University of Iowa
Iowa Research Online
Theses and Dissertations
Spring 2013
Internal and marginal fit Of pressed and cad lithium
disilicate crowns made from digital and
conventional impressions
Evanthia Anadioti
University of Iowa
Copyright 2013 Evanthia Anadioti
This dissertation is available at Iowa Research Online: http://ir.uiowa.edu/etd/2435
Recommended Citation
Anadioti, Evanthia. "Internal and marginal fit Of pressed and cad lithium disilicate crowns made from digital and conventional
impressions." MS (Master of Science) thesis, University of Iowa, 2013.
http://ir.uiowa.edu/etd/2435.
Follow this and additional works at: http://ir.uiowa.edu/etd
Part of the Oral Biology and Oral Pathology Commons
INTERNAL AND MARGINAL FIT OF PRESSED AND CAD LITHIUM DISILICATE
CROWNS MADE FROM DIGITAL AND CONVENTIONAL IMPRESSIONS
by
Evanthia Anadioti
A thesis submitted in partial fulfillment
of the requirements for the Master of
Science degree in Oral Science
in the Graduate College of
The University of Iowa
May 2013
Thesis Supervisor: Professor Steven A. Aquilino
Copyright by
EVANTHIA ANADIOTI
2013
All Rights Reserved
Graduate College
The University of Iowa
Iowa City, Iowa
CERTIFICATE OF APPROVAL
_______________________
MASTER’S THESIS
_______________
This is to certify that the Master’s thesis of
Evanthia Anadioti
has been approved by the Examining Committee
for the thesis requirement for the Master of Science
degree in Oral Science at the May 2013 graduation.
Thesis Committee: __________________________________
Steven A. Aquilino Thesis Supervisor
__________________________________
David G. Gratton
__________________________________
Julie A. Holloway
__________________________________
Isabelle L. Denry
__________________________________
Geb W. Thomas
To my family, your love and support made it all worthwhile.
ii
ACKNOWLEDGMENTS
First and foremost I wish to express my sincere appreciation and gratitude to Dr.
Steven A. Aquilino, my thesis supervisor, for his phenomenal knowledge, invaluable
guidance, patience during the frustrating times and commitment to the highest standards
in every step of this research project. I would, also, like to thank my thesis committee,
Drs. David G. Gratton, Julie A. Holloway, Isabelle L. Denry and Geb W. Thomas, for
their help, time, encouragement and recommendations throughout the last three years.
I, also, wish to thank Dr. Fang Qian, for the statistical analysis and Dr. Marcos
Vargas for his help with the E4D system. Special thanks to Mr. R Henry Husemann for
his time, skills and help with the pressing procedure and to Mr. Josh Kistner, from the
Geomagic technical support, for his generous time, support and knowledge in developing
a protocol for the measuremnets.
I would like to acknlowledge the University of Iowa for providing me the
facilities to complete this project.
I am grateful for the financial support received from the Academy of Esthetic
Denstirty and the Greater New York Academy of Prosthodontics, as well as for the
generous donation of their porducts from Ivoclar Vivadent and Whip Mix Corp.
iii
TABLE OF CONTENTS
LIST OF TABLES ............................................................................................................. vi
LIST OF FIGURES .......................................................................................................... vii
CHAPTER
I.
INTRODUCTION ........................................................................................... 1
Research Objectives......................................................................................... 3
Research Hypotheses ....................................................................................... 4
II.
LITERATURE REVIEW ................................................................................ 5
Background of full-coverage restorations ....................................................... 5
Materials used for full-coverage dental restorations ....................................... 5
All-ceramic ............................................................................................... 6
IPS e.max all-ceramic ............................................................................... 8
Longevity of all-ceramic restorations ............................................................ 13
Marginal and internal fit of dental restorations ............................................. 15
Methods to measure the marginal gap ........................................................... 18
Marginal adaptation of all-ceramics .............................................................. 27
Dental impressions......................................................................................... 30
Dental plaster and stone ................................................................................. 35
Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM)
systems ........................................................................................................... 37
Stereolithography (SLA) ............................................................................... 43
Digital dental impressions ............................................................................. 45
Lava™ C.O.S. ........................................................................................ 48
Accuracy of Lava™ C.O.S. .................................................................... 55
Repeatability of Lava™ C.O.S. .............................................................. 56
Fit of crowns made from Lava™ C.O.S. impressions............................ 57
E4D Dentist System™............................................................................ 59
Accuracy of E4D Dentist System™ ....................................................... 63
Summary-Purpose.......................................................................................... 64
III.
MATERIALS AND METHODS .................................................................. 65
Introduction.................................................................................................... 65
Pilot study ...................................................................................................... 65
Results of the pilot study ........................................................................ 68
Validation of the Digital Measurement Technique ................................ 70
Definitive study ............................................................................................. 72
Study design................................................................................................... 73
Master die fabrication ............................................................................. 73
Impression making ................................................................................. 74
Conventional impression ........................................................................ 74
Digital impression .................................................................................. 77
IPS e.max Press crown fabrication ......................................................... 78
IPS e.max CAD crown fabrication ......................................................... 81
Measurement of the crown fit ........................................................................ 84
iv
Statistical analysis .......................................................................................... 91
IV.
RESULTS ...................................................................................................... 93
3D results ....................................................................................................... 93
One-way ANOVA for 3D Marginal fit .................................................. 93
Two-way ANOVA for 3D Marginal fit.................................................. 95
2D results ....................................................................................................... 96
One-way ANOVA for 2D Marginal fit .................................................. 96
Two-way ANOVA for 2D Marginal fit.................................................. 97
One-way ANOVA for 2D Internal fit .................................................... 99
Two-way ANOVA for 2D Internal fit .................................................. 100
V.
DISCUSSION .............................................................................................. 103
Study design................................................................................................. 111
Possible limitations of the study .................................................................. 116
Avenues for future research ......................................................................... 117
Clinical significance .................................................................................... 117
VI.
CONCLUSIONS ......................................................................................... 118
APPENDIX A. RAW DATA ........................................................................................ 120
APPENDIX B. GEOMAGIC IMAGES ........................................................................ 124
REFERENCES ............................................................................................................... 132
v
LIST OF TABLES
Table
1.
Properties of contemporary all-ceramic materials ................................................... 12
2.
Current digital impression systems .......................................................................... 47
3.
Comparisons of the ten variables among the four Experimental Groups: Pilot
data ........................................................................................................................... 69
4.
Pressing program parameters for IPS e.max Press LT ............................................ 80
5.
Speed crystallization/Glaze LT program parameters............................................... 83
6.
Mean 3D marginal gap in mm of 4 experimental groups ........................................ 94
7.
Result of One-Way ANOVA for 2D marginal fit.................................................... 96
8.
Result of Two-Way ANOVA for 2D marginal fit ................................................... 97
9.
Pairwise comparisons of mean 2D marginal gap by experimental group ............... 98
10.
Result of One-Way ANOVA for 2D internal fit.................................................... 100
11.
Result of Two-Way ANOVA for 2D internal fit ................................................... 100
12.
Pairwise comparisons of mean 2D internal gap by experimental group ............... 102
A1. Average marginal gap for 3D measurements ........................................................ 120
A2. Average marginal and internal gaps for 2D measurements ................................... 124
vi
LIST OF FIGURES
Figure
1.
Laser Triangulation. ................................................................................................. 25
2.
The Lava™ C.O.S. system ...................................................................................... 48
3.
The rotation of the aperture mechanism .................................................................. 50
4.
In-plane object coordinates ...................................................................................... 51
5.
The depth information ............................................................................................. 51
6.
The Active Waveform Sampling. ............................................................................ 52
7.
The E4D Dentist System™...................................................................................... 60
8.
Study Groups for the pilot study .............................................................................. 66
9.
Study Groups for the definitive study. ..................................................................... 72
10.
Master die frontal view ............................................................................................ 73
11.
Master die occlusal view.......................................................................................... 74
12.
Stone die .................................................................................................................. 77
13.
Resin die .................................................................................................................. 78
14.
Intaglio of one indicative crown from each experimental group ............................. 84
15.
Defined area around the margin of the Master Die with 0.75mm occlusalgingival width .......................................................................................................... 86
16.
Grooves on the base of the Master Die in order to standardize the sections ........... 87
17.
Facial-lingual section with the 7 standardized points .............................................. 88
18.
Mesial-distal section with the 7 standardized points ............................................... 88
19.
3D measurement of the predefined area .................................................................. 93
20.
Mean 3D marginal gap of 4 experimental groups ................................................... 95
21.
Mean 2D marginal gap in mm ................................................................................. 99
22.
Mean 2D internal gap in mm ................................................................................. 102
B1. Group A (PVS/press) 3D colored map .................................................................. 124
B2. Group A (PVS/press) Facial-Lingual section for 2D measurements ..................... 125
vii
B3. Group A (PVS/press) Mesial-Distal section for 2D measurements ...................... 125
B4. Group B (PVS/CAD) 3D colored map .................................................................. 126
B5. Group B (PVS/CAD) Facial-Lingual section for 2D measurements ..................... 127
B6. Group B (PVS/CAD) Mesial-Distal section for 2D measurements ...................... 127
B7. Group C (Lava/press) 3D colored map .................................................................. 128
B8. Group C (Lava/press) Facial-Lingual section for 2D measurements .................... 129
B9. Group C (Lava/press) Mesial-Distal section for 2D measurements ...................... 129
B10. Group D (Lava/CAD) 3D colored map ................................................................. 130
B11. Group D (Lava/CAD) Facial-Lingual section for 2D measurements .................... 131
B12. Group D (Lava/CAD) Mesial-Distal section for 2D measurements...................... 131
viii
1
CHAPTER I
INTRODUCTION
Although marginal opening alone does not directly correlate with microleakage,
the accuracy of marginal fit is valued as one of the most important criteria for the clinical
quality and success of prosthetic restorations (1). The importance of precise marginal
adaptation and the subsequent implications of marginal discrepancies, including
microleakage, caries and periodontal inflammation, have been emphasized in many
studies (2-7). In addition to marginal fit, internal fit and accuracy play a significant role
in the longevity of a full-coverage restoration as well (8-17). Several definitions for
marginal deficiencies have been proposed, such as internal gap, marginal gap, horizontal
marginal discrepancy, over-extended margin, seating discrepancy and others (18). In
addition, several methods, both destructive and non-destructive, to measure marginal and
internal fit have been discussed in the literature; including sectioning the crowns, replica
technique, profilometry, SEM, image analysis and 3D scanning (19-39).
All the required steps during the fabrication of a crown necessitate precision and
exactness in order to produce an accurately fitting restoration. Recent advances in
technology have dramatically altered impression and crown fabrication procedures;
specifically, digital impressions and computer-aided design/computer-aided
manufacturing (CAD/CAM) systems have been introduced in dental clinical practice.
The impression of the hard and soft tissue of the oral cavity is one of the most
crucial steps for a successful dental restoration. The dental impression can strongly affect
the fit and accuracy of the indirect restoration. Over the past several decades, the
2
impression materials have changed and today with proper selection and manipulation,
excellent impressions can be obtained (40-47). In addition to the impression material, the
choice of the impression technique is of great importance (48-51). The combination of
the proper material, the most reliable technique and adequate understanding and
knowledge by the operator gives the most accurate results (52, 53). The introduction of
dental digital impressions is a breakthrough in our specialty (54-57). Digital or virtual
impression systems have the potential to produce accurate results while simplifying the
entire prosthesis fabrication process, since several laboratory steps are eliminated (5861). Nevertheless, the recent introduction, the limited use and the very limited research
with conflicting results do not allow for valid conclusions with regard to the accuracy and
reliability of digital impression systems (62-64).
Most digital impression systems are designed to be used in conjunction with allceramic restorations. This has coincided with the growing demand for all-ceramic
restorations that most closely mimic tooth appearance and the development of all-ceramic
materials with strength comparable to metal-ceramic restorations (65-68). Lithium
disilicate (IPS e.max, Ivoclar Vivadent) is a glass-ceramic, which claims to combine high
flexural strength along with optimum esthetics. It can be processed using either lost-wax
hot pressing techniques or CAD/CAM milling procedures. Apart from the properties of
the all-ceramic material itself, a very important consideration with regard to the longterm success of the restoration is its internal and marginal fit. Pressed ceramics have been
shown to demonstrate marginal accuracy comparable to that of metal restorations (69).
On the other hand, the marginal accuracy of milled ceramic restoration is mainly
depended on the CAD/CAM system used (70, 71). Studies have shown the latter
3
restorations had inferior marginal fit compared to pressed restorations (72, 73). However,
several advancements have occurred in milling technologies and new systems have been
introduced that claim to produce accurately fitting restorations (74).
There are no studies evaluating the influence of both the impression technique and the
prosthesis fabrication technique on the overall fit of the complete final all-ceramic
restoration.
Research Objectives
The purpose of this study was to evaluate in vitro the marginal and internal fit of allceramic crowns made from two different impression techniques (digital vs. conventional)
and two different fabrication methods (CAD vs. press).
The objectives of this study were:
1. To evaluate in vitro the marginal and internal fit of all-ceramic crowns made from
two different impression techniques (digital vs. conventional).
2.
To evaluate in vitro the marginal and internal fit of all-ceramic crowns made
from two different fabrication methods (CAD vs. press).
3. To determine if there is an interaction between the impression and crown
fabrication techniques with regard to the accuracy of the final crown.
4. To determine which combination of impression and crown fabrication technique
results in the most accurately fitting crown.
4
Research Hypotheses
HO (1) There is no difference in accuracy between the two impression techniques,
conventional and digital, considering the marginal and internal fit of the crowns
fabricated by those methods.
HA (1) There is a difference in accuracy between the two impression techniques,
conventional and digital, considering the marginal and internal fit of the crowns
fabricated by those methods.
HO (2) There is no difference in accuracy between the crown fabrication methods, press
and CAD, considering the marginal and internal fit of the crowns fabricated by those
methods.
HA (2) There is a difference in accuracy between the crown fabrication methods, press
and CAD, considering the marginal and internal fit of the crowns fabricated by those
methods.
HO (3) There is no interaction between the impression technique (conventional and
digital) and the crown fabrication method, considering the marginal and internal fit of the
crowns fabricated by any combination of those methods.
HA (3) There is an interaction between the impression technique (conventional and
digital) and the crown fabrication method, considering the marginal and internal fit of the
crowns fabricated by any combination of those methods.
5
CHAPTER II
LITERATURE REVIEW
Background of full-coverage restorations
Full-coverage dental restorations are integral part of fixed prosthodontics. The
reasons that compel patients to seek any type of dental restorations including inlays,
onlay, veneers and crowns, could be divided into the following: 1) Dental disease
including caries or periodontal causes, 2) Trauma such as accidents and 3) Esthetics to
improve the appearance of their smile. The number of crowns delivered in a
prosthodontic practice is high because their use can be incorporated into any treatment
plan with any combination of teeth, dental implants and removable prostheses.
Throughout the years, crowns have been the restoration most studied with regard to
longevity, causes of failures, materials, and techniques; thus, there is some evidence to
support their successful clinical use.
Materials used for full-coverage dental restorations
The restorations that prosthodontists use in clinical practice include full coverage
crowns, veneers, onlays, inlays and fixed partial dentures. Along with the diversity of the
restoration type, comes the diversity of materials used to produce each one of those types.
Many materials have been used throughout the history of fixed prosthodontics, and each
one presents its own indications, advantages and disadvantages. Currently, based on the
most commonly used materials, restorations could be categorized as cast veneer (full
gold), metal-ceramic and all-ceramic.
6
All-ceramic
With the increased demand for more esthetic appearance, all-ceramic restorations
have become very popular over the last decades. Such restorative all-ceramic systems
must fulfill biomechanical requirements and should provide longevity similar to metal–
ceramic restorations while providing enhanced esthetics (66). Dental ceramics can be
classified according to their fusion temperature, application, fabrication technique and
crystalline phase (41).
According to Kelly, there are two concepts behind the science of ceramics used
in dentistry (68). The first concept includes three main groups: predominantly glassy
materials, particle-filled glasses and polycrystalline ceramics and the second concept
includes any composition of two or more of those groups. The ceramics that best mimic
the optical properties of enamel and dentin belong to the first group and the filler
particles that improve the mechanical properties and control optical results belong to the
second group. A special subgroup in the second category is glass-ceramic, such as the
crystalline lithium disilicate filler. The third group has no glassy components and is much
tougher and stronger than glassy materials; these are used as substructure materials
(cores) upon which glassy ceramics are veneered, including glass-infiltrated alumina
ceramic, polycrystalline alumina ceramic, lithium disilicate based glass–ceramic (75) as
well as the recently introduced yttria-stabilized zirconia polycrystals (Y-TZP) (76). After
the core has been fabricated, veneering porcelain is placed in order to give esthetic result
most closely matched to natural tooth appearance.
7
Culp and McLaren presented three disadvantages of veneered all-ceramic
restorations (75). The first disadvantage is the high value and increased opacity of the
substructure material, which prevent it from being used for the whole thickness of the
prosthesis especially in aesthetic areas. The second disadvantage is that although the
high-strength material has excellent mechanical properties, the layering ceramic, to which
is veneered, exhibits a much lower flexural strength and fracture toughness; for example,
the zirconia core (900-1000 MPa flexural strength) is less than half of the cross-sectional
width of a restoration. Veneering material, which has only 80-110 MPa, covers the rest
and inevitably it tends to chip or fracture (77). The same concept applies to lithium
disilicate, which has flexural strength of 440 MPa, and the nano-fluorapatite glassceramic (IPS e.max Ceram) that is layered upon it has flexural strength of 80-100 MPa.
The third disadvantage is the combination of two incompatible materials in a synergistic
way, whether that combination is metal with metal-ceramic or zirconia with zirconia
layering ceramic, where a strong bond is difficult to create since it depends on several
variables (cleanliness of bond surface, furnace calibration, cooling schedule, operator’s
experience) (75).
The interaction of core and veneer material can be complex. Fahmy evaluated the
influence of three different veneering materials (Vitadur-N, Vitadur-α, and VM7) on the
marginal fit and fracture resistance of an alumina core (In-Ceram) (78). The gaps were
measured before and after veneering. The results showed that Vitadur-N veneered cores
had statistically significant larger marginal gaps and decreased fracture resistance,
whereas no significant difference was established between the other two materials tested.
The fracture patterns were different with Vitadur-N veneered cores showing
8
delaminations, while the other groups showed complete failure involving both core and
veneer. After the specimens were fractured, selected fragments were examined using
SEM. For the Vitadur-N veneered crowns, the core/veneer interface appeared clear and
evident with multiple spaces showing incomplete adherence. For the Vitadur-α group, the
boundary appeared to have no gaps suggesting a good bond between the veneer and the
core. For the VM7 veneered crowns, the boundary appeared evident; however, an
apparent interlocking between the core and the veneer was present. The study concluded
that veneering materials might alter the properties of alumina cores with regard to fit,
strength and failure pattern.
Because of these disadvantages, current research has focused on transitioning
towards increasing the volume percentage of crystalline material with less or even no
glassy components. Full polycrystalline ceramics have become practical for fixed
prostheses as a result of the use of highly controlled starting powders and the application
of computers to ceramic processing.
IPS e.max all-ceramic
Ivoclar Vivadent (AG, Schaan, Liechtenstein) first developed IPS Empress which
is a leucite-reinforced glass ceramic. It is used with the hot-pressing technique that
involves the use of a precolored glass-leucite ingot that is heated and pressed into a
phosphate-bonded investment. Although, this technique produces a restoration with good
marginal adaptation, the strength of the material itself has limited its use to single unit
full-coverage restorations in the anterior segment (79-81); in the posterior segment it can
only be used as onlays or partial veneer crowns with 97.1% survival rate in 3 years (82).
9
The same company introduced IPS Empress 2, in 1998. It was a lithium-silicate
based glass ceramic (SiO2-Li2O) using the hot pressing procedure with in vitro mean
fitting accuracy of posterior crowns amounted to less than 50 µm (83). The survival rate
of this new all-ceramic material was found to be 100% for posterior single crowns and
70% for 3-unit FDPs, in the anterior and premolar area, in a 5-year prospective clinical
study (84).
IPS e.max lithium disilicate was introduced in 2005, as an improved hot-pressed
ceramic material, in order to expand the range of indications of the previously used IPS
Empress 2. This lithium disilicate is a glass ceramic that is composed of quartz, lithium
dioxide, phosphor oxide, alumina, potassium oxide and other components. The properties
that the material possesses include high flexural strength (360 MPa to 440 MPa), high
fracture toughness (2-3 MPa) and high thermal shock resistance due to the low thermal
expansion (85).
Lithium disilicate can be processed using either lost-wax hot pressing techniques
(IPS e.max Press) or CAD/CAM milling procedures (IPS e.max CAD). The pressable
lithium disilicate (IPS e.max Press) consists of approximately 70% needle-like lithium
disilicate crystals embedded in a glassy matrix. The desired color is controlled by the use
of homogeneously distributed polyvalent ions that are dissolved in that matrix (85). On
the other hand, the machineable lithium disilicate (IPS e.max CAD) consists of 40%
platelet-shaped lithium metasilicate crystals embedded in a glassy phase which is
produced after an “intermediate” crystallization process (blue, translucent state). The
color is again controlled by the use of coloring ions with the difference being the
oxidation state (intermediate phase); thus a blue color is produced. The final crystallized
10
state and desired tooth color is achieved during the post milling firing process in which
lithium metasilicate transforms into lithium disilicate (85).
There are several different IPS E.max ingots with different opacity and
translucency levels; high opacity (HO), medium opacity (MO), low translucency (LT),
and high translucency (HT). IPS e.max Ceram is the nano-fluorapatite layering ceramic
material that is provided by the manufacture in order to create more esthetically
acceptable restorations when HO or MO ingots are chosen (85).
The IPS e.max CAD blocks are partially crystalized with moderate strength and
easy to machine. The two levels of translucency depend on the crystallization pretreatment. The HT blocks contain few and large crystals of lithium metasilicate in the
pre-crystallized state, whereas the LT blocks contain a high density of small crystals (65).
As mentioned above, a disadvantage of all ceramic materials is the inevitable
combination of dissimilar materials (core and veneering porcelain) in order to achieve
optimum esthetics. With regard to that, lithium disilicate provides the option of a
monolithic/fully anatomical restoration fabricated exclusively from this material. This
produces a final restoration with high strength and good esthetics; however, surface
colorants or even a partial layering technique may still be incorporated in particularly
aesthetically demanding cases. Nevertheless, disadvantages, previously discussed, such
as chipping of the veneering porcelain, are eliminated (86). Additionally, Guess et al.
showed that IPS e.max CAD as a monolithic/fully anatomical configuration resulted in
fatigue-resistant crowns, whereas the IPS e.max ZirCAD veneered IPS e.max Ceram
crowns revealed a high susceptibility to mouth-motion cyclic loading with early veneer
failures (chipping) (87). Another, very recent, use of the IPS e.max CAD, that needs to
11
be mentioned at this point, is as the actual veneer material for zirconia frameworks.
