Contributing to better patient care
advertisement

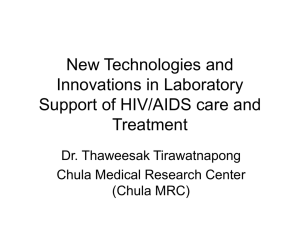
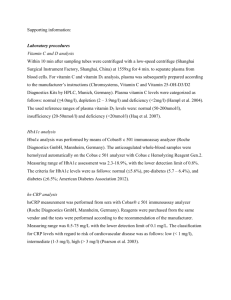
Therapeutic drug monitoring Contributing to better patient care cobas® modular platform Flexible configurations for tailor made solutions With the cobas modular platform (cobas 4000 and 6000 analyzer series and cobas 8000 modular analyzer series) Roche has developed a platform concept based on a common architecture that delivers tailor-made solutions for diverse workload and testing requirements. The cobas modular platform is designed to reduce the complexity of laboratory operation and provide efficient and compatible solutions for network cooperation. Flexible and intelligent solutions •Multiple configurations with tailor-made solutions for higher efficiency and productivity •Consolidation of clinical chemistry and immunochemistry with more than 200 parameters for cost and workflow improvements •Future sustainability through easy adaptation to changing throughput and parameter needs cobas 8000 modular analyzer series Large volume <c 502> <e 602> <c 701> cobas 6000 analyzer series Mid volume <c 501> 38 configurations <c 702> * 7 configurations <e 601> cobas 4000 analyzer series Low volume <c 311> •Consistency of interaction with hardware, software and reagents for less training and more staff flexibility •Consistency of patient results due to a universal reagent concept <e 411> * TDM assays in development 3 configurations COBAS, COBAS C, COBAS E and LIFE NEEDS ANSWERS are trademarks of Roche. ©2011 Roche Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com Therapeutic drug monitoring Precision and method comparison study in routine laboratories on the COBAS INTEGRA® 800 analyzer and cobas c 501 module G. Brandhorst1, M. Shipkova2, E. Rosler3, D. Petrova1, M. Orth2, J. Engelmayer1, E. Wieland2, M. Oellerich1 1 Department of Clinical Chemistry, Universitätsmedizin Goettingen, Germany 2 Klinikum Stuttgart, Department of Clinical Chemistry and Laboratory Medicine, Stuttgart, Germany 3 Marienhospital Stuttgart, Stuttgart, Germany Introduction Therapeutic drug monitoring (TDM) is a common laboratory routine used to measure a serum or plasma drug ­concentration for patients using drugs that are typically ­prescribed for long-term intake and which have a narrow therapeutic range. Within this range most patients will ­experience significant therapeutic effects without an undesirable degree of adverse reactions. Below the range, drugs are most likely ineffective. Above the range, there is a possible toxic side effect without any improvement in the efficacy of the drug. Consequently, precision at the relevant medical decision points – the low and high end of the therapeutic range - is a key performance measure for this range of tests. TDM has experienced a degree of technological change over the past years: historically, HPLC was used for measurement. Today, most tests are run on automated systems to improve laboratory efficiency. Key conclusion The study clearly demonstrates the consistent performance parity between the COBAS INTEGRA 800 analyzer and cobas c 501 module and the excellence of the ­intermediate precision of the cobas c 501 module. For six of the eight assays (including Carbamazepine, Phenobarbital, Phenytoin, Theophylline, Vancomycin and Valproic Acid) excellent intermediate precision results were obtained on both analytical systems. An evaluation of eight TDM tests was carried out on the cobas c 501 module and the COBAS INTEGRA® 800 analyzer. The study was carried out across three sites in Germany. Evaluator Laboratory Country Hr. Prof. M. Oellerich Hr. Dr. G. Brandhorst Fr. J. Engelmayer Fr. S. Götze Universitätsmedizin Göttingen Germany, Göttingen Fr. Dr. M. Shipkova Fr. K. Rapp Fr. S. Stier Katharinenhospital Stuttgart Germany, Stuttgart Hr. Dr. A. E. Rosler Marienhospital Stuttgart Germany, Stuttgart The CVs for both Digoxin and Tobramycin were slightly higher overall - however, the results were still comparable between the two analyzers. The method comparison yielded excellent results for 4 of 8 assays with slopes less or equal to +/- 4%. The remaining assays showed a good comparison (1.05 - 1.07). The results showed an excellent correlation (r) of 0.98 - 1.00. Study design The study objectives were 1) to analyze the precision of immunoassays based on different technologies and 2) to compare the results using routine samples on the cobas c and COBAS INTEGRA® platforms. For the study, eight routine TDM tests using different test principles have been evaluated. (Table 1). Detailed results & conclusions Overall, the comparison between the two Roche systems COBAS INTEGRA 800 analyzer and cobas c 501 module demonstrated very consistent and precise results and excellent % CV at the relevant medical decision points. For intermediate precision, the following detailed results were obtained: Carbamazepine: excellent results with CVs between 2.0 and 4.7% were obtained on both systems. Digoxin: comparable results on both analyzers. CVs up to 8% measured at low ­concentration levels. Phenobarbital: Very good results with CVs below 5.1% with one exception of 6.3%. Samples were collected at each site and shared between the sites. The measurements were done in 2 replicates, 2 runs /day, over 10 days. Intermediate precision was calculated from 40 replicates. The comparison of the methods was performed by calculation of the Passing / Bablok regression analysis. Implausible results were discussed and repeated if necessary. Phenytoin: Theophylline: Tobramycin: Vancomycin: Valproic acid: excellent results on both analyzers. excellent results on both analyzers. Slightly superior results on cobas c 501 module with CVs between 2.4 and 3.0%. in mid and high concentration, results superior