Mortality Among Foreign Nationals in Chiang Mai City, Thailand
advertisement

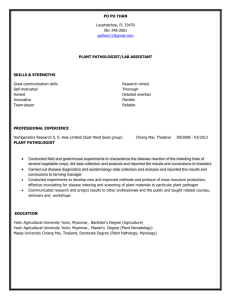
344 ORIGINAL ARTICLE Mortality Among Foreign Nationals in Chiang Mai City, Thailand, 2010 to 2011 Vichan Pawun, MD, MPH,∗† Surasing Visrutaratna, DDS, DrPH,‡ Kumnuan Ungchusak, MD, MPH,§ Suteerat Mahasing, MA,‡ Chosita Khumtalord, MS,‡ Siriying Tipsriraj, MS,|| Chalermpol Chenwittaya, BA,|| Thomas E. Guadamuz, PhD,†¶ and Stephen R. Wisniewski, PhD† ∗ Department of Disease Control, Bureau of General Communicable Disease, Ministry of Public Health, Nonthaburi, Thailand; of Epidemiology, University of Pittsburgh Graduate School of Public Health (GSPH), Pittsburgh, PA, USA; ‡ Chiang Mai Provincial Public Health Office, Ministry of Public Health, Chiang Mai, Thailand; § Department of Disease Control, Ministry of Public Health, Nonthaburi, Thailand; || Department of Disease Control, Office of Disease Prevention and Control, 10th, Chiang Mai Province, Chiang Mai, Thailand; ¶ Center for Health Policy Studies, Faculty of Social Sciences and Humanities, Mahidol University, Nakorn Pathom, Thailand † Department DOI: 10.1111/j.1708-8305.2012.00654.x Background. Up to 65% of travelers to less developed countries report health problems while traveling. International travel is an increasing concern for health practitioners. To date, there have not been any published analyses of mortality amongst foreign nationals visiting Thailand. Our objectives are to examine the magnitude and characterize the deaths among foreign nationals in Chiang Mai, a popular tourist province in Thailand. Methods. The study commenced with a review of the Thai death registration. Death certificates were retrieved, reviewed, and classified by the causes of death. Basic statistics and proportionate mortality ratio (PMR) were used to describe the pattern of deaths. Standardized mortality ratio (SMR) was used to assess the excess mortality risk among foreign nationals. Results. Between January 1, 2010 and May 31, 2011, there were 1,295 registered deaths in Chiang Mai City, of which 102 records (7.9%) were foreign nationals. Median age of decedents was 64 years (range 14–102 y). Female-to-male ratio was 1 : 5.4. The highest mortality was among Europeans (45.1%). Most of the deaths were natural causes (89.2%) including 36 cardiac diseases (PMR = 35.3) and 20 malignancy diseases (PMR = 19.6). Deaths due to external causes were low. The SMRs range between 0.15 and 0.30. Conclusion. Communicable diseases and injuries were not the leading causes of death among foreign nationals visiting Chiang Mai, Thailand. It is essential that travelers are aware of mortality risk associated with their underlying diseases and that they are properly prepared to handle them while traveling. A s overseas travel becomes more affordable, the number of people traveling outside their home countries has increased. According to data from the United Nations World Tourism Organization, approximately 880 million travelers visited foreign countries in 2009.1 The number increased by 7% in 2010, to 940 million travelers.1 The numbers of international travelers visiting Southeast Asia has also Corresponding Author: Vichan Pawun, MD, MPH, Department of Disease Control, Bureau of General Communicable Disease, Ministry of Public Health, Nonthaburi 11000, Thailand. E-mail: vichpw@health2.moph.go.th © 2012 International Society of Travel Medicine, 1195-1982 Journal of Travel Medicine 2012; Volume 19 (Issue 6): 344–351 increased significantly; by 2010, this region hosted 69.6 million travelers.1 Thailand hosted approximately 15.8 million in 2010, about 12.6% higher than in 2009.2 With the increase in international tourism, Thailand has augmented its efforts to address health issues related to international travel. The Thai government commended the implementation of International Health Regulations (IHR 2005), which entered into effect in June 2007.3 In accordance with these regulations (Annex 1 of the IHR 2005) the local public health agencies shall utilize their resources to improve their capacity of epidemiological surveillance