Schmitter et al. assessed the ultimate load to failure of zirconia-based crowns veneered
with IPS e.max CAD (CAD-on technology), compared to the ones veneered using
conventional manual layering techniques (88). For the CAD-on technology, after the
zirconia framework and the veneer structure were milled separately, fusion ceramic (IPS
e.max CAD Crystal/Connect) was applied to the interior veneer surface and dispersed by
means of vibration. Then, the assembly of framework and veneer was joined by pressure
and vibration until the fusion ceramic mass was processed (i.e. turned flowable). At last,
fusion, crystallization and glaze firing took place. For the layering technique, the
framework was manually veneered using conventional veneering porcelain, which is
recommended for zirconia cores. The results showed that the CAD/CAM veneers were
non-sensitive to artificial ageing; with ultimate loads of failure for this particular material
being above 1600N, concluding that this type of material may offer a way to reduce
failures resulting from chipping of the veneering porcelain.
Etman evaluated the relationship between crack propagation and ceramic
microstructure following cyclic fatigue loading (89). The ceramics tested were AllCeram,
IPS e.max Press and Sensation. There was a statistically significant difference among the
three materials with the lithium disilicate material showing the highest resistance to crack
formation and propagation. This has been attributed to the crystalline phases which have
been reported to act as “crack stoppers” to prevent crack propagation.
Table 1, included in Wiedhahn’s paper, summarizes and compares some of the
properties of contemporary all-ceramics (90):
12
Glass-
Lithium-disilicate
Zirconia
Ceramic
VITA
IPS
IPS
IPS
IPS e.max ZirCAD/
MKII/IPS
e.max
e.max
e.max
InCeram YZ
CAD LT
CAD MO
Press
120-160
360+/-60
360+/-60
440+/-40
800-1000
1.2-1.4
2-2.5
2-2.5
2.5-3
5.5-5.9
50-75
70-80
80-90
70-80
94
no
no
yes
optional
yes
Empress
CAD
Flexural
strength
(3-point
MPa)
Fracture
toughness
(MPa m1/2)
Translucency
(CR Value
%)
Veneering
Cementation
Use
adhesive
conventional
Chairside/
Chairside/
Lab
Lab
Lab
conventional
Lab
Table 1. Properties of contemporary all-ceramic materials.
Lab
13
Longevity of all-ceramic restorations
Several studies reviewed the long-term performance of all-ceramic crowns by
comparing the different systems with each other or with the metal-ceramic prostheses.
However, different criteria, different methodologies and different statistical analyses
were used in the existing studies and do not allow for direct comparisons between them.
Pjetursson et al. published a systematic review of all-ceramic and metal-ceramic
crowns. After the exclusion criteria were applied, a final number of 34 (28 all-ceramics
and 6 metal-ceramics) studies were evaluated (91). The authors were surprised to find
that there were only 6 studies evaluating long-term survival of metal-ceramic restorations
available and moreover, that four of them had been published very recently. In metaanalysis, the 5-year survival of all-ceramic crowns was estimated to be 93.3% and 95.6%
for metal–ceramic crowns. All-ceramic crowns were also analyzed according to the
material utilized; Procera crowns showed the highest 5-year survival rate of 96.4%,
followed by reinforced glass-ceramic (Empress) and InCeram crowns with survival rates
of 95.4% and 94.5%, respectively. A significantly lower survival rate of 87.5% was
calculated for Empress crowns after 5 years. All-ceramic crowns were also grouped and
analyzed according to the position in the mouth. Lower survival rates were found when
crowns were seated on posterior teeth; for Empress crowns (84.4%) and InCeram crowns
(90.4%), this difference reached statistical significance.
In the same analysis, the most frequent complication for all-ceramic crowns was
core fracture, leading to 85% of the losses. With the exception of ceramic chipping, the
incidences of technical complications like loss of retention and ceramic fracture causing
loss of the crown were lower for metal-ceramic crowns than for all-ceramic crowns. On
14
the other hand, biological complications like caries, periodontitis and abutment tooth
fracture were more frequent in the metal-ceramic group, which is expected based on the
considerably longer exposure time of the metal-ceramic crowns (mean exposure time for
metal-ceramic crowns (9.2 years) was almost twice as long as that of the all-ceramic
crowns (4.9 years).
Guess et al. in a 5-year prospective clinical splitmouth investigation evaluated the
survival rate and long-term behavior of IPS e.max Press (IP) and ProCAD (PC) allceramic partial coverage restorations (PCRs) on molars (92). Forty PC and forty IP PCRs
were inserted in 25 patients. The modified United States Public Health Service (USPHSAlpha, Bravo, Charlie) criteria were used at baseline and after 13, 25, and 36 months
post-insertion. The Kaplan–Meier survival probability of the PC restorations was 97% (1
mandibular PC-PCR demonstrated an absolute failure by a clinically unacceptable
marginal ceramic fracture of the lingual-occlusal cusp area after a service time of 9
months). All IP restorations remained in situ indicating survival probability of 100%.
Regarding the criterion marginal adaptation, a distinct deterioration was found over time,
independently of the fabrication techniques and all-ceramic materials used; alpha ratings
decreased from 95% to 83.3% for IPS e.max Press and from 92.5% to 65.2% for ProCAD
restorations.
Etman and Woolford, in another study, compared Procera AllCeram and IPS
e.max Press to metal ceramic restorations, and the 3-year clinical evaluation indicated
similar success rates for all 3 groups (93). The modified United States Public Health
Services (USPHS) evaluation showed that the IPS e.max Press and metal-ceramic crowns
experienced fewer clinical changes than Procera AllCeram.
15
Fasbinder et al. evaluated the 2-year clinical performance of chairside (Cerec 3,
Sirona Dental Systems) lithium disilicate IPS e.max CAD all-ceramic crowns (94). They
found no crown fracture or surface chipping, indicating that monolithic lithium disilicate
CAD/CAM performed well after 2 years of service.
Marginal and internal fit of dental restorations
The accuracy of fit is the characteristic that is most closely related to the longevity
of a restoration (1, 2). Ideally the cemented crown should precisely meet the finish line of
the prepared tooth. In reality, clinical perfection is challenging to achieve and to verify.
The importance of a well-fitting full-coverage restoration can be illustrated most clearly
when considering the implications that occur with an ill-fitting restoration. Luting agent
dissolution (4), microleakage (3, 6), caries (2, 3, 6), hypersensitivity and periodontal
inflammation (5, 7) are the most common of such implications. Caries have been shown
to be the most common reason (36.8%) for crown failure according to a 3-year clinical
survey study by Schwartz et al. (2). Bader et al. found that plaque and calculus scores,
gingival inflammation and bleeding were significantly higher on crowned teeth than
uncrowned teeth (5). Reeves, also, reported that open margins and overhangs associated
with subgingival crown margin location were areas where chronic inflammatory response
and greater attachment loss could be expected (7).
Although White et al. reported that marginal opening alone did not directly
correlate with marginal microleakage (1), the accuracy of marginal fit is valued as one of
the most important criteria for the clinical quality and success of prosthetic restorations.
According to Holmes et al., “the fit of a casting can be defined best in terms of the
16
‘misfit’ measured at various points between the casting surface and the tooth” (18). The
definitions that they used to describe this “misfit” included internal gap, marginal gap,
vertical marginal gap, horizontal marginal discrepancy, overextended margin,
underextended margin, absolute marginal discrepancy and seating discrepancy.
Christensen found, using a linear regression prediction formula, that an acceptable
gingival margin range is 34-119µm (95). McLean and von Faunhofer, also, suggested
that restorations with marginal gap less 120µm are more likely to be successful (8).
Several studies have investigated the internal fit with regard to crown adaptation
(8-17). Specifically, Fusayama et al. showed that internal relief with either manicure
liquid or tinfoil (40µm thickness) improved the seating of complete cast crowns
regardless of whether a complete or partial relief was used (17). Eames et al. discovered
that a 25µm thickness of a die spacer not only improved the casting seating but also
increased retention by 25% (10). Grajower and Lewinstein said that the thickness of the
spacer should allow for the cement film thickness, roughness of the tooth and casting
surfaces, dimensional inaccuracies of the die and distortions of the wax pattern (11).
Wilson showed that there was a significant correlation between increased spacing and
decreased seating time and decreased seating discrepancy (12). He also concluded that
spacing of less than 40µm prevented the crown from seating well before the set of the
cement, which resulted in marginal discrepancy.
Olivera and Saito evaluated the effect of die spacer on the fit and retention of
complete cast crowns by using three different cements (13). They used four layers of die
spacer using three different techniques: covering the occlusal and 1/3 of the axial
surfaces, covering the occlusal and 2/3 of the axial surfaces and covering the entire
17
preparation except the apical 0.5 mm. The crowns were assigned to one of three luting
agents: resin modified glass-ionomer cement, resin cement and zinc phosphate. The
results showed that better marginal fit was obtained when the die spacer covered all but
the area 0.5mm short of the margin of the preparation; however after cementation the
resin modified glass-ionomer cement had the best fit with the same application of die
spacer.
Another aspect of the importance of the internal fit of the crowns is its effect on
fracture resistance of all-ceramic restorations. More specifically, Tuntiprawon and
Wilson evaluated the effect of increasing cement thickness (using platinum foil and die
spacer) on the fracture strength of all-ceramic crowns (14). Each crown was cemented
onto a metal die with zinc phosphate cement and loaded until fracture. They found that a
decrease in strength was observed with increase of cement thickness and the strength
decrease was possibly attributed to the greater deformation of the porcelain into the
cement as well as the decreased thickness of the crown itself.
Bottino et al. studied the cervical adaptation of metal crowns with regard to the
influence of cervical finish line, internal relief and cement type (15). They compared
three full crown preparations (chamfer, 135-degree shoulder and rounded shoulder),
internal relief of 30µm 0.5mm above the finish line vs. none, three types of cement (zinc
phosphate, glass-ionomer and resin cement). Significant influence of all three variables
tested was observed on the cervical adaptation. The least marginal discrepancy was
achieved with chamfer finish line, internal relief and use of glass-ionomer cement. Their
results showed that in order to optimize the cervical adaptation and enhance the complete
seating of the crown, creating a correct finish line, the use of a minimum thickness die
18
spacer 1 mm above the cervical line, using the cement with favorable flow and adequate
load application during cementation are all essential for a successful restoration.
A different factor that has been investigated by Ayad is the effect of tooth
preparation burs on the marginal adaptation (16). In that study diamond, tungsten carbide
finishing and crosscut carbide burs of similar shape were used in combination with
different luting cements: zinc phosphate cement (Fleck’s), glass ionomer cement (KetacCem), and adhesive resin cement (Panavia 21). Marginal fit was measured with a light
microscope in a plane parallel to the tooth surface before and after cementation. Results
revealed a statistically significant difference for burs used to finish tooth preparations,
whereas luting cement measurements were not significantly different. Ayad showed that
tooth preparations refined with finishing burs may favor the placement of restorations
with the smallest marginal discrepancies, regardless of the type of cement used.
Methods to measure the marginal gap
In the literature several techniques have been suggested for the measurement of
the marginal fit alone or in combination with the internal fit of crowns. All of these
present advantages and disadvantages, and a small description of the most commonly
used ones will follow.
To begin, the dental explorer is the most common tool used to detect marginal
adaptation, as it is often the only clinical instrument available. Hayashi et al. studied the
influence of the explorer tip diameter and the visual condition in evaluating vertical steps
and horizontal gaps (20, 21). A significant correlation was found between explorer tip
diameter and Alpha/Bravo boundary for horizontal gaps, but not for vertical steps. There
19
was no significant difference among the visual conditions tested. Apart from the explorer
tip, the amount of clinical experience seems to exert the greatest influence on the
identification of those gaps. The latter is further supported by another study, which
showed that operators with clinical experience had a threshold that detected crowns with
a smaller gap while maintaining a higher degree of consistency in their personal
judgment than did the operators without any clinical experience (22). This finding,
according to the authors, suggests that the use of the explorer is characterized by
subjectivity, introducing the bias of the investigator. Apart from that limitation, this
technique becomes even less accurate with subgingivally placed margins where,
according to Christensen, in an ideal environment, the acceptable mean opening of
subgingivally marginated cast restorations was shown to be almost 3.5 times the
acceptable mean opening of supragingival margins (95).
The radiograph could also be considered a tool that would provide information
with regard to the marginal fit of the crown; again most importantly during the clinical
practice. Assif et al. compared the tactile method (the use of explorer) to the use of
radiographs and to a technique using impression material in order to examine the
marginal fit (23). The results supported that neither the explorer nor the radiographs were
superior in detecting discrepancies, with the impression technique presenting the most
accurate data of the three.
A technique used in vitro is the classic destructive method of sectioning the
specimens and then studying them under an optical or scanning electron microscope (24,
25). The advantage of this technique is the accuracy and the precision in repeatability of
the measurements; however the obvious limitations of this method are the destruction of
20
the specimens which creates the need for duplicates, the limited area that is evaluated
since the sections have a minimum thickness and the additional steps that are required
(embedding in resin and sectioning).
Romeo et al. used a stereomicroscope under 50x magnification to measure the
marginal adaptation of CAD/CAM restorations (26). Photographs were taken under the
microscope and the measurements were performed with PC software. Despite the nondestructive nature of the method, which is very favorable, it is very technique-sensitive; a
slight deviation of the photographic angle will distort the measurement. Specifically,
because the microscope is set perpendicular to the margin of the restoration, it makes it
impossible to evaluate the marginal gap of an overhanging restoration (vertical overextension); thus, a 0µm value would not necessarily mean that the restoration has a
perfect fit.
Tan et al. used a similar setting (and therefore similar technique limitation) in
order to compare the marginal adaptation of CAD/CAM, wax/CAM and wax/cast
restorations (27). They took a 1:1 photograph of each of four sides of the die using a
digital camera mounted on a tripod. All photographs were taken sequentially with no
change in the horizontal inclination of the camera. Calibrated digital measurement
software was used to measure the marginal openings.
Gonzalo et al. measured the external marginal fit of zirconia vs. metal-ceramic
posterior FPDs with two different measurement methods: 1) An image analysis (IA)
system (software and microscope) and 2) A scanning electron microscope (28). The twoway repeated measures ANOVA showed significant interaction between measurement
method and material, with the measurements obtained with IA values being lower than
21
those obtained with SEM except from metal-ceramic FPDs. The authors concluded that
the measurement method was not independent of the material, and therefore a
standardized method to analyze marginal fit of full coverage restorations should be
established.
Mitchell et al. compared, in vitro, the marginal fit of 4 types of complete crowns
on human premolar teeth with the use of a nondestructive technique called profilometry
(29). This method determined whether the fit was influenced by type of the crown or
surface morphology of the tooth (grooved or ungrooved surfaces). It was found to be an
accurate method, but considering that this technique does not identify cases of vertical
overextension, the results once again are subjected to false interpretation.
A technique that has been suggested by Pelekanos et al. was the computerized xray microtomography, where multiple projections of an object were taken as the source
rotated around it (30). The projections were transferred to a computer and with special
software; small slices of the object’s internal structure could be added to the object’s 3-D
image. Advantages of this technique included the ability to produce images of the internal
structure of the specimen, in section form, while allowing for 3-D reconstruction, and the
possibility of obtaining very proximate sections. On the other hand, the disadvantages
that this method presented included the low capacity of discrimination of CT
microtomography in comparison with the optical or electron microscope, the possible
artifacts from refraction of the images from radiation, the compulsory radiopacity of the
material tested and the difficulty to define the materials that have different coefficients of
absorption.
22
The most commonly found nondestructive technique in literature is the replica
technique (RT) (31-37). Replicas of the intermediate space between the inner surface of
the crown and tooth surface are made by the method described by Molin and Karlsson
(31). The important characteristic of this technique is that it can be used in vivo as well as
in vitro since it does not involve the destruction of the specimens. Boening et al., using an
RT based on the previously mentioned study, measured in vivo the marginal fit of Procera
AllCeram crowns using a light body silicone to fill space between crown and tooth and a
heavy body silicone to stabilize the light body film (32). After removal from the artificial
crowns, the replicas were segmented, and measurements of the film thickness were
performed with a light microscope. The main limitation of this method is the distortion or
even the damage of the material during manipulation.
A very interesting study was conducted to evaluate the validity of the replica
technique after its wide use (96). The purpose of that study was to compare the film
thickness of the cement resulting from the cementation of Procera copings with the film
thickness obtained from the light body silicone using the RT. The RT, using a light body
silicone impression material instead of cement, was developed based on the assumption
the two materials behave in a similar way in terms of film thickness, despite the different
nature and different physical and mechanical properties that they possess (36). In that
study, replicas were fabricated by the technique described by Molin and Karlsson (31);
the same copings were cemented with glass-ionomer cement and then were sectioned. All
cuts produced by both techniques were measured under an optical microscope. The
results showed that the mean values measured with the RT were similar to the ones
measured using glass-ionomer cement, and no significant difference was established for
23
either the different groups (premolars and incisors) or the different areas (occlusal, axial,
and cervical) tested. Therefore, the authors concluded that the RT is accurate and reliable
for reproducing cement film thickness, and the use of this technique for the measurement
of crown gap spaces can be recommended.
More recently the measurement using the RT has changed. Luthardt et al.
developed an indirect technique in order to achieve 3-D analysis of the internal space
between the crown and the metal master die (38). The method used gypsum duplicate
dies along with silicon films (replicas) that represent the internal surface of the crowns,
which were, then, digitized using the same measuring position.
As technology evolved further, a new method of 3D fit assessment for dental
restorations has been proposed. Holst et al. developed a new triple-scan protocol; using a
non-contact scanner, three scans were performed: 1) Coping solo, 2) Master cast solo and
3) Coping placed on master cast in a clinically correct final position (97). After the
objects (coping and master cast) were digitized, surface tessellation/triangulation
language (STL) surfaces were generated from point clouds with the scanner software
(ATOS system, GOM mbH, Braunschweig, Germany). First, the master cast STL and the
coping-master cast STL were registered by manual alignment followed by best-fit
registration. Then the same was done to match the coping and coping-master cast. The
coping-master cast data were deleted and the aligned coping-master cast data were used
for fit assessment. To measure the cement gap, the outer surface of the coping was
deleted, followed by reversion of the surface normal of the intaglio of the coping and
calculation of deviations from the master cast. The investigators obtained the mean value
of the cement space for 50 copings on their respective abutments and they repeated the
24
measurement three times. Their results showed no significant differences among these
measurements (p=.170), Pearson correlation coefficient revealed almost perfect
associations (r=1) and intraclass correlation coefficient also revealed almost perfect
coefficient for repeatability (r=0.981, p<.001).
The same main investigator used this protocol in order to assess the precision of
fit of CAD/CAM dental implant superstructures (39). The statistical analysis, again
similar to the previous study, resulted in an intraclass correlation of 0.991 (95%-CI
between 0.978 und 0.998) and therefore a statistically significant repeatability of
measurements (p<0.001, F = 112.95). Both of those studies proved that the triple-scan
protocol was a highly reliable approach in order to evaluate the 3D fit of both
conventional and implant retained restorations. The disadvantages of 2D measurements
were eliminated, while the advantages of the non-destructive approach of this method
made it a superior alternative for future dental research.
The one inherent problem of all non-contact optical digitizers is the accuracy and
capability to actually capture the different surfaces/materials. Usually for highly
reflective or translucent materials (such as all-ceramic crowns) the surfaces need to be
coated with a contrast agent which may introduce error. However, for comparative
studies the absolute values might not be of great importance.
Where high accuracy measurements are needed, a high precision coordinate
measurement machine (CMM) integrated with 3D laser scanning system should be used
(98). That non-contact measurement method consists of a laser sensor that is mounted to
a 3-6-axis computer controlled positioning system (i.e. CMM). The Surveyor ZS-Series
scanner with scan accuracy (accuracy describes how closely the measurements of the
25
laser conform to the true dimensions of the object being measured) of +/- 0.00898mm
(Laser Design Inc, GKS, Minneapolis, MN, USA) is such a system that was used in this
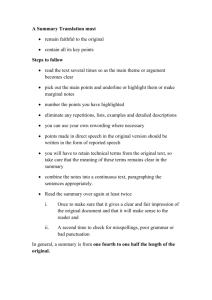
study. The principal behind the laser scanning is called Laser Triangulation, (Figure 1).
Laser triangulation is an active stereoscopic technique that computes the distance of an
object with a directional light source and a video camera. A laser beam is deflected from
a mirror onto a scanning object. The object scatters the light, which is then collected by a
video camera located at a known triangulation distance from the laser. Using
trigonometry, the 3D spatial (XYZ) coordinates of a surface point are calculated. The
charge-coupled device (CCD) camera’s 2D array captures the surface profile’s image and
digitizes all data points along the laser (98).
Figure 1. Laser Triangulation. Available from:
http://www.laserdesign.com/resources_and_downloads/faq/
26
The shape of the single “2D” profile is recorded by the digital CCD and
subsequently, based on the calibration and look up tables of the lasers; a Z position is
determined and stored for each pixel value by the software. This location along with the
machine axes positions are used to compute the X,Y,Z coordinates of the points along
that profile. Hundreds of thousands of similar profiles are thus collected as the probe
sweeps over the object and the software stores this information into a database for later
retrieval. Each profile comes into the database as a single polyline entity with points
distributed along the length of the line. These polylines are displayed graphically on the
computer screen as they are gathered (98).
Once the data (points) are acquired Digital Shape Scanning and Processing
(DSSP) is applied using sophisticated processing software (i.e. Geomagic Qualify 12,
Geomagic, Research Triangle Park, NC, USA) (99). DSSP is based on two main
technology developments: scanners and other hardware to capture point data and
software to process the data into useful forms. Each point measurement is subject to a
wide variety of measurement errors. While sources of error (contamination on the part,
vibration, operator error, etc.) are on the same order of magnitude as traditional
measurement methods, the sheer volume of point cloud data requires sophisticated
algorithms to catch problems, such as minute surface defects, and properly register the
entire shape. Point cloud data may be converted to an accurate polygonal mesh or a
surface representation (typically NURBS, used by most CAD systems) (99).
27
Subsequently, the 3D digital object can be processed and analyzed accordingly;
automated reports, including 3D PDF, numeric inspection data, annotated user-defined
views, notes and conclusions may be generated (100).
A synopsis of a flow diagram using this method includes:
Test object > 3D scanning > Scan processing and merging > CAD object > Aligment >
Comparison > Evaluation > Reporting (Statistics database, Print, Online) (99).
In summary, the measuring techniques used for marginal and internal fit of
crowns were categorized by Sorensen (1990) as follows: 1) Direct view, 2) Crosssectional, 3) Impression technique, and 4) Explorer and visual examination (19).
However, with the advancement of the technology, new categories will be added. By
digitizing the specimens (dies, silicon films or even the intaglio of the crown itself), the
data sets acquired allow for several measurements and comparisons.
Marginal adaptation of all-ceramics
Despite the great variety of available restorative materials, the cast restorations
continue to be considered the gold standard for vertical marginal adaptation (101, 102).
