scandinavica 2004;83:511–8.
Danielian 1996
Danielian PJ, Wang J, Hall MH. Long term outcome by
method of delivery of fetuses in breech presentation at term:
population based follow up. BMJ 1996;312:1451–3.
Devendra 2002
Devendra K. Introducing routine external cephalic version
for the management of the malpresenting fetus near term.
Medical Journal of Malaysia 2002;57:454–9.
Elbourne 2002
Elbourne DR, Altman DG, Higgins JPT, Curtin F,
Vaillancourt JM. Meta-analyses involving cross-over trials:
methodological issues. International Journal of Epidemiology
2002;31:140–9.
Ferber 1999
Ferber A, Peleg D, Bar-Hava I, Orvieto R, Ben-Rafael Z.
Optimal fetal outcome despite persistent sinusoidal pattern
after external cephalic version. Journal of Obstetrics and
Gynaecology 1999;19:314–5.
Ferguson 1985
Ferguson JE, Dyson DC. Intrapartum external cephalic
version. American Journal of Obstetrics and Gynecology 1985;
152:297–8.
Flamm 1991
Flamm BL, Fried MW, Lonky NM, Giles WS. External
cephalic version after previous cesarean section. American
Journal of Obstetrics and Gynecology 1991;165:370–2.
Fortunato 1988
Fortunato SJ, Mercer LJ, Guzick DS. External cephalic
version with tocolysis: factors associated with success.
Obstetrics & Gynecology 1988;72:59–62.
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
9
Fung Kee Fung 2003
Fung Kee Fung K, Eason E, Crane J, Armson A, De La
Ronde S, Farine D, et al.Prevention of Rh alloimmunization.
Journal of Obstetrics and Gynaecology Canada: JOGC 2003;
25:765–73.
Guyer 2001
Guyer CH, Heard MJ. A prospective audit of external
cephalic version at term: are ultrasound parameters
predictive of outcome?. Journal of Obstetrics and Gynaecology
2001;21:580–2.
Higgins 2009
Higgins JPT, Green S, editors. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.0.2 [updated
September 2009]. The Cochrane Collaboration, 2009.
Available from www.cochrane-handbook.org.
Hughes 1997
Hughes GW. Establishing an external cephalic version
clinic: outcome of the first year. Journal of Obstetrics and
Gynaecology 1997;17:127–31.
Hutton 2006
Hutton EK, Hofmeyr GJ. External cephalic version for
breech presentation before term. Cochrane Database
of Systematic Reviews 2006, Issue 1. [DOI: 10.1002/
14651858.CD000084.pub2]
Impey 1999
Impey L, Lissoni D. Outcome of external cephalic version
after 36 weeks’ gestation without tocolysis. Journal of
Maternal-Fetal Medicine 1999;8(5):203–7.
Hofmeyr 1986
Hofmeyr GJ, Sadan O, Myer IG, Gallal KC, Simko G.
External cephalic version and spontaneous version rates:
ethnic and other determinants. British Journal of Obstetrics
and Gynaecology 1986;93:13–6.
Impey 2005
Impey L, Pandit M. Tocolysis for repeat external cephalic
version in breech presentation at term: a randomised,
double-blinded, placebo-controlled trial. BJOG: an
international journal of obstetrics and gynaecology 2005;112
(5):627–31.
Hofmeyr 1989
Hofmeyr GJ. Breech presentation and abnormal lie in late
pregnancy. In: Chalmers I, Enkin MW, Keirse MJNC
editor(s). Effective care in pregnancy and childbirth. Oxford:
Oxford University Press, 1989:653–65.
Lau 1997
Lau TK, Lo KWK, Wan D, Rogers MS. Predictors of
successful external cephalic version at term: a prospective
study. British Journal of Obstetrics and Gynaecology 1997;
104:798–802.
Hofmeyr 1991
Hofmeyr GJ. External cephalic version at term: how high
are the stakes?. British Journal of Obstetrics and Gynaecology
1991;98:1–3.
Le Bret 2004
Le Bret T, Grange G, Goffinet F, Cabrol D. External
cephalic version: experience about 237 versions at PortRoyal maternity. Journal de Gynecologie, Obstetrique et
Biologie de la Reproduction (Paris) 2004;33:297–303.
