• For all subjects, the average maximum SCR amplitude increased
advertisement

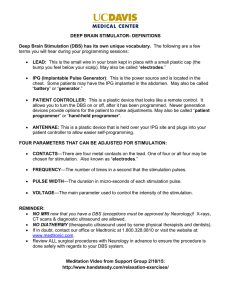
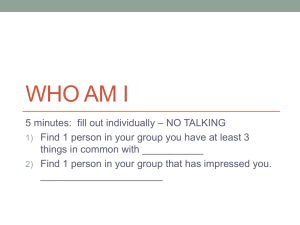
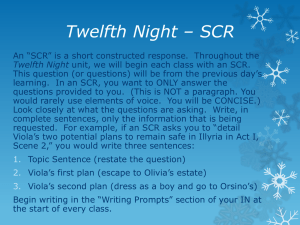
Subcallosal cingulate DBS produces current-dependent changes in autonomic arousal Skin Conductance Results Abstract Subcallosal cingulate (SCC) deep brain stimulation (DBS) has shown preliminary long-term efficacy and safety for treatmentresistant depression (TRD). Immediate changes in mood and behavior with intra-operative testing have also been observed. These immediate behavioral effects have successfully guided selection of the optimal electrode contact, and these effects are often predictive of long-term outcome. Spontaneous self-reported intra operative effects include: “feeling lighter, calmer”, “more connected, “feeling warm, flushed”, “more interested”, “tingling”, “feeling aroused”, “more awake, more aware, more reactive”; many suggestive of acute autonomic sensations in addition to changes in mood and attention. These subjective responses are accompanied by concurrent changes in sympathetic arousal as indexed by skin conductance responses (SCR) during blinded intraoperative testing. These SCR changes are observed within seconds of initiating acute stimulation and prior to verbalization of subjective feelings and appear to correlate with the optimal anatomical target for long-term stimulation. To test the potential utility of SCR to further define optimal stimulation parameters, SCR was measured during an acute stimulation protocol performed after 3 months of chronic DBS. Methods Three participants in an ongoing research study of SCC DBS for TRD were tested. At the time of the experiment the patients were receiving bilateral stimulation at a single, monopolar contact in each hemisphere with stimulation parameters held constant over 3 months (frequency =130 Hz, pulse width = 91 μsec, current=8 mA). Time-locked changes in SCR were recorded while simultaneously varying the current amplitude on the chronically stimulated DBS contacts. SCR was recorded from the medial phalanges of the index and middle fingers on the non-dominant hand. Participants were instructed to remain quiet for the duration of the experiment and were blinded to the parameter modifications. Stimulation parameters other than current amplitude (e.g., frequency and pulse width) were held constant. After recording baseline SCR (stimulation ON, chronic parameters), the current was discontinued. Current amplitudes were then varied using a stepwise design, alternating 2 minutes OFF and 2 minutes ON, with steps at 2, 4, 6, 8 mA and then descending in reverse order. Sham stimulation was performed at the beginning and end of the protocol. Three measures were derived for each of the two-minute stimulation periods: (1) the average maximum SCR amplitude, (2) the proportion total number of SCRs, and (3) the proportion cumulative SCR magnitude. SCRs were defined as any phasic deviation in the skin conductance level that exceeded 0.1 micro Siemens (μS). The two repetitions of the same dose of stimulation were averaged for analysis. The average maximum SCR amplitude measure was defined as the maximal change in SCR over the two minute stimulation period. The proportion total number of SCRs is indicative of SC reactivity to stimulation. The proportion cumulative SCR magnitude is a combined measure of the total number of SCRs and the magnitude of each of these non-specific SCRs. Thus, this measure is indicative of SC reactivity and SCR size during stimulation. Proportions were computed by dividing the derived value for a particular dose of stimulation current by the total derived value across all stimulation periods to adjust for the overall reactivity of each participant. Results For the three subjects, the average maximum SCR amplitude increased as a function of increases in stimulation current across the stimulation period. 8 mA, the current used in these participants for chronic stimulation, generated the most robust acute SCR effects. The proportion total number of SCRs also increased with increasing current. Finally, the proportion cumulative SCR magnitude showed a similar dose-dependent effect to the other SC measures with a larger cumulative SCR magnitude for 8 mA of stimulation than for any other current dose. SCR count and SCR magnitude for all of the stimulation conditions (2, 4, 6, 8 mA) were larger than the corresponding SCR measures for the sham condition for both participants. Conclusion SCC DBS elicits a current-dependent increase in sympathetic arousal in patients with TRD. This effect is seen with initial stimulation in the operating room, maintained with chronic DBS delivered over 3 months and reproduced following short-term discontinuation and repeat acute testing, with maximal effects seen at clinically relevant parameters. At present, DBS contact selection is based purely on SCC anatomy and trial and error testing of individual contacts. These findings suggest that SCC DBS modulates brain regions involved in autonomic regulation consistent with known anatomical connectivity of SCC to brainstem in humans and animals. As such, these physiological findings may both help to optimize contact selection as well as identify thresholds for stimulation parameters for chronic