to tracking health problems among those residing and visiting their jurisdiction.3,4 Mortality Analysis in Chiang Mai Several factors contribute to morbidity and mortality for international travelers. Individual characteristics, behaviors, and underlying disease conditions of travelers may increase or exacerbate the likelihood of a travelrelated health complication.5 Among travel-related morbidity studies, Freedman reported the morbidity rates for illness after traveling in developing countries to be about 22% to 64%.6 Mortality studies among international travelers are limited. The US Department of State reports that over 6,000 Americans die abroad each year.7 The Health Protection Agency Office in the UK reports more than 4,000 British nationals die abroad each year.8 In Thailand, epidemiological data on the health status among international travelers are limited. Most travel-related health research in Thailand has focused on tropical diseases such as dengue hemorrhagic fever, and malaria.9 – 11 There have not been any epidemiological studies on international travelers who expire while visiting Thailand. This is the first study to do so, and we elected to examine mortality data among foreign travelers in Chiang Mai Province, one of the most frequented tourist destinations in Thailand. Chiang Mai is one of 77 provinces in Thailand, and the provincial city is about 700 km north of Bangkok, the capital city of Thailand. The population was approximately 1.7 million in 2009. The province hosted approximately 4.3 million visitors in 2009, including 3.1 million Thais and 1.2 million foreign nationals.12 The primary objective of this study is to assess characteristics, patterns, and causes of death among foreign nationals in Chiang Mai City. The secondary objective is to develop public health strategies to monitor health problems among foreign nationals in Thailand. Methods We assessed the mortality registration system in Thailand from 1991 to 2010. The system flow of the death registration was evaluated by reviewing publicly available documents, official websites, and work manuals.13 – 15 All registered deaths of foreign nationals under the jurisdiction of the Chiang Mai Municipality were manually reviewed. The Chiang Mai Municipality is governed by an elected official, a ‘‘mayor,’’ that oversees four administration offices in four divisions of the Chiang Mai City. These included the administration offices at the Sriwichai, Mengrai, Kawila, and Nakhonping subdistricts.16 In order to gain permissions to access the death certificates, an official letter was sent to the respective mayor, and then allowance letters were submitted to the chief officers of these four offices. At the local offices, which do not utilize electronic databases, all processes of data collection were based on manually reviewing paper documents, including logbook records of death registrations, accessing the stored folders of death certificates, and extracting data from the selected certificates. The selection criteria were 345 specified for all death records of non-Thai nationals, all ages and genders from January 1, 2010 to May 31, 2011. Certificates of death among immigrant workers were excluded from this study. Data Retrieval and Analysis Data on nationality, age, gender, cause of death, place of death, and date of death were extracted and recorded using a standardized form. To ensure the confidentiality of individuals, data with personal identifiers were not collected. Local administrators supervised all data extraction to ensure that confidentiality was observed. Data analysis included the summary of the causes of death, the proportion of death stratified by nationalities, geographical continent, age group, and gender. As the exact number of international travelers visiting Chiang Mai City could not be determined, the mortality rates among this specific population were not calculated. In order to characterize the pattern of death, proportionate mortality ratio (PMR) was used to represent the proportional comparisons of cause-specific death of all registered deaths among foreign