expert zone
Clinical topic
28
What is the evidence?
Thierry G Guitton, Jesse B Jupiter
90–90 versus parallel plating of
distal humeral fractures
While relatively uncommon injuries, intraarticular fractures
of the distal humerus continue to provide operative challenges
to the surgeon in order that such complications as nonunion,
malunion, decreased motion, and instability, are minimized.
One way to accomplish this is to enhance the stability of the
plate and screw fixation construct. The long established technique of orientation of two plates relatively perpendicular to
each other (90–90) has recently been challenged on both biomechanical and clinical perspectives by the concept of parallel
plate application.
This fixation strategy focuses on maximizing stability between
the distal fragments and the shaft of the humerus at the metaphyseal level. According to O’Driscoll this can be achieved by
following a set of eight technical objectives:
1. Every screw should pass through a plate.
2. Each screw should engage a fragment on the opposite side
that is also fixed to a plate.
3. As many screws as possible should be placed in the distal
fragments.
4. Each screw should be as long as possible.
5. Each screw should engage as many articular fragments as
possible.
6. The screws should lock together by interdigitation within the
distal fragment, thereby creating a fixed-angle architecture
that provides stability to the entire distal humerus.
2 | 09
7. Plates should be applied such that compression is achieved
at the supracondylar level for both columns.
8. Plates used must be strong enough and stiff enough to resist
breaking or bending before union occurs at the supracondylar level (Fig 1a–h).
This review will investigate the evidence for both plating techniques for the treatment for complex distal articular humeral
fractures.
Materials and methods
The studies considered for possible inclusion in the current review were identified in a search (MeSH), in MEDLINE (National
Library of Medicine, Bethesda, MD), EMBASE (Elsevier, Amsterdam, the Netherlands) and the Cochrane review for randomized
controlled trials (Wiley InterScience, Hoboken, NJ) for the word
distal humerus fractures and the key words plating, perpendicular or parallel. The bibliographic citations for each of the
articles ultimately selected were also examined to identify any
other acceptable studies that were not captured by the database
searches. Furthermore, a grey literature search was conducted
in an effort to identify all available literature that may not have
been identified by the database searches. Selection of core articles
was restricted to original research in the English language with
human subject that examined the different plating orientations of
distal humeral fractures. Randomized controlled and retrospective studies were included while animal studies, review articles,
commentary, editorial, or letters were excluded.
expert zone
29
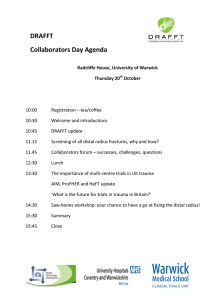
Fig 1a–h The technique an important facts developed by the Mayo
Clicinc “school” (O’Ddriscoll). (a) Every screw in the distal fragment
should pass through a plate. (b) Every screw in the distal fragment
should be anchored in a fragment on the opposite side that is fixed by
a plate. (c) As many screws as possible should be placed in the distal
fragment. (d) Every screw in the distal fragment should be as long as
possible. (e) Every screw in the distal fragment should engage as many
articular fragment as possible. (f) The screws in the distal fragments
should lock together by interdigitation, creating a fixed angle structure,
thereby completing the arch or closing the loop. (g) The plate should
be applied with compression at the supracondylar level. (h) The plate
should be strong and stiff enough to resist bending or breakage.
1a
1b
1c
1d
1e
1g
1f
1h
Results
Clinical evidence: While there are numerous reports on internal
fixation of distal humeral fractures, they are for the most part
retrospective studies using a single plating technique. Unfortunately no prospective studies specifically comparing both
methods, exist up to the present time.
While the placement of plates nearly perpendicular to each other
was promoted early on by the AO group the biomechanical study
of Helfet and Hotchkiss added credibility to this technique (Fig
2a–e and 3). A number of subsequent clinical studies revealed
nearly 75–85% good to excellent results with 90–90 plating. A
long term follow-up study at a mean of 19 years after injury by
Doornberg concluded that the long term results of open reduction and internal fixation of 19 Type C fractures of the distal
part of the humerus treated with perpendicular orientation are
similar to those reported in the short term. They suggested that
the results are durable over time.
The clinical experience with parallel plating has not been as
extensive or with longer follow up, however current reports
reveal no evidence of failure of the fixation and comparable
clinical results as with 90-90 plating.
Biomechanical evidence: Which technique is more stable?
Several biomechanical studies compared parallel plating with
perpendicular 90–90 orientation, concluding that parallel plating with additional use of bolts was favorable to perpendicular
plating. Their observations were supported by Arnander who
concluded that, parallel plating was superior to the perpendicu2 | 09
expert zone
Clinical topic
30
2a
2b
lar orientation although they expressed concern that placing a
plate lateral can be technically difficult.
Jacobson concluded that perpendicular plate orientation was
strongest in the sagittal plane while Korner stated that perpendicular plating had increased stiffness to torsional and anteroposterior bending forces. Schwartz found similar stabilization
among both plate orientations.
How do the results of stability testing relate to physiologic loading? Wong tested both fixation methods and concluded that
both methods may be above the threshold necessary for early
motion and predictable fracture healing, rendering the marginal
strength of parallel plating clinically unimportant. Kimball
found that the risk of delayed union or nonunion increased
by the extensive subperiosteal elevation with parallel plating
orientation. Schutzer tested the perpendicular plate orientation
with different plate types and concluded that implant choice was
not critical in good bone quality. Korner showed that locking
plates have a substantial advantage in poor bone quality or if
significant metaphysical comminution is present. Otherwise
they concluded that there was no difference in plate type and
that plate position is critical.