Hofmeyr 1992
Hofmeyr GJ. Breech presentation and shoulder dystocia in
childbirth. Current Opinion in Obstetrics and Gynecology
1992;4:807–12.
Hofmeyr 1993
Hofmeyr GJ. External cephalic version at term. Fetal
Maternal Medicine Review 1993;5:213–22.
Hofmeyr 2000
Hofmeyr GJ, Kulier R. Cephalic version by postural
management for breech presentation. Cochrane Database
of Systematic Reviews 2000, Issue 3. [DOI: 10.1002/
14651858.CD000051]
Hofmeyr 2004a
Hofmeyr GJ. Obstructed labor: using better technologies
to reduce mortality. International Journal of Gynaecology &
Obstetrics 2004;85 Suppl 1:S62–72.
Lojacono 2003
Lojacono A, Donarini G, Valcamonico A, Soregaroli M,
Frusca T. External cephalic version for breech presentation
at term: an effective procedure to reduce the caesarean
section rate. Minerva Ginecologica 2003;55:519–24.
Nzewi 1999
Nzewi N, Clerk P, Bowen-Simpkins C. Prolonged fetal
tachycardia-an unusual complication of external cephalic
version. Journal of Obstetrics and Gynaecology 1999;19:
427–8.
Owens 2003
Owens M, Bhullar A, Carlan SJ, O’Brien WF, Hirano
K. Effect of fundal pressure on maternal to fetal
microtransfusion at the time of cesarean delivery. Journal of
Obstetrics and Gynaecology Research 2003;29:152–6.
Hofmeyr 2004b
Hofmeyr GJ, Gyte GML. Interventions to help external
cephalic version for breech presentation at term. Cochrane
Database of Systematic Reviews 2004, Issue 1. [DOI:
10.1002/14651858.CD000184.pub2]
Papp 2004
Papp S, Dhaliwal G, Davies G, Borschneck D. Fetal
femur fracture and external cephalic version. Obstetrics &
Gynecology 2004;104:1154–6.
Holmes 2004
Holmes W, Hofmeyr GJ. Management of breech
presentation in areas with high prevalence of HIV infection.
International Journal of Gynaecology & Obstetrics 2004;87:
272–6.
Raynes-Greenow 2004
Raynes-Greenow CH, Roberts CL, Barratt A, Brodrick
B, Peat B. Pregnant women’s preferences and knowledge
of term breech management, in an Australian setting.
Midwifery 2004;20:181–7.
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
10
RevMan 2003
The Cochrane Collaboration. Review Manager (RevMan).
4.2 for Windows. Oxford, England: The Cochrane
Collaboration, 2003.
RevMan 2008
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan). 5.0. Copenhagen: The Nordic
Cochrane Centre, The Cochrane Collaboration, 2008.
Schachter 1994
Schachter M, Kogan S, Blickstein I. External cephalic
version after previous cesarean section - a clinical dilemma.
International Journal of Gynecology & Obstetrics 1994;45:
17–20.
Shankar 2004
Shankar M, Gough GW, Chakravarti S, Vellacott ID.
Massive feto-maternal haemorrhage with good perinatal
outcome following failed external cephalic version. Fetal
Diagnosis and Therapy 2004;19:68–71.
Skupski 2003
Skupski DW, Harrison-Restelli C, Dupont RB. External
cephalic version: an approach with few complications.
Gynecologic and Obstetric Investigation 2003;56:83–8.
Vezina 2004
Vezina Y, Bujold E, Varin J, Marquette GP, Boucher M.
Cesarean delivery after successful external cephalic version of
breech presentation at term: a comparative study. American
Journal of Obstetrics and Gynecology 2004;190:763–8.
Williams 1999
Williams J, Bjornsson S, Cameron AD, Mathers A, Yahya
Jill SZS, Pell P. Prospective study of external cephalic
version in Glasgow: patient selection, outcome and
factors associated with outcome. Journal of Obstetrics and
Gynaecology 1999;19:598–601.
Yogev 2002
Yogev Y, Horowitz E, Ben-Haroush A, Chen R, Kaplan B.
Changing attitudes toward mode of delivery and external
cephalic version in breech presentations. International
Journal of Gynecology & Obstetrics 2002;79:221–4.