nationals. For the PMR estimation, it is important to note that a high PMR of death in one category will result in the low proportion of another category.17 The study proposes to use the standardized mortality ratio (SMR) as an epidemiological measure to assess risk of death among foreign nationals in Chiang Mai City. The SMR was calculated by totaling the actual observed number of deaths and dividing it by the expected number of deaths.18,19 The expected number of deaths was estimated by applying the mortality rate in reference populations to the total number of international arrivals by age group, which include all types of international traveler arrivals (eg, airport, seaport, and ground crossing). International arrival data were collected from the Ministry of Tourism and Sport’s database. This database provides information about the number of foreign nationals visiting Thailand by age group. However, it does not provide such information in a specific location. Hence, the total number of foreign nationals visiting Chiang Mai City was assumed to be 10% of all international arrivals, per the estimate provided by the Chiang Mai Governor’s House.12 The reference mortality rates were taken from the World Health Organization’s database.20 We utilized the global population and the populations of the top three nationalities in terms of frequency of deaths in this study as the reference population. As most mortality rates in our reference populations were the annual death rates, an average length of stay among international travelers visiting Thailand was about 9 days.21 Therefore, before applying the age-specific death rates to population in each age group, we converted the annual death rates to the 9-day-period death rate. To do so, we assumed that mortality rates in reference populations were constant throughout the year. J Travel Med 2012; 19: 344–351 346 Pawun et al. Figure 1 Death registration system and flow of mortality data in Thailand. Mortality System in Thailand The Population Registration System is the source of population demographic data in Thailand. The system provides nationality status information including the authentication of birth and death certificates. The Civil Registration Act (No. 1) of B.E. 2534 and the additional revision (No. 2) of B.E. 2551 specifies that all deaths occur in Thailand must be registered within 24 hours of being witnessed. There is no specific death registration system for foreign nationals. The process of death reporting and registering is similar to the process for Thai citizens (Figure 1). In cases of unknown or uncertain death, the investigation officers are charged to investigate. As pursuant to Thailand Criminal Procedure Code 148, the investigative officials may conduct or request a forensic autopsy to determine the cause of death before issuing the investigation report to the next of kin. The next of kin is then required to submit the report to the local administration office to obtain an authenticated death certificate. For deaths occurring within medical establishments, the attending physicians are authorized to issue the medical certificate of death. The original medical certificate of death is given to the next of kin, and a copy is kept in the hospital files. The next of kin is required to submit the medical death certificate to the local J Travel Med 2012; 19: 344–351 administration office to obtain an authenticated death certificate. All registered death records are automatically sent to the central database at the Bureau of Registration Administration, Ministry of Interior. This database is shared with the Ministry of Public Health and the National Statistical Office.12 – 15,22 As all authenticated death certificates are issued in the official Thai language, translated death certificates authorized by the embassy or general consulate are helpful for the next of kin in resolving assets and estate matters in their respective countries. The certification of death in Thailand classifies deaths into three categories: death within medical establishment due to medical illnesses; death outside medical establishment