Holden et al. compared a traditional metal-ceramic restoration (MCR) fabricated from
feldspathic porcelain fused to metal, a leucite-glass ceramic pressed to metal restoration
(PTM) and a restoration from all leucite-glass-pressed ceramic (PCR) with porcelain butt
joints (69). All restorations were evaluated on their respective dies at 45x magnification
using an Olympus SZX-12. The results showed that the MCR group had the highest
values with regard to marginal openings, whereas the PTM group showed the best
marginal adaptation. The restorations with pressed ceramic margins may be less
28
technique sensitive for the laboratory to fabricate when compared to the traditional metalceramic and that may be the reason for the difference on the adaptation.
Yeo et al. evaluated, in vitro, the marginal discrepancies of 3 different all-ceramic
crown systems (Celay In-Ceram, conventional In-Ceram, and IPS Empress 2 layering
technique) in comparison to a control group of metal ceramic restorations using an
optical microscope (103). The results indicated that the IPS Empress 2 system showed the
smallest and most homogeneous gap dimension, whereas the conventional In-Ceram
system presented the largest and more variable gap dimension compared with the metal
ceramic (control) restoration.
Baig et al. compared the marginal fit with respect to gap and overhang, at 6
designated margin locations of zirconia (Cercon Y-TZP) ceramic crowns to lithium
disilicate pressable (IPS Empress II) and complete metal crowns (control group) using a
computerized digital image analysis system (72). It was found that the mean marginal gap
for those three groups was 66.4µm, 36.6µm and 37.1µm, respectively. The 2-way
ANOVA revealed significant differences in marginal gap between the machinable
ceramic (Cercon) and pressed ceramic system (IPS Empress II) and complete metal
crowns (control). The significantly higher marginal gap of the Cercon crowns compared
to IPS Empress II crowns was attributed to the type of manufacturing of these two
ceramic systems. Specifically, the distortion of the ceramic coping was thought to be less
in IPS Empress II compared with Cercon, as the pressed technique involves a less
complicated process, using a more manual than computer program computation, and is
process dependent.
29
Stappert et al. investigated the marginal fit of IPS e.max Press material by
fabricating partial coverage restorations on teeth with different preparation designs (104).
The restorations were adhesively luted and exposed to a mastication simulator. The
discrepancies of the marginal fit were examined on epoxy replicas before and after luting
as well as after masticatory simulation at 200x magnification. The authors found that
before cementation the mean (geometrical) marginal gap width consistently decreased as
the dimensions of the restorations increased (mean range 84.3-50.3µm), the cementation
increased the marginal gap of most of the groups except one (mean range 104.7-93.8µm)
and the masticatory loading increased the gap of all groups but significantly only to two
preparation designs (mean range 117.5-106.1µm). The conclusions of this study point out
that the IPS e.max Press (VP 1989) can be used to fabricate inlays and partial crowns
which meet the requirements in terms of a clinically acceptable marginal gap, irrespective
of the preparation design used, given that all mean marginal gaps were below 120µm.
However, the preparation design and dimensions of the restorations appeared to affect the
initial marginal fit and escape of luting material during the cementation process.
In another study, Stappert et al. evaluated the marginal accuracy of partial
coverage restorations under mouth-motion fatigue and thermal cycling (73). The
materials tested were: gold (GO), hybrid composite (Targis) (TA), IPS e.max Press (EX),
IPS-Empress (EM) and ProCAD/Cerec( PC). After the cementation the mean marginal fit
was: GO-47 [43–51]µm, TA-42 [38–45]µm, EX-60 [52–67]µm, EM-52 [45–60]µm and
PC-75 [59–94]µm, indicating that IPS e.max Press had similar marginal fit to gold and
IPS-Empress, whereas the ProCAD group demonstrated poorer marginal fit. Similar
results were found after the aging test (GO-42 [38–45]µm, TA-42 [38–47]µm, EX-56
30
[49–65]µm, EM-54 [46–64]µm and PC-71 [59–84]µm) without compromising the
marginal fit of the restorations under the given testing conditions.
Dental impressions
The dental impression is of great importance in dentistry in general, and in fixed
prosthodontics in particular. The materials and techniques have gone through major
evolution throughout the years. At the beginning, rigid materials including zinc oxide
eugenol paste, wax, modeling compound and impression plaster were used. Because of
the obvious rigidity, distortion and breakage that occurred, their use was significantly
reduced during the later years. In the 20th century, elastomeric materials were introduced.
They are classified as aqueous and non-aqueous elastomers. The first category consists of
the reversible hydrocolloid (agar) and the irreversible hydrocolloid (alginate). Agar is
dimensionally unstable thus casts must be poured immediately. Alginate is the most
commonly used material for diagnostic impressions, mainly because it is inexpensive.
However, it is also dimensionally unstable and it must be poured within 10 minutes (40).
The second category, non-aqueous, consists of polysulfides (1950), condensation
silicones (1955), polyethers (1965) and addition silicones (1975). Polysulfides were also
called “rubber base”; they reproduced details with excellent results, were not rigid and
captured subgingival margins but they were dimensionally unstable, did not have good
elastic recovery and had long setting time. For the condensation silicones, the release of
ethyl alcohol during polymerization that causes shrinkage was the main disadvantage.
However, it was shown that this shrinkage was greater in the low viscosity than in the
putty-like viscosity. Polyethers are hydrophilic (contact angle 49 degrees); thus they have
31
superior detail reproduction in the presence of moisture. They are, also dimensionally
stable and they provide an excellent reproduction of detail. However, strict disinfection
guidelines should be respected in order to prevent expansion. Also, their rigidity makes
them more difficult to remove than addition silicones and more likely to fracture delicate
gypsum dies. Addition silicones, Polyvinyl siloxanes (PVS), have become the most
widely used impression material in dentistry (42). They have the best detail reproduction
and elastic recovery of all available materials, and their dimensional stability allows
multiple pours; thus, PVS materials are the materials of choice in fixed prosthodontics
(42, 43). They are moderately rigid, have good tear strength, relatively short setting time
and can be used with most disinfection protocols. Their disadvantages include
susceptibility to contamination as a result of sulfur and sulfur compound and hydrophobic
behavior (contact angle 98 degrees) caused by hydrophobic aliphatic hydrocarbon groups
around the siloxane bond. Today, in order to overcome this, nonionic surfactants
(nonylphenoxypolyethannol homologues) have been incorporated and the new PVS
materials, have improved wettability (contact angle 53 degrees); however they are still
clinically acceptable only in dry conditions (41).
According to the ANSI/ADA Specification No. 19 (ISO 4823) regarding detail
reproduction, all elastomeric materials, except from very high-viscosity products, should
reproduce a V-shape groove and a 0.02mm wide line (41). Walker et al. evaluated the
detail reproduction of polyether and PVS material by observing the continuous
replication of at least two out of three horizontal lines (105). The impressions were made
under dry and moist conditions. They found that under dry conditions all materials
produced satisfactory detail reproduction 100% of the time; however under moisture only
32
29% of PVS materials produced satisfactory detail while 100% of polyether met the
detail criteria.
Dimensional stability over time allows the operator to pour the impression at any
time. Thongthammachat et al. evaluated the influence on dimensional accuracy of dental
casts made with different types of trays and impression materials when they were poured
at different and multiple times (53). The researchers concluded that an impression made
from polyether should be poured only once within one day after impression making
because of the distortion of the material that occurs over time. Addition silicone
impression materials had clearly better dimensional stability than polyether up to 720
hours which is in agreement with previous studies (46, 47). In the study, addition silicone
also showed deviations increasing over time, but these were relatively small. The
possibility of imbibiton should be considered- especially with polyether impression
materials- due to the fact that polyether absorbs water from the gypsum and swells with
each successive pour.
Elastic recovery allows the material to return to its original dimensions when the
impression is removed from the mouth. No contemporary material has 100% elastic
recovery. PVS materials have the best elastic recovery at over 99% with a specific test
undercut (106).
In addition to the material, the impression technique is a factor that has been
studied with relation to the influence on the success of the impression. Hung et al.
reported that the accuracy of addition silicone was affected more by the type of materials
than by the technique (48), while Johnson and Craig stated that accuracy could be better
controlled with technique than by the material itself (45). The findings in the latter study
33
indicated that impressions made in stock trays, that is, the putty wash two-step technique
with polyethylene spacer, were as accurate as those for impression techniques in custom
trays.
The use of custom tray versus a stock tray is a controversial issue. The rationale
behind the need for custom tray is that it provides the essential uniform thickness of the
impression material with different researchers suggesting different amount of space (1 to
5 mm). Although custom trays have been recommended to produce more accurate
impressions, stock trays remain popular because they are readily available and easy to
use. Valderhaug and Floystrand reported no significant difference in the linear
dimensional stability of impressions made from custom and stock trays, even when the
thickness of the material ranged from 2 to 9 mm (50). Rueda et al. examined the
dimensional stability of several impression materials made from stock and custom trays
by measuring the linear dimensions of the casts poured at 1 hour, 1 day and 1 week (51).
There was a significant but very small difference in the linear dimensions of the casts
produced with both impression materials using stock and custom tray (dimensions varied
form 15 to 50 µm). The least amount of variation was noted when 2.0- 2.5 mm of spacer
was used. Thongthammachat et al. also showed that if stock trays were properly oriented
and the impression thickness was uniform, stock trays could give a better result than
custom trays (53).
The influence of dimensional change of the impression tray upon the accuracy of
the impression material has been reported as well as the time when the adhesive should
be applied ranging from 5 minutes to 48 hours, with the 48hr adhesive drying time
exhibiting the highest mean adhesive tensile bond strength (52).
34
In Donovan and Chee’s review article three approaches to putty/wash impressions
were presented (42). For the first approach, putty material was used to fabricate the
custom tray by making an impression of the diagnostic cast. For the second, a preoperative putty impression was made intraorally, material was removed from the
embrasures and a “wash” impression with low-viscosity material was made. The third
approach involved “simultaneous” technique using a tray loaded with putty and a syringe
with low viscosity used around the teeth. According to Chee and Donovan, the third
approach is unacceptable because it is impossible to control the thickness of the
impression material and what material records the margin detail of the preparation (44).
Mishra and Chowdhary tested the following different impression techniques using
polyvinyl siloxanes- group 1: putty wash two-step technique with polyethylene spacer,
using a stock tray; group 2: putty wash one-step technique, using a stock tray; group 3:
single-mix technique, utilizing medium viscosity in a custom tray; group 4: multiple-mix
technique, utilizing a heavy and low-viscosity combination in custom trays (49). The oneway ANOVA revealed that all of the dimensions tested (anterior-posterior, lateral and
vertical) were significantly different among the impression techniques. The findings of
this study showed that group 4 produced the most accurate result in the anterior-posterior
and vertical dimensions, followed by group 1 in the anterior-posterior dimension, and
group 3 in the vertical dimension. Groups 1 and 3 were the most accurate in the lateral
dimensions. Group 2 produced the least accurate results in all dimensions. The accuracy
of group 4 was attributed to a controlled amount of bulk of impression material and
adhesive systems and low polymerization contraction with the heavy-body material,
compared with the light-body products due to a greater concentration of inert fillers. The
35
increased lateral dimension, as compared to the master model that was found for group 4
was possibly due to the contraction of the impression material toward the tray. According
to Eames and Sieweke (107) and Lewinstein (108), the impression material contraction
toward the tray wall may produce stone dies wider horizontally (interabutment) and
shorter vertically.
In summary, several materials and techniques have been used for impressing soft
and hard oral tissues. All present advantages and disadvantages; knowledge and
experience lead to proper selection and successful results.
Dental plaster and stone
Gypsum products are widely used in dentistry. Dental plaster, stone, highstrength/high expansion stone, and casting investment constitute this group of closely
related products. All forms are derived from natural gypsum deposits with the main
difference being the manner of driving off part of the water from the calcium sulfate
dihydrate. The most important and well-organized theory for the mechanism of the
setting is the crystalline theory; the setting reaction of the water with calcium sulfate
hemidrate to form calcium sulfate dihydrate caused by the difference in solubility
between those two components. Regardless of the type of gypsum product employed, an
expansion of the mass can be detected during the change from hemidrate to dihydrate.
Depending on the composition of the gypsum product, the observed linear expansion may
be as low as 0.06% to as high as 0.5%. On the other hand, if equivalent volumes of the
materials used for this reaction are compared, the volume of the dihydrate formed will be
less than the equivalent volumes of the hemidrate and water; thus a volumetric reaction
36
should occur during setting. However, a setting expansion is observed and this
phenomenon can be rationalized on the basis of the crystallization mechanism. This
expansion is affected by multiple factors such as water to powder ratio, spatulation (speed
or time), temperature (water and environment), humidity, presence of colloidal systems
(agar and alginate) and pH (such as saliva) (41).
According to the ANSI/ADA Specification No.25 (ISO 6873) there are 5 types of
gypsum (41). Type I is the impression plaster, but it is rarely used today because less
rigid impression materials are available. Type II is model plaster, which is now used in
prosthodontics principally to fill flasks in denture construction, where setting expansion,
is not critical. Type III, dental stone, has a minimum one-hour compressive strength of
20.7MPa, but it does not exceed 34.5Mpa. Type III gypsum can be used for diagnostic
casts. Type IV is high-strength/low expansion dental stone and it is used for die stone,
which needs strength, hardness, abrasion resistance, and minimum setting expansion.
Type V is a high-strength/high-expansion dental stone. Setting expansion is increased
from a maximum of 0.15% to 0.30.
Several physical properties should be taken into consideration when a die material
is used, such as linear dimensional change, detail reproduction, surface hardness,
abrasion resistance and transverse strength. Kenyon et al. compared the linear
dimensional accuracy of 7 die materials including Vel-Mix (Type IV), Hard Rock (Type
V), Resin Rock (Type IV- resin impregnated), Die Epoxy fast set (Epoxy resin), ModelTech (Polyurethane resin), Integrity (Bis-Acryl Composite) and Copper-plated (109).
Resin Rock and copper-plated dies most closely approximated the dimensions of the
master die and were not significantly different from each other in any of the three
37
measurements but they were significantly different from the other 5 for at least one
measurement. Type IV and V dental stones exhibited setting expansion within the range
appropriate for gypsum.
Both impression material and die material are essential for the production a
consistent and reliable cast or die. The fit and the ultimate clinical success of an indirect
restoration depend on the accuracy of the die reproduction, which is subject to possible
deformation during the prosthesis fabrication process. Ragain et al. compared the detail
reproduction, contact angle and surface hardness between various combinations of
contemporary elastomeric (PVS, condensation silicon, polyether, polysulfide and
reversible hydrocolloid) and die materials (Type IV, V and Resin-reinforced Type IVResin Rock) (110). According to the findings of this study, when using PVS or polyether,
a Resin Rock stone may produce dies that have less scratch resistance on the surface than
the Type IV die stone. Overall, no combination was identified to be superior for all the
parameters tested.
Casts and die materials must reproduce an impression accurately and remain
dimensionally stable under normal storage and usage conditions (41). The particular
impression material used and the purpose that is made for, determine the selection among
the gypsum products.
Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM) systems
The clinical success of the all-ceramic restorations depends not only on the
mechanical and physical properties of the materials used but also on the precision of the
particular computer-aided-designed/computer-aided-manufacturing systems used to
38
fabricate those restorations. The application of CAD/CAM systems in dentistry had
initiated as early as 1970s by Duret and colleagues, but it was not until the 1980s when
Mormann and colleagues developed the CEREC system, that they gained popularity (74,
111). Today, a rapidly increasing number of milling systems have established themselves
on the dental market (57, 74). Some of them are:
•
Cercon smart ceramics (DeguDent Frankfurt GmbH)
•
CEREC inLab (Sirona Dental Systems, LLC, Charlotte, NC, USA)
•
DCS Dental (DSC Dental AG, Allschwil, Germany)
•
E4D (D4D Technologies, Richardson, TX. USA)
•
Etkon (etkon AG, Gräfelfingen, Germany)
•
Hint Els DentaCAD systeme (Hint-Els GmbH)
•
KaVo Everest (KaVo Dental GmbH, Biberach, DEU)
•
LAVA (3M, St. Paul, MN, USA)
•
Nobel Biocare Procera (Nobel Biocare, Yorda Linda, CA, USA)
•
Wieland Zeno (Wieland Dental and Technik GmbH & Co. Pforzheim,
DEU)
•
ZirkonZahn (GmbH, Gais, Italy)
and many more (57, 74).
Beuer et al. presented an overview of the parameters of available contemporary
CAD/ CAM systems (56).
To begin with, the components of all CAD/CAM systems include:
1. The scanner, which is the tool that measures tooth, structures and transforms them
into digital data sets. Two categories of scanners are available the optical and the
39
mechanical ones. The optical scanners use the triangulation procedure, as
described above, which consist the majority of the contemporary scanners in
dentistry. The mechanical scanners use a ruby ball to measure the threedimensional object. The only scanner in this category is the Nobel Biocare
Procera one (Nobel Biocare, Yorda Linda, CA, USA).
2. Design software that can design the crown and fixed partial denture framework or
the fully anatomical restorations.
3. The processing device where the restoration will be milled. Those devices are
categorized based on the number of milling axes.
a. The 3-axis milling device has degrees of movement in the three spatial
directions defined by the X -, Y -, and Z – values. The calculation
investment is minimal, but a milling of subsections, axis divergences and
convergences is not possible. All 3-axis devices used in the dental area can
also turn the component by 180° in the course of processing the inside and
the outside. The advantages of these milling devices are short milling
times and simplified control by means of the three axes. Such devices are:
inLab (Sirona), Lava (3M ESPE), Cercon brain (DeguDent).
b. The 4-axis milling device has the three spatial axes as well as a rotatable
tension bridge which helps to adjust bridge constructions with a large
vertical height displacement into the usual mold dimensions and thus save
material and milling time. Example: Zeno (Wieland-Imes).
c. The 5-axis milling device in addition to the three spatial dimensions and
the rotatable tension bridge (4th axis), gives the possibility of rotating the
40
milling spindle (5th axis), which enables the milling of complex
geometries with subsections. Example in the Laboratory Area: Everest
Engine (KaVo). Example in the Production Centre: HSC Milling Device
(etkon).
The authors stated that the increase of the number of axes does not increase the quality of
the restoration which is much more dependent on the result of the digitalization, data
processing and production process.
Depending on the location of the components of the CAD/CAM systems the
production can either be chairside, laboratory or centralized fabrication in a production
center.
The processing can be dry (i.e. Wieland Zeno, LAVA and Cercon smart ceramics)
or wet (i.e. KaVo Everest, Zeno 8060, inLab (Sirona), E4D).
The materials that can be milled with those devices are metals (titanium, titanium
alloys and chrome cobalt alloys), resin materials, silica-based ceramics (especially
lithium-disilicate ceramic blocks that are used for fully anatomical crowns, copings for
crowns and anterior FPD frameworks), infiltration ceramics (Vita In-Ceram Alumina,
Vita In-Ceram Zirconia, VITA In-Ceram Spinell) and aluminum and yttrium-stabilized
zirconium oxide blocks (56).
The CAD/CAM technology can be used either with fully sintered ceramic blocks
(hard machining) or with partially sintered ceramics (soft machining) (65). Lithium
disilicate (IPS e.max CAD) along with feldspar-based and leucite-based ceramics are the
available materials used in hard machining, while partially-sintered zirconia blocks are
used in soft machining.
41
McLaren and Terry reported that the poor marginal and internal fit of the
restorations produced by the early CAD/CAM systems was due to the low resolution
scanning and inadequate computing power of those systems and not to the ceramic
material itself (71).
Shannon et al. compared the absolute horizontal marginal adaptation of
zirconium-dioxide cores fabricated from seven contemporary dental laboratory based
CAD/CAM systems: KaVo Everest, Nobel Biocare Procera (MOD40, Piccolo, Forte
scanners), 3M ESPE Lava, Wieland Zeno and Sirona CEREC (112). Standardized digital
photographs were taken of each core on the master die. All the systems except one
resulted in cores that were over-extended requiring adjunctive procedures to produce
acceptable all-ceramic crowns, which showed that there was area for further
improvement.
Tan et al. evaluated the vertical marginal openings of the cast, CAM and
CAD/CAM restorations (27). The last were titanium restorations fabricated using the
scanning and crown design modules of the KaVo Everest system. The CAM titanium
restorations were made with the double-scan technique with the same system, and the
cast restorations were fabricated using the conventional lost wax technique. Digital
photos were taken and the openings were measured with digital software program. The
results revealed the following mean vertical openings: CAD/CAM 79.43µm, CAM
73.12µm, cast 23.91µm. This study found that the cast restorations had a significantly
smaller vertical marginal gap compared to both the CAD/CAM and CAM groups.
Lee et al. evaluated the marginal and internal fit of all-ceramic crowns
manufactured by conventional double-layer type (high-strength core) CAD/CAM system
42
(Procera) versus single layer type (without a core-the entire crown is CAD/CAMed)
system (Cerec 3D) (70). For the marginal fit, the crowns and the copings were positioned
on the die and the distance between each crown’s margin and the metal die was recorded
at 50 points randomly using a measuring microscope at a magnification of 100x. For the
internal fit, silicon paste was used and the gap was calculated based on the surface area of
the abutment and the weight and density of the silicone material. Comparing separately
the coping and the crown for the first system, it was shown that the marginal discrepancy
width of Procera crowns (89.6±9.5 µm) after porcelain firing showed significantly larger
gaps than Procera copings (72.2±7.0 µm). This was attributed to the negative effect of
double-layer type CAD/CAM system where porcelain was added to the coping. There
was no statistically significant difference in maginal fit between Procera and Cerec 3D,
but there was difference in the internal fit. Nevertheless both systems produced crowns
within the clinically acceptable range.
An important aspect/limitation of the CAD/CAM restorations that needs to be
mentioned is the potential for machining-induced damaged and more specifically
marginal chipping. Tsitrou et al. conducted a study in order to investigate any possible
correlation between the brittleness index (BI) of machinable dental materials and the
chipping factor (CF) of the final restorations (113). The BI is the machinability of a
material that can be simply assessed qualitatively as the ease with which a given material
is cut. The CF is an estimation of the degree of marginal chipping, which can be derived
by estimating the ratio of overall marginal chipping over the total marginal circumference
of the restoration multiplied by 100. The materials tested were Paradigm MZ100TM
(3M/ESPE), Vita Mark II (VITA), ProCAD (Ivoclar-Vivadent) and IPS e.max CAD
43
(Ivoclar-Vivadent) milled in CEREC system (Sirona Dental Systems Gmbh, Bensheim,
Germany). Tsitrou et al. showed that the CF increases as the BI increases, with Paradigm
MZ100 having the lowest BI and CF, and IPS e.max CAD demonstrating the highest BI
and CF.
Following on from that study, Giannetopoulos et al. investigated whether the
CAD/CAM system would influence the marginal integrity of IPS e.max CAD copings
made with different finishing lines (114). Cerec inEOS system/Cerec 3D software and
KAVO Everest system were compared. The finish lines were 60-degree bevel, 30-degree
bevel and 0-degree bevel (or 90-degree shoulder). The CF was calculated, as in the above
study(113); the CF was increased as the bevel angle increased for Cerec group, whereas
this factor did not influence the marginal integrity for the Everest group. The conclusions
of the study were that different milling processes produce different amount of marginal
chipping, although that was apparent only for the 60-degree bevel.