Zhang 1993
Zhang J, Bowes WA, Fortney JA. Efficacy of external
cephalic version: a review. Obstetrics & Gynecology 1993;82:
306–12.
References to other published versions of this review
Hofmeyr 1995
Hofmeyr GJ. External cephalic version at term. [revised
04 October 1993]. In: Enkin MW, Keirse MJNC,
Renfrew MJ, Neilson JP, Crowther C (eds.) Pregnancy and
Childbirth Module. In: The Cochrane Pregnancy and
Childbirth Database [database on disk and CDROM]. The
Cochrane Collaboration; Issue 2, Oxford: Update Software;
1995.
∗
Indicates the major publication for the study
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
11
CHARACTERISTICS OF STUDIES
Characteristics of included studies [ordered by study ID]
Brocks 1984
Methods
65 women who agreed to enter the trial “randomly allocated” to ECV or control group
Participants
Inclusion criteria: singleton breech presentation on ultrasound in 37th week. Agree to
enter study. Exclusion criteria: contraindication to ECV
Interventions
Single ECV attempt following ritodrine 15 µg/minute for 15 minutes. ECV repeated
successfully in two women in whom reversion to breech occurred. Compared with no
ECV attempt
Outcomes
Presentation at delivery; method of delivery.
Notes
A further 65 women who had ECV or no ECV according to request not included in this
review as not randomised. Neonatal outcomes given according to presentation rather
than allocation and therefore not included in the review
Risk of bias
Item
Authors’ judgement
Description
Adequate sequence generation?
Unclear
“Randomly allocated”.
Allocation concealment?
No
Inadequate.
Blinding?
All outcomes
No
Not possible.
Incomplete outcome data addressed?
All outcomes
Unclear
Neonatal outcomes given according to presentation not allocation
Free of selective reporting?
Unclear
Neonatal outcomes given according to presentation not allocation
Free of other bias?
Unclear
Neonatal outcomes given according to presentation rather than allocation and therefore not included in the review
Dafallah 2004
Methods
Stated as ‘randomised control study’; women were ‘randomly allocated to the study group
or the control group’. No other details provided except that randomisation was stratified
by parity (nulliparas and multiparas)
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
12
Dafallah 2004
(Continued)
Participants
620 healthy women with uncomplicated breech pregnancy at 36-38 weeks in Sudan
from 1995-2001 (135 nulliparas and 175 multiparas in the study group compared to
125 nulliparas and 185 multiparas in the control group). Ultrasound examination before
randomisation excluded congenital malformation, oligohydramnios, placenta praevia,
uterine abnormality. Other exclusions were previous CS, APH, hypertensive disorders,
IUGR
Interventions
ECV attempt of up to five minutes without tocolysis versus no ECV attempt. If the
procedure failed or when reversion occurred, the manoeuvre was repeated up to three
times at subsequent antenatal visits
Outcomes
Mode of delivery, Apgar scores at 1, 5, 10 min, fetal weight
Notes
Baseline characteristics were similar except for maternal age (multiparas in control group
older than study group). There were 750 ECV attempts in 310 women: 196/750 successful (26%) with greater success in multiparas. Apgar scores not reported. Additional
information requested but not obtained from authors
Risk of bias
Item
Authors’ judgement
Description
Adequate sequence generation?
Unclear
’Randomly allocated’.
Allocation concealment?
Unclear
Not described.
Blinding?
All outcomes
No
Not described.
Incomplete outcome data addressed?
All outcomes
Yes
No loss to follow-up reported.
Free of selective reporting?
No
The authors do not report on all prespecified outcomes e.g. Apgar scores, or other
key outcomes of interest e.g. morbidity
Free of other bias?
No
Potentially high risk of bias.
Hindawi 2005
Methods
Stated ’randomised controlled trial’. No details of randomisation or allocation concealment are given.
Participants
192 singleton breech pregnancies > 37 weeks gestation at King Hussein Medical Center
in Amman, Jordan (Jan 1999-Dec 2001). Included if: reactive CTG and fetal movements, known Rh group, fasted for 6 hours prior to procedure. Excluded if: fetal abnormality, abnormal CTG, placenta praevia, established labour, ruptured membranes, gestational diabetes requiring insulin, IUGR, proteinuric hypertension disorders, previous
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
13
Hindawi 2005
(Continued)
CS, oligohydramnios, polyhydramnios
Interventions
ECV (90) with tocolysis vs no ECV (102).