on cobas c 501 module. However, at the low level a high CV was obtained on this analyzer. excellent and well comparable results on both analyzers. very good results below 6%. Slightly superior results on COBAS INTEGRA 800 analyzer. Parameter Expected range guide System Carbamazepine 8 – 12 mg/L cobas c 501 module KIMS 0.35 – 20 mg/L COBAS INTEGRA® 800 analyzer FPIA 0.12 – 20 mg/L cobas c 501 module KIMS 0.3 – 5.0 μg/L COBAS INTEGRA 800 analyzer KIMS 0.3 – 5.0 μg/L cobas c 501 module KIMS 2.4 – 60 mg/L COBAS INTEGRA 800 analyzer FPIA 1.0 – 60 mg/L cobas c 501 module KIMS 0.8 – 40 mg/L COBAS INTEGRA 800 analyzer FPIA 0.61 – 40 mg/L cobas c 501 module KIMS 0.8 – 40 mg/L Digoxin 0.6 – 1.2 μg/L Phenobarbital 10 – 30 mg/L Phenytoin 10 – 20 mg/L Test principle Measuring range package insert Theophylline 10 – 20 mg/L COBAS INTEGRA 800 analyzer FPIA 0.18 – 40 mg/L Tobramycin 6 – 10 mg/L and 0.5 – 2.0 mg/L cobas c 501 module EMIT 0.33 – 10 mg/L COBAS INTEGRA 800 analyzer FPIA 0.04 – 10 mg/L 25 – 40 mg/L and 5 – 10 mg/L cobas c 501 module EMIT 1.7 – 80 mg/L COBAS INTEGRA 800 analyzer FPIA 1.3 – 80 mg/L 50 – 100 mg/L cobas c 501 module EMIT 2.8 – 150 mg/L COBAS INTEGRA 800 analyzer FPIA 3.15 – 150 mg/L Vancomycin Valproic Acid Table 1: Overview about parameters and test principles Intermediate precision For six of the eight assays excellent intermediate precision results were obtained on both analytical systems. The CVs for both Digoxin and Tobramycin were slightly higher overall - however, the results were still comparable between the two analyzers. 12.0 12.0 10.0 10.012.0 CV [%] 6.0 8.0 10.0 6.0 8.0 4.0 6.0 4.0 4.0 2.0 2.0 0 0 TDM level 1 2 3 cobas c 501 module TDM level 1 2 3 COBAS INTEGRA 800 analyzer Fig. 1: Carbamazepine CV [%] 12.0 8.0 CV [%] CV [%] 8.0 *Level 3 not measured 10.0 2.0 0 6.0 4.0 2.0 TDM level TDM level TDM level TDM level 1 2 3 1 2 3 1 2 3 1 2 3* TDM level TDM level ® ® cobas c2501 COBAS INTEGRA® 800 Abbott AxSym 1 3 1 2 Abbott 3 Architect cobas c 501 module 0 COBAS INTEGRA 800 analyzer Fig. 2: Digoxin TDM level TDM level TDM level TDM level 1 2 3 1 2 3 1 2 3 1 2 3* ® ® cobas c 501 COBAS INTEGRA 800 Abbott AxSym Abbott Architect® analyzer module 10.0 10.0 8.0 8.0 6.0 4.0 12.0 6.0 4.0 2.0 2.0 0 0 TDM level 1 2 3 Abbott AxSym® TDM level 1 2 3* Abbott ® *Level 3 not measured Architect 10.0 8.0 CV [%] CV [%] 12.0 CV [%] 12.0 6.0 4.0 2.0 TDM level 1 2 3 cobas c 501 module Fig. 3: Phenobarbital TDM level 1 2 3 COBAS INTEGRA 800 analyzer 0 TDM level TDM level TDM level TDM level TDM level TDM level 1 1 1 2 23 3 12 2 3 3 1 2 3 1 2 3* COBAS INTEGRA cobas c 501 cobas c 501 COBAS INTEGRA® 800 Abbott AxSym® 800 Abbott Architect® analyzer module Fig. 4: Phenytoin TDM level 1 2 3 Abbott AxSym® TDM level 1 2 3* Abbott Architect® 10.0 10.0 8.0 8.0 6.0 4.0 12.0 6.0 4.0 2.0 2.0 0 0 *Level 3 not measure 10.0 8.0 CV [%] CV [%] 12.0 CV [%] 12.0 6.0 4.0 2.0 TDM level 1 2 3 COBAS INTEGRA 800 analyzer Fig. 5: Theophylline Fig. 6: Tobramycin 12.0 10.0 10.0 8.0 8.0 CV [%] 12.0 CV [%] 0 TDMTDM levellevel TDM level TDM level TDM level TDM level 1 2 1 2 33 1 1 22 3 3 1 2 3 1 2 3* ® ® INTEGRA cobas c 501c 501 COBAS INTEGRA COBAS cobas 800 Abbott AxSym 800 Abbott Architect analyzer module 6.0 4.0 12.0 6.0 4.0 2.0 2.0 0 0 TDM level 1 2 3 Abbott AxSym® TDM level 1 2 3* Abbott Architect® *Level 3 no 10.0 8.0 CV [%] TDM level 1 2 3 cobas c 501 module 6.0 4.0 2.0 TDM level 1 2 3 cobas c 501 module Fig. 7: Vancomycin TDM level 1 2 3 COBAS INTEGRA 800 analyzer 0 TDM level TDM level TDM level TDM level TDM level TDM 1 2 31 2 3 2 1 23 3 1 2 3 1 1 2 ® COBAS 800 ® Abbott Ar cobas c 501 cobas c 501 COBAS INTEGRA 800INTEGRA Abbott AxSym analyzer module Fig. 8: Valproic Acid TDM level TDM level TDM level TDM level 1 2 3 1 2 3 1 2 3 1 2 3* ® ® cobas c 501 COBAS INTEGRA 800 Abbott AxSym Abbott Architect® TDM level TDM level analyzer module 1 2 3 Abbott AxSym® 1 2 3* Abbott Architect® Correlation COBAS INTEGRA 800® analyzer vs. cobas c 501 module The method comparison yielded excellent results for 4 of 8 assays with slopes less or equal to +/- 4%. The remaining assays showed a good comparison (1.05 - 1.07). The results showed an excellent correlation (r) of 0.98 - 1.00. 16.0 14.0 12.0 10.0 8.0 6.0 4.0 2.0 0.0 0.0 4.0 8.0 12.0 16.0 20.0 Carbamazepine [mg/L] COBAS INTEGRA 800 analyzer Fig. 9: Carbamazepine 2.5 2.0 1.5 5.0 1.0 P/B regression Y = 1.033 * X – 0.005 md(95) = 0.092 N = 67 r = 0.9920 t = 0.8751 4.5 4.0 3.5 3.0 2.5 20.0 2.0 1.5 18.0 1.0 16.0 0.5 Carbamacepin [mg/L] cobas c 501 module Carbamazepine [mg/L] cobas c 501 module 18.0 AAGP2 Immunoturbidimetry g/L cobas c 501 module P/B regression Y = 1.074 * X – 0.0314.0 md(95) = 1.453 3.5 N = 77 r = 0.9769 t = 0.9026 3.0 Digoxin [µg/L] cobas c 501 module 20.0 0.0 14.0 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 0.5 12.0 Digoxin 0 [µg/L] COBAS INTEGRA 800 analyzer 0 0.5 1.0 1.5 2.0 2.5 3.0 10.0 3.5 AAG Fig. 10: Digoxin 8.0 Immunonephelometry g/L BN II 6.0 4.0 50.0 40.0 30.0 20.0 10.0 35.0 30.0 25.0 [mg/L] COBAS INTEGRA® 70.0 20.0 15.0 60.0 10.0 5.0 0.0 0.0 P/B regression Y = 1.014 * X + 0.074 0.0 md(95) = 1.94 0.0 2.0 4.0 r = 6.00.9868 8.0 10.0 12.0 1 N = 63 t = 0.9171 Carbamacep 2.0 40.0 Phenobarbital [mg/L] cobas c 501 module Phenobarbital [mg/L] cobas c 501 module 60.0 45.0 Phenytoin [mg/L] cobas c 501 module P/B regression Y = 0.982 * X + 0.18 md(95) = 1.609 N = 58 r = 0.9961 t = 0.9525 70.0 50.0 0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0 0.05.0 10.015.0 20.025.030.035.040.045.0 Phenobarbital [mg/L] COBAS INTEGRA 800 analyzer Phenytoin 40.0 [mg/L] COBAS INTEGRA 800 analyzer Fig. 11: Phenobarbital Fig. 12: Phenytoin 30.0 20.0 10.0 0.0 0.0 10.0 20.0 30.0 40.0 50.0 60.0 Phenobarbital [mg/L] COBAS INTEGRA® 800 analyzer 7 25.0 20.0 15.0 10.0 5.0 0.0 35.0 9.0 8.0 7.0 6.0 5.0 4.0 3.0 2.0 1.0 0.0 0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.0 P/B regression Y = 1.069 * X – 0.041 md(95) = 0.473 N = 47 r = 0.9911 t = 0.9541 30.0 25.0 20.0 15.0 10.0 5.0 0.0 0.06.0 5.07.010.0 15.010.0 20.0 25.0 30.0 35.0 0.0 1.0 2.0 3.0 4.0 5.0 8.0 9.0 Tobramycin Theophylline [mg/L] COBAS INTEGRA analyzer [mg/L] 800 COBAS INTEGRA® 800 analyzer Theophylline [mg/L] COBAS INTEGRA 800 analyzer Fig. 13: Theophylline 35. 