Since the introduction of CAD/CAM technology in dentistry, more than 20 years
ago, much advancement has been made regarding the milling process of dental
prosthesis. Research on this field is dynamic at this point of time, and new technologies
with new potentials are introduced continuously.
Stereolithography (SLA)
Stereolithography (SLA), a typical modality of rapid prototyping (RP), is a
relatively new technology that produces physical models from computer-aided design via
3D printers (115). Out of all the RP technologies available, the most commonly used for
medical applications are stereolithography and 3D printing (3DP). Stereolithography is a
44
process by which liquid UV-sensitive resin contained in a vat is polymerized via UVlaserbeam into solid resin, which comprises both the 3D model and support pillars, which
help maintain the structural integrity as the model is being created. The model is then
rinsed in alcohol and again polymerized in a UV chamber. Afterward, the support pillars
must be separated from the model by hand.
Although RP has been used in the field of industrial design for decades, only in
the last decade have applications been developed for medicine and dentistry. This is
attributable to the advantages that the technology provides which include fast model
fabrication, the ability to use various raw materials and diverse finishing techniques, and
the capacity to produce complex 3-D models (115). Those models already serve in the
diagnosis, treatment and operation planning in oral and maxillofacial surgery including
malformations, craniofacial surgery, tumor surgery, traumatology, orthognathic surgery
and implantology (116). Even more recently, this type of model was incorporated in
fixed prosthodontics with the introduction of the digital impressions. Lava™ C.O.S.
(Lava™ Chairside Oral Scanner, 3M Lexington, USA) works with stereolithography
apparatus (SLA) technology to produce the models derived from its data.
Ogledzki et al. compared the accuracy of full-arch dental models from a digital
intra-oral scanning system, the Lava™ C.O.S. to those produced using traditional 3M
PVS impression materials cast in type III stone (117). The SLA and the stone models
were scanned using the Lava desktop model scanner to produce digital image
representations of the casts. Geomagic Studio (Geomagic, Research Triangle Park, NC,
USA) graphical analysis software compared the digital images of the casts to digital
reference images provided by an independent agent who conducted a laser scan of the
45
original metal models. The results showed no significant difference in models produced
using either the intra-oral scanning system or traditional PVS materials.
Moore et al. determined to what extent the micro layer steps resulting from the
additive process of SLA models were transferred to the margins of copings used in metalceramic crowns (118). Nine cast chrome-cobalt prepared dies were scanned using the
Lava™ C.O.S.; SLA models were created and metal copings were manufactured. Four
locations per coping were randomly selected and microscopic photographs were taken of
the SLA model and coping interface. The margins of the chrome cobalt teeth
preparations, SLA models and copings were digitally traced on the micrographs. It was
found that 25 of a total of 36 margins locations had no steps in the SLA model. Only
three of those locations were the steps transferred to the metal coping, which gave a
stepped appearance. The remaining transfers showed slight transfer to the copings with
rounded wave-like appearance. The authors concluded that there was only a very slight
correlation (approximately 8%) between the micro layers on the SLA models and
marginal characteristics.
Digital dental impressions
The CAD/CAM technology has been used in dentistry for several years, but its
application was limited mainly to the dental laboratory environment. The first clinical use
of this technology was introduced more than 20 years ago, when the first intraoral
scanner was created. Today, technical evolution is rapid with new scanners for dental
impressions entering the common clinical practice continuously. The claimed advantages
of digital impressions which may make the conventional impression technique obsolete
46
include accuracy of fit, time and cost savings, lab and dentist benefits and improved
communication as well as patients’ comfort and acceptability. A concise and comparative
table with all the current intraoral scanners is presented in Logozzo’s et al. and Scotti’s et
al. studies (Table 2) (54, 55). The scanners that are not included in that table are the new
models of 3M ESPE (i.e. True Definition Scanner) and of Sirona Dental System (i.e.
CEREC® AC- Omnicam).
For this study, two of those scanners were used; the Lava™ C.O.S. and the E4D.
A basic description of the science behind those two scanners will follow as presented on
the manufacturer’s brochures and on-line sites as well as scientific papers:
Company
Sirona Dental System
GmbH (DE)
Cadent Inc (IL)
D4D Technologies, LLC
(US)
3M ESPE (US)
IOS Technologies, Inc (US)
Densys Ltd (IL)
Dimensional Photonics
International, Inc (US)
MHT SpA (IT)-MHT Optic
Research AG (CH)
Hint-Els GmbH (DE)
3Shape A/S (DK)
Intraoral
scanner
CEREC®ACBluecam
iTero
E4D
Lava™ C.O.S.
IOS FastScan
MIA3d
DPI-3D
3D Progress
directScan
Trios
Confocal microscopy
Stereoscopic vision
Confocal microscopy and
Moire̩ effect
Accordion fringe
interferometry (AFI)
Active
stereophotogrammetry
Active triangulation and
Schleimpflug principle
Active wavefront sampling
Optical coherence tomography
and confocal microscopy
Parallel confocal
microscopy
Active triangulation and
optical microscopy
Working principles
Not disclosed
Not disclosed
Not disclosed
Wavelength 350500 nm
Visible light
Laser
Pulsating visible
blue light
Laser
Red laser
Visible blue light
Light source
Multiple
images
Multiple
images
3
images
Multiple
images
2
images
3
images
Video
Multiple
Multiple
Multiple
images
Imaging
type
None
Not
discloses
Occasional
None
Yes
Yes
Yes
Occasional
None
Yes
Coating
No
No
No
No
No
No
No
Yes
No
Yes
In-office
milling
Proprietary
or STL
Not
disclosed
STL
STL
ASCII
STL
Proprietary
Proprietary
Proprietary
or selective
STL
Proprietary
Output
format
47
48
Lava™ C.O.S.
The Lava™ Chairside Oral Scanner (C.O.S.) was created at Brontes Technologies
in Lexington, Massachusetts, and was acquired by 3M ESPE (St. Paul, MN). The Lava™
C.O.S. system consists of a mobile cart containing a central processing unit (CPU), a
touch screen display, and a scanning wand (Figure 2) (61).
Figure 2. The Lava™ C.O.S. system (54).
The method used for capturing 3D impressions involves Active Wavefront
Sampling. Active (optical) wavefront sampling refers to getting three dimensional
49
information from the Lava™ C.O.S. proprietary single-lens imaging system by
measuring depth based on the defocus of the primary optical system (119). In order to
understand the concept, the manufacturers refer to classical photography; changing the
aperture size, the focal range changes too: a small aperture results in a larger focal range,
whereas if the aperture is large the objects in focus are mainly those on the focal plane
while all other points become fuzzy. When two wide apertures are used instead of only
one, the object point is virtualized as two points, encoding the depth information by
means of the image disparity. Image disparity gives the system the Z information to
calculate 3D data.
Similarly, the Lava™ C.O.S. system provides an active three-dimensional
imaging system that includes an off-axis rotating aperture element placed either in the
illumination path or in the imaging path of an optical apparatus (120). The system
includes a lens 140, a rotating aperture element 160 and an image plane 18A, (Figure 3).
50
Figure 3. The rotation of the aperture mechanism (120).
The single aperture avoids overlapping of images from different object regions
hence it increases spatial resolution. The rotating aperture allows taking images at several
aperture positions and this can be interpreted as having several cameras with different
viewpoints, which generally increases measurement sensitivity. The aperture movement
makes it possible to record on a CCD element a single exposed image at different
aperture locations. To process the image, localized cross-correlation can be applied to
reveal image disparity between image frames. As shown in Figure 3, at least two image
recordings on the image plane 18A at different angles of rotation of the aperture 160 are
used to generate the measured displacement for target object 8A. The separate images are
51
captured successively as the aperture rotates to position #1 at time t and position #2 at
time t+At. The rotation center of the image gives the in-plane object coordinates as
follows (Figure 4) (120):
Figure 4. In-plane object coordinates.
where X0,Y0 , are the in-plane object coordinates, f is the focal length of the lens
objective, L is the depth of in-focus object points (focal plane), R is the radius of the
circle along which the off-axis pupil is rotating, and d is the diameter of a circle along
which the relevant out-of-focus point is moving on the image plane 18A as the aperture is
rotated. The magnitude of the pattern movement represents the depth information (Z0)
measured from the lens plane. Z0, can be evaluated from two Snell’s lens laws for infocus and out-of-focus object points and by using similar triangles at the image side
(Figure 5) (120):
Figure 5. The depth information.
52
This method enables “3-D video in Motion” which means that Lava™ C.O.S. is
able to capture approximately 20 3D data sets per second, or close to 2,400 data sets per
arch. A series of 5 slides, provided by the 3M ESPE Product Marketing Manager,
illustrates the concept of measuring out-of-plane coordinates of object points by sampling
the optical wavefront, with an off-axis rotating aperture element, and measuring the
defocus blur diameter, (Figure 6):
Figure 6. The Active Waveform Sampling. Courtesy of Todd W. Deckard.
53
Figure 6. Continued.
54
Figure 6. Continued.
55
After the preparation of the tooth and gingival retraction, the entire arch is dried
and lightly dusted with powder to locate reference points for the scanner. During the
scan, a pulsating blue light emanates from the wand head and an on-screen image of the
teeth appears instantaneously (54). Once the data have been received, the digital
prescription is sent to the laboratory where by the use of specific software, they digitally
cut the die and mark the margin. 3M ESPE receives the digital file, generates a
stereolithography (SLA) model and sends it to the laboratory. When the lab receives the
SLA model, they can create a conventional restoration such as PFM, gold, glass-ceramic,
or CAD/CAM LAVA™ all-ceramic.
Accuracy of Lava™ C.O.S.
Ender and Mehl compared the accuracy (trueness and precision) of digital
impressions of the full arch with that of conventional impressions on an in-vitro model
(121). The master model was acquired, with a reference scanning process, with known
measuring trueness and precision. Plaster models of this model made of conventional
impressions were produced and then digitized with the same reference scanning process.
Also, digital impressions were made with the Cerec AC Bluecam and the Lava™ C.O.S..
The data records were superimposed and the deviations from the master model defined
the trueness of the impression method. Their results showed that the accuracy of the
digital impressions was similar to that of the conventional impression.
In another study, the most accurate scanner with the scanning protocol that would
ensure the most accurate digital impression for implant dentistry was studied (122). A
56
master model made of stone was fitted with three high precision manufactured PEEK
(polyether-ether-ketone) cylinders and scanned with three intra-oral scanners: the
CEREC (Sirona), the iTero (Cadent) and the Lava™ C.O.S (3M). The digital files were
imported in software and the distance between the centers of the cylinders and the
angulation between the cylinders was assessed. The Lava™ C.O.S. had the smallest and
most consistent distance errors, while the CEREC had the largest and most inconsistent.
The accuracy of this system was assessed again, this time with regard to direct
and indirect digitalization (123). More specifically, test datasets were generated in vitro
1) with the Lava™ C.O.S. 2) by digitizing polyether impressions and 3) by scanning the
referring gypsum cast by the Lava Scan ST (3M ESPE, Seefeld, Germany) laboratory
scanner. Using inspection software (Qualify 12.0, Geomagic, Research Triangle Park,
NC, USA), these datasets were superimposed by a best-fit algorithm with the reference
dataset (REF), gained from industrial computed tomography, and divergences were
analyzed. The direct digitalization with Lava C.O.S. showed statistically significantly
higher accuracy compared to the conventional procedure of impression taking and
indirect digitalization.
Repeatability of Lava™ C.O.S.
Balakrishnama et al. determined the dimensional repeatability from the Lava™
C.O.S. over a single prepared tooth from a single scanning system over a two-week
period of time (124). According to the investigators, the repeatability should determine
the system's capability for capturing the proper location and dimensions of the margin of
the prepared tooth. Copper dies were scanned with the Lava C.O.S. system 25 times
57
during a period of two weeks. Geomagic (Research Triangle Park, NC, USA) software
was used to compare each of the scans, using the original scan as a reference for every
comparison, in order to determine the dimensional repeatability from the system. The
results revealed that the anterior repeatability was ≤5.8 µm, and posterior repeatability
≤10.9 µm, so the authors concluded that this scanner demonstrated a dimensional
repeatability for single preparations that is beyond the requirement to achieve clinical
acceptability for marginal adaptation in a crown or bridge restoration (normally accepted
to be 50 to 100 µm).
Fit of crowns made from Lava™ C.O.S. impressions
Lava™ C.O.S. is a system that has attracted the attention of the researchers and
thus it has been much studied since its introduction to clinical practice.
Syrek et al. compared the fit of all-ceramic crowns fabricated from intraoral
digital impressions with the fit of all-ceramic crowns fabricated from PVS impressions
(58). Two LavaTM (zirconia) crowns were fabricated for the same preparation in each of
20 patients. One crown was fabricated using the Lava™ C.O.S. and the other crown from
the PVS impression material. Prior to cementation, two calibrated and blinded examiners
clinically evaluated the fit of both crowns. The marginal fit was also scored using the
replica technique. The results revealed significant difference between the two groups; allceramic crowns resulting from Lava™ C.O.S. demonstrated significantly better marginal
fit than all-ceramic crowns fabricated from conventional impressions (both groups were
within clinically acceptability).
58
Scotti et al. published a very similar paper to the above, where they measured the
marginal and internal fit of zirconia crowns made from Lava™ C.O.S. using the replica
technique (55). Four different points were evaluated using stereomicroscopy with a
magnification of 50x. The results showed that all values were clinically acceptable and
the authors considered this method to be accurate enough to be used as an alternative to
conventional impressions.
Seelbach et al. compared the accuracy of all-ceramic crowns obtained from
intraoral scans with Lava™ C.O.S. (3M ESPE), CEREC (Sirona), and iTero (Straumann)
with conventional impression techniques (two-step and single-step putty-wash
impressions) (62). For both conventional techniques 10 crowns were made of two
materials (Lava zirconia (3M ESPE, USA) and Cera E cast crowns (Elephant Dental
B.V., The Netherlands)). Then, 10 digital impressions (Lava C.O.S.) were taken and Lava
zirconia (3M ESPE, USA) crowns were manufactured, 10 all-ceramic crowns were
fabricated with CEREC (Empress CAD, Ivoclar Vivadent, Liechtenstein) and 10 allceramic crowns were made with iTero (Copran Zr-I, White Peaks Dental Systems,
Germany). Measurements were performed with a 3D-coordinate measuring system (CNC
Rapid, Thome Präzision GmbH, Germany). The deviation was assessed at 50 points per
crown (3D measuring precision, 3µm in this setup). Metrolog XG (Version 12.003 HF1,
Metrologic Group S.A., France) was used as controlling software. Both, marginal and
internal fit, were assessed. With regard to internal fit, the best results were obtained for
Lava zirconia restorations made on the basis of Lava™ C.O.S. scans, while the biggest
deviations were found for CEREC manufactured Empress CAD crowns. Both differed
statistically from the other groups. With regard to marginal fit, CEREC crowns neither
59
differed statistically significantly from Lava™ C.O.S. crowns nor from crowns made on
the basis of single-step putty-wash impressions.
The internal and marginal fit of the zirconia copings generated from scanning a
definitive cast made from a conventional impression and copings generated from a digital
impression system were evaluated, in a Master’s thesis, by Hirayama et al. (125).
Specimens were divided into 2 groups; group A: 18 Zirconia copings fabricated by
scanning stone models from PVS impressions and group B: 19 Zirconia copings
fabricated by scanning the master cast and transmitting the scanned data to the Lava™
milling center in St. Paul, MN. To evaluate the fit, the authors used the replica technique
described by Boening et al (32) and Molin & Karlsson (31). They found a statistically
significant difference between groups A and B, with group B having a better marginal
adaptation. That study concluded that both groups had clinically acceptable marginal fit;
however the ones made from the digital impression had significantly smaller marginal
discrepancies.
E4D Dentist System™
The E4D Dentist System™ (D4D Technologies LLC, Richardson, TX) was
introduced in early 2008. It consists of a cart containing the design center (computer and
monitor) and laser scanner, a separate milling unit (center), and a job server and router
for communication (Figure 7) (61).
60
Figure 7. The E4D Dentist System™ (54).
According to the company’s brochure, the E4D is the only CAD/CAM system
that uses a true laser for scanning hard and soft dental tissue, impression material,
occlusal registration material and dental stone. It combines laser technology with micromirrors developed exclusively for D4D technologies by Texas Instruments. The mirror
system allows a single laser point to be generated across a large area in a patterned
approach thereby eliminating any speckling or diffusion of the laser point. This laser does
not require a contrast agent.
The working principle of this system is called optical coherence tomography and
confocal microscopy. Optical coherence tomography (OCT) is analogous to ultrasound
61
imaging, except that the imaging is performed using light rather than sound (126). By
measuring the echo time delay and intensity of back-reflected light, OCT can reveal
tissue microstructure with micron-level resolution; image resolutions of 1–15 µm, one to
two orders of magnitude finer than standard ultrasound (127). The axial resolution of
OCT is determined by the coherence length of the light source: Dz = (2ln2/pi
(pi=3.14159)) (l2/Dl), where Dl is the full-width-at-half-maximum of the source
spectrum (the difference between the two wavelength values at which the power is equal
to half of its maximum value) and l is the center wavelength of the source spectrum
(128). Confocal microscopy increases optical resolution and contrast; it enables the
reconstruction of three dimensional (3D) structures by stacking individual 2D en-face
images at different depths (126).
The laser digitizer includes a laser source coupled to a fiber optic cable, a coupler
and a detector (54). The coupler splits the light from the light source into two paths. The
first path leads to the imaging optics, which focuses the beam onto a scanner mirror,
which steers the light to the surface of the prepared tooth. The second path of light from
the light source via the coupler is coupled to the optical delay line and to the reflector;
this reference path is of a controlled and known path length, as configured by the
parameters of the optical delay line. Light is reflected from the surface of the object,
returned via the scanner mirror and combined by the coupler with the reference path light
from the optical delay line. The combined light is coupled to an imaging system and
imaging optics via a fiber optic cable. By utilizing a low coherence light source and
varying the reference path by a known variation, the laser digitizer provides an Optical
Coherence Tomography (OCT) sensor. The focusing optics is placed on a positioning
62
device in order to alter the focusing position of the laser beam and to operate as a
confocal sensor (129). A series of imaged laser segments on the object from a single
sample position interlace between two or multiple 3D maps of the sample from
essentially the same sample position. The time period to measure each interlaced 3D map
is reduced to a short interval and relative motion effects between the intra-oral device and
the patient are reduced. The interlaced 3D maps may be aligned with software to produce
an effective single view dense 3D point cloud that has no motion induced inaccuracies or
artifacts. The motion of the operator between each subframe may be tracked
mathematically through reference points in the dataset itself. The operator motion is
removed in subsequent analysis (129).
The scanner must be held a specific distance from the surface being scanned; this
is achieved with the help of rubber-tipped “boots” that extend from the head of the
scanner (60). Placing these rests on adjacent teeth steadies the scanner at this optimal
distance. The ICEverything™ feature of the E4D takes actual pictures of the teeth and
gingiva. A diagram on the monitor shows the user how to orient the scanner to obtain the
next image. As successive pictures are taken, they are wrapped around the 3D model to
create the ICEverything model.
Once captured the 3D data are displayed as virtual model. The software allows the
operators to design as many as 16 units at once and switch back and forth to select any
tooth to alter the design. The milling center communicates wirelessly with the design
center so that the finished restoration can be milled in the office or remotely (60).
63
Accuracy of E4D Dentist System™
Plourde et al. evaluated in vitro the marginal and internal fit of all-ceramic crowns
made with E4D Dentist System™ (63). All monolithic lithium disilicate crowns (IPS
e.max® CAD LT A1/C14) were cemented under constant pressure, embedded in acrylic
and then sectioned facial-lingually. The sections were evaluated under microscope in 3
locations (marginal-edge, mid-axial wall, and cusp-tip). The results showed that the mean
fits ranged from 66.37 µm to 207.61 µm depending on location of measurement. The
marginal gap on the facial was 71.96 ± 62.19µm and on the lingual 149.11 ± 67.93µm.
They concluded that the marginal and internal fits fell within the range of what several
previous studies considered to be clinically acceptable and that the large standard
deviations suggest a high degree of variability in scanning, designing, and milling
capabilities.
In another study, by Kugel et al., tooth #14 was prepared per standard
specification to receive an all-ceramic crown restoration on typodont (130). All-ceramic
CAD/CAM crowns (Group 1) were fabricated with the E4D Dentist System™. For press
laboratory-made crowns, impressions were taken with two-step impression techniques
using a custom triple tray with light and putty consistency VPS. Impressions were sent to
two dental laboratories (Group 2 and 3) for fabricating the monolithic press lithium
disilicate crown. All crowns were cemented using Multilink® Automix (Ivoclar
Vivadent) under constant pressure of 100 N, then they were embedded in acrylic and
sectioned facial-lingually. Sections were evaluated under digital microscope and
measured on three locations per facial and lingual side of section: marginal edge, midaxial wall, and cusp tip. The results showed no significant difference at the facial (Group
64
1: 44.88±32.06, Group 2: 33.46±38.77 and Group 3: 45.22±41.87) and lingual (Group 1:
39.07±32.44, Group 2: 36.09±38.47and Group 3: 62.02±49.96) margins in all groups.
However, there was significant difference for cement thickness in midaxial, cusp and
occlusal within the group. The authors concluded that there was no statistical difference
in marginal fit of all-ceramic crowns made by CAD/CAM system or laboratory press
ceramic.
Summary-Purpose
With the evolving technology and the incorporation of new materials in
restorative dentistry, research is mandatory in order to indicate which ideas are
appropriate for clinical use and support the need for further research. The purpose of this
study was to evaluate the fit of one of the most currently used restorative material
(lithium disilicate- press and CAD) made from two different impression techniques (PVS
and Lava™ C.O.S.).
65
CHAPTER III
MATERIALS AND METHODS
Introduction
The marginal and internal adaptation of IPS e.max crowns made from two
impression techniques and two fabrication methods were evaluated. The impression
techniques evaluated in this study were a conventional impression using polyvinyl
siloxane material and custom tray, and a digital impression using Lava™ C.O.S. The
crown fabrication methods used in this study were the hot-pressed and the computeraided design/computer-aided manufactured (CAD/CAM). Four groups were created:
Group A: conventional impression/IPS e.max Press, Group B: conventional
impression/IPS e.max CAD, Group C: digital impression/IPS e.max Press, and Group D:
digital impression/IPS e.max CAD. The dies and the crowns were digitized using a laser
scanner and the adaptation was measured using sophisticated software.
Pilot study
A pilot study was conducted prior to the main study in order to test the proposed
protocol and conduct a power analysis (Figure 8). A brief description of the materials and
methods used as well as the results will be presented at the beginning of this chapter prior
to the definitive study.