Outcomes
’All clinical details concerning the pregnancy, external cephalic version and delivery were
recorded and reviewed.’
Notes
No explanation given for the large difference in group size (90 vs 102). Baseline characteristics similar except for fetal weight (3350 in ECV group vs 3120 in control group).
Outcomes not clearly pre-specified. High risk of bias. Additional information requested
but not obtained from author
Risk of bias
Item
Authors’ judgement
Description
Adequate sequence generation?
Unclear
Stated ’randomised’. No other details provided.
Allocation concealment?
Unclear
Not described.
Blinding?
All outcomes
No
Not described.
Incomplete outcome data addressed?
All outcomes
Unclear
Unclear whether there were protocol deviations, post randomisation exclusions or
missing data
Free of selective reporting?
No
Outcomes are not clearly prespecified.
Free of other bias?
No
Baseline difference in fetal weight; large unexplained difference in group size (control
group 13% bigger than treatment group).
Potentially high risk of bias
Hofmeyr 1983
Methods
Participants allocated by randomly ordered, concealed cards.
Participants
Inclusion criteria: singleton breech presentation on ultrasound examination at 36 or
more weeks’ gestation; consent to participate.
Exclusion criteria: contraindication to ECV.
Interventions
ECV attempt initially without tocolysis. If unsuccessful (7 cases), attempt repeated following hexoprenaline 10 µg by slow IVI injection. Compared with no ECV attempt
Outcomes
Presentation at delivery; method of delivery; Apgar score < 7 at 1 and 5 minutes; perinatal
mortality
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
14
Hofmeyr 1983
(Continued)
Notes
Risk of bias
Item
Authors’ judgement
Description
Adequate sequence generation?
Yes
Previously shuffled cards marked ’V’ or ’C’.
Allocation concealment?
Yes
Concealed cards.
Blinding?
All outcomes
No
Not possible.
Incomplete outcome data addressed?
All outcomes
Yes
Free of selective reporting?
Yes
Free of other bias?
Yes
Mahomed 1991
Methods
Allocation by consecutively numbered sealed opaque envelopes, randomised in blocks
of 6
Participants
Inclusion criteria: singleton breech presentation at 37 weeks or more; consent to participate. Exclusion criteria: contraindication to ECV; non-reactive nonstress test
Interventions
ECV attempt following hexoprenaline 10 µg intravenously over 1 minute, compared
with no ECV attempt
Outcomes
Presentation at delivery; caesarean section rate; 5 minute Apgar score < 7 and < 5;
perinatal mortality; enrolment-labour interval; gestation at delivery
Notes
Factors affecting ECV success rate evaluated in the 103 women in the trial together with
another 104 non-trial ECV attempts. In the latter group one stillbirth occurred 17 days
after successful ECV. The baby was born with the cord tightly around the neck. In the
randomised to ECV group, a baby born vaginally 23 days after successful version was
severely asphyxiated and died at 3 days old. Two perinatal deaths occurred in the control
group following vaginal breech delivery
Risk of bias
Item
Authors’ judgement
Description
Adequate sequence generation?
Yes
Randomised in blocks of 6.
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
15
Mahomed 1991
(Continued)
Allocation concealment?
Yes
Sealed opaque envelopes.
Blinding?
All outcomes
No
Not possible.
Incomplete outcome data addressed?
All outcomes
Yes
No withdrawals or loss to follow-up.
Free of selective reporting?
Yes
Free of other bias?
Yes
Van de Pavert 1990
Methods
Randomisation by sealed envelope.
Participants
Inclusion criteria: singleton breech presentation at more than 36 weeks’ gestation; agree
to participate. Exclusion criteria: contraindication to ECV
Interventions
ECV without tocolysis, followed by ECV attempt with ritodrine infusion, compared
with no ECV attempt
Outcomes
Presentation at delivery; caesarean section rate.
Notes
4 in the ECV group refused ECV attempt, while 5 in the control group had ECV attempt
on request. Analysis was according to intention-to-treat
Risk of bias
Item
Authors’ judgement
Adequate sequence generation?
Yes
Allocation concealment?