30. Theophylline [mg/L] cobas c 501 module 30.0 10.0 Theophylline [mg/L] cobas c 501 module P/B regression Y = 1.049 * X – 0.008 md(95) = 0.779 N = 79 r = 0.9966 t = 0.9518 Tobramycin [mg/L] cobas c 501 module Theophylline [mg/L] cobas c 501 module 35.0 25. 20. 15. 10. Fig. 14: Tobramycin 5. 0. 50.0 40.0 30.0 20.0 10.0 0.0 0.0 10.0 20.0 30.0 40.0 50.0 60.0 Vancomycin [mg/L] COBAS INTEGRA 800 analyzer Fig. 15: Vancomycin 120.0 P/B regression Y = 1.018 * X – 2.47 md(95) = 3.322 N = 80 r = 0.9911 t = 0.9259 100.0 80.0 60.0 60.0 50.0 40.0 20.0 0.0 Vancomycin [mg/L] cobas c 501 module P/B regression Y = 1.05 * X + 0.226 md(95) = 1.34 N = 81 r = 0.9952 t = 0.9511 Valproic Acid [mg/L] cobas c 501 module Vancomycin [mg/L] cobas c 501 module 60.0 40.0 0.0 20.0 40.0 60.0 80.0 100.0 120.0 30.0 Valproic Acid [mg/L] COBAS INTEGRA 800 analyzer Fig. 16: Valproic Acid 20.0 10.0 0.0 0.0 10.0 20.0 30.0 40.0 50.0 Vancomycin [mg/L] COBAS INTEGRA® 800 analyzer Acknowledgement A special thank you to all investigators - especially I. Domke and A. Fahle - at the various locations for performing the study. Thanks also to the Roche colleagues for their dedicated support. COBAS, COBAS C, COBAS INTEGRA and LIFE NEEDS ANSWERS are trademarks of Roche. All other trademarks are property of their respective owners. ©2011 Roche Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com Carbamazepine ONLINE TDM Carbamazepine, CARB2 Kinetic interaction of microparticles in solution (KIMS) immunoassay for the quantitative in vitro determination of carbamazepine in serum and plasma on cobas c systems* Indication Carbamazepine is an anticonvulsant drug used for the treatment of trigeminal neuralgia,1 all forms of partial epilepsy, generalized tonic-clonic (grand mal) seizures, as well as simple and complex partial seizures.2,3,4 Some dosage forms, e.g. Equetrol, have been approved for treating bipolar mood disorder.5 The specific mechanism of carbamazepine is proposed as a depressant action on the transmission through the nucleus ventralis anterior of the thalamus.2,3 In combination with other clinical information, monitoring carbamazepine levels provides physicians with an effective tool to aid in adjusting dosage and achieving optimal therapeutic effect while avoiding both sub-therapeutic and toxic drug levels. Test principle: Kinetic interaction of microparticles in solution (KIMS) Negative Bi-drug hapten conjugated micro-particles + Anti-carbamazepine antibody Liquid, R1 ready-to-use, two-reagent formulation eliminates the need for mixing R2 Biotinylated drug Anticarbamazepine antibody + Streptavidine coated latex beads Aggregation Aggregation indicates absence of target drug in sample •Biotinylated drug hapten serves as binding partner to •anti-carbamazepine antibody •Streptavidin coated latex beads •A competitive reaction to a limited amount of specific anti-carbamazepine antibody takes place between the hapten and free carbamazepine in the sample •A decrease in apparent signal is ­proportionate to the amount of drug present in the sample Positive Bi-drug hapten conjugated micro-particles + Anti-carbamazepine antibody + Drug in sample No aggregation Lack of aggregation indicates presence of target drug in sample Negative Antibody conjugated Micro-particles + Drug-conjugate * all cobas c systems except cobas c 111 analyzer Carbamazepine test characteristics Reaction time 10 min Test principle Kinetic interaction of microparticles in solution (KIMS) Calibration 6-point after reagent lot change, and as required following quality control procedures Traceability Standardized against USP reference standards Sample material Serum, Plasma (sodium or lithium heparin plasma and K2-EDTA plasma) Sample volume 2 μL Measuring range 0.35 – 20 μg/mL (1.5 – 85 μmol/L) Carbamazepine expected values guide Troupin et al. 6 – when used as sole agent Shorvon et al. 7 8 – 12 μg/mL (33.8 – 50.8 μmol/L) 4 – 8 μg/mL (16.9 – 33.8 μmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean μg/mL 2.7 8.2 13.9 μmol/L 11.4 34.7 58.8 CV% 3.5 2.1 1.3 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean μg/mL 2.7 8.2 13.9 μmol/L 11.4 34.7 58.8 CV% 3.4 2.5 2.5 Interferences Patients with renal insufficiency, such as those on hemodialysis, may exhibit carbamazepine levels in serum or plasma that are not consistent with clinical expectations for patients with normal renal function. If results are greater than the expected range, determine if the patient has renal insufficiency. Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity Order information Online TDM Carbamazepine 100 tests 04490819 190 Preciset TDM I Calibrators CAL A-F Diluent 03375790 190 6 x 5 mL 1 x 10 mL Codes 691-696 TDM Control Set Level I Level II Level III 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 References 1 Blom, S. (1962). Trigeminal neuralgia: its treatment with a new anticonvulsant drug (G-32883). Lancet: 839-840. 2 Eadie, M.J., Tyler, J.H. (1974). Anticonvulsant Therapy: Pharmacological Basis and Practice. COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. Edinburgh, Great Britain. Churchill Livingstone. Chap. 7. 3 Penry, J.K., Newmark, M.E. (1979). The use of antiepileptic drugs. Ann Int Med. 90: 207-218. 