66
Master Die
10 PVS
Impressions
Group A
5 IPS e.max Press
crowns
Group B
5 IPS e.max CAD
crowns
10 Lava™ C.O.S. Impressions
Group C
5 IPS e.max Press
crowns
Group D
5 IPS e.max CAD
crowns
Figure 8. Study Groups for the pilot study.
A dentaform replica mandibular first molar tooth number thirty (#30) (Dentaform,
Frenso, CA, USA) was prepared for an all-ceramic crown. Ten (10) conventional
impressions were made with, light and heavy body polyvinyl siloxanes (Extrude Type 3low consistency; Extrude Type 1-high consistency, Kerr Dental, Orange, CA) and a
custom tray (SternTek, Sterngold Restorative Systems, Attlebono, MA, USA). The
impressions were poured with Type IV gypsum (Resinrock, Whip Mix Corp, Louisville,
KY, USA). Ten (10) digital impressions were made using the Lava™ C.O.S. (Lava™
Chairside Oral Scanner, 3M Lexington, USA) and SLA resin casts ((In’Tech, Minessota,
MN, USA) were produced. Five (5) dies from each impression technique were used to
fabricate the pressed crowns and five (5) to fabricate the CAD crowns. For the pressed
crowns, one (1) coat of die spacer (Rem-e-die, Ivoclar Vivadent, Schaan, Liechtenstein)
was used to within 1mm of the margin. A full contoured crown was waxed up, invested
and pressed using IPS e.max Press (IPS e.max Press HT A1, Ivoclar Vivadent, Schaan,
67
Liechtenstein). The intaglio of the crown was adjusted twice, if needed in order to
improve the fit, simulating clinical conditions. For the CAD crowns, the dies were
scanned using the Kavo Everest ScanPro (Kavo Dental GmbH, Biberach, DE), a noncontact 3D strip-light projection scanner. One (1) coat of spray (Occlude® The Indicator,
Pascal Int. Co, Bellevue, WA) was applied prior to scanning. The full contoured crowns
were designed with 55µm die spacer and 10µm marginal horizontal overextension. IPS
e.max CAD blocks (IPS e.max CAD HT Block I12 A1, Ivoclar Vivadent, Schaan,
Liechtenstein) were milled using the Kavo Everest milling engine. The intaglio of the
crowns was adjusted twice as with the pressed crowns and then they were crystallized.
The intaglio of all the crowns and the master die were digitized using the same
Kavo scanner. A data set was created for the Qualify 2012 software (Geomagic, Research
Triangle Park, NC, USA). The intaglio of the each crown and the master die were
manually aligned first and then further refined by using the software’s Best-Fit
Alignment. Sections were made in facial-lingual (FL) and mesio-distal (MD) directions.
Five (5) points in each section were measured (2 on the margins, 2 in the middle of the
axial walls and 1 on the middle of the occlusal surface); a total of ten (10) points per
crown were analyzed (margin-M, margin-D, margin-F, margin-L, mid-M, mid-D, mid-F
and mid-L, occlusal-MD and occlusal-FL).
A two-sample t-test and the nonparametric Wilcoxon rank-sum test (i.e. when the
assumption of normality was violated) were used to detect a difference in the marginal
and internal gap values between two impression techniques and between two crown
fabrication methods. One-way ANOVA with post-hoc Tukey’s HSD test was conducted
to determine whether there was a significant difference in the marginal gap values among
68
the four experimental groups. The Shapiro-Wilk test was applied to verify the assumption
of normality. If the assumption of normality was violated, one-way ANOVA to the
ranked data followed by post-hoc Bonferroni multiple comparison test, an equivalent test
statistic to the nonparametric Kruskal-Wallis test, was used as the test statistic.
Results of the pilot study
The results showed that when the impression techniques were compared: between
Group A vs. Group C (pressed crowns) the mean marginal gap values for digital
impression were significantly greater than those using the conventional impression for
two variables (mid-M and margin-M). No statistical difference was found for the
remaining 8 variables. Between Group B vs. Group D (CAD crowns) the mean marginal
gap values for digital impression were significantly greater than those using the
conventional impression for 4 variables (mid-F, occlusal-FL, mid-M, margin-M). No
statistical difference was found for the remaining 6 variables (Table 3).
When the crown fabrication techniques were compared, between Group A vs.
Group B (conventional impression) the mean marginal gap values for CAD crowns were
significantly greater than the pressed crowns for two variables (occlusal-MD and
occlusal-FL). No statistical difference was found for the remaining 8 variables. Between
Group C vs. Group D (Digital impression) the mean marginal gap values for CAD
crowns were significantly greater than those using the conventional impression for four
variables (margin-F, mid-F, occlusal-FL, occlusal-MD, margin-L). No statistical
difference was found for the remaining five variables (Table 3).
N
5
5
5
5
Experiment Groups
Conventional/press
Conventional/CAD
Lava/press
Lava/CAD
0.187
(0.05)
0.087
(0.05)
0.151
(0.06)
0.152
(0.09)
Mean
Avg
margi
n-F in
mm
(SD)
0.200
(0.05)
0.121
(0.01)
0.130
(0.02)
0.113
(0.04)
Mean
Avg
mid-F
in mm
(SD)
0.331
(0.06)
0.164
(0.08)
0.224
(0.04)
0.126
(0.02)
Mean
Avg
occlusal
-FL in
mm
(SD)
0.128
(0.04)
0.133
(0.04)
0.080
(0.03)
0.080
(0.06)
Mean
Avg
mid-L
in mm
(SD)
0.128
(15.00)
0.030
(5.00)
0.120
(13.80)
0.056
(8.20)
Mean
Avg
marginL in mm
(mean
rank
scores)
0.097
(0.03)
0.122
(0.07)
0.104
(0.08)
0.046
(0.03)
Mean
Avg
margi
n-D in
mm
(SD)
0.145
(0.02)
0.165
(0.05)
0.159
(0.04)
0.114
(0.04)
Mean
Avg
mid-D
in mm
(SD)
0.323
(0.07)
0.169
(0.04)
0.255
(0.03)
0.157
(0.02)
Mean
Avg
occlusal
-MD in
mm
(SD)
0.178
(0.03)
0.128
(0.04)
0.045
(0.02)
0.046
(0.04)
Mean
Avg
mid-M
in mm
(SD)
0.132
(0.04)
0.099
(0.03)
0.053
(0.01)
0.037
(0.02)
Mean
Avg
margi
n-M in
mm
(SD)
69
70
Intraclass correlation coefficients were also computed to assess intra-observer
agreement in tracing of marginal and internal gap between the two duplicate
measurements of all variables. Overall, there was very strong evidence that these
intraclass correlations differed from zero (p<0.001 for each instance), and the correlation
coefficients indicated from a moderate to a strong agreement between the two
measurements made by the single observer.
Based on the pilot data, the sample size per group that was required to distinguish
statistical difference among the four groups with 80% (or 90%) power for each of the 10
variables was calculated.
Validation of the Digital Measurement Technique
Since the digital measurement is a new method of evaluating the fit in prosthetic
dentistry, in order to validate it, it was compared to the classic replica technique. Light
body Extrude material was injected in the intaglio surface of five (5) IPS e.max CAD
crowns. The crowns were seated on the master die and held for 10 minutes with finger
pressure. After the material set the crown was removed and the PVS material was
sectioned with a blade at the same reference points as were the digital sections. The
sectioned PVS material was placed on a glass slide with PVS adhesive parallel to
horizontal plane. A Zeiss Axiotech Microscope (X50) (Carl Zeiss Microscopy, LLC,
Thornwood, NY, USA) was used to make the digital photographs and the NIH-ImageJ
software (NIH, ImageJ 1.46) was used to measure the thickness. A paired-sample t-test
was used to determine whether a significant difference in marginal gap existed between
71
the two techniques (replica vs. digital). A p-value of less than 0.05 was used as a criterion
for statistical significance.
Based on the paired-sample t-test, there was no significant difference in marginal
and internal gap between the two measurement techniques (p>0.05 for each instance) for
most of the points tested. Out of ten measurements, three cases showed that mean
marginal gap values were significantly greater for the replica technique than those
measured using digital technique; occlusal-MD (p=0.0122), occlusal-FL (p=0.0709) and
mid-M (p=0.0032).
After the completion of the pilot study, the following changes were made to the
protocol for the definitive study:
1. Fifteen (15) samples per study group would be included.
2. Low translucency (LT) ingots instead of high translucency (HT) would be used to
facilitate scanning of the crowns.
3. No adjustments in the intaglio of the crowns would be performed in order to
adjust the fit since the standardization of this procedure was difficult and
subjective.
4. A chairside scanner and milling engine was selected for the fabrication of the
CAD crowns (E4D vs. Kavo).
5. A different scanner would be used in order to digitize the specimens for the
measurements from the one used to fabricate the CAD crowns, in order to avoid
errors related to the scanner.
72
6. A more detailed protocol would be developed to align the crown and master die.
After Best-Fit Alignment, manual alignment would be done until the most
realistic fit was obtained.
7. Different statistical analysis would be performed; the average mean marginal and
internal gap would be assessed instead of the individual points in each section.
8. The 3D marginal fit would be calculated as well.
Definitive study
A thorough description of the materials and methods used in the definitive study
will be discussed in this chapter (Figure 9).
Master Die
30 PVS
Impressions
Group A
15 IPS e.max
Press crowns
Group B
15 IPS e.max CAD
crowns
Figure 9. Study Groups for the definitive study.
30 Lava™ C.O.S. Impressions
Group C
15 IPS e.max
Press crowns
Group D
15 IPS e.max CAD
crowns
73
Study design
Master die fabrication
A full dentate dentaform (Dentaform, Frenso, CA, USA) with teeth numbers 1-32
was used. A dentaform replica mandibular first molar tooth number thirty (#30) was
prepared for an all-ceramic crown by a single operator. High-speed hand piece (Brasseler,
Savabbah, GA, USA) was used to prepare the tooth according to standard tooth
preparation procedures. The prepared margin of the tooth was clearly defined by a
distinct heavy chamfer made with diamond bur (No. 6856SU, Brasseler, Savabbah, GA,
USA). The circumferential reduction of tooth substance was 1.5 mm. The occlusal
reduction was 1.5 mm. All internal line and point angles were rounded. The convergence
angle of the prepared tooth was at 5-10°. The margin was placed 1mm above the gingiva
(Figure 10, 11).
Figure 10. Master die frontal view.
74
Figure 11. Master die occlusal view.
Impression making
Two impression techniques, conventional impression, and digital impression with
Lava™ C.O.S were used in the study. These are described separately below.
Conventional impression
Custom trays extended only in the mandibular right quadrant were fabricated as
follows: two layers of baseplate wax (Shurwax, Modern Materials, Heraeus Kulzer, LLC
IN, USA) were applied on the dentaform to create approximately 2mm of uniform space
for custom tray fabrication. The wax extended from tooth #26 to #32, 3mm below the
CEJ. Two tissue stops were created on #29 and 31 by removing wax until the tooth was
seen. An aluminum foil separator was used to cover the wax. One layer of lightpolymerized resin (SternTek, Sterngold Restorative Systems, Attlebono, MA, USA) was
75
adapted to the foil covered wax spacer. The resin was extended from the distal of #32 to
tooth #24 in direct contact with #24 and #25 for stability. It was cured in the visible lightpolymerizing unit (Triad 2000, Dentsply, York, PA, USA) for 2 minutes to fabricate the
custom tray. The wax and the aluminum foil were carefully removed using a Buffalo
knife and the intaglio of the tray was light-cured for 2 more minutes. Custom trays were
fabricated 72 hours before the impressions were made to allow them to become
dimensionally stable.
A thin layer of tray adhesive (Tray Adhesive 16622, Kerr Dental, Orange, CA)
was brushed onto the tray 24 hours after the tray fabrication. The adhesive bonds the
impression material to the tray, and thus, controls the direction of polymerization
shrinkage of the material. All the custom trays were allowed to dry for 48hr after the
application of the tray adhesive.
Cartridges of polyvinyl siloxane, light and heavy body, (Extrude Type 3-low
consistency; Extrude Type 1-high consistency, Kerr Dental, Orange, CA) were loaded
individually into dispensing guns. An impression syringe and intraoral tip were attached
to dispensing guns. The heavy body was injected into the half arch custom tray. At the
same time, the light body material was carefully injected on the prepared tooth (#30)
including the sulcus until the tooth was completely covered. The custom tray loaded with
heavy body was seated on the dentaform. After 11 minutes from the start of mix, the set
impression material/custom tray was removed from the master cast by pulling slowly to
break the seal, then snapped out along the long axis of the teeth. The impression was
carefully examined under a microscope (10x) to make sure the preparation margin was
intact.
76
After 24 hours, each of the 30 PVS impressions was treated with a surface tension
reducing agent (Vacufilm; Kerr Dental, Orange, CA) and light compressed air was used
to remove the excess. Type IV gypsum (Resinrock, Whip Mix Corp, Louisville, KY,
USA) was used to fabricate the definitive casts. Resinrock was mixed with the ratio of
70g powder to 14 ml water. Hand spatulation was performed until all powder was
incorporated and then was mechanically spatulated under a vacuum for an additional 30
seconds. Resinrock was carefully poured into the impression using a spatula. After 72
hours the gypsum cast was removed from the impression. The same procedure was
repeated 30 times to obtain 30 stone casts (Group A and B). The stone casts were then
prepared to receive two pins (Pindex; Coltene/ Whaledent, Mahwah, N.J.) per removable
section. Pins were attached with cyano-acrylate cement to the facial and lingual aspect on
working dies. Dental stone (Flowstone, Whip Mix Corp, Louisville, KY, USA) was
poured around the pins to form a base. After the base was set, the cast was separated and
prepared tooth #30 was sectioned using a diamond disk (No. 6924HP400, Brasseler,
Savabbah, GA, USA). The die was trimmed under microscope (10x) (Meiji Techno,
Model BM 47491) using a carbide bur (No. H78060, Brasseler, Savabbah, GA, USA) and
stainless steel surgical blade No.21 (Figure 12).
77
Figure 12. Stone die.
Digital impression
For the digital impressions, a thin dusting with titanium dioxide powder (3M
ESPE, Lexington, USA) was applied to the lower right quadrant of the dentoform to
facilitate the scanning of the prepared tooth and the adjacent teeth. The prepared tooth
(#30) was scanned with the Lava™ C.O.S. (Lava™ Chairside Oral Scanner, 3M
Lexington, USA) intraoral scanner. After verification that the margins were clearly
visible, all details of the preparation were captured. Then, the occlusal, facial and lingual
surfaces of the quadrant were scanned. The scans were individually checked for
contiguous data before their acceptance. The scanning data were sent to the
manufacturing center (In’Tech, Minessota, MN, USA). This procedure was repeated 30
times (Group C and D). Thirty (30) resin (SLA) models with removable dies (SLA resin
casts, St.Paul, 3M Lexington, USA) were produced (Figure 13).
78
Figure 13. Resin die.
IPS e.max Press crown fabrication
IPS e.max Press (IPS e.max Press LT A1, Ivoclar Vivadent, Schaan,
Liechtenstein) ingots were used to make the full coverage crowns using the lost wax
technique. Fifteen (15) stone casts produced by the conventional impression and fifteen
(15) resin casts produced by the digital impression were used. The margins were clearly
defined by using a blue pencil (Margin liner, Kerr, Orange, CA). One layer of die
hardener (Industrial Krazy Glue, Aron Alpha, Type 202, OH, USA) was applied on the
stone dies, extending 1 mm occlusal and apical to the margin. One layer of rubber-based
removable die spacer (Rem-e-die, Ivoclar Vivadent, Schaan, Liechtenstein) was used on
all dies, stone and resin, extending 1 mm occlusal to the margin, as recommended by the
laboratory technician of the manufacturer company (Ivoclar Vivadent). The dies were
lubricated (DieLube, Ney, Denstply Ceramco, York, PA) and then dipped in hot dipping
79
wax (Bellewax, Kerr, Orange, CA). A wax pattern for the full contoured crown was
fabricated using wax addition technique on one of the stone casts. A matrix from PVS
material (Exaflex putty and light body Extrude) was made in order to standardize the
thickness and the shape of the pressed crowns. A hole was made on the facial of the
matrix in order to inject the melted wax (Yeti Dental, Thowax, Eugen, Germany). The
matrix was adapted on each cast and the wax was injected. After 1 minute the matrix was
removed and the excess wax was cleaned. If there were any irregularities, more wax was
added to finish the contours. The margins were carefully finished and checked under the
microscope (10x) using margin wax (Almore, INC, Portland, OR, USA) with an electric
waxer (Dual Carving Pencil, Whip Mix Corp, Louisville, KY, USA).
The wax patterns were sprued at the mesial facial cusp, which was the thickest
part of the wax-up, using an 8 gauge wax sprue (Kerr, Orange, CA) 3mm long. The
sprues were attached to the IPS investment ring (IPS investment ring System 200g,
Ivoclar Vivadent, Schaan, Liechtenstein) base with rope wax and sticky wax, positioning
with 45-degree inclination from the center. Four crowns were invested in each investment
ring. The investment (IPS PressVEST Speed, Ivoclar Vivadent, Schaan, Liechtenstein)
was mixed according to the manufacturer’s instructions. The filled investment ring was
allowed to set for 35 min. The ring gauge and the ring base were removed with a turning
movement. The investment ring was placed in the preheated furnace (850oC) at the final
temperature for 45 min. The cold IPS e.max Press ingot and the IPS Alox Plunger, after it
was dipped in IPS Alox Plunger Seperator, were placed into the hot investment ring using
metal tongs. The assembled investment ring was placed in the center of the hot press
80
furnace (Programat EP5000, Ivoclar Vivadent, Schaan, Liechtenstein). The recommended
pressing program for IPS e.max Press LT was used (Table 4).
B
t ì
T
H
E
o
o
o
C
mm:ss
µm/Min
917
25:00
250
C
700
C/Min
60
Table 4. Pressing program parameters for IPS e.max Press LT.
The ring was left to cool to room temperature for 60 minutes. The length of the
plunger was marked on the cooled ring. The investment ring was sectioned using a
separating disk. The crowns were divested with Type 50µm Al2O3 (Blasting compound,
Ivoclar Vivadent, Schaan, Liechtenstein) at 4bar pressure. After fine divesting, the
crowns were immersed in a plastic cup with the IPS e.max Press Invex Liquid (Ivoclar
Vivadent, Schaan, Liechtenstein) and placed in an ultrasonic cleaner for 15 minutes in
order for the reaction layer to be removed. The restorations were cleaned under running
water and then dried. The reaction layer was removed with Type 50µm Al2O3 at 4bar
pressure.
The sprues were cut using a fine diamond disk (No. 6918BHP220 Brasseler,
Savabbah, GA, USA) 1mm away from the actual cusp tip in order to avoid perforation.
The sprue attachment area was smoothed and rounded using a polishing disk (No.
94002CHP170 Brasseler, Savabbah, GA, USA). The intaglio of the crowns was observed
81
under the microscope (10x). Any residual positives from the investing procedure were
carefully removed with a diamond bur (Brasseler, Savabbah, GA, USA). No further
adjustments were made to the intaglio surface.
IPS e.max CAD crown fabrication
The remaining 15 stone casts and 15 resin models were scanned using the E4D
scanner (D4D Technologies, Richardson, TX, USA) and the crowns were designed with
the E4D Design Center. Based on the software instructions (Dentalogic TM 4.5.0.34), a
new file was created for each die, and the following steps were performed:
1.
Setup: Select “Crown,” “Bite Registration,” Library “A,” Material “IPS
e.max CAD LT” and Shade “A1.”
2.
Scan: The die alone was scanned.
3.
Margin: Select “Trace” in order to define the margin.
4.
Design: Select “Thickness;” spacer thickness “0.04” and margin ramp
“1.00” of the crown. The thickness of the crown was adjusted to be
more than 1mm all around. The margin was enhanced in order to avoid
chipping during milling, by enabling the default settings under Margin
Boost Settings “0.150” and “2.000”.
5.
Mill: The sprue was placed in the proximal surfaces as far from the
margin as possible. Select “Detail mill.”
6.
Data were sent to the E4D milling engine.
82
7.
IPS e.max CAD blocks (IPS e.max CAD LT Block I12 A1, Ivoclar
Vivadent, Schaan, Liechtenstein) were tightened into the milling
engine.
After the crowns were milled, the sprues were cut a using diamond bur (No.
6918BHP220 Brasseler, Savabbah, GA, USA). The horizontally overhanging margins
were adjusted under microscope (10x) with a polishing disk (No. 94002CHP170
Brasseler, Savabbah, GA, USA). No adjustments on the intaglio surface were made.
The intaglio surface of the crowns was filled with IPS Object Fix Putty/Flow
(Ivoclar Vivadent, Schaan, Liechtenstein) and then it was placed on a crystallization pin.
The crowns were crystallized using a ceramic furnace (Ney Centurion Qex, Denstply
Ceramco, NJ, USA). The recommended speed crystallization/Glaze LT program used is
presented in Table 5. Representative examples of the crystallized crown intaglio surfaces
are depicted in Figure 14.
6:00
403 oC
o
S
B
min
rate
time
temperature
C/min
90
t1
Heating
Closing
Stand-by
820 oC
T1
temperature
Firing
min
0:10
H1
time
Holding
o
C/min
30
t2
rate
Heating
840 oC
T2
temperature
Firing
min
7:00
H2
time
Holding
o
C
o
C
820/840
21/22
11/12
550/820
Vacuum 2
Vacuum 1
700 oC
L
cooling
Longterm
o
C/min
20
tl
rate
Cooling
83
84
Figure 14. Intaglio of one indicative crown from each experimental group.
Measurement of the crown fit
The fit of a crown on a tooth refers to the adaptation of the prosthesis on the walls
of the prepared tooth. For this study, in order to assess the fit, the gap between the
intaglio of the crown and the tooth surfaces was acquired. A small gap means close
proximity of the two surfaces, which is interpreted as a good fit. In other words, the
smaller the gap, the better the fit, and conversely the bigger the gap, the poorer the fit. A
description of the how that gap was calculated in 3D and 2D follows.
The master die and the intaglio of each of the crowns were digitized using the
Surveyor ZS-Series scanner which is a 3D laser coordinate measurement machine
(CMM) with scan accuracy of +/- 0.00898mm (Laser Design Inc, GKS, Minneapolis,
85
MN, USA). A light coat of spray was used to facilitate the scanning (Spotcheck® SKDS2 Non-Halogenated Solvent Developer, Magnaflux, Glenview, IL, USA).
Three different scans were made according to the triple-scan protocol by Holst et
al. (39): 1) The prepared dentaform tooth (Master Die) secured on a standardized metal
base with PVS material, 2) The intaglio of each one of the all-ceramic crowns, and 3)
Each crown on the tooth in a clinically correct final position.
Digital Shape Scanning and Processing (DSSP) was applied using Geomagic
Qualify 2012 software (Geomagic, Research Triangle Park, NC, USA). For each
specimen a separate data set in STL format was generated from point clouds with the
Geomagic Qualify 2012 software. First, the master die STL file and the crown-master die
STL file were registered by manual alignment followed by best-fit registration. Then the
same procedure was done to register the crown STL file and crown-master die STL file.