due to natural causes; and death due to unnatural or external causes such as suicides, homicides, deaths from beastly attacks, deaths from accidents, and deaths of unknown cause.13,14,22 Descriptive Analysis During the 17-month study period, between January 1, 2010 and May 31, 2011, there were a total of 1,295 deaths registered in the Chiang Mai Municipality. Of these 1,295 deaths, 102 (7.9%) were among non-Thai nationals, with 66 deaths registered in 2010 (64.7%) and 36 deaths registered in 2011 (35.3%). On average, there were six (SD ± 3.52) deaths of foreign nationals registered at Chiang Mai City each month. The median 347 Mortality Analysis in Chiang Mai Table 1 Number and proportion of deaths among foreign nationals in Chiang Mai City by gender, age groups, and causes of deaths, from January 1, 2010 to May 31, 2011 (N = 102) Age group Female 10–19 20–29 30–39 40–49 50–59 60–69 70–79 >80 Total Male 10–19 20–29 30–39 40–49 50–59 60–69 70–79 >80 Total Grand total ∗ † Cardiac diseases Malignant neoplasm Infectious diseases All other diseases∗ Unnatural causes Total (%) 0 2 0 1 1 0 1 2 7 (43.7) 0 0 0 0 0 1 0 0 1 (6.3) 0 0 1 0 0 1 0 1 3 (18.7) 0 0 0 1 1 1 0 2 5 (31.3) 0 0 0 0 0 0 0 0 0 (0.0) 0 (0.0) 2 (12.5) 1 (6.3) 2 (12.5) 2 (12.5) 3 (18.7) 1 (6.3) 5 (31.3) 16 (15.7)† 0 0 0 3 5 11 6 4 29 (33.7) 36 (35.3) 1 0 0 0 5 6 6 1 19 (22.1) 20 (19.6) 0 0 0 1 1 2 1 4 9 (10.5) 12 (11.8) 0 2 0 1 2 7 3 3 18 (20.9) 23 (22.5) 0 3 1 3 3 1 0 0 11 (12.8) 11 (10.8) 1 (1.2) 5 (5.8) 1 (1.2) 8 (9.3) 16 (18.6) 27 (31.4) 16 (18.6) 12 (13.9) 86 (84.3)† 102 (100.0) Other medical diseases include respiratory diseases, gastrointestinal disease, and other nonspecific medical condition. Proportion of deaths among foreign nationals by gender. age of death among foreign nationals was 64 years (range 14–102 y). The highest number of deaths was among the 60 to 69 years age group (n = 30 deaths, 29.4%) followed by 50 to 59 years (17.6%), 70 to 79 years (16.7%), and over 80 years (16.7%) (Table 1). The female-to-male ratio of death among non-Thai nationals was 1 to 5.4. The region of residence and nationalities of the decedents is shown in Table 2. The largest number of deaths were among travelers from Europe (46 deaths; 45.1%), followed by North America (28 deaths; 27.5%), Asia (18 deaths; 17.7%), and Australia and Oceania (9 deaths; 8.8%). Among Europeans, the main countries of residence included the UK (11 deaths; 23.9%) and Germany (9 deaths; 19.6%). Among North American visitors, the United States had the largest number of deaths in Chiang Mai City (25 deaths; 89.3%). For Australia and Oceania, Australia had the highest number of deaths (8 deaths; 88.9%). For Asia, there were 8 deaths (44.4%) of Japanese and 6 deaths (33.3%) of Chinese visitors. Deaths from medical illnesses were predominant for all age groups, accounting for 89.2% of all deaths. Table 3 shows that medical illnesses were the main cause of death among all foreign nationals. The unnatural deaths were relatively high among Europeans compared with other regions (p = 0.538). Suicide and drug abuse-related deaths were highest among Australia and Oceania compared with other regions (p < 0.001). Figure 2 characterizes the cause-specific deaths among foreign nationals in Chiang Mai City. Cardiovascular disease was the most common cause of death among foreign nationals (36 cases; PMR = 35.3), followed by malignant neoplasms (20 cases; PMR = Table 2 Regional origin distribution of deaths among foreign nationals in Chiang Mai City, from January 1, 2010 to May 31, 2011 (N = 102) Region Number of deaths (%) Selected countries Number of deaths per country (%) Europe 46 (45.10) North America 28 (27.45) Asia 18 (17.65) UK Germany The Netherlands France The United States Canada Japan China Australia New Zealand — 11 (23.91) 9 (19.57) 7 (15.22) 5 (10.67) 25 (89.29) 3 (10.71) 8 (44.44) 6 (33.33) 8 (88.89) 1 (11.11) — Australia and Oceania 9 (8.82) Unidentified 1 (0.98)∗ ∗ There is one record of unknown nationality. 