Yes
Sealed envelope.
Blinding?
All outcomes
No
Not possible.
Incomplete outcome data addressed?
All outcomes
Yes
Free of selective reporting?
Yes
Free of other bias?
Unclear
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Description
4 in the ECV group refused ECV attempt, while 5
in the control group had ECV attempt on request.
Analysis was according to intention-to-treat
16
Van Dorsten 1981
Methods
Allocation by random number table.
Participants
Inclusion criteria: low-risk pregnant women; breech presentation at 37 to 39 weeks’ gestation; normal ultrasound examination; reactive nonstress test. Exclusion criteria: medical conditions; hypertension; premature labour; premature rupture of membranes; suspected impaired fetal growth; previous uterine surgery; multiple gestation; third trimester
bleeding
Interventions
ECV attempt following terbutaline sulphate infusion at 5 µg per minute for 10 to 15
minutes, compared with no ECV attempt
Outcomes
Presentation at delivery; caesarean section rate; Apgar score < 7 at 1 and 5 minutes;
enrolment-delivery interval; birthweight; meconium during labour or at delivery
Notes
There were 3 exclusions after selection because of oligohydramnios, placenta praevia and
non-reactive nonstress test
Risk of bias
Item
Authors’ judgement
Description
Adequate sequence generation?
Yes
Random number table.
Allocation concealment?
Unclear
Not described.
Blinding?
All outcomes
No
Not possible.
Incomplete outcome data addressed?
All outcomes
Yes
Free of selective reporting?
Yes
Free of other bias?
Unclear
3 post-randomisation exclusions.
APH: antipartum haemorrhage
CS: caesarean section
CTG: cardiotocograph
ECV: external cephalic version
IUGR: intrauterine growth restriction
IVI: intravenous
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
17
Characteristics of excluded studies [ordered by study ID]
Study
Reason for exclusion
Besio 1994
Controlled trial of ECV at term, not randomised. Cephalic presentation at term in 32/45 versus 4/45 in the
control group. Caesarean sections 22/45 versus 39/45 respectively
El-Muzaini 2008a
This is an abstract from a conference presentation of intrapartum ECV (30 women) without tocolysis compared
to no ECV attempt (30 women). No mention of whether randomisation was used in group allocation. Attempts
to contact authors for clarity failed
El-Muzaini 2008b
This is an abstract from a conference presentation of outpatient ECV without tocolysis (40 women) compared
to no ECV attempt (47 women) in women with a singleton breech and one previous lower segment caesarean
section. No mention of whether randomisation was used in group allocation. Attempts to contact authors for
clarity failed
Rust 2005
This randomised trial compares late ECV with early ECV.
Stine 1985
Non-randomised follow-on study after completion of the Van Dorsten randomised trial. ECV was successful
in 108/148 women. Six were lost to follow-up and seven reverted to abnormal lies. Of the remaining 95,
23 underwent caesarean section. One unexplained intrauterine death occurred 3 weeks after successful ECV.
One maternal death occurred at caesarean section 4 days after successful ECV, from amnionitis, septicaemia,
intravascular coagulation and amniotic fluid embolus
Van Veelen 1989
Excluded because ECV attempts commenced at 33 weeks, and continued up to term. See review ’External
cephalic version for ECV before term’ (Hutton 2006).