4 Scheuer, M.L., Pedley, T.A. (1990). The evaluation and treatment of seizures. N Engl J Med; ©2011 Roche 322(21): 1468- 1474 5 bipolar disorder Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com 6 Troupin, A., Ojemann, L.M., Halpem, L., et al. (1977). Carbamazepine- a double blind comparison with phenytoin. Neurology; 27: 511-519. 7 Shorvon, S.D., Chadwick, D., Galbraith, A.W., et al. (1978). One drug for epilepsy. Br Med J. 1: 474–476. Digoxin ONLINE TDM Digoxin, DIG Kinetic interaction of microparticles in solution (KIMS) immunoassay for the quantitative in vitro determination of digoxin in serum and plasma ­ on cobas c systems* Indication Digoxin is a digitalis glycoside which is widely used in the treatment of various heart conditions. Digoxin exerts a positive inotropic effect which increases the contractile response of the myocardial fibers in patients experiencing congestive heart failure.1 Cardiac glycosides can also produce several electrophysiological effects that produce negative chronotropic effects on the human heart.2 These effects tend to slow down and regulate a rapid, irregular beat found in patients experiencing cardiac arrhythmias.3 Due to its extremely narrow therapeutic range, monitoring digoxin concentration provides physicians with an effective tool to aid in achieving optimal therapeutic effect while avoiding both sub-therapeutic and toxic drug levels. Test principle: Kinetic interaction of microparticles in solution (KIMS) Negative Bi-drug hapten conjugated micro-particles + Anti-carbamazepine antibody Liquid, R1 ready-to-use, two-reagent formulation eliminates the need for mixing R2 Aggregation Aggregation indicates absence of target drug in sample Positive Bi-drug hapten conjugated micro-particles + Anti-carbamazepine antibody + Drug in sample No aggregation Lack of aggregation indicates presence of target drug in sample Negative Antibody conjugated Micro-particles + Drug-conjugate •Liquid, ready-to-use, two-reagent formulation •anti-digoxin monoclonal antibody •Conjugated digoxin derivative microparticles •A competitive reaction to a limited amount of specific anti-digoxin antibody takes place •Aggregation indicates absence of target drug in sample •Lack of aggregation indicates presence of drug in sample •By monitoring the change in scattered light or absorbance, a concentration dependant curve is obtained * all cobas c systems except cobas c 111 analyzer Digoxin test characteristics Reaction time 10 min Test principle Kinetic interaction of microparticles in solution (KIMS) Calibration 6-point after reagent lot change, and as required following quality control procedures Traceability Standardized against USP reference standards Sample material Serum, Plasma (Li heparin plasma and K2-EDTA plasma) Sample volume 5.5 μL Measuring range 0.3 – 5.0 ng/mL (0.38 – 6.4 nmol/L) Digoxin Expected Values Guide Therapeutic effects 4 ESC Guidelines for diagnosis and treatment of acute and chronic heart failure 5 0.8 – 2 ng/mL (1.0 – 2.6 nmol/L) 0.6 – 1.2 ng/mL (0.77 – 1.5 nmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean ng/mL 0.87 1.8 3.0 nmol/L 1.1 2.3 3.8 CV% 4.0 1.6 1.0 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean ng/mL 0.87 1.8 3.0 nmol/L 1.1 2.3 3.8 CV% 6.0 2.4 1.6 Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity Order information Online TDM Digoxin Preciset TDM I Calibrators CAL A-F Diluent TDM Control Set Level I Level II Level III 250 tests 20737836 322 03375790 190 6 x 5 mL 1 x 10 mL Codes 691-696 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 References 1 Lee, K.S., Klaus, W. (1971). The subcellular basis for the mechanism of inotropic action of cardiac glycosides. Pharmacol Rev. 23: 193-261. 2 Hoffman, B.F. (1969). In: Fisch, C., Surawicz, B., eds. Effects of digitalis on electrical activity of cardiac fibers. Digitalis. New York, NY: Grune and Stratton: 93-109. 3 Moe, G.K., Farah, A.E. (1970). In: Goodman, L.S., Gilman, A. eds. Digitalis and allied cardiac COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. 4 Huffman, D.H., Crow, J.W., Pentikaimen, P., Azarnoff, D.L. (1976). Clinical cardiac status, labo- ©2011 Roche 5 Dickstein, K., Cohen-Solal, A., Filippatos, G., McMurray, J.J., Ponikowski, P., Poole-Wilson, glycosides. The Pharmacologist Basis of Therapeutics. New York, NY. MacMillan Company. ratory parameters and digoxin usage. Am Heart J. 91: 28. P.A., et al. (2008). ESC Guidelines for the diagnosis and treatment of acute and chronic heart Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com failure 2008:the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. 29: 2388-442. Phenobarbital ONLINE TDM Phenobarbital, PHNO2 Kinetic interaction of microparticles in solution (KIMS) immunoassay for the quantitative in vitro determination of phenobarbital in serum and plasma on cobas c systems* Indication Phenobarbital is one of the most commonly used drugs for the treatment of grand mal, psychomotor epilepsy and other forms of focal epilepsy. Monitoring the serum level of the drug is essential in order to achieve maximum seizure control while maintaining minimal blood levels to avoid negative side effects.1,2 As with other anti-convulsant drugs, it is imperative that each patient’s dosage be individualized.3 Test principle: Kinetic interaction of microparticles in solution (KIMS) Negative Antibody conjugated micro-particles + Drug-conjugate Liquid, R1 ready-to-use, two-reagent formulation eliminates the need for mixing R2 Aggregation Aggregation indicates absence of target drug in sample Positive Antibody conjugated micro-particles + Drug-conjugate + Drug in sample •Phenobarbital antibody is covalently coupled to microparticles and the drug derivative is linked to a macromolecule •The kinetic interaction of the microparticles in solutions is induced by binding of drug conjugate to the antibody on the microparticles and is inhibited by the presence of phenobarbital