19.6), infections (12 cases; PMR = 11.8), and cerebrovascular disease (6 cases; PMR = 5.9). Lung infection and sepsis were the most common cause of death from infections. Among the deaths that were classified as unnatural causes, there were four accidental deaths (PMR = 3.9), four suicides (PMR = 3.9), two cases of drug overdose (PMR = 2.0), and one case of drowning (PMR = 1.0). There was no record of homicide during the study period. As shown in Table 4, all of the expected deaths of foreign nationals, based on different standard population death rates, are greater than the observed number of deaths among foreign nationals in Chiang Mai City. The SMRs range between 0.15 and 0.30 (Table 5). J Travel Med 2012; 19: 344–351 348 Pawun et al. Table 3 Geographical distribution of deaths among foreign nationals in Chiang Mai City by the causes of death, from January 1, 2010 to May 31, 2011 (N = 102) Region Medical illnesses Accident Suicide Drug overdose Drowning Total 40 27 18 5 1 91 4 0 0 0 0 4 1 1 0 2 0 4 0 0 0 2 0 2 1 0 0 0 0 1 46 28 18 9 1 102 Europe North America Asia Australia and Oceania None∗ Total ∗ There is one record of unknown nationality. Cardiovascular diseases Malignant neoplasms Infectious diseases Cerebrovascular disease Gastrointestinal disease Lung disease All other diseases Accidents Suicide Drug overdose Drowning Homicide 0.0% 5.0% 10.0% 15.0% 20.0% 25.0% 30.0% 35.0% 40.0% Figure 2 The proportionate mortality ratios (PMRs) of each cause-specific death among foreign nationals in Chiang Mai City, from January 1, 2010 to May 31, 2011 (N = 102). Discussion The distribution of mortality among foreign travelers by age and gender shows a similar pattern with the studies conducted in Canada,23,24 the United States,25,26 and Australia.27 The study reveals that mortality distribution was predominant in older persons (≥50 y). This finding might be as a result of the large number of senior foreign nationals aged 50 years and above who reside in Thailand. Data from the Thailand Immigration Bureau show that the number of senior foreign nationals approved for retirement visas to reside in Thailand increased by 20% from 22,000 visas in 2008 to 27,000 visas in 2009.28 We found a much greater proportion of deaths among male foreign nationals. However, this is not a measurement of mortality rate, and therefore it cannot imply that the risk of death among males is higher than that of females. A significant finding of our study was that the leading causes of death among foreign nationals less than 50 years were medical illnesses. Cardiovascular disease was the leading cause of death, accounting for approximately 35%, which is consistent with studies of travelers from Australia, Canada, the United States, and Scotland.23 – 27,29,30 We also found malignancy deaths ranked second among all causes of deaths, accounting for approximately 20%. This finding differs from many previously cited studies, but it was similar to the findings of Leggat and Wilks in Australia.27 J Travel Med 2012; 19: 344–351 We applied the SMRs to examine whether foreign nationals in Chiang Mai City have a higher mortality than one would expect in their home countries. Surprisingly, we found that no matter what the choice of reference populations, the results yielded very low SMRs. All of the calculated SMRs are less than 1, indicating that the mortality risk among foreign nationals visiting Chiang Mai City did not exceed mortality risk as compared with the risk in their home countries. In other words, there was no evidence of any increased risk of death from residing in or traveling to Chiang Mai City. There were several assumptions and limitations in this study. First, because there is no specific death registry for foreign nationals, the administrative database was assumed to be the complete database for all foreign nationals. We also assumed that the accuracy and completeness of death registration data for foreign nationals were similar to the registration data for Thai citizens. According to Tangcharoensathien et al.’s study in 2006, the completeness of the death registration in Thailand was high with 95% completeness of registration; however, only 30% of the causes of death described in the registers