The crown-master die STL data set was deleted and the aligned crown to master die STL
data set was used for fit assessment.
For the 3D measurements, an area above the cavosurface margin with 0.75mm
occlusal-gingival width circumferentially was defined using the Geomagic Studio 2012
software as follows (Figure 15):
1. Trace the margin using Draw Curves under the Curves menu.
2. Right Mouse Click>Duplicate the curve in the Model Manager.
3. Tools>Move>Exact Movement to move the duplicated curve 0.75mm above the
margin.
4. Project the translated curve down to the polygon surface using Curves>Free
Curves>Project
86
5. Convert both curves to boundaries by using Curves>Projected Curves>Convert
To
6. Finally, save the model as an independent object
Figure 15. Defined area around the margin of the Master Die with 0.75mm occlusalgingival width.
For the 2D measurements, two sections, one facial-lingual and one mesial-distal,
were made through the grooves on the standardized metal base of the tooth. The distance
between the die and the intaglio surface of the crown were measured at 7 standardized
points (2 on the margins, 2 at 0.75mm above the margin, 2 on the axial walls and 1 on the
occlusal surface), as follows (Figure 16-18):
87
1. Use Analysis>Dimensions>Section Through Object to create cross sections
2. Go to Analysis>Dimensions>2D Dimension to define the 7 points
Figure 16. Grooves on the base of the Master Die in order to standardize the sections.
88
Figure 17. Facial-lingual section with the 7 standardized points.
Figure 18. Mesial-distal section with the 7 standardized points.
89
The steps taken to obtain the measurements using the Geomagic Qualify 2012
software are the following:
1. Right Mouse Click on the Master Die to set as “Reference” and again on the
crown to set it as “Test”.
2. The intaglio of the crown and the coronal part of the master die are selected
3. Go to Alignment>Object Alignment>Best-fit Alignment. Click Apply twice for
fine adjustments. Click OK.
4. A macro program was created that automated the following steps.
a. Reverse the normals: where the test object becomes the intaglio of the
crown instead of the outside, which the software automatically selects.
b. Reduce noise prismatic (conservative) twice
c. Remove Spikes at 70%
d. The intaglio is set as an independent object.
e. AutoCreate features from the Reference Object over to the Test Object.
In order to Autocreate the features only one crown was used
and then the point targets were applied to the rest of them. The
following steps describe the point target positioning:
i.
Select the inside of the crown.
ii.
Right Mouse Click>Reverse Selection.
iii.
Tools>Create>New Object>From Selection
iv.
Select the inside of the crown.
v.
Polygons>Repair>Repair>Flip Normals
vi.
Select the tooth.
90
vii.
Alignment>Object Alignment>Best Fit alignment
viii.
Analysis>Compare>3D Compare
a. Set the Objects box to Compare Selected Only
b. Set the Max Deviation to .75mm
c. Set the Max Critical and Max Nominal to
.06mm
d. Set the Min Critical and Min Nominal to .06mm
ix.
This creates a color map of highs and lows of the
alignment. Use Create Annotations to annotate the low
spots (blue).
x.
Export the table of the XYZ positions of the
Annotations
xi.
Use the XYZ coordinates from the annotations to create
the Point Target features
5. Go to Analysis >Section Through Object to section the tooth through the grooves
to evaluate the fit. If there was an overlap, where the crown seemed to be inside
the tooth, the crown needed to be repositioned.
6. Go to Tools >Move >Exact movement. The crown was moved in any direction
and as many times as needed, until the most realistic and acceptable seating was
established.
7. An “Automation” was created that included the following steps:
a. RPS Alignment
91
b. 3D Comparison around the margin, as well as the
c. 2D measurements on the pre-determined locations.
8. All the data were obtained. For the 3D data go to “Export table” and save the
values in an Excel file. For the 2D data, go to “Create report” and save it as a
PowerPoint file.
Statistical analysis
Two different data sets were created, one for the 3D and one for the 2D data
obtained from the measurements.
For the 3D data, descriptive statistics were conducted. One-way ANOVA with
post-hoc Tukey’s HSD (Honestly Significant Difference) test was used to determine
whether there were significant differences in mean marginal gap values among the four
experimental groups. Additionally, a two-way ANOVA was performed to detect a
significant interaction between the type of impressions and the type of crowns on the
marginal fit.
For the 2D data, a two-way ANOVA was performed to detect a significant
interaction between the type of impressions and the type of crowns on the marginal and
internal fit. Two-sample t-test was used to detect the difference in marginal and internal
fit between two types of crowns within each type of impressions or between two types of
impressions within each type of crowns. Additionally, when the test groups were
considered as four individual experimental groups, one-way ANOVA with post-hoc
Tukey’s HSD (Honestly Significant Difference) test was used to determine whether there
92
was a significant difference in the mean marginal and internal gap values among the four
experimental groups.
A p-value of less than 0.05 was used as a criterion for statistical significance.
Statistical analyses were carried out with the statistical package SAS® System version 9.3
(SAS Institute Inc, Cary, NC, USA).
Note:
(i)
An interaction is a condition in which the effect of one independent variable on
the dependent variable is different at different levels of the second independent
variable. In this study, independent variables were crown and impression, while
dependent variable was marginal fit. For example, a significant interaction
between impression and crown on marginal fit means that the influence of the
type of crowns on marginal fit was different for the two types of impression or the
influence of the type of impressions on marginal fit was different for the two
types of crown. If an interaction is non-significant, only the main effects are
tested, whereas when a significant interaction exists, the simple effects must be
tested.
(ii)
If there is a significant simple effect for independent variable A at given level of
independent variable B, it means that there is a significant relationship between
independent variable A and the dependent variable at that level of independent
variable B.
93
CHAPTER IV
RESULTS
Separate statistical analyses were conducted in order to assess the threedimensional (3D) and two-dimensional (2D) marginal and internal gaps of pressed and
CAD lithium disilicate crowns made from conventional and digital impressions.
3D Results
One-way ANOVA for 3D Marginal fit
Sixty study samples were used (n=15/per group). Marginal gap value of each
sample was an average of all 3D measurement values, and it was used for the statistical
analysis. Negative values were excluded from the study (Figure 19).
Figure 19. 3D measurement of the predefined area.
94
Table 6 and Figure 20 provide the final descriptive statistics of the 3D marginal
gap values for each experimental group. Results of one-way ANOVA revealed that there
was a significant effect for the type of the combinations of impression and crown on the
3D marginal fit (F(3,56)=15.73; p<0.0001). The post-hoc Tukey’s HSD test indicated
that the mean 3D marginal gap for conventional impressions with pressed crown was
significantly smaller than those obtained from other three experimental groups, and no
significant differences were found among digital impressions with pressed crown,
conventional impressions with CAD crown, and digital impressions with CAD crown.
Table 6 provides detailed results from the post-hoc Tukey’s HSD test.
Experimental Groups
N
15
Mean Marginal Gap
in mm (SD)
0.048 (0.009)
Group
Comparisons**
B
PVS/press (Group A)
PVS/CAD (Group B)
Lava/press (Group C)
Lava/CAD (Group D)
15
15
15
0.088 (0.024)
0.089 (0.020)
0.084 (0.021)
A
A
A
Table 6. Mean 3D marginal gap in mm of 4 experimental groups.
**
means with the same letter are not significantly different using the post-hoc Tukey’s
HSD test (P>.05).
95
0.12 0.1 0.08 0.06 mm 0.04 0.02 0 PVS/press (Group A) PVS/CAD (Group B) Lava/press (Group C) Lava/CAD (Group D) Figure 20. Mean 3D marginal gap of 4 experimental groups.
Two-way ANOVA for 3D Marginal fit
Results of two-way ANOVA revealed that there was a significant interaction
between impression techniques and crown types (F(1, 56)=20.10; p<0.0001). Subsequent
analyses demonstrated that there was a significant simple effect for the type of crowns
with conventional impression (p<0.0001) using a two-sample t-test. Results showed that
the mean 3D marginal gap for the pressed crowns was significantly smaller than that for
the CAD crowns (0.0476mm vs. 0.0877mm). However, no significant simple effect was
found for the type of crowns with digital impression. That is, with digital impressions, no
significant difference was found in the mean 3D marginal gap between the two crown
types (p=0.5574).
96
Analysis also showed that there was a significant simple effect for the type of
impressions with pressed crown (p<0.0001) using a two-sample t-test. Results showed
that the mean 3D marginal gap for the conventional impressions was significant less than
that for the digital impressions (0.0476mm vs. 0.0887mm). However, no significant
simple effect was found for the type of impressions with the CAD crowns. That is, with
the CAD crowns, there was no significant difference between the two impression
techniques (p=0.672).
2D Results
One-way ANOVA for 2D Marginal fit
Results of one-way ANOVA revealed that there was a significant effect for the
type of experimental groups on the 2D marginal fit (F(3,56)=12.27; p<0.0001). Detailed
results of one-way ANOVA are shown in Table 7. Subsequently, the post-hoc Tukey’s
HSD test indicated that the 2D marginal gap obtained from the PVS-press group was
significantly smaller than other three groups, while no significant difference was found
among those three groups.
Source
d.f.
SS
MS
F
Type of experimental groups
3
0.0139 0.0046 12.27
Within groups
56
0.0211 0.0004
Total
59
0.0350
d.f.: degrees of freedom; SS: sum of squares; MS: mean square; N=60
Table 7. Result of One-Way ANOVA for 2D marginal fit.
P value
<0.0001
97
Two-way ANOVA for 2D Marginal fit
Results of two-way ANOVA revealed that there was a significant interaction
between impression and crown on the 2D marginal fit (F(1, 56)=14.32; p=0.0004).
Detailed results of two-way ANOVA are shown in Table 8.
Source
d.f.
SS
MS
F
P value
Type of crowns
1
0.0044 0.0044 11.74
0.0012
Type of impressions
1
0.0041 0.0041 10.76
0.0018
Interaction between type of crowns
and type of impressions
1
0.0054 0.0054 14.32
0.0004
Within groups
56
0.0211 0.0004
Total
59
0.0350
d.f.: degrees of freedom; SS: sum of squares; MS: mean square; N=60
Table 8. Result of Two-Way ANOVA for 2D marginal fit.
Since a significant interaction was found, further analyses for simple effects were
conducted. The subsequent analyses demonstrated that there was a significant simple
effect for the type of crowns with PVS impression on the 2D marginal fit (p<0.0001, twosample t-test). Results showed that the mean 2D marginal gap for the pressed crowns was
significantly smaller than that for the CAD crowns (0.0399mm vs. 0.0760mm). However,
no significant simple effect was found for the type of crowns with the digital Lava
impressions (p=0.8177, two-sample test). That is, with the Lava digital impressions, no
98
significant difference was found in the 2D marginal fit between the two crown types
(Table 9).
Moreover, the data also showed that there was a significant simple effect for the
type of impressions with the pressed crowns on the 2D marginal fit (p<0.0001, twosample t-test). Results showed that the mean marginal gap for the PVS impressions was
significantly less than that for the digital impressions (0.0399mm vs. 0.0753mm).
However, no significant simple effect was found for the type of impressions with the
CAD crowns (p=0.7812, two-sample t-test). That is, with the CAD crowns, there was no
significant difference between the two impression techniques (Table 9).
Table 9 and Figure 21 provide the mean marginal gap and standard deviation of
the 2D marginal gap values for each experimental group.
Experimental groups
N
PVS/press (Group A)
PVS/CAD (Group B)
Lava/press (Group C)
Lava/CAD (Group D)
15
15
15
15
Mean Marginal Gap in mm
Group
(SD)
Comparisons**
0.0399 (0.0086)
B
0.0760 (0.0234)
A
0.0753 (0.0148)
A
0.0735 (0.0258)
A
Table 9. Pairwise comparisons of mean 2D marginal gap by experimental group.
***means with the same letter are not significantly different using post-hoc Tukey’s HSD
test (P>.05).
99
0.12 0.1 0.08 0.06 mm 0.04 0.02 0 PVS/press (Group A) PVS/CAD (Group B) Lava/press (Group C) Lava/CAD (Group D) Figure 21. Mean 2D marginal gap in mm.
One-way ANOVA for 2D Internal fit
Results of one-way ANOVA revealed that there was a significant effect for the
crown fabrication techniques on the 2D internal fit (F(3,56)=25.91; p<0.0001). Detailed
results of one-way ANOVA are shown in Table 10. Subsequently, the post-hoc Tukey’s
HSD test indicated that the 2D internal gap obtained from the Lava/press group was
significantly greater than other three groups, while no significant differences were found
between Lava/CAD and PVS/CAD, and between PVS/press and PVS/CAD. Table 10
provides detailed results from the post-hoc Tukey’s HSD test.
100
Source
d.f.
SS
MS
Type of experimental groups
3
Within groups
56 0.0690 0.0012
Total
59 0.1647
F
P value
0.0957 0.0319 25.91
<0.0001
d.f.: degrees of freedom; SS: sum of squares; MS: mean square; N=60
Table 10. Result of One-Way ANOVA for 2D internal fit.
Two-way ANOVA for 2D Internal fit
Results of two-way ANOVA revealed that there was a significant interaction
between impression technique and crown type on the 2D internal fit (F(1, 56)=15.22;
p=0.0003). Detailed results of two-way ANOVA are shown in Table 11.
Source
d.f.
SS
MS
F
P value
Type of crowns
1
0.0136 0.0136 11.03
0.0016
Type of impressions
1
0.0634 0.0634 51.47
<0.0001
Interaction between type of crowns
and type of impressions
1
0.0187 0.0187 15.22
0.0003
Within groups
56
0.0690 0.0012
Total
59
0.1647
d.f.: degrees of freedom; SS: sum of squares; MS: mean square; N=60
Table 11. Result of Two-Way ANOVA for 2D internal fit.
101
Since a significant interaction was found, further analyses for simple effects were
conducted. Subsequent analyses demonstrated that there was no significant simple effect
for the type of crowns with the PVS impressions on the 2D internal fit (p=0.6967, twosample t-test). That is, with PVS impression, no significant difference was found between
the two types of crown fabrication methods. However, results showed that there was a
significant simple effect on the 2D internal fit for the type of crowns with the digital
impressions (p<0.0001, two-sample t-test). The mean 2D internal gap for the pressed
crowns was significantly greater than that for the CAD crowns (0.2109mm vs.
0.1454mm) (Table 12).
Moreover, data also showed that there was a significant simple effect for the type
of impressions with the pressed crowns on the 2D internal fit (p<0.0001, two-sample ttest). Results showed that the mean 2D internal gap for the PVS impressions was
significantly smaller than that for the digital impressions (0.1105mm vs. 0.2109mm).
Also, a significant simple effect was found for the type of impressions with the CAD
crowns on the 2D internal fit (p=0.0011, two-sample t-test). That is, with the CAD
crowns, the mean 2D internal gap for the PVS impressions was significantly smaller than
that for the digital impressions (0.1158mm vs. 0.1454mm) (Table 12).
Table 12 and Figure 22 provide the final descriptive statistics of the 2D internal
gap values for each experimental group.
102
Experimental groups
N
15
Mean Internal Gap in mm
(SD)
0.1105 (0.0474)
Group
Comparisons**
C
PVS/press (Group A)
PVS/CAD (Group B)
15
0.1158 (0.0200)
B, C
Lava/press (Group C)
15
0.2109 (0.0410)
A
Lava/CAD (Group D)
15
0.1454 (0.0245)
B
Table 12. Pairwise comparisons of mean 2D internal gap by experimental group.
***means with the same letter are not significantly different using post-hoc Tukey’s HSD
test (P>.05).
0.3 0.25 0.2 0.15 mm 0.1 0.05 0 PVS/press (Group A) PVS/CAD (Group B) Figure 22. Mean 2D internal gap in mm.
Lava/press (Group C) Lava/CAD (Group D) 103
CHAPTER V
DISCUSSION
One of the main purposes of the study was to evaluate if there was an interaction
between the impression technique (conventional and digital) and the crown fabrication
method (press and CAD/CAM), considering the marginal and internal fit of the crowns
fabricated by any combination of those methods. There were no studies in the literature to
assess the adaptation of all-ceramic crowns made from the combination of those
techniques. Therefore, this study provided information as to how either impression
technique can be combined with either crown fabrication method in order to facilitate the
needs or the availability of each clinical practice. The marginal fit was the main
parameter tested, as it has been used extensively in the literature for similar studies, since
it is very critical for the quality and success of the prostheses. Moreover, the internal fit
was assessed in order to obtain a more complete picture as to how the crowns actually
adapted to the tooth surface.
This study, not only tested the new technology available in dentistry, but also
utilized similar industrial methodology in obtaining the measurements of the digital
specimens. The 3D and 2D data were obtained by digitizing the physical specimens. The
digital models could be moved, rotated, sectioned and measured as many times and in
any way as desired. This method has the potential of providing a vast amount of
information that was not possible before.
Results from this study indicated that the combination of conventional (PVS)
impression method and press fabrication technique produced the most accurate 3D
104
(0.048mm) and 2D (0.04mm) marginal adaptation. These results coincide with the
findings of previously published studies that compare the fit of pressed crowns to that of
cast crowns (which is still considered the gold standard) (72, 73).
More specifically, Baig et al. compared the marginal fit with respect to gap and
overhang of zirconia (Cercon Y-TZP) ceramic crowns to lithium disilicate pressable (IPS
Empress II) and complete metal crowns (control group) using a computerized digital
image analysis system (72). They found that the mean marginal gap for those three
groups was 66.4µm, 36.6µm and 37.1µm, respectively. The significantly higher marginal
gap of the Cercon crowns compared to IPS Empress II crowns was attributed to the type
of manufacturing of these 2 ceramic systems; the distortion of the ceramic coping was
thought to be less in IPS Empress II compared with Cercon, as the pressed technique
involves a less complicated process, using a more manual than computer program
computation, and is process dependent. Similarly, Stappert et al. evaluated the marginal
accuracy of partial coverage restorations made from gold, hybrid composite (Targis), IPS
e.max Press, IPS-Empress and ProCAD/Cerec under mouth-motion fatigue and thermal
cycling (73). They found that after cementation, the IPS e.max Press had similar marginal
fit to gold and IPS-Empress whereas the ProCAD group demonstrated decreased
marginal fit. Both of the above studies compared the pressed IPS e.max Press crowns to
CAD crowns. The marginal fit of the pressed crowns were 36.6µm and 60[52–67]µm
respectively. Despite the difference in the measurement methods, the present study found
very similar results regarding the marginal fit (3D: 48µm and 2D: 40µm) of the pressed
crowns from the conventional impressions.
105
The surprizing finding, in the present study, was that the pressed crowns made
from the digital impressions (Group C) had a statistically significant larger marginal gap
than the pressed crowns made from the conventional impressions (Group A). This means
that the combined techniques (digital impression/pressed crowns) were not as accurate as
the conventional impression/pressed crown combination. However, no difference was
found between the CAD/CAM crowns made from the conventional (Group B) and the
digital impressions (Group D), indicating that the combined techniques had similar
accuracy. Direct comparison between the pressed and the CAD/CAM fabrication
techniques should be done with caution, since the production methods are so different; in
other words, since for the CAD/CAM crowns the dies were scanned, there was the
possibility that any irregularities on the dies were “smoothed out” by the software in
order to facilitate the crown fabrication. The reason why the marginal gap of the Group B
was statistically larger than that of Group A, might be attributed to the overall fit of the
crown, which may have been affected by the internal adaptation. A thorough explanation
regarding the internal fit of Group C will follow below where the internal fit of the
crowns is discussed.
The early CAD/CAM systems were developed with the goal to simplify the
processing of dental prostheses while producing accurately fitted restorations. In the
1980s, this was not the reality due to the increased total cost, the increased operation time
and manipulation of the systems in comparison to the conventional techniques, inaccurate
mechanical milling of sharp corners and delicate margins (111). In addition to that, the
low resolution scanning and inadequate computing power also resulted in poor marginal
and internal fit of the produced prostheses (71). However, advancements in technology,
106
engineering and chemistry since then has led to the great variety of CAD/CAM systems
available today that use highly accurate scanners, more sophisticated software with high
precision in digitizing the complex shapes required in dentistry (70, 111, 112).
In this study, two of the newly introduced CAD/CAM systems were used; the
Lava™ C.O.S. (testing the impression technique) and the E4D scanner and milling
engine (testing the crown fabrication method). Taking into consideration the results of
either the 3D or the 2D measurements, no statistically significant differences were found
among the remaining three experimental groups; Conventional Impression/CAD Crown
(Group B), Digital Impressions/Pressed Crown (Group C), and Digital Impression/CAD
Crown (Group D). This means that, if we compare within the digital impression groups
(C and D), the fabrication of either a press or a CAD lithium disilicate crown will result
to similar marginal fit. Also, those results show that CAD/CAM crown margins can be
accurately produced when either a stone or a SLA model are scanned using the E4D
scanner.
Despite the statistical difference between Group A and the remaining three groups
for the marginal fit, the clinical difference might not be of great importance. Specifically,
the marginal gaps for Groups B, C, and D in 3D were 0.088mm, 0.089mm and 0.084mm
and in 2D were 0.076mm, 0.075mm and 0.074mm, respectively. It has been established
that a gap of less than 120µm is the clinical acceptable limit (8, 95).
Research is ongoing on digital impressions and several studies have been
conducted to evaluate the fit of the newly introduced systems. Similar to this study, only
in vivo, Syrek et al. compared the fit of all-ceramic crowns fabricated from intraoral
digital impressions with the fit of all-ceramic crowns fabricated from PVS impressions
107
(58). Two LavaTM (zirconia) crowns were fabricated for the same preparation in each of
20 patients. One crown was fabricated using the Lava™ C.O.S. and the other crown from
the PVS impression material. Prior to cementation, two calibrated and blinded examiners
clinically evaluated the fit of both crowns. The marginal fit was also scored using the
replica technique. The results revealed significant difference between the two groups; allceramic crowns resulting from Lava™ C.O.S. demonstrated significantly better marginal
fit than all-ceramic crowns fabricated from conventional impressions (both groups were
within clinically acceptability). Scotti et al. published a very similar paper to the above,
where they measured the marginal and internal fit of zirconia crowns made from Lava™
C.O.S. using the replica technique (55). Four different points were evaluated using
stereomicroscopy with a magnification of 50x. The results showed that all values were
clinically acceptable and the authors considered this method to be accurate enough to be
used as an alternative to conventional impressions. Both studies found that all-ceramic
CAD/CAM crowns (zirconia) made from the Lava™ C.O.S. were as accurate or even
more than the ones made from PVS impressions. Similar findings were shown in the
present study; when the CAD crowns (IPS e.max CAD), made from conventional and
Lava™ C.O.S. impressions (Group B vs. D), were compared, no significant differences
were found for both 3D and 2D measurements.
With regard to the internal fit, when the crown fabrication method was compared
within the digital impression groups (C and D), Group C (Lava/press) appeared to have
significantly bigger internal gap than Group D (Lava/CAD) (0.2109mm vs. 0.1454mm).