stimulation. Further, current-dependent changes in sympathetic arousal with SCC DBS provide a novel strategy for examining the interactions of affective experience and the autonomic nervous system in TRD. A B Figs. 1 A & B: Sagittal (A) and Coronal (B) views of the Subcallosal Cingulate Area with implanted DBS leads in situ for a characteristic depression case (post-op high resolution CT superimposed on preop 3T MRI) Figure 3. A B C • Skin Background conductance activity is a sensitive index of autonomic arousal, resulting from sympathetic innervation of the skin, and measured by alterations in the conductance of an applied current. • Intraoperative Subcallosal Cingulate Deep Brain Stimulation (SCC DBS) produces spontaneous reports of symptoms that suggest autonomic activation • Autonomic arousal, measured by Skin Conductance Activity, is seen seconds after stimulation is initiated and prior to the subject’s spontaneous report of an effect • Measurements of skin conductance responses (SCR) were conducted three months after chronic SCC DBS to further define optimal stimulation parameters Methods • Three subjects (2 females, 1 male; mean age 50.6 years old) enrolled in an ongoing research study of SCC DBS for treatment-resistant depression were tested. All patients had Major Depressive Disorder. Mean 17-item HAMD at inclusion was 22.3 points. Mean HAMD score at time of testing was 14.3 points. • Subjects had received chronic bilateral DBS with constant stimulation parameters for three months (single, monopolar contact in each hemisphere, frequency= 130 Hz, pulse width = 91 μsec, current=8 mA) (Figures 1 A & B). • Time-locked changes in SCR were recorded while simultaneously varying the current amplitude on the chronically stimulated DBS contacts. SCR was recorded from the medial phalanges of the index and middle fingers on the non-dominant hand. • Baseline SCR was recorded (stimulation ON, chronic parameters). Current amplitudes were then varied using a stepwise design, alternating 2 minutes OFF and 2 minutes ON, with steps at 2, 4, 6, 8 mA and then descending in reverse order. Sham stimulation was performed at the beginning and end of the protocol (Figure 2). • Three measures were derived for each of the two-minute stimulation periods: (1) the average maximum SCR amplitude, (2) the proportion total number of SCRs, and (3) the proportion cumulative SCR magnitude. • The two repetitions of the same dose of stimulation were averaged for analysis. The average maximum SCR amplitude measure was defined as the maximal change in SCR over the two minute stimulation period. SCRs were defined as any phasic deviation in the skin conductance level that exceeded 0.1 micro Siemens (μS). The proportion total number of SCRs is indicative of SC reactivity to stimulation. The proportion cumulative SCR magnitude is a combined measure of the total number of SCRs and the magnitude of each of these non-specific SCRs. Thus, this measure is indicative of SC reactivity and SCR size during stimulation. Proportions were computed by dividing the derived value for a particular dose of stimulation current by the total derived value across all stimulation periods to adjust for the overall reactivity of each participant. Fig 2: Stepwise experiment with AB BA design. Blue line shows SCR. Red line shows heart rate (BPM). Green line is facial surface EMG, showing artifact when stimulation is ON. Results • For all subjects, the average maximum SCR amplitude increased as a function of increases in stimulation current across the stimulation period (Figure 3A). • 8 mA, the current used in these participants for chronic stimulation, generated the most robust acute SCR effects. • The proportion total number of SCRs also increased with increasing current (Figure 3B). • The proportion cumulative SCR magnitude showed a similar dosedependent effect to the other SC measures with a larger cumulative SCR magnitude for 8 mA of stimulation than for any other current dose (Fig. 3C). Grant Support: Hope for Depression Research Foundation, Dana Foundation Devices donated by St Jude Medical Inc. FDA IDE G060028 (sponsor HSM) Clinicaltrials.gov ID#: NCT00367003 Disclosure: HSM has IP licensing and consulting agreements with SJM, Inc For more information please email Patricio Riva Posse, MD privapo@emory.edu Conclusion • SCC DBS elicits a current-dependent increase in sympathetic arousal in patients with TRD. • This effect is seen upon initial stimulation in the operating room, maintained with chronic DBS delivered over 3 months and reproduced following short-term discontinuation and repeat acute testing, with maximal effects seen at clinically relevant parameters. • At present, DBS contact selection is based purely on SCC anatomy and trial and error testing of individual contacts. • These findings suggest that SCC DBS modulates brain regions involved in autonomic regulation consistent with known anatomical connectivity of SCC to brainstem in humans and animals. • As such, these physiological findings may both help to optimize contact selection as well as identify thresholds for stimulation parameters for chronic stimulation. • Current-dependent changes in sympathetic arousal with SCC DBS provide a novel strategy for examining the interactions of affective experience and the autonomic nervous system in TRD.