matched the causes determined by the medical review.31 These inherent limitations of the death registry may impact the accuracy of our study’s results. Second, the study was unable to determine the exact number of foreign nationals visiting Chiang Mai City and it was unable to distinguish shortterm travelers from long-term travelers (stay of ≥6 m). As a result, the mortality rate of foreign nationals was unable to be determined. Finally, the mortality rates in reference populations were assumed to be constant throughout the year. This assumption may influence an accuracy of the SMR estimation. Disease exacerbation among individuals with chronic illnesses while traveling is not unexpected. Seeking pre-travel consultation early, at least 4 to 6 weeks prior to departure is recommended for all travelers with underlying diseases.32 Our results indicate that infections were not the common cause of travel-related death in Thailand, thus health professionals should highlight the likelihood of disease exacerbation and provide a proper preparation for travelers, rather than focusing on antimalarial or antibiotic prophylaxis. In order to gain a better understanding of travelers’ health 349 Mortality Analysis in Chiang Mai Table 4 rates Comparison of the expected deaths and observed deaths among foreign nationals using different standard population Age group Approximate numbers of foreign nationals in Chiang Mai City∗ UK population death rate† (per 100,000) US population death rate† (per 100,000) AUS population death rate† (per 100,000) Global population death rate† (per 100,000) Under 15 15–24 25–34 35–44 45–54 55–64 >65 Total 59,767 155,624 385,135 343,223 276,758 166,322 59,594 1,446,423 0.31 0.94 1.60 3.22 7.03 17.24 254.71 0.48 1.90 2.53 4.40 10.17 21.61 235.12 0.37 1.47 2.16 3.29 6.99 16.57 270.57 4.80 4.88 7.02 11.22 23.18 51.74 348.67 Observed deaths among foreign nationals‡ 1 0 4 1 12 16 32 66 Age group Approximate numbers of foreign nationals in Chiang Mai City∗ Expected deaths based on UK population Expected deaths based on US population Expected deaths based on AUS population Expected deaths based on global population Observed deaths among foreign nationals‡ Under 15 15–24 25–34 35–44 45–54 55–64 >65 Total 59,767 155,624 385,135 343,223 276,758 166,322 59,594 1,446,423 0.19 1.46 6.17 11.04 19.45 28.67 151.79 218.77 0.28 2.95 9.73 15.11 28.15 35.95 140.12 232.29 0.22 2.28 8.31 11.30 19.35 27.56 161.24 230.26 2.87 7.60 27.02 38.51 64.15 86.06 207.79 433.98 1 0 4 1 12 16 32 66 ∗ The approximate numbers of foreign nationals visiting Chiang Mai were estimated from the 10% of total international arrivals in Thailand in 2007 (most updated data) from the Department of Tourism, Ministry of Tourism and Sports. † The 9-d-period period population mortality rates. These rates were estimated from the annual death rates of the reference populations in 2009 (most recent database) published by the World Health Organization. ‡ The observed number of deaths among foreign nationals in Chiang Mai City in 2010 (1-y period). Table 5 Comparison of the standardized mortality ratios using different standard populations Choice of standard population rate SMR∗ 95% confidence interval UK population death rate US population death rate AUS population death rate Global death rate 0.30 0.28 0.29 0.15 0.09–0.51 0.16–0.41 0.08–0.49 0.11–0.19 ∗ The standardized mortality ratio (SMR) is defined as SMR = observed number of deaths among foreign nationals per year/expected number of deaths among foreign nationals per year. and provide an appropriate health intervention for international travelers, host countries should strengthen their capacity to monitor health status among this specific population using the most accurate and applicable approach. Updating information of the characteristics of travelers’ risks and understanding characteristics of health problems among foreign nationals will be useful for expanding epidemiological knowledge on providing a better prepared public health infrastructure that may include accessible emergency services as well as targeted prevention programs. In Thailand, we