ECV: external cephalic version
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
18
DATA AND ANALYSES
Comparison 1. External cephalic version at term
Outcome or subgroup title
No. of
studies
No. of
participants
7
7
2
4
1
1
6
2
1245
1245
108
368
52
52
1053
256
1 Non-cephalic births
2 Caesarean section
3 Apgar score < 7 at 1 minute
4 Apgar score < 7 at 5 minutes
5 Umbilical vein pH < 7.20
6 Neonatal admission
7 Perinatal death
8 Enrolment-delivery interval
Statistical method
Effect size
Risk Ratio (M-H, Random, 95% CI)
Risk Ratio (M-H, Random, 95% CI)
Risk Ratio (M-H, Fixed, 95% CI)
Risk Ratio (M-H, Fixed, 95% CI)
Risk Ratio (M-H, Fixed, 95% CI)
Risk Ratio (M-H, Fixed, 95% CI)
Risk Ratio (M-H, Fixed, 95% CI)
Mean Difference (IV, Fixed, 95% CI)
0.46 [0.31, 0.66]
0.63 [0.44, 0.90]
0.95 [0.47, 1.89]
0.76 [0.32, 1.77]
0.65 [0.17, 2.44]
0.36 [0.04, 3.24]
0.34 [0.05, 2.12]
-0.25 [-2.81, 2.31]
Analysis 1.1. Comparison 1 External cephalic version at term, Outcome 1 Non-cephalic births.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 1 Non-cephalic births
Study or subgroup
Treatment
Control
n/N
n/N
17/31
29/34
16.5 %
0.64 [ 0.45, 0.91 ]
Dafallah 2004
135/310
210/310
18.6 %
0.64 [ 0.55, 0.75 ]
Hindawi 2005
34/90
92/102
17.4 %
0.42 [ 0.32, 0.55 ]
Hofmeyr 1983
1/30
20/30
3.1 %
0.05 [ 0.01, 0.35 ]
18/103
87/105
15.3 %
0.21 [ 0.14, 0.32 ]
Van de Pavert 1990
16/25
20/27
16.2 %
0.86 [ 0.60, 1.25 ]
Van Dorsten 1981
8/25
19/23
12.8 %
0.39 [ 0.21, 0.71 ]
614
631
100.0 %
0.46 [ 0.31, 0.66 ]
Brocks 1984
Mahomed 1991
Total (95% CI)
Risk Ratio
Weight
M-H,Random,95% CI
Risk Ratio
M-H,Random,95% CI
Total events: 229 (Treatment), 477 (Control)
Heterogeneity: Tau2 = 0.19; Chi2 = 45.45, df = 6 (P<0.00001); I2 =87%
Test for overall effect: Z = 4.10 (P = 0.000041)
0.001 0.01 0.1
1
10 100 1000
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
19
Analysis 1.2. Comparison 1 External cephalic version at term, Outcome 2 Caesarean section.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 2 Caesarean section
Study or subgroup
Treatment
Control
n/N
n/N
7/31
12/34
11.4 %
0.64 [ 0.29, 1.42 ]
Dafallah 2004
44/310
45/310
20.1 %
0.98 [ 0.67, 1.44 ]
Hindawi 2005
35/90
62/102
22.1 %
0.64 [ 0.47, 0.87 ]
Hofmeyr 1983
6/30
13/30
10.9 %
0.46 [ 0.20, 1.05 ]
13/103
35/105
15.6 %
0.38 [ 0.21, 0.67 ]
Van de Pavert 1990
7/25
3/27
6.3 %
2.52 [ 0.73, 8.69 ]
Van Dorsten 1981
7/25
17/23
13.5 %
0.38 [ 0.19, 0.74 ]
614
631
100.0 %
0.63 [ 0.44, 0.90 ]
Brocks 1984
Mahomed 1991
Total (95% CI)
Risk Ratio
Weight
M-H,Random,95% CI
Risk Ratio
M-H,Random,95% CI
Total events: 119 (Treatment), 187 (Control)
Heterogeneity: Tau2 = 0.13; Chi2 = 15.49, df = 6 (P = 0.02); I2 =61%
Test for overall effect: Z = 2.55 (P = 0.011)
0.1 0.2
0.5
1
2
5
10
Analysis 1.3. Comparison 1 External cephalic version at term, Outcome 3 Apgar score < 7 at 1 minute.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 3 Apgar score < 7 at 1 minute
Study or subgroup
Treatment
Control
n/N
n/N
Hofmeyr 1983
3/30
5/30
40.7 %
0.60 [ 0.16, 2.29 ]
Van Dorsten 1981
9/25
7/23
59.3 %
1.18 [ 0.53, 2.66 ]
55
53
100.0 %
0.95 [ 0.47, 1.89 ]
Total (95% CI)
Risk Ratio
Weight
M-H,Fixed,95% CI
Risk Ratio
M-H,Fixed,95% CI
Total events: 12 (Treatment), 12 (Control)
Heterogeneity: Chi2 = 0.74, df = 1 (P = 0.39); I2 =0.0%
Test for overall effect: Z = 0.16 (P = 0.87)
0.1 0.2
0.5
1
2
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
5
10
20