The same result was noted when the two impression techniques were compared within
the pressed groups (Group A and C). In that case Group C had significantly bigger
108
internal gap than Group A (PVS/press) (0.2109mm vs. 0.1105mm). Furthermore, when
all groups were considered as four individual experimental groups, and one-way ANOVA
with post-hoc Tukey’s HSD test was used to determine whether there was a significant
difference in the mean internal gap values among the groups, the only group with
statistical difference in internal fit was Group C (Lava/press). This showed that
consistently with any combination of analyses that when the pressed crowns were
fabricated on the SLA dies they had a larger internal gap. The 2D digital sections provide
the ability to see the adaptation of the crown on the die surfaces, and by evaluating those,
it was found that two of the crowns had very poor internal adaptation. The data of those
two were removed and the statistical analysis was repeated, thinking that maybe the
difference was due to those two “outliers”. However, the new analysis showed the same
statistical significance as the first one, indicating that the Group C had poorer internal
adaptation (a larger gap) when compared to the remaining three groups.
A suggestion for this occurrence was thought to be possible irregularities on the
SLA model surfaces as a result of the fabrication procedure that would not allow a
uniform internal adaptation of the crowns. The two SLA dies that produced the most
irregularly fitted pressed crowns were subsequently examined under the microscope
(10x), and no defects were detected. If there were defects on the SLA dies, since they
were randomly divided, the same appearance should be detected for Group D
(Lava/CAD) that also had the same type of SLA models. As mentioned above, the fact
that this was not noticed in that group might suggest that surface irregularities were not
the reason for poor adaptation, but it cannot be concluded because of the difference in
crown fabrication technique between the two groups. For the CAD/CAM crowns, the
109
SLA models were scanned, which could change the model surface either because of the
resolution of the scanner or because of processing of the software that would eliminate
any defects interfering with the CAD/CAM procedure.
Another suggestion for the poorer internal fit of Group C (Lava/press) was the use
and the type of die spacer. The die spacer used for this study was rubber-based,
recommended by the manufacturer (Ivoclar Vivadent). Although, this type of material
was used successfully with the stone dies, it might not be compatible with the SLA resin
models, leading to poor wettability of the dies. This would result in the material not
adapting evenly on all surfaces of the die and would cause a non-uniform or irregular
appearance of the intaglio of the crowns, as seen in Group C. This assumption is further
supported by the fact that, there was no statistical difference in the marginal fit of this
group when compared to B and D; since the area where the marginal gap measurements
were taken was not covered by die spacer.
For the internal fit, the results also revealed that within the CAD/CAM crown
fabrication method groups (Group B and D), the mean internal gap for PVS impression
(Group B) was significantly smaller than that for digital impression (Group D)
(0.1158mm vs. 0.1454mm). In other words, the combination of digital impression and
CAD/CAM crowns produced a poorer internal adaptation compared to the conventional
impression and CAD/CAM crown. The E4D scanner has established protocols for 3
different types of scanning: a. Intraoral scanning or direct digitalization, b. Scanning of
the impression or indirect digitalization and c. Scanning of the cast/model or indirect
digitalization. This scanner, therefore, should be able to capture data from surfaces with
different properties including translucency, reflection, smoothness etc. For this project,
110
the indirect digitalization was used, by scanning the stone and SLA models. The gypsum
and the resin dies have very different surfaces with stone being more opaque and smooth
and the resin being more reflective and less smooth due to the lines produced when
printed. It may be assumed that the scanner did not capture the data from the SLA model
with as high a degree of accuracy. It is common that most of the scanners available today,
in order to accurately capture the surface, need it to be coated with an opaque spray or
dye. The E4D claims to achieve that accuracy without the use of a spray, but it has not
been tested with SLA models before.
Hirayama et al. evaluated the internal and marginal fit of zirconia copings
generated from scanning definitive casts made from a conventional impression and
copings generated from a digital impression system (125). Specimens were divided into 2
groups: group A, Zirconia copings fabricated by scanning stone models from PVS
impressions and group B, Zirconia copings fabricated by scanning the master cast and
transmitting the scanned data to the Lava™ milling center in St. Paul, MN. To evaluate
the fit, the authors used the replica technique described by Boening et al. (32) and Molin
and Karlsson (31). They found that group B had a statistically better marginal adaptation
than group A. That study concluded that the both groups of copings had clinically
acceptable marginal fit; however the ones made form the digital impression had
significantly smaller marginal discrepancies. In this study, when the CAD/CAM crowns
(IPS e.max CAD) (Group B vs. D) were compared the crowns made from the Lava™
C.O.S. did not appear to have a statistically better marginal or internal fit than the ones
made from the conventional impressions. However, both groups had clinically acceptable
adaptation.
111
As described previously, Tuntiprawon and Wilson evaluated the effect of
increasing cement thickness (using platinum foil and die spacer) on the fracture strength
of all-ceramic crowns (14). They found that there was a decrease in strength when the
cement thickness was increased. The strength decrease was possibly attributed to the
greater deformation of the ceramic into the cement as well as the decreased thickness of
the crown itself. In this study the internal gap for Group C (Lava/press) at 0.2109mm was
almost twice as much as Group A (PVS/press) 0.1105, and significantly bigger than the
remaining two groups (0.1158mm and 0.1454mm respectively). This may result in
reduced fracture strength due to greater deformation of the ceramic into the cement when
the all-ceramic crowns are made with this combination of impression/crown fabrication
techniques, however this was not tested in this study.
Study design
As mentioned previously, an important limitation of the CAD/CAM prostheses is
marginal chipping due to machining induced damaged. Tsitrou et al. conducted a study in
order to investigate any possible correlation between the brittleness index (BI) of
machinable dental materials and the chipping factor (CF) of the final restorations (113).
The materials tested were Paradigm MZ100TM (3M/ESPE), Vita Mark II (VITA),
ProCAD (Ivoclar-Vivadent) and IPS e.max CAD (Ivoclar-Vivadent) milled in CEREC
system (Sirona Dental Systems Gmbh, Bensheim, Germany). Tsitrou et al. showed that
the CF increases as the BI increases, with Paradigm MZ100 having the lowest BI and CF,
and IPS e.max CAD demonstrating the highest BI and CF. Giannetopoulos et al.
112
investigated whether the CAD/CAM system would influence the marginal integrity of
IPS e.max CAD copings made with different finishing lines (114). The Cerec inEOS
system/Cerec 3D software and KAVO Everest system were compared. The finish lines
were 60-degree bevel, 30-degree bevel and 0-degree bevel (or 90-degree shoulder). The
CF was calculated, as in the above study (113); the CF was increased as the bevel angle
increased for Cerec group, whereas this factor did not influence the marginal integrity for
the Everest group. The conclusions of the study were that different milling processes
produce different amount of marginal chipping, although that was apparent only for the
60-degree bevel. Taking into consideration those two studies and the potential of
marginal chipping, in this study, the IPS e.max CAD crowns were designed with an
overhang. This limited the machining induced damage that could affect the results. After
the crowns were milled and before they were crystallized, they were adjusted under
microscope using a diamond-polishing disk, as recommended by the manufacturer
(Ivoclar Vivadent). Any chipping from the adjusting would be expected to be to a lesser
degree compared to the machining and it simulates normal clinical conditions. However,
no chipping was observed during the adjustment under the microscope.
Multiple techniques have been described in literature in order to measure the
marginal and internal fit of full coverage restorations. The most commonly found
nondestructive technique in literature is the replica technique (31-37). Replicas of the
intermediate space between the inner surface of the crown and tooth surface are made by
the method that was described by Molin and Karlsson (31). The important characteristic
of this technique is that it can be used in vivo as well as in vitro since it does not involve
the destruction of the specimens. However, handling of the materials, applied pressure
113
during setting, and positioning under the microscope are some of the limitations of this
technique.
For this particular study, a newly introduced digital method was selected for data
acquisition using the new triple-scan protocol developed by Holst et al. (97). By using a
non-contact scanner, three scans were performed: 1) Coping solo, 2) Master cast solo and
3) Coping placed on master cast in a clinically correct final position. After the objects
(coping and master cast) were digitized, STL files were generated from point clouds with
the scanner software (ATOS system, GOM mbH, Braunschweig, Germany). First, the
master cast STL file and the coping-master cast STL file were registered by manual
alignment followed by best-fit registration. Then the same was done to match the coping
and coping-master cast. The coping-master cast data was deleted and the aligned coping
to master cast data were used for fit assessment. To measure the cement gap, the outer
surface of the coping was deleted, followed by reversion of the surface normal of the
intaglio of the coping and calculation of deviations from the master cast. The authors
recommended that where high accuracy measurements are needed, a high precision
coordinate measurement machine (CMM) integrated with 3D laser scanning system
should be used (97).
In addition, the digital measurement technique was validated before applying it to
the definitive study. Part of the pilot study was the comparison of the new technique with
the replica technique that is well documented in the literature (31, 32, 96). Seven out of
ten variables had no statistical difference indicating that the two techniques produced
similar results. The variables that were significantly different were mainly the occlusal
measurements, which generally had a greater gap and variability (based on SD). No
114
difference was found in the margins, which was considered the more critical area of
measurement.
In the pilot study, the same scanner was used for both the fabrication of the CAD
crowns and the digitizing of the specimens. In order to avoid errors that could be
introduced by using the same scanner, for the final study, a CMM, the Surveyor ZSSeries scanner with scan accuracy of +/- 0.00898mm (Laser Design Inc, GKS,
Minneapolis, MN, USA), was used. The selection for the particular type of scanner was
based on Holst’s et al. recommendation that a CMM system should be used in order to
assure the best capture of the surfaces tested (98). This assured that any problems with
the scanner produced CAD crowns were not transferred to the next step of the study.
Moreover, by using such an accurate scanner that is used in several fields of engineering
with complex shapes and targets it was the best option available for the accuracy of this
project.
Usually for highly reflective or translucent materials (such as all-ceramic crowns)
the surfaces need to be coated which may introduce error. Similarly, in this case,
although low translucency ingots were used, the use of spray was still necessary to
acquire the best data quality, according to the operators of the scanner.
After the specimens were digitalized any type of section and measurement was
possible. Most of the studies, until now, presented 2D data, with fiduciary marks, either
sectioned or not, taken by photos or with microscopes (31-37). This limits the results to
the specific point measured without providing with any information for the fit as a whole.
The replica technique produced a 3D representation of the cement space but the actual
measurements were taken from the sections of it. A 3D measurement was not possible
115
with any of those instruments or techniques used. Holst et al. developed the triple
scanning protocol and made it possible to obtain the 3D fit of the entire contacting
surface (97).
For the 3D measurement, all the values (25,000-30,000) obtained by Geomagic
software were averaged and the mean was used for the comparisons. Any negative values
(denoting that the crown was smaller than the tooth) were excluded from the calculations,
since they do not represent a realistic scenario, but only a limitation of the software.
In this study, two different types of measurements were made by utilizing the
capacities of the software. The 2D measurements were done by sectioning the digital
specimens and defining 7 fiduciary points in each section. With those sections, it was
easier to visualize the internal gap in each part of the tooth desired, and also to compare it
with previous studies in the literature. However, it should be taken into account, that
direct comparisons with previous studies reporting 2D measurements made from physical
sections should be avoided because of the innate difference of a physical to a digital
model. For the statistical analysis, all the measurements obtained from each of the 7
fiduciary marks, where averaged, and the internal fit was one variable, instead of having
14 variables for each crown, that would complicate and obscure the analysis.
The marginal fit, as previously described, is considered the most important
criterion for clinical success and longevity, was assessed both by 3D and 2D
measurements. The 2D data set was the continuum of the internal fit fiduciary marks that
were defined, visually showing the distance of the intaglio from the tooth. The 3D
measurement provided a qualitative colored map of the defined area, indicating the
adaptation circumferentially, showing what other studies had failed to show before. The
116
width of the measured area (0.75mm) was identified as the area below the die spacer,
where the closest proximity is expected.
The fact that the 2D and 3D measurements resulted in the same conclusion, that
the Group A had the smallest marginal gap, with no difference among the remaining
three groups, validated the reliability of the software and the protocol used. The
consistent 10µm difference between the two data sets was due to the different processing
of the software when calculating 3D versus 2D data, and not due to an error in the
developed protocol.
Possible limitations of the study
The main limitation of the study was the software used for the obtaining the
measurements. After using the Best-Fit Alignment twice, the fit had to be adjusted
manually in order to simulate a clinically relevant crown position. The Best-Fit
Alignment finds the path of least resistance between the two objects and then
superimposes them. This may result in a situation where the crown seems to be “inside”
the tooth. Each time a crown was fitted, a section was made and if it seemed like it is
“inside” the tooth, it was manually moved until the closest marginal and internal fit was
achieved. However, the fact that the fit was improved at the given section does not mean
that it was correctly seated three dimensionally. The protocol used for the digital fitting
was developed with the assistance of the Geomagic technical support and this was the
best result they could assure.
Other limitations include the use of rubber-based die spacer on the SLA models,
the grinding of the overhanging margin of the CAD crowns and the spray used for
117
digitizing the crowns and the master die. In addition, the crowns were not cemented on
the master die as they would in a clinical setting; cementation may produce different
results.
Avenues for future research
With the introduction of the 3D digital measurements, by using the triple scanning
protocol by Holst at al. (97) and a sophisticated processing software, the door has opened
to unlimited research in the fit of dental restorations. The standardization, the nondestructive nature, the rapid processing of data and the storage/availability of that
information will enable the comparison and analysis of any material desired. The infinite
designs of measurements will allow for very detailed and consistent data acquisition.
Clinical significance
Any combination of PVS or Lava™ C.O.S. impression with press or CAD lithium
disilicate crowns will result to a clinically acceptable restoration considering the marginal
and internal fit. However, when the strength of the crown is taken into consideration, the
increased internal gap of the all-ceramic pressed crowns made from Lava™ C.O.S.
impressions and SLA dies may predispose to a reduced fracture resistance that could
compromise the longevity and survival of the restoration.
118
CHAPTER VI
CONCLUSIONS
This study examined the three-dimensional and two-dimensional marginal and internal fit
of pressed and CAD/CAM lithium disilicate crowns made from conventional and digital
impressions. Based on the results the null hypotheses were rejected and the alternative
were accepted:
•
There was a difference in accuracy between the two impression techniques,
conventional and digital, considering the marginal and internal fit of the crowns
fabricated by those methods.
•
There was a difference in accuracy between the crown fabrication methods, press
and CAD/CAM, considering the marginal and internal fit of the crowns fabricated
by those methods.
•
There was an interaction between the impression technique (conventional and
digital) and the crown fabrication method (press and CAD/CAM), considering the
marginal and internal fit of the crowns fabricated by any combination of those
methods.
Within the limitations of the present study, the following conclusions were drawn:
•
The combination of the conventional impression and the pressed crown produced
the most accurate marginal fit.
119
•
There was no statistical difference among the conventional impression/CAD
crown, digital impression/ press crown and digital impression/CAD/CAM crown
with regard to the marginal fit.
•
The combination of the digital impression and pressed crown produced the least
accurate internal fit.
•
There was no statistical difference among the conventional impression/CAD
crown, conventional impression/press crown and digital impression/CAD crown
with regard to the internal fit.
•
All combinations produced crowns with clinically acceptable marginal fit.
120
APPENDIX A
RAW DATA
Table A1. Average marginal gap for 3D measurements.
SAMPLE
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
1
2
3
4
GROUP
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
3
3
3
3
MARGINAL GAP
0.0593
0.0378
0.0595
0.0494
0.0452
0.0427
0.0389
0.0559
0.0441
0.0542
0.0581
0.0403
0.0548
0.0395
0.0336
0.0791
0.0922
0.1278
0.0923
0.132
0.1038
0.0695
0.0797
0.0561
0.0691
0.0715
0.0613
0.1191
0.0744
0.0877
0.0826
0.0703
0.1116
0.0889
CROWN
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
IMPRESSION
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
121
5
6
7
8
9
10
11
12
13
14
15
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
3
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
Table A1. Continued.
0.0809
0.0498
0.1134
0.0805
0.0915
0.0843
0.0834
0.0969
0.0814
0.1346
0.0798
0.0534
0.1184
0.0848
0.0689
0.0684
0.0803
0.0623
0.1185
0.0771
0.0885
0.068
0.0845
0.1245
0.0918
0.0734
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
122
Table A2. Average marginal and internal gaps for 2D measurements.
SAMPLE
1
2
3
4
5
6
7
8
19
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
GROUP
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
MARG. GAP
0.047
0.036125
0.0485
0.04475
0.028125
0.03575
0.04175
0.04525
0.04275
0.059625
0.037375
0.04
0.033
0.027875
0.030375
0.075125
0.08375
0.11175
0.0835
0.101875
0.092375
0.064375
0.068875
0.040875
0.045875
0.057375
0.049125
0.116375
0.061875
0.0875
0.08675
0.062625
0.08975
0.067625
0.061125
0.0445
INTER. GAP
0.08
0.056916667
0.124666667
0.103
0.082333333
0.064166667
0.099333333
0.132166667
0.2535
0.085333333
0.112666667
0.138333333
0.142
0.104833333
0.0785
0.124
0.126
0.139333333
0.0855
0.134
0.134
0.117666667
0.095166667
0.105166667
0.091
0.115666667
0.103333333
0.157166667
0.102333333
0.106333333
0.222166667
0.175166667
0.262166667
0.259666667
0.157333333
0.164333333
IMPRESSION
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
CROWN
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
123
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
2
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
4
4
4
4
4
Table A2. Continued.
0.087875
0.0775
0.089375
0.06775
0.077125
0.09075
0.0545
0.08925
0.083125
0.037875
0.119125
0.070875
0.0455
0.068125
0.075875
0.048875
0.107625
0.0655
0.070125
0.04775
0.076375
0.116625
0.095875
0.056625
0.243333333
0.194833333
0.216
0.187333333
0.177
0.2305
0.201
0.176
0.296333333
0.114833333
0.1575
0.164
0.116666667
0.1335
0.112
0.107666667
0.167333333
0.149833333
0.173166667
0.131833333
0.163666667
0.184833333
0.153833333
0.150833333
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
124
APPENDIX B
GEOMAGIC IMAGES
Three-dimensional (3D) and two-dimensional (2D) images of one indicative specimen
from each experimental group.
Group A
Figure B1. Group A (PVS/press) 3D colored map.
125
Figure B2. Group A (PVS/press) Facial-Lingual section for 2D measurements.
Figure B3. Group A (PVS/press) Mesial-Distal section for 2D measurements.
126
Group B
Figure B4. Group B (PVS/CAD) 3D colored map.
127
Figure B5. Group B (PVS/CAD) Facial-Lingual section for 2D measurements.
Figure B6. Group B (PVS/CAD) Mesial-Distal section for 2D measurements.
128
Group C
Figure B7. Group C (Lava/press) 3D colored map.
129
Figure B8. Group C (Lava/press) Facial-Lingual section for 2D measurements.
Figure B9. Group C (Lava/press) Mesial-Distal section for 2D measurements
130
Group D
Figure B10. Group D (Lava/CAD) 3D colored map.
131
Figure B11. Group D (Lava/CAD) Facial-Lingual section for 2D measurements.
Figure B12. Group D (Lava/CAD) Mesial-Distal section for 2D measurements.
132
REFERENCES
1. White SN, Ingles S, Kipnis V. Influence of marginal opening on microleakage of
cemented artificial crowns. J Prosthet Dent. 1994 Mar;71(3):257-64.
2. Schwartz NL, Whitsett LD, Berry TG, Stewart JL. Unserviceable crowns and fixed
partial dentures: Life-span and causes for loss of serviceability. J Am Dent Assoc. 1970
Dec;81(6):1395-401.
3. Jahn KR, Baum W, Zuhrt R. Secondary caries frequency under complete crowns in
relation to the material and design of the crown as well as the crown margin finish.
Stomatol DDR. 1985 Nov;35(11):665-70.
4. Jacobs MS, Windeler AS. An investigation of dental luting cement solubility as a
function of the marginal gap. J Prosthet Dent. 1991 Mar;65(3):436-42.
5. Bader JD, Rozier RG, McFall WT,Jr, Ramsey DL. Effect of crown margins on
periodontal conditions in regularly attending patients. J Prosthet Dent. 1991 Jan;65(1):759.
6. Zoellner A, Bragger U, Fellmann V, Gaengler P. Correlation between clinical scoring
of secondary caries at crown margins and histologically assessed extent of the lesions. Int
J Prosthodont. 2000 Nov-Dec;13(6):453-9.
7. Reeves WG. Restorative margin placement and periodontal health. J Prosthet Dent.
1991 Dec;66(6):733-6.
8. McLean JW, von Fraunhofer JA. The estimation of cement film thickness by an in
vivo technique. Br Dent J. 1971 Aug 3;131(3):107-11.
9. Campagni WV, Wright W, Martinoff JT. Effect of die spacer on the seating of
complete cast gold crowns with grooves. J Prosthet Dent. 1986 Mar;55(3):324-8.
10. Eames WB, O'Neal SJ, Monteiro J, Miller C, Roan JD,Jr, Cohen KS. Techniques to
improve the seating of castings. J Am Dent Assoc. 1978 Mar;96(3):432-7.
11. Grajower R, Lewinstein I. A mathematical treatise on the fit of crown castings. J
Prosthet Dent. 1983 May;49(5):663-74.
12. Wilson PR. Effect of increasing cement space on cementation of artificial crowns. J
Prosthet Dent. 1994 Jun;71(6):560-4.
13. Olivera AB, Saito T. The effect of die spacer on retention and fitting of complete cast
crowns. J Prosthodont. 2006 Jul-Aug;15(4):243-9.
133
14. Tuntiprawon M, Wilson PR. The effect of cement thickness on the fracture strength
of all-ceramic crowns. Aust Dent J. 1995 Feb;40(1):17-21.
15. Bottino MA, Valandro LF, Buso L, Ozcan M. The influence of cervical finish line,
internal relief, and cement type on the cervical adaptation of metal crowns. Quintessence
Int. 2007 Jul-Aug;38(7):e425-32.
16. Ayad MF. Effects of tooth preparation burs and luting cement types on the marginal
fit of extracoronal restorations. J Prosthodont. 2009 Feb;18(2):145-51.
17. Fusayama T, Ide K, Hosoda H. Relief of resistance of cement of full cast crowns.
J Prosthet Dent. 1964;14(1):95-106.
18. Holmes JR, Bayne SC, Holland GA, Sulik WD. Considerations in measurement of
marginal fit. J Prosthet Dent. 1989 Oct;62(4):405-8.
19. Sorensen JA. A standardized method for determination of crown margin fidelity. J
Prosthet Dent. 1990 Jul;64(1):18-24.
20. Hayashi M, Watts DC, Ebisu S, Wilson NH. Influence of vision on the evaluation of
marginal discrepancies in restorations. Oper Dent. 2005 Sep-Oct;30(5):598-601.
