Sufotidine 600 mg bd virtually eliminates 24 hour
advertisement

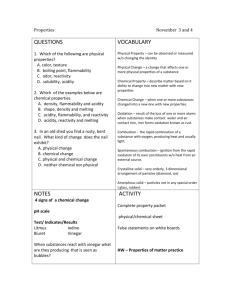
Downloaded from http://gut.bmj.com/ on September 30, 2016 - Published by group.bmj.com Gut, 1990, 31, 291-293 291 Sufotidine 600 mg bd virtually eliminates 24 hour intragastric acidity in duodenal ulcer subjects J T L Smith, R E Pounder Abstract In a double blind study, 24 hour intragastric acidity and 24 hour plasma gastrin concentrations were measured simultaneously in seven duodenal ulcer subjects on the fifth day of receiving either sufotidine 600 mg bd or placebo. Compared with placebo, during treatment with sufotidine 600 mg bd the median integrated 24 hour intragastric acidity was decreased by 95% (range 74% to 99%) from 1000 to 51 mmol/h/l, whilst the median integrated 24 hour plasma gastrin concentration increased from 416 to 927 pmol/h/l. First generation histamine H2-receptor blockers cause a short lived pulse of decreased intragastric Academic Department of Medicine, Royal Free Hospital School of Medicine, London J T L Smith R E Pounder Correspondence to: Dr R E Pounder, Royal Free Hospital School of Medicine, Pond Street, London NW3 2QG Accepted for publication 6 June 1989 acidity.'1- Meta-analysis of the results of published studies has suggested that the more profound the drug induced decrease of nocturnal intragastric acidity by a particular regimen, the greater the percentage of duodenal ulcers which are healed after four weeks of treatment with that regimen. A new meta-analysis has suggested that the four week duodenal ulcer healing rate can be predicted most accurately by a drug's ability to maintain 24 hour intragastric pH above 3 (H+ activity below 1 mmol/1),7 suggesting that control of daytime acidity may also be important. This finding is supported by the fact that the highest four week duodenal ulcer healing rates have been reported during treatment with 30 to 40 mg/day of omeprazole,5 which inhibits nocturnal and daytime acidity.9'0 Omeprazole has also had particular success in the management of difficult duodenal ulceration, the more severe grades of oesophagitis, and the Zollinger Ellison syndrome," 14 because of the profound antisecretory effect of this drug. Sufotidine is a new competitive, long acting histamine H2-blocker.'5 Earlier healthy volunteer studies, using single day dosing with sufotidine, suggested that sufotidine 600 mg bd taken before breakfast and at bed time could induce a sustained 24 hour decrease of acidity (J T L Smith and R E Pounder; H Merki; unpublished data). The objectives of the present study