Analysis 1.4. Comparison 1 External cephalic version at term, Outcome 4 Apgar score < 7 at 5 minutes.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 4 Apgar score < 7 at 5 minutes
Study or subgroup
Treatment
Control
n/N
n/N
Hofmeyr 1983
0/30
0/30
0.0 [ 0.0, 0.0 ]
Mahomed 1991
8/103
10/105
0.82 [ 0.34, 1.98 ]
Van de Pavert 1990
0/25
1/27
0.36 [ 0.02, 8.43 ]
Van Dorsten 1981
0/25
0/23
0.0 [ 0.0, 0.0 ]
183
185
0.76 [ 0.32, 1.77 ]
Total (95% CI)
Risk Ratio
Risk Ratio
M-H,Fixed,95% CI
M-H,Fixed,95% CI
Total events: 8 (Treatment), 11 (Control)
Heterogeneity: Chi2 = 0.24, df = 1 (P = 0.62); I2 =0.0%
Test for overall effect: Z = 0.64 (P = 0.52)
0.01
0.1
1
10
100
Analysis 1.5. Comparison 1 External cephalic version at term, Outcome 5 Umbilical vein pH < 7.20.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 5 Umbilical vein pH < 7.20
Study or subgroup
Treatment
Control
n/N
n/N
3/25
5/27
100.0 %
0.65 [ 0.17, 2.44 ]
25
27
100.0 %
0.65 [ 0.17, 2.44 ]
Van de Pavert 1990
Total (95% CI)
Risk Ratio
Weight
M-H,Fixed,95% CI
Risk Ratio
M-H,Fixed,95% CI
Total events: 3 (Treatment), 5 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.64 (P = 0.52)
0.1 0.2
0.5
1
2
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
5
10
21
Analysis 1.6. Comparison 1 External cephalic version at term, Outcome 6 Neonatal admission.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 6 Neonatal admission
Study or subgroup
Treatment
Control
n/N
n/N
1/25
3/27
100.0 %
0.36 [ 0.04, 3.24 ]
25
27
100.0 %
0.36 [ 0.04, 3.24 ]
Van de Pavert 1990
Total (95% CI)
Risk Ratio
Weight
M-H,Fixed,95% CI
Risk Ratio
M-H,Fixed,95% CI
Total events: 1 (Treatment), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.91 (P = 0.36)
0.01
0.1
1
10
100
Analysis 1.7. Comparison 1 External cephalic version at term, Outcome 7 Perinatal death.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 7 Perinatal death
Study or subgroup
Treatment
Control
n/N
n/N
Brocks 1984
0/31
0/34
0.0 [ 0.0, 0.0 ]
Dafallah 2004
0/310
2/310
0.20 [ 0.01, 4.15 ]
Hofmeyr 1983
0/30
0/30
0.0 [ 0.0, 0.0 ]
Mahomed 1991
1/103
2/105
0.51 [ 0.05, 5.54 ]
Van de Pavert 1990
0/25
0/27
0.0 [ 0.0, 0.0 ]
Van Dorsten 1981
0/25
0/23
0.0 [ 0.0, 0.0 ]
524
529
0.34 [ 0.05, 2.12 ]
Total (95% CI)
Risk Ratio
Risk Ratio
M-H,Fixed,95% CI
M-H,Fixed,95% CI
Total events: 1 (Treatment), 4 (Control)
Heterogeneity: Chi2 = 0.23, df = 1 (P = 0.63); I2 =0.0%
Test for overall effect: Z = 1.16 (P = 0.25)
0.01
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
0.1
1
10
100
22
Analysis 1.8. Comparison 1 External cephalic version at term, Outcome 8 Enrolment-delivery interval.
Review:
External cephalic version for breech presentation at term
Comparison: 1 External cephalic version at term
Outcome: 8 Enrolment-delivery interval
Study or subgroup
Treatment
Mahomed 1991
Van Dorsten 1981
Total (95% CI)
Control
Mean Difference
Weight
Mean Difference
14 (9)
87.6 %
0.0 [ -2.73, 2.73 ]
17.6 (13.9)
12.4 %
-2.00 [ -9.25, 5.25 ]
100.0 %
-0.25 [ -2.81, 2.31 ]
N
Mean(SD)
N
Mean(SD)
103
14 (11)
105
25
15.6 (11.5)
23
128
IV,Fixed,95% CI
IV,Fixed,95% CI
128
Heterogeneity: Chi2 = 0.26, df = 1 (P = 0.61); I2 =0.0%
Test for overall effect: Z = 0.19 (P = 0.85)
Test for subgroup differences: Not applicable
-10
-5
0
5
10
APPENDICES
Appendix 1. Methods used to assess trials included in previous versions of this review
The following methods were used to assess Brocks 1984; Hofmeyr 1983; Mahomed 1991; Van de Pavert 1990; Van Dorsten 1981.