in the sample •A competitive reaction to a limited amount of specific anti-phenobarbital antibody takes place between the drug conjugate and free phenobarbital in the sample •A decrease in apparent signal is ­proportionate to the amount of drug present in the sample * all cobas c systems except cobas c 111 analyzer No aggregation Lack of aggregation indicates presence of target drug in sample Phenobarbital test characteristics Reaction time 10 min Test principle Kinetic interaction of microparticles in solution (KIMS) Calibration 6-point after reagent lot change, and as required following quality control procedures Traceability Standardized against USP reference standards Sample material Serum, Plasma (K2 or K3-EDTA , lithium or sodium heparin) Sample volume 2 μL Measuring range 2.4 – 60 μg/mL (10.3 – 258.6 μmol/L) Phenobarbital expected values guide 10 – 30 μg/mL (43.1 – 129 μmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean μg/mL 9.8 24.4 45.1 μmol/L 42.2 105.2 194.4 CV% 5.0 2.4 1.8 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean μg/mL 9.8 24.4 45.1 μmol/L 42.2 105.2 194.4 CV% 5.4 2.4 2.0 Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. Order information Online TDM Phenobarbital 100 tests 200 tests 04490924 190 05027446 190 Preciset TDM I Calibrators CAL A-F Diluent 6 x 5 mL 1 x 10 mL 03375790 190 Codes 691-696 TDM Control Set Level I Level II Level III 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 References 1 Johannessen, S.I. (1981). Anti-epileptic drugs: pharmacokinetic and clinical aspects. Ther ©2011 Roche Drug Monit. 3(1): 17. 2 Koch-Weser, J. (1981). Serum drug concentrations in clinical perspective. Ther Drug Monit. Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com 3(1): 3-16 3 Pippenger, C.E. (1980). Effective seizure control requires drug monitoring. Battaglia, B.J., ed. Clin Chem. New Special Section. Washington, DC: American Association of Clinical Chemistry. 1s and 10s. Phenytoin ONLINE TDM Phenytoin, PHNY2 Kinetic interaction of microparticles in solution (KIMS) immunoassay for the quantitative in vitro determination of phenytoin in serum and plasma on cobas c systems* Indication Phenytoin has been used extensively for seizure control in patients suffering from grand mal epilepsy, cortical focal seizures and temporal lobe epilepsy.1 Monitoring the serum level of the drug is essential in order to achieve maximum seizure control while maintaining minimal blood levels to avoid negative side effects.1,2,3 Due to individual patient variation in absorption and metabolism, optimum levels may vary. Test principle: Kinetic interaction of microparticles in solution (KIMS) Negative Antibody conjugated micro-particles + Drug-conjugate Liquid, R1 ready-to-use, two-reagent formulation eliminates the need for mixing R2 Aggregation Aggregation indicates absence of target drug in sample Positive Antibody conjugated micro-particles + Drug-conjugate + Drug in sample •Phenytoin is covalently coupled to microparticles and the drug derivative is linked to the macromolecule •The kinetic interaction of microparticles in solutions is induced by binding of drug­ ­conjugate to the anti-body on the ­microparticles and is inhibited by the ­presence of phenytoin in the sample •A competitive reaction to a limited amount of specific anti-phenytoin antibody ­t akes place betweenthe drug conjugate and free phenytoin in the sample •A decrease in apparent signal is ­proportionate to the amount of drug present in the sample * all cobas c systems except cobas c 111 analyzer No aggregation Lack of aggregation indicates presence of target drug in sample Phenytoin test characteristics Reaction time 10 min Test principle Kinetic interaction of microparticles in solution (KIMS) Calibration 6-point after reagent lot change, and as required following quality control procedures Traceability Standardized against USP reference standards Sample material Serum, Plasma (K2 or K3-EDTA , lithium or sodium heparin) Sample volume 1.7 μL Measuring range 0.8 – 40 μg/mL (3.2 – 158.4 μmol/L) Phenobarbital expected values guide4 10 – 20 μg/mL (39.6 – 79.2 μmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean μg/mL 6.8 13.0 22.9 μmol/L 26.9 51.5 90.7 CV% 3.4 2.2 2.5 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean μg/mL 6.8 13.0 22.9 μmol/L 26.9 51.5 90.7 CV% 3.8 3.4 3.6 Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity Order information Online TDM Phenytoin Preciset TDM I Calibrators CAL A-F Diluent TDM Control Set Level I Level II Level III 100 tests 200 tests 04490932 190 05108411 190 03375790 190 6 x 5 mL 1 x 10 mL Codes 691-696 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 References COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. 1 Buchthal, F., Klennox-Buchthal, M.A. (1972). In: Antiepileptic Drugs. Woodbury DM, Penry JK, Schmidt RP, eds. New York, NY: Raven Press. 93. 209. 2 Buchthal, F, Svensmark, O. (1971). Serum concentration of diphenylhydantoin (phenytoin) and ©2011 Roche phenobarbital and their relation to therapeutic and toxic effects. Psychiatr Neurol Neurochir. 74: 117-136. Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com 3 Booker, H.E., Hosokowa, K., Burdette, R.D., Darcey, B. (1970). A clinical study of serum primidone levels. Epilepsia. 11: 395-402. 4 Booker, H. (1978). In: Pippenger CE; Perry JKC, Jutt H, eds. Anti-epileptic Drugs: Quantitative Analysis and Interpretation. New York, NY: Raven Press. 