Discussion
2c
2d
Although some biomechanical evidence may favor parallel
orientation, the real take home message may be that both orientations are strong enough to be able to mobilize the elbow
after fracture fixation. Additionally it should be noted that
biomechanical evidence raises as many questions as solutions.
Some biomechanical studies fail to actually resemble the true
clinical setting, and often have low samples sizes and a lack of
statistical power.
From a clinical perspective, there are not sufficient data to
make valid comparisons. Several different outcome measures
are used; fractures types vary and non-homogenous patient
selections have been reported.
Long term follow-up for parallel plating and clinical trials are
needed to compare different plate orientation. Until then both
fractures orientations seem adequate enough to treat complex
distal articular humeral fractures and the choice should be made
by fracture specifications and surgeon’s preference.
2e
3
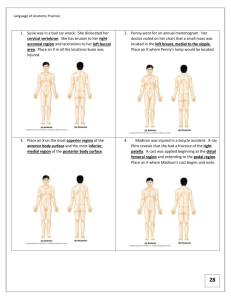
Figure 2a–e The AO technique: Reconstructing a multifragmentary
distal humeral fracture.
Figure 3 Fixation with two anatomically precontoured perpendicular
plates.
2 | 09
expert zone
31
Suggested reading
Ackerman G, Jupiter JB (1988) Non-union of fractures of the distal
end of the humerus. J Bone Joint Surg Am; 70(1):75–83.
Caja VL, Moroni A, Vendemia V, et al (1994) Surgical treatment of
bicondylar fractures of the distal humerus. Injury; 25(7):433–438.
Thierry G Guitton
Harvard Medical School,
Orthopedic Hand and
Upper Extremity Service
Boston, United States
tguitton@partners.org
Henley MB, Bone LB, Parker B (1987) Operative management of intraarticular fractures of the distal humerus. J Orthop Trauma; (1):24–35.
Jupiter JB, Neff U, Holzach P, et al (1985) Intercondylar fractures of
the humerus. An operative approach. J Bone Joint Surg Am; 67(2):226–239.
Ring D, Jupiter JB (2000) Fractures of the distal humerus. Orthop Clin
North Am; 31(1):103–113.
Helfet DL, Hotchkiss RN (1990) Internal fixation of the distal
humerus: a biomechanical comparison of methods. J Orthop Trauma;
4(3):260–264.
Jesse B Jupiter
Harvard Medical School,
Orthopedic Hand and
Upper Extremity Service
Boston, United States
jjupiter1@partners.org
Self J, Viegas SF, Buford WL Jr, et al (1995) A comparison of doubleplate fixation methods for complex distal humerus fractures.
J Shoulder Elbow Surg; 4(1 Pt 1):10–16.
O’Driscoll SW (2005) Optimizing stability in distal humeral fracture
fixation. J Shoulder Elbow Surg; 4(1 Suppl S):186S–194S.
Sanchez-Sotelo J, Torchia ME, O’Driscoll SW (2007) Complex distal
humeral fractures: internal fixation with a principle-based parallel-plate
technique. J Bone Joint Surg Am; 89(5):961–969.
Sanchez-Sotelo J, Torchia ME, O’Driscoll SW (2008) Complex distal
humeral fractures: internal fixation with a principle-based parallel-plate
technique. Surgical technique. J Bone Joint Surg Am;
90 Suppl 2 Pt 1:31–46.
Doornberg JN, van Duijn PJ, Linzel D, et al (2007) Surgical
treatment of intra-articular fractures of the distal part of the humerus.
Functional outcome after twelve to thirty years. (2007)
J Bone Joint Surg Am; 89(7):1524–1532.
McKee MD, Wilson TL, Winston L, et al (2000) Functional outcome
following surgical treatment of intra-articular distal humeral fractures
through a posterior approach. J Bone Joint Surg Am; 82-A(12):1701–1707.
Wong AS, Baratz ME (2009) Elbow fractures: distal humerus.
J Hand Surg [Am]; 34(1):176–190.
Arnander MW, Reeves A, MacLeod IA, et al (2008) A biomechanical
comparison of plate configuration in distal humerus fractures. J Orthop
Trauma; 22(5):332–336.
Jacobson SR, Glisson RR, Urbaniak JR (1997) Comparison of distal
humerus fracture fixation: a biomechanical study. J South Orthop Assoc;
6(4):241–249.
Korner J, Diederichs G, Arzdorf M, et al (2004) A biomechanical
evaluation of methods of distal humerus fracture fixation using locking
compression plates versus conventional reconstruction plates. J Orthop
Trauma; 18(5):286–293.
Schwartz A, Oka R, Odell T, et al (2006) Biomechanical comparison
of two different periarticular plating systems for stabilization of complex
distal humerus fractures. Clin Biomech (Bristol, Avon); 21(9):950–955.
Kimball JP, Glowczewskie F, Wright TW (2007) Intraosseous blood
supply to the distal humerus. J Hand Surg [Am]; 32(5):642–646.
Schuster I, Korner J, Arzdorf M, et al (2008) Mechanical comparison
in cadaver specimens of three different 90-degree double-plate
osteosyntheses for simulated C2-type distal humerus fractures with
varying bone densities. J Orthop Trauma; 22(2):113–120.
Korner J, Lill H, Muller LP, et al (2003) The LCP-concept in
the operative treatment of distal humerus fractures—biological,
biomechanical and surgical aspects. Injury; 34 Suppl 2:B20–30.
2 | 09
 0
0