recommended that both national and local health authorities utilize a vital statistic for monitoring health status among foreign nationals and review this statistic frequently. The usefulness of this statistic can be strengthened by increasing completeness and accuracy of the death records, as well as checking consistency with medical or autopsy data. Conclusion Increasing our understanding of travel-related risks and how they relate to mortality is important to improve preventive responses. It is valuable to know the characteristics of deaths among foreign nationals visiting Thailand because this information can be used for identifying high-risk travelers and high-risk activities and for developing specific interventions to reduce likelihood of overseas mortality. This study has produced encouraging results in identifying the potential value of exploring the vital statistics and tourism statistics to estimate mortality risk among foreign nationals in Thailand. It is however only a first step. Further work at national level will be needed to validate the findings of this study. Our results suggest that the risk of overseas mortality among foreign nationals visiting Chiang Mai City was not high as compared with the mortality risk in their home countries. Hence, Chiang Mai City may not be J Travel Med 2012; 19: 344–351 350 a high-risk destination for foreign nationals. The common causes of death among foreign nationals visiting Chiang Mai City were not infections or injuries, but the major causes of death were chronic illnesses such as cardiovascular diseases and malignancies. It is essential that travelers are aware of the mortality risk associated with chronic diseases and that they are properly prepared to handle them. We recommend that travelers who have chronic diseases should seek medical advice and prepare for a risk of disease exacerbation while traveling. Health care providers should underline the importance of pre-travel planning for persons with underlying diseases. Contributing to the literature of travel epidemiology, particularly for Thailand, will be useful for improving better health advocacy for travelers. Public health practitioners should outline the usefulness of travel epidemiology and the importance of pre-travel consultation. Acknowledgments We would like to thank many individuals who have made this study possible. We are especially grateful to the mayor of Chiang Mai City; the chief officers of Sriwichai, Mengrai, Kawila, and Nakhonping subdistricts; a director of the Bureau of Epidemiology; a director and all staffs in the Field Epidemiology Training Program (FETP) Thailand; and all officials at Chiang Mai Health Office and the Office of Disease Prevention and Control Region 10, Chiang Mai Province. Declaration of Interests The authors state that they have no conflicts of interest to declare. References 1. The World Tourism Organization. UNWTO tourism highlights. 2011 Ed. Available at: www.unwto.org/pub. (Accessed 2011 Sep 21) 2. Department of Tourism, Ministry of Tourism and Sports. International tourist arrivals to Thailand. Available at: http://secretary.mots.go.th. (Accessed 2011 Sep 21) 3. Ungchusak K, Prempree P, Thepsoontorn S, Tantinimitkul C. Thailand national core capacity development plan in compliance with international health regulations (2005), 2008–2012. Bangkok: Thaiveteran Organization, 2008:3–10. 4. World Health Organization. International health regulations. 2nd Ed. Switzerland: WHO Press, 2008. 5. Poumerol G, Wilder-Smith A. World Health Organization. International travel and health. 2010 Ed. Geneva, 2010: 1–3. Available at: http://www.who.int/ ith/ITH2010.pdf. (Accessed 2011 Sep 21) 6. Freedman DO. Travel epidemiology. In: Brunette GW, Kozarsky PE, Magill AJ, Shlim DR, eds. CDC health information for international travel 2012. New York: Oxford University Press, 2012:11–15. J Travel Med 2012; 19: 344–351 Pawun et al. 7. The U.S. Department of State. Tips for travelling abroad. Available at: http://travel.state.gov/travel/tips. (Accessed 2011 Nov 10) 8. The Health Protection Agency Office. Mortality and non-infectious morbidity in travellers. Available at http://www.hpa.org.uk. (Accessed 2011 Nov 10) 9. Thimasarn K, Jatapadma S, Vijaykadga S, et al. Epidemiology of malaria in Thailand. J Travel Med 1995; 2:59–65. 