We evaluated trials under consideration for methodological quality and appropriateness for inclusion according to the prespecified
selection criteria, without consideration of their results. Individual outcome data were included in the analysis if they met the prespecified
criteria in ’Types of outcome measures’.
Assessment of methodological quality of included studies
We assessed the validity of each study using the criteria outlined in the Cochrane Reviewers’ Handbook (Alderson 2004). Each study
was assessed for quality of allocation of concealment, completeness to follow up and blinding in the assessment of outcome.
(1) Selection bias (randomisation and allocation concealment)
We assigned a quality score for each trial, using the following criteria:
(A) adequate concealment of allocation, such as telephone randomisation, consecutively numbered sealed opaque envelopes;
(B) unclear whether adequate concealment of allocation;
(C) inadequate concealment of allocation, such as open list of random number tables, sealed envelopes.
(2) Performance bias (blinding of participants, researchers and outcome assessment)
(A) Blinding of participants and caregiver was not possible due to the type of intervention being assessed;
(B) blinding of outcome assessment (yes/no/unclear).
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
23
(3) Attrition bias (loss to follow up)
We assessed completeness to follow up using the following criteria:
(A) less than 5% of participants excluded;
(B) 5% to 10% of participants excluded;
(C) more than 10% and less than 20% of participants excluded;
(D) more than 20% of participants excluded.
We extracted data from the sources and entered them onto the Review Manager software (RevMan 2003), checked for accuracy, and
analysed as above using RevMan 2003. For dichotomous data, we calculated risk ratios and 95% confidence intervals. Continuous
data were pooled using weighted mean differences and 95% confidence intervals. Results were pooled using a fixed-effect model or, if
heterogeneity was significant, and random-effects model.
WHAT’S NEW
Last assessed as up-to-date: 7 December 2010.
Date
Event
Description
10 September 2010
New search has been performed
Search updated. Two new studies included (Dafallah 2004; Hindawi 2005)
and three studies excluded (Rust 2005; El-Muzaini 2008a; El-Muzaini
2008b). Conclusions not changed.
HISTORY
Protocol first published: Issue 2, 1996
Review first published: Issue 2, 1996
Date
Event
Description
2 July 2010
Amended
Contact details edited.
2 September 2008
Amended
Converted to new review format.
1 April 2005
Amended
Revised to be consistent with revision of review ’External cephalic version
for breech presentation before term’ (Hutton 2006). Van Veelen 1989 trial
reassigned to the latter review.
Search updated. No new trials identified.
31 December 2004
New search has been performed
Literature search revised. No new data identified.
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
24
CONTRIBUTIONS OF AUTHORS
GJ Hofmeyr prepared the original version and maintains the review. R Kulier revised and quality-checked the review.
DECLARATIONS OF INTEREST
Justus Hofmeyr is an author of one of the papers included in this review (Hofmeyr 1983) but he was not involved in assessing this
study for inclusion, assessing trial quality, or data extraction.
SOURCES OF SUPPORT
Internal sources
• (GJH) Effective Care Research Unit, University of the Witwatersrand/Fort Hare, Eastern Cape Department of Health, South
Africa.
• Department of Obstetrics and Gynaecology, Geneva University Hospital, Switzerland.
External sources
• (GJH) South African Medical Research Council, South Africa.
• (GJH) HRP-UNDP/UNFPA/WHO/World Bank Special Programme in Human Reproduction, Geneva, Switzerland.
• Rockefeller Foundation, USA.
INDEX TERMS
Medical Subject Headings (MeSH)
∗ Breech
Presentation; ∗ Version, Fetal
MeSH check words
Female; Humans; Pregnancy
External cephalic version for breech presentation at term (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
25