21. Hayashi M, Wilson NH, Ebisu S, Watts DC. Influence of explorer tip diameter in
identifying restoration margin discrepancies. J Dent. 2005 Sep;33(8):669-74.
22. Leknius C, Giusti L, Chambers D, Hong C. Effects of clinical experience and
explorer type on judged crown margin acceptability. J Prosthodont. 2010 Feb;19(2):13843.
23. Assif D, Antopolski B, Helft M, Kaffe I. Comparison of methods of clinical
evaluation of the marginal fit of complete cast gold crowns. J Prosthet Dent. 1985
Jul;54(1):20-4.
24. Brukl CE, Philp GK. The fit of molded all-ceramic, twin foil, and conventional
ceramic crowns. J Prosthet Dent. 1987 Oct;58(4):408-13.
25. Hunt JL, Cruickshanks-Boyd DW, Davies EH. The marginal characteristics of
collarless bonded porcelain crowns produced using a separating medium technique.
Quintessence Dent Technol. 1978 Nov;2(9):21-6.
26. Romeo E, Iorio M, Storelli S, Camandona M, Abati S. Marginal adaptation of fullcoverage CAD/CAM restorations: In vitro study using a non-destructive method.
Minerva Stomatol. 2009 Mar;58(3):61-72.
134
27. Tan PL, Gratton DG, Diaz-Arnold AM, Holmes DC. An in vitro comparison of
vertical marginal gaps of CAD/CAM titanium and conventional cast restorations. J
Prosthodont. 2008 Jul;17(5):378-83.
28. Gonzalo E, Suarez MJ, Serrano B, Lozano JF. Comparative analysis of two
measurement methods for marginal fit in metal-ceramic and zirconia posterior FPDs. Int
J Prosthodont. 2009 Jul-Aug;22(4):374-7.
29. Mitchell CA, Pintado MR, Douglas WH. Nondestructive, in vitro quantification of
crown margins. J Prosthet Dent. 2001 Jun;85(6):575-84.
30. Pelekanos S, Koumanou M, Koutayas SO, Zinelis S, Eliades G. Micro-CT evaluation
of the marginal fit of different in-ceram alumina copings. Eur J Esthet Dent. 2009
Autumn;4(3):278-92.
31. Molin M, Karlsson S. The fit of gold inlays and three ceramic inlay systems. A
clinical and in vitro study. Acta Odontol Scand. 1993 Aug;51(4):201-6.
32. Boening KW, Wolf BH, Schmidt AE, Kastner K, Walter MH. Clinical fit of procera
AllCeram crowns. J Prosthet Dent. 2000 Oct;84(4):419-24.
33. Coli P, Karlsson S. Fit of a new pressure-sintered zirconium dioxide coping. Int J
Prosthodont. 2004 Jan-Feb;17(1):59-64.
34. Nakamura T, Tanaka H, Kinuta S, Akao T, Okamoto K, Wakabayashi K, et al. In
vitro study on marginal and internal fit of CAD/CAM all-ceramic crowns. Dent Mater J.
2005 Sep;24(3):456-9.
35. Kokubo Y, Nagayama Y, Tsumita M, Ohkubo C, Fukushima S, Vult von Steyern P.
Clinical marginal and internal gaps of in-ceram crowns fabricated using the GN-I system.
J Oral Rehabil. 2005 Oct;32(10):753-8.
36. Kokubo Y, Ohkubo C, Tsumita M, Miyashita A, Vult von Steyern P, Fukushima S.
Clinical marginal and internal gaps of procera AllCeram crowns. J Oral Rehabil. 2005
Jul;32(7):526-30.
37. Reich S, Uhlen S, Gozdowski S, Lohbauer U. Measurement of cement thickness
under lithium disilicate crowns using an impression material technique. Clin Oral
Investig. 2011 Aug;15(4):521-6.
38. Luthardt RG, Bornemann G, Lemelson S, Walter MH, Huls A. An innovative method
for evaluation of the 3-D internal fit of CAD/CAM crowns fabricated after direct optical
versus indirect laser scan digitizing. Int J Prosthodont. 2004 Nov-Dec;17(6):680-5.
135
39. Holst S., Tawdrous RE, Karl M. Description of a novel technique for threedimensional fit assessment of dental restorations. 6th world congress of biomechanics,
IFMBE proceedings; August 1–6, 2010; Singapore. Springer; 2010.
40. Anusavice K, editor. Philips’ science of dental materials. 10th ed. ; 1996.
41. Powers JM SR, editor. Craig’s restorative dental materials. 12th ed. Elsevier; 2006.
42. Donovan TE, Chee WW. A review of contemporary impression materials and
techniques. Dent Clin North Am. 2004 Apr;48(2):vi,vii, 445-70.
43. Michalakis KX, Bakopoulou A, Hirayama H, Garefis DP, Garefis PD. Pre- and postset hydrophilicity of elastomeric impression materials. J Prosthodont. 2007 JulAug;16(4):238-4.
44. Chee WW, Donovan TE. Fine detail reproduction of very high viscosity poly(vinyl
siloxane) impression materials. Int J Prosthodont. 1989 Jul-Aug;2(4):368-70.
45. Johnson GH, Craig RG. Accuracy of four types of rubber impression materials
compared with time of pour and a repeat pour of models. J Prosthet Dent. 1985
Apr;53(4):484-90.
46. Lacy AM, Bellman T, Fukui H, Jendresen MD. Time-dependent accuracy of
elastomer impression materials. part I: Condensation silicones. J Prosthet Dent. 1981
Feb;45(2):209-15.
47. Lacy AM, Fukui H, Bellman T, Jendresen MD. Time-dependent accuracy of
elastomer impression materials. part II: Polyether, polysulfides, and polyvinylsiloxane. J
Prosthet Dent. 1981 Mar;45(3):329-33.
48. Hung SH, Purk JH, Tira DE, Eick JD. Accuracy of one-step versus two-step putty
wash addition silicone impression technique. J Prosthet Dent. 1992 May;67(5):583-9.
49. Mishra S, Chowdhary R. Linear dimensional accuracy of a polyvinyl siloxane of
varying viscosities using different impression techniques. J Investig Clin Dent.
2010;1:37-46.
50. Valderhaug J, Floystrand F. Dimensional stability of elastomeric impression materials
in custom-made and stock trays. J Prosthet Dent. 1984 Oct;52(4):514-7.
51. Rueda LJ, Sy-Munoz JT, Naylor WP, Goodacre CJ, Swartz ML. The effect of using
custom or stock trays on the accuracy of gypsum casts. Int J Prosthodont. 1996 JulAug;9(4):367-73.
136
52. Dixon DL, Breeding LC, Brown JS. The effect of custom tray material type and
adhesive drying time on the tensile bond strength of an impression material/adhesive
system. Int J Prosthodont. 1994 Mar-Apr;7(2):129-33.
53. Thongthammachat S, Moore BK, Barco MT,2nd, Hovijitra S, Brown DT, Andres CJ.
Dimensional accuracy of dental casts: Influence of tray material, impression material, and
time. J Prosthodont. 2002 Jun;11(2):98-108.
54. Logozzo S, Franceschini G, Kilpelä A, Caponi M, Governi L, Blois L. A comparative
analysis of intraoral 3d digital scanners for restorative dentistry. The Internet Journal of
Medical Technology [Internet]. 2011;5(1). Available from:
10.5580/1b90#sthash.nKoGlwm3.dpuf.
55. Scotti R, Cardelli P, Baldissara P, Monaco C. Clinical fitting of CAD/CAM zirconia
single crowns generated from digital intraoral impressions based on active wavefront
sampling. J Dent. 2011 Oct 17.
56. Beuer F, Schweiger J, Edelhoff D. Digital dentistry: An overview of recent
developments for CAD/CAM generated restorations. Br Dent J. 2008 May
10;204(9):505-11.
57. Strub JR, Rekow ED, Witkowski S. Computer-aided design and fabrication of dental
restorations: Current systems and future possibilities. J Am Dent Assoc. 2006
Sep;137(9):1289-96.
58. Syrek A, Reich G, Ranftl D, Klein C, Cerny B, Brodesser J. Clinical evaluation of allceramic crowns fabricated from intraoral digital impressions based on the principle of
active wavefront sampling. J Dent. 2010 Jul;38(7):553-9.
59. Fasbinder DJ. Digital dentistry: Innovation for restorative treatment. Compend Contin
Educ Dent. 2010;31 Spec No 4:2-11.
60. Birnbaum NS, Aaronson HB. Dental impressions using 3D digital scanners: Virtual
becomes reality. Compend Contin Educ Dent. 2008 Oct;29(8):494, 496, 498-505.
61. Birnbaum NS, Aaronson HB, Stevens C, Cohen B. 3D digital scanners: A high-tech
approcah to more accurate dental impressions. Inside Dentistry. 2009 4/2/2009;5(4):70-7.
62. Seelbach P, Brueckel C, Wostmann B. Accuracy of digital and conventional
impression techniques and workflow. Clin Oral Investig. 2012 Oct 21.
63. Plourde J, Harsono M, Fox L, Hill TJ, Finkelman M, Kugel G. Marginal and internal
fit of E4D CAD/CAM all-ceramic crowns. J Dent R. 2011;90(A):Abstract # 638.
137
64. Matthes J, Silva N, Wolff MS, Witek L, Zavanelli RA, Conciatori L, et al. Marginal
microscopic analysis of CAD/CAM all ceramic crown. J Dent R. 2011;90(A):Abstract #
3200.
65. Denry I, Holloway J. Ceramics for dental applications: A review. Materials [Internet].
2010;3(1):11 January 2010,351-368. Available from: www.mdpi.com/journal/materials.
66. Holand W, Schweiger M, Watzke R, Peschke A, Kappert H. Ceramics as biomaterials
for dental restoration. Expert Rev Med Devices. 2008 Nov;5(6):729-45.
67. Conrad HJ, Seong WJ, Pesun IJ. Current ceramic materials and systems with clinical
recommendations: A systematic review. J Prosthet Dent. 2007 Nov;98(5):389-404.
68. Kelly JR. Dental ceramics: Current thinking and trends. Dent Clin North Am. 2004
Apr;48(2):viii, 513-30.
69. Holden JE, Goldstein GR, Hittelman EL, Clark EA. Comparison of the marginal fit of
pressable ceramic to metal ceramic restorations. J Prosthodont. 2009 Dec;18(8):645-8.
70. Lee KB, Park CW, Kim KH, Kwon TY. Marginal and internal fit of all-ceramic
crowns fabricated with two different CAD/CAM systems. Dent Mater J. 2008
May;27(3):422-6.
71. McLaren EA, Terry DA. CAD/CAM systems, materials, and clinical guidelines for
all-ceramic crowns and fixed partial dentures. Compend Contin Educ Dent. 2002
Jul;23(7):637-53.
72. Baig MR, Tan KB, Nicholls JI. Evaluation of the marginal fit of a zirconia ceramic
computer-aided machined (CAM) crown system. J Prosthet Dent. 2010 Oct;104(4):21627.
73. Stappert CF, Chitmongkolsuk S, Silva NR, Att W, Strub JR. Effect of mouth-motion
fatigue and thermal cycling on the marginal accuracy of partial coverage restorations
made of various dental materials. Dent Mater. 2008 Sep;24(9):1248-57.
74. Miyazaki T, Hotta Y. CAD/CAM systems available for the fabrication of crown and
bridge restorations. Aust Dent J. 2011 Jun;56 Suppl 1:97-106.
75. Culp L, McLaren EA. Lithium disilicate: The restorative material of multiple options.
Compend Contin Educ Dent. 2010 Nov-Dec;31(9):716,20, 722, 724-5.
76. Denry I, Kelly JR. State of the art of zirconia for dental applications. Dent Mater.
2008 Mar;24(3):299-307.
138
77. Sailer I, Feher A, Filser F, Gauckler LJ, Luthy H, Hammerle CH. Five-year clinical
results of zirconia frameworks for posterior fixed partial dentures. Int J Prosthodont. 2007
Jul-Aug;20(4):383-8.
78. Fahmy NZ. Influence of veneering materials on the marginal fit and fracture
resistance of an alumina core system. J Prosthodont. 2011 Jan;20(1):45-51.
79. Fradeani M, Redemagni M. An 11-year clinical evaluation of leucite-reinforced glassceramic crowns: A retrospective study. Quintessence Int. 2002 Jul-Aug;33(7):503-10.
80. Heintze SD, Rousson V. Fracture rates of IPS empress all-ceramic crowns--a
systematic review. Int J Prosthodont. 2010 Mar-Apr;23(2):129-33.
81. El-Mowafy O, Brochu JF. Longevity and clinical performance of IPS-empress
ceramic restorations--a literature review. J Can Dent Assoc. 2002 Apr;68(4):233-7.
82. Murgueitio R, Bernal G. Three-year clinical follow-up of posterior teeth restored with
leucite-reinforced ips empress onlays and partial veneer crowns. J Prosthodont. 2012
Jul;21(5):340-5.
83. Stappert CF, Dai M, Chitmongkolsuk S, Gerds T, Strub JR. Marginal adaptation of
three-unit fixed partial dentures constructed from pressed ceramic systems. Br Dent J.
2004 Jun 26;196(12):766-70.
84. Marquardt P, Strub JR. Survival rates of IPS empress 2 all-ceramic crowns and fixed
partial dentures: Results of a 5-year prospective clinical study. Quintessence Int. 2006
Apr;37(4):253-9.
85. Tysowski GW. The science behind lithium disilicate: A metal-free alternative.
Dentistry Today 03/01/2009.
86. Aboushelib MN, de Jager N, Kleverlaan CJ, Feilzer AJ. Effect of loading method on
the fracture mechanics of two layered all-ceramic restorative systems. Dent Mater. 2007
Aug;23(8):952-9.
87. Guess PC, Zavanelli RA, Silva NR, Bonfante EA, Coelho PG, Thompson VP.
Monolithic CAD/CAM lithium disilicate versus veneered Y-TZP crowns: Comparison of
failure modes and reliability after fatigue. Int J Prosthodont. 2010 Sep-Oct;23(5):434-42.
88. Schmitter M, Mueller D, Rues S. Chipping behaviour of all-ceramic crowns with
zirconia framework and CAD/CAM manufactured veneer. J Dent. 2012 Feb;40(2):15462.
89. Etman MK. Confocal examination of subsurface cracking in ceramic materials. J
Prosthodont. 2009 Oct;18(7):550-9.
139
90. Wiedhahn K. From blue to white: New high-strength material for cerec--IPS e.max
CAD LT. Int J Comput Dent. 2007 Jan;10(1):79-91.
91. Pjetursson BE, Sailer I, Zwahlen M, Hammerle CH. A systematic review of the
survival and complication rates of all-ceramic and metal-ceramic reconstructions after an
observation period of at least 3 years. part I: Single crowns. Clin Oral Implants Res. 2007
Jun;18 Suppl 3:73-85.
92. Guess PC, Strub JR, Steinhart N, Wolkewitz M, Stappert CF. All-ceramic partial
coverage restorations--midterm results of a 5-year prospective clinical splitmouth study. J
Dent. 2009 Aug;37(8):627-3.
93. Etman MK, Woolford MJ. Three-year clinical evaluation of two ceramic crown
systems: A preliminary study. J Prosthet Dent. 2010 Feb;103(2):80-9.
94. Fasbinder DJ, Dennison JB, Heys D, Neiva G. A clinical evaluation of chairside
lithium disilicate CAD/CAM crowns: A two-year report. J Am Dent Assoc. 2010 Jun;141
Suppl 2:10S-4S.
95. Christensen GJ. Marginal fit of gold inlay castings. J Prosthet Dent. 1966 MarApr;16(2):297-305.
96. Rahme HY, Tehini GE, Adib SM, Ardo AS, Rifai KT. In vitro evaluation of the
"replica technique" in the measurement of the fit of procera crowns. J Contemp Dent
Pract. 2008 Feb 1;9(2):25-32.
97. Holst S, Karl M, Wichmann M, Matta RE. A new triple-scan protocol for 3D fit
assessment of dental restorations. Quintessence Int. 2011 Sep;42(8):651-7.
98. Laser desing inc and GKS [Internet]. Available from:
http://www.laserdesign.com/resources_and_downloads/faq/.
99. Marks P. Capturing a competitive edge through digital shape sampling & processing
(DSSP). SME Blue Book Series ed. Society of Manufacturing Engineers; 2005.
100. Geomagic [Internet]. Available from:
http://dl.geomagic.com/media/marketing/2012_Brochures/MASTER12_29_11_QQP_A4_English_eVersion.pdf.
101. Leong DK, Chai JY, Gilbert JL. Marginal fit of machine-milled and cast titanium
single crowns. Northwest Dent Res. 1994 Winter;4(2):13-4.
102. Harris IR, Wickens JL. A comparison of the fit of spark-eroded titanium copings
and cast gold alloy copings. Int J Prosthodont. 1994 Jul-Aug;7(4):348-55.
140
103. Yeo IS, Yang JH, Lee JB. In vitro marginal fit of three all-ceramic crown systems. J
Prosthet Dent. 2003 Nov;90(5):459-64.
104. Stappert CF, Denner N, Gerds T, Strub JR. Marginal adaptation of different types of
all-ceramic partial coverage restorations after exposure to an artificial mouth. Br Dent J.
2005 Dec 24;199(12):779,83; discussion 777.
105. Walker MP, Petrie CS, Haj-Ali R, Spencer P, Dumas C, Williams K. Moisture effect
on polyether and polyvinylsiloxane dimensional accuracy and detail reproduction. J
Prosthodont. 2005 Sep;14(3):158-63.
106. Klooster J, Logan GI, Tjan AH. Effects of strain rate on the behavior of elastomeric
impression. J Prosthet Dent. 1991 Sep;66(3):292-8.
107. Eames WB, Sieweke JC. Seven acrylic resins for custom trays and five putty-wash
systems compared. Oper Dent. 1980 Autumn;5(4):162-7.
108. Lewinstein I. The ratio between vertical and horizontal changes of impressions. J
Oral Rehabil. 1993 Jan;20(1):107-14.
109. Kenyon BJ, Hagge MS, Leknius C, Daniels WC, Weed ST. Dimensional accuracy
of 7 die materials. J Prosthodont. 2005 Mar;14(1):25-31.
110. Ragain JC, Grosko ML, Raj M, Ryan TN, Johnston WM. Detail reproduction,
contact angles, and die hardness of elastomeric impression and gypsum die material
combinations. Int J Prosthodont. 2000 May-Jun;13(3):214-20.
111. Miyazaki T, Hotta Y, Kunii J, Kuriyama S, Tamaki Y. A review of dental
CAD/CAM: Current status and future perspectives from 20 years of experience. Dent
Mater J. 2009 Jan;28(1):44-56.
112. Shannon AJT, Qian F, Tan P, Gratton DG. In vitro horizontal marginal adaptation
comparison of CAD/CAM zirconium copings. J Dent R. 2008;87(A):Abstract #0188.
113. Tsitrou EA, Northeast SE, van Noort R. Brittleness index of machinable dental
materials and its relation to the marginal chipping factor. J Dent. 2007 Dec;35(12):897902.
114. Giannetopoulos S, van Noort R, Tsitrou E. Evaluation of the marginal integrity of
ceramic copings with different marginal angles using two different CAD/CAM systems. J
Dent. 2010 Dec;38(12):980-6.
115. Cohen A, Laviv A, Berman P, Nashef R, Abu-Tair J. Mandibular reconstruction
using stereolithographic 3-dimensional printing modeling technology. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod. 2009 Nov;108(5):661-6.
141
116. Bill JS, Reuther JF, Dittmann W, Kubler N, Meier JL, Pistner H, et al.
Stereolithography in oral and maxillofacial operation planning. Int J Oral Maxillofac
Surg. 1995 Feb;24(1 Pt 2):98-103.
117. Ogledzki M, Wenzel K, Doherty E, Kugel G. Accuracy of 3M-brontes
stereolithography models compared to plaster models. J Dent R. 2010;89(A):Abstract
#1060.
118. Moore W, Dunne P, Doherty E, Nelson M, Finkelman M, Kugel G. Margin
characteristics of PFM crown copings fabricated on stereolithography models. 3M ESPE
Web site: 3MESPE com [Internet]. Available from:
http://multimedia.3m.com/mws/mediawebserver?mwsId=SSSSSufSevTsZxtUO8_xnYt9
evUqevTSevTSevTSeSSSSSS--.
119. Lava chairside oral scanner C.O.S. [Internet]. Technical Datasheet: 3M ESPE; 2009.
Available from: www.multimedia.3m.com.
120. Hart D, Lammerding J, Rohaly J, inventors; 3-D imaging system. US patent
2004/0155975 A1. 2004 Aug 12.
121. Ender A, Mehl A. Full arch scans: Conventional versus digital impressions--an invitro study. Int J Comput Dent. 2011;14(1):11-2.
122. Van der Meer WJ, Andriessen FS, Wismeijer D, Ren Y. Application of intra-oral
dental scanners in the digital workflow of implantology. PLoS One [Internet]. 2012 2012
August 22;7(8). Available from:
http://dx.crossref.org/10.1371%2Fjournal.pone.0043312.
123. Guth JF, Keul C, Stimmelmayr M, Beuer F, Edelhoff D. Accuracy of digital models
obtained by direct and indirect data capturing. Clin Oral Investig. 2012 Jul 31.
124. Balakrishnama S, Wenzel K, Bergeron J, Ruest C, Reusch B, Kugel G. Dimensional
repeatabilty from the LAVA COS 3D intra-oral scanning system. J Dent R.
2009;88(A):Abstract #2951.
125. Hirayama H, Chang YC, Kugel G, Kang KH, Finkelman M. Fit of zirconia copings
generated from a digital impression technique and conventional impression technique.
3M ESPE Web site: 3MESPE com [Internet]. Available from:
http://multimedia.3m.com/mws/mediawebserver?mwsId=SSSSSufSevTsZxtUO8_xnYtB
evUqevTSevTSevTSeSSSSSS--.
126. Chen Y, Liang CP, Liu Y, Fischer AH, Parwani AV, Pantanowitz L. Review of
advanced imaging techniques. J Pathol Inform [Internet]. 2012 2012 May 28;3(22).
Available from: http://dx.crossref.org/10.4103%2F2153-3539.96751.
142
127. Fujimoto JG. Optical coherence tomography for ultrahigh resolutionin vivoimaging.
Nature Biotechnology [Internet]. 2003 31 October 2003;21. Available from:
10.1038/nbt892.
128. Swanson EA, Huang D, Hee MR, Fujimoto JG, Lin CP, Puliafito CA. High-speed
optical coherence domain reflectometry. Opt Lett. 1992 Jan 15;17(2):151-3.
129. Quadling H, Quadling M, Blair A, inventors; Laser digitizer system for dental
applications. US patent 2010/0060900 A1. 2010 Mar 11.
130. Kugel G, Beyarl M, Iamfon HA, Harsono M, Fox L, Plourde J, et al.
Marginal/internal crown fit evaluation of CAD/CAM versus press-laboratory all ceramic
crown. J Dent R. 2007;86(A):Abstract # 1366.