10. Schwartz E. Study of dengue fever among Israeli travelers to Thailand. Dengue Bull 2002; 26:162–167. 11. Wiwanitkit V. Rate of malarial infection among foreigners in a tertiary hospital of Thailand: change of epidemiology and importance of travel medicine (1996–2005). J Vect Borne Dis 2007; 44:219–222. 12. Chiang Mai Province. Chiang Mai Province’s general information. Available at: http://www.chiangmai.go.th. (Accessed 2011 Jun 22) 13. Department of Provincial Administration. Death registration process. Available at: http://www.dopa.go.th/. (Accessed 2011 Jul 5) 14. Department of Provincial Administration. The 1991 Population Registration Act. Available at: http://www.dopa. go.th/. (Accessed 2011 Jul 5) 15. World Health Organization, South-East Asia Regional Office (WHO SEARO). Mortality system in Thailand. Available at: www.searo.who.int/. (Accessed 2011 Jul 5) 16. Chiang Mai Municipality. Chiang Mai municipality’s organization. Available at: http://www.cmcity.go.th. (Accessed 2011 Jun 22) 17. Guptill KS, Hargarten SW, Baker TD. American travel deaths in Mexico: causes and prevention strategies. West J Med 1991; 154:169–171. 18. Curtin LR, Klein RJ. Direct standardization (age-adjusted death rates). National Center for Health Statistics. Stat Note 1995; 6:1–11. 19. Gordis L. Measuring of disease occurrence: II. Mortality. In: Gordis L, ed. Epidemiology. 4th Ed. Philadelphia, PA: US Elsevier, 2008:59–80. 20. World Health Organization. Global health observatory data repository. Geneva. Available at: http://apps.who.int/ ghodata/?vid=61780. (Accessed 2011 Sep 21) 21. Department of Tourism, Ministry of Tourism and Sports. Summary of tourism statistic in Thailand, 2004–2010. Available at: http://www.mots.go.th. (Accessed 2011 Dec 13) 22. Vapattanawong P, Sarplone O. Deaths outside residential area of Thais: study from death registration, 1996–2009. Thai Population Association, 2011. Available at http://www.thaipopulation.org. (Accessed 2011 Jun 22) 23. MacPherson DW, Gushulak BD, Sandhu J. Death and international travel—the Canadian experience: 1996 to 2004. J Travel Med 2007; 14:77–84. 24. MacPherson DW, Guérillot F, Streiner DL, et al. Death and dying abroad: the Canadian experience. J Travel Med 2000; 7:227–233. 25. Hargarten SW, Baker TD, Guptill K. Overseas fatalities of United States citizen travelers: an analysis of deaths related to international travel. Ann Emerg Med 1991; 20:622–626. 26. Lawson CJ, Dykewicz CA, Molinari NAM, et al. Deaths in international travelers arriving in the United States, July 1, 2005 to June 30, 2008. J Travel Med 2012; 19:96–103. 27. Leggat PA, Wilks J. Overseas visitor deaths in Australia, 2001 to 2003. J Travel Med 2009; 16:243–247. Mortality Analysis in Chiang Mai 28. Immigration Bureau. Immigration statistic. Police Department, Nonthaburi. Available at: http://www.immi gration.go.th/. (Accessed 2011 Dec 13) 29. Redman CA, MacLennan A, Walker E. Causes of death abroad: analysis of data on bodies returned for cremation to Scotland. J Travel Med 2011; 18:96–101. 30. Tonellato DJ, Guse CE, Hargarten SW. Injury deaths of US citizens abroad: new data source, old travel problem. J Travel Med 2009; 16:304–310. 351 31. Tangcharoensathien V, Faramnuayphol P, Teokul W, et al. A critical assessment of mortality statistics in Thailand: potential for improvement. Bull World Health Organ 2006; 84:233–238. 32. Barbeau D. Travelers with chronic illnesses. In: Brunette GW, Kozarsky PE, Magill AJ, Shlim DR, eds. CDC health information for international travel 2012. New York: Oxford University Press, 2012:532–536. Wat Arun Pagoda on the west bank of the Chao Phraya river in Bangkok is a much-frequented tourist spot. Thailand is one of the most popular tourist destinations, with more than 20.5 million tourist arrivals annually. Photo Credit: Nicolas Bossard (Setting: Wat Arun Pagoda, Bangkok, Thailand) J Travel Med 2012; 19: 344–351