253-260. Theophylline ONLINE TDM Theophylline, THEO2, THE-2 Kinetic interaction of microparticles in solution (KIMS) immunoassay for the quantitative in vitro determination of theophylline in serum and plasma on cobas c systems* Indication Theophylline, a bronchodilator, is widely used to treat patients with asthma, apnea (temporary asphyxia) and other obstructive lung diseases. Monitoring the serum level of the drug is essential as individual patients can vary in their rate of theophylline clearance1,2 and severe toxicity has been observed without prior occurrence of minor side effects.3 Several factors can alter theophylline elimination: it is slowed in obese patients, patients with hepatic disease and those on a high carbohydrate, low protein diet. Premature infants have very low rates of theophylline elimination.4 Conversely, theophylline elimination in more rapid among patients who smoke.5 In combination with other clinical data, monitoring serum theophylline levels can provide the physician with useful information to aid in adjusting a patient’s dosage to achieve optimal therapeutic effect while avoiding drug toxicity. Test principle: Kinetic interaction of microparticles in solution (KIMS) Negative Antibody conjugated micro-particles + Drug-conjugate Liquid, R1 ready-to-use, two-reagent formulation eliminates the need for mixing R2 Aggregation Aggregation indicates absence of target drug in sample Positive Antibody conjugated micro-particles + Drug-conjugate + Drug in sample •Theophylline antibody is covalently coupled to microparticles and the drug derivative is linked to a macromolecule •The kinetic interaction of microparticles in solution is induced by binding of drug ­conjugate to the antibody on the ­microparticles and is inhibited by the ­presence of theophylline in the sample •A competitive reaction to a limited amount of specific anti-theophylline antibody takes place between the drug conjugate and free ­theophylline in the sample •A decrease in apparent signal is ­proportionate to the amount of drug present in the sample * all cobas c systems except cobas c 111 analyzer No aggregation Lack of aggregation indicates presence of target drug in sample Theophylline test characteristics Reaction time 10 min Test principle Kinetic interaction of microparticles in solution (KIMS) Calibration 6-point after cobas c pack change, after reagent lot change, and as required following quality control procedures Traceability Standardized against USP reference standards Sample material Serum, Plasma (sodium, ammonium or lithium heparin, K2 or K3-EDTA, sodium citrate) Sample volume 2.0 μL Measuring range6 0.8 – 40 μg/mL (4.4 – 222 μmol/L) Phenobarbital expected values guide4 10 – 20 μg/mL (55.5 – 111 μmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean μg/mL 4.3 14.3 34.1 μmol/L 23.9 79.4 189.3 CV% 1.7 1.3 1.2 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean μg/mL 4.3 14.3 34.1 μmol/L 23.9 79.4 189.3 CV% 2.8 1.7 1.9 Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity Order information Online TDM Theophylline Preciset TDM I Calibrators CAL A-F Diluent TDM Control Set Level I Level II Level III 100 tests 04491025 190 03375790 190 6 x 5 mL 1 x 10 mL Codes 691-696 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 References 1 Piafsky, K.M., Ogilvie, R.I. (1975). Drug therapy. Dosage of theophylline in bronchial asthma. N Engl J Med. 292: 1218-1222. 2 Leung, P., Kalisker, A., Bell, T.D. (1977). Variation in theophylline clearance rate with time in chronic COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. 3 Zwillich, C.W., Sutton, F.D., Neff, T.A., et al. (1975). Theophylline-induced seizures in adults. ©2011 Roche 4 Ogilvie, R.I. (1978). Clinical pharmacokinetics of theophylline. Clinical Pharmacokinetics. 3: 267-293. childhood asthma. J Allergy Clin Immun. 59: 440-444. Correlation with serum concentrations. Ann Intern Med. 82: 784-787. 5 Hendeles, L., Weinberger, M.M. (1981). Theophylline therapeutic use and serum concentration Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com monitoring. In: Taylor WJ, Finn AL, eds. Individualizing Drug Therapy: Practical Applications of Drug Monitoring, I. New York, NY: Gross Townsend Frank, Inc. 31-66. 6 Jackson, F.R., Garrido, R., Silverman, H.I., Salem, H. (1973). Blood levels following oral administration of theophylline preparations. Ann Allergy. 31: 413-419. Tobramycin ONLINE TDM Tobramycin, TOBR2 Kinetic interaction of microparticles in solution (EMIT) immunoassay for the quantitative in vitro determination of tobramycin in serum and plasma on cobas c systems* Indication Tobramycin is an aminoglycoside antibiotic used in the treatment of infections caused by Pseudomonas aeruginosa, Proteus species, E.coli, Klebsiella, Serratia, Citrobacter, Staphylococcus aureus, Enterobacter and other microorganisms. The half-life of tobramycin in serum or plasma correlates closely with renal function and thus is quite variable between individuals over time.1,2 Serum or plasma tobramycin concentration is also impacted by mode of administration, the volume of extracellular fluid, the duration of the treatment and physiological changes during the illness and therapy. A peak therapeutic range is suggested for antimicrobial effectiveness. However, patients with pre-existing renal damage, or those to whom tobramycin has been administered for prolonged periods, may develop hearing impairment and/or nephrotoxicity.3 Elevated or increasing trough levels are an indication of drug accumulation due to renal impairment. Therefore, the monitoring of tobramycin at peak and trough concentrations is critical in the prevention of these serious complications.4 Test principle: Homogeneous enzyme immunoassay technique (EMIT) No drug in the sample Anti-drug antibody Drug labeled enzyme: Enzyme = Glucose-6phosphate dehydrogenase + + Drug in the sample Substrate = Glucose-6phosphate Nicotinamide adenin dinucleotide + NAD The enzyme is only active if not bound to antibody. Drug sample NADH absorbs at 340 nm Reaction direction: increase + + NAD Drug labeled enzyme is bound to anti-drug-antibody Enzyme inactive + + + NAD + + NAD In a competition, the free drug competes with drug-enzyme-conjugate for the antibody More drug in the sample more antibody–binding-sites are blocked by drug • less drug-enzyme-conjugates are bound to antibody • more NADH is built •The assay is based on competition between drug in the sample and drug labeled with the enzyme glucose-6-phosphate dehydrogenase (G6PDH) for antibody binding sites •Enyzme activity decreases upon binding to the antibody, so the drug concentration in the sample can be measured in terms of enzyme activity •Active enzyme converts oxidized NAD to NADH, resulting in an absorbance change that is measured spectrophotometrically * all cobas c systems except cobas c 111 analyzer Tobramycin test characteristics Reaction time 10 min Test principle Homogeneous enzyme immunoassay technique (EMIT) Calibration 6-point after cobas c pack change, after reagent lot change, and as required following quality control procedures. Calibration on cobas c includes a recalibration every 3 days. Traceability Standardized against USP reference standards Sample material Serum, Plasma (K2 or K3-EDTA, sodium citrate, fluoride oxalate, sodium or lithium heparin) Sample volume 2.4 μL Measuring range 0.33 – 10 μg/mL (0.71 – 21.4 μmol/L) Tobramycin expected values guide4 Peak Trough 6 – 10 μg/mL (12.8-21.4 μmol/L) 0.5 – 2.0 μg/mL (1.1-4.3 μmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean μg/mL 1.6 3.6 7.7 μmol/L 3.4 7.7 16.5 CV% 4.2 2.8 2.9 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean μg/mL 1.6 3.6 7.7 μmol/L 3.4 7.7 16.5 CV% 4.5 3.1 2.8 Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity Order information Online TDM Tobramycin Preciset TDM I Calibrators CAL A-F Diluent 100 tests 04491033 190 03375790 190 6 x 5 mL 1 x 10 mL Codes 691-696 TDM Control Set Level I Level II Level III 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 Multiclean 59 mL 04708725 190 COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. References ©2011 Roche 2 Naber, K.G., Westinfelder, S.R., Madsen, P.O. (1973). Pharmacokinetics of the aminoglycoside Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com 3 Sande, M.A., Mandell, G.L. (1980). Antimicrobial Agents, the aminoglycosides. In: Gilman, A.G., 1 Cipoll, R.J., Seifert, R.D., Zaske, D.E., et al. (1980). Systematically individualizing tobramycin dosage regimens. J Clin Pharm. 20: 570-580. antibiotic tobramycin in humans. Antimicrob Agents Chemother. 3: 469-473. Goodman, L.S., Gilman, A., eds. The Pharmacological Basis of Therapeutics. New York, NY: MacMillan. 1162-1180. 4 Baselt, R.C., Cravey, R.H. (1990). Disposition of Toxic drugs and Chemicals in Man. 3rd ed. 805-807. Valproic Acid ONLINE TDM Valproic Acid, VALP2 Kinetic interaction of microparticles in solution (EMIT) immunoassay for the quantitative in vitro determination of valproic acid in serum and plasma on cobas c systems* Indication Valproic acid (VPA) is an anticonvulsant medication which is used mainly for the treatment of primary and secondary­generalized seizures, but is also effective against absence seizures.1,2 It is particularly effective in myoclonus and is the drug of choice in photosensitive epilepsy.2 Although VPA is used in conjunction with other anti-epileptic medications, more recent studies have shown benefits of converting treatment to VPA monotherapy.3 Also, a growing body of evidence suggests that VPA is useful in the treatment of affective disorders, in particular lithium-insensitive bipolar disorders.4 Valproic acid has the fewest adverse side effects of all the widely-used anti-epileptic agents. Some incidences of tremor, coma or stupor have been noted – often in ­conjunction with other co-administration of other anti-epileptic drugs. Pharmacokinetics of VPA are highly variable depending on the form of drug and route of administration, as well as individual variations in metabolism and clearance.5 Therefore, monitoring VPA concentrations during therapy is essential in order to provide the physician with an indicator for adjusting dosage. Test principle: Homogeneous enzyme immunoassay technique (EMIT) No drug in the sample Anti-drug antibody Drug labeled enzyme: Enzyme = Glucose-6phosphate dehydrogenase + + Drug in the sample Substrate = Glucose-6phosphate Nicotinamide adenin dinucleotide + NAD The enzyme is only active if not bound to antibody. Drug sample NADH absorbs at 340 nm Reaction direction: increase + + NAD Drug labeled enzyme is bound to anti-drug-antibody Enzyme inactive + + + NAD + + NAD In a competition, the free drug competes with drug-enzyme-conjugate for the antibody More drug in the sample more antibody–binding-sites are blocked by drug • less drug-enzyme-conjugates are bound to antibody • more NADH is built •The assay is based on competition between drug in the sample and drug labeled with the enzyme glucose-6-phosphate dehydrogenase (G6PDH) for antibody binding sites •Enyzme activity decreases upon binding to the antibody, so the drug concentration in the sample can be measured in terms of enzyme activity •Active enzyme converts oxidized NAD to NADH, resulting in an absorbance change that is measured spectrophotometrically * all cobas c systems except cobas c 111 analyzer Valproic Acid test characteristics Reaction time 10 min Test principle Homogeneous enzyme immunoassay technique (EMIT) Calibration 6-point after cobas c pack change, after reagent lot change, and as required following quality control procedures. Calibration on cobas c includes a recalibration every 3 days. Traceability Standardized against USP reference standards Sample material Serum, Plasma (K2 or K3-EDTA, sodium or lithium heparin) Sample volume 2.0 μL Measuring range 2.8 – 150 μg/mL (19.4 – 1040 μmol/L) Valproic Acid expected values guide 2 50 - 100 μg/mL (346.5 - 693.0 μmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean μg/mL 37.9 80.5 117.4 μmol/L 262.6 557.9 813.6 CV% 3.0 2.1 2.6 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean μg/mL 37.9 80.5 117.4 μmol/L 262.6 557.9 813.6 CV% 4.4 3.3 4.2 Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity Order information Online TDM Valproic Acid Preciset TDM I Calibrators CAL A-F Diluent TDM Control Set Level I Level II Level III 100 tests 200 tests 04491041 190 05108438 190 03375790 190 6 x 5 mL 1 x 10 mL Codes 691-696 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 References 1 Chadwick, D. (1988). Comparison of monotherapy with valproate and other antiepilepticdrugs COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. 2 Wallace, S.J. (1986). Use of ethosuximide and valproate in the treatment of epilepsy. Neurol ©2011 Roche 3 Wilder, B.J., Rangel, R.J. (1988). Review of valproate monotherapy in the treatment of gener- Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com 4 Post, R.M. (1989). Emerging perspectives on valproate in affective disorders. J Clin Psychiatry. in the treatment of seizure disorders. AM J Med. 84 (suppl 1A): 3-6 Clin. 4: 601-616. alized tonic-clonic seizures. Am J Med. 84 (suppl 1A): 7 -13. 50: 23-29. 5 Zaccara, G., Messori, A., Moroni, F. (1989). Clinical pharmacokinetics of valproic acid. Clin Pharmacokinet. 17: 327-344. Vancomycin ONLINE TDM Vancomycin, VANC2 Kinetic interaction of microparticles in solution (EMIT) immunoassay for the quantitative in vitro determination of vancomycin in serum and plasma on cobas c systems* Indication Vancomycin is a complex glycopeptide antibiotic, which has been used to treat penicillinase-producing staphylococci.1 It is the treatment of choice for antibiotic resistant Staphylococcus aureus,2,3 as well as for the treatment of gram-positive infections where allergies to penicillin or cephalosporin play a role. Vancomycin is also used in the treatment of antibiotic-induced enterocolitis associated with Clostridium difficile and streptococcal or enterococcal endocarditis, the latter in conjunction with an aminoglycoside, when penicillin or ampicillin is not an option.4 Monitoring the peak and trough serum or plasma levels is essential to optimize therapy and avoid potentially serious side effects including ototoxicity, nephrotoxicity, phlebitis and reversible neutropenia.5 Test principle: Homogeneous enzyme immunoassay technique (EMIT) No drug in the sample Anti-drug antibody Drug labeled enzyme: Enzyme = Glucose-6phosphate dehydrogenase + + Drug in the sample Substrate = Glucose-6phosphate Nicotinamide adenin dinucleotide + NAD The enzyme is only active if not bound to antibody. Drug sample NADH absorbs at 340 nm Reaction direction: increase + + NAD Drug labeled enzyme is bound to anti-drug-antibody Enzyme inactive + + + NAD + + NAD In a competition, the free drug competes with drug-enzyme-conjugate for the antibody More drug in the sample more antibody–binding-sites are blocked by drug • less drug-enzyme-conjugates are bound to antibody • more NADH is built •The assay is based on competition between drug in the sample and drug labeled with the enzyme glucose-6-phosphate dehydrogenase (G6PDH) for antibody binding sites •Enyzme activity decreases upon binding to the antibody, so the drug concentration in the sample can be measured in terms of enzyme activity •Active enzyme converts oxidized NAD to NADH, resulting in an absorbance change that is measured spectrophotometrically * all cobas c systems except cobas c 111 analyzer Vancomycin test characteristics Reaction time 10 min Test principle Homogeneous enzyme immunoassay technique (EMIT) Calibration 6-point after cobas c pack change, after reagent lot change, and as required following quality control procedures. Calibration on cobas c includes a recalibration every 3 days. Traceability Standardized against USP reference standards Sample material Serum, Plasma (K2 or K3-EDTA, sodium citrate, fluoride oxalate) Sample volume 2.0 μL Measuring range 1.7 – 80 μg/mL (1.2 – 55.2 μmol/L) Vancomycin expected values guide 4 Peak Trough 25 - 40 μg/L 5 - 10 μg/L (17.3 - 27.6 μmol/L) (3.5 - 6.9 μmol/L) Repeatability (Within-run precision) Control 1 Control 2 Control 3 Mean μg/mL 6.8 21.5 40.9 μmol/L 4.7 14.8 28.2 CV% 1.8 1.7 2.6 Intermediate precision (total precision/between-run precision/between-day precision) Control 1 Control 2 Control 3 Mean μg/mL 6.8 21.5 40.9 μmol/L 4.7 14.8 28.2 CV% 3.5 2.4 3.1 Key ONLINE TDM points •high specificity to parent drug •negligible cross-reactivity to a broad spectrum of compounds •no significant interference to 16 common drugs •no HAMA cross-reactivity Order information Online TDM Vancomycin Preciset TDM I Calibrators CAL A-F Diluent TDM Control Set Level I Level II Level III 100 tests 200 tests 04491050 190 05108420 190 03375790 190 6 x 5 mL 1 x 10 mL Codes 691-696 2 x 5 mL 2 x 5 mL 2 x 5 mL 04521536 190 Code 310 Code 311 Code 312 References COBAS, COBAS C and LIFE NEEDS ANSWERS are trademarks of Roche. 1 McCormick, M.H., Stark, W.M., Pittinger, R.C., McGuire, J.M. (1956). In:antibiotics Annual. New York, NY: Medical Encyclopedia. 606-611. 2 Crossley, K.B., Landesman, B., Zaske, D. (1979). An outbreak of infections caused by strains of ©2011 Roche Staphylococcus aureus resistant to methicillin and aminoglycosides. J Infect Dis. 139: 273-279. 3 Sorrell, T.C., Packham, S., Shanker, M., Foldes, M., Munro, R. (1982). Vancomycin therapy for Roche Diagnostics Ltd. CH-6343 Rotkreuz Switzerland www.cobas.com methicillin-resistant Staphylococcus aureus. Ann Intern Med. 97: 344-350. 4 Cook, F.V. (1978). Vancomycin revisited. Ann Intern Med. 88: 813-818. 5 Zaccara, G., Messori, A., Moroni, F. (1989). Clinical pharmacokinetics of valproic acid. Clin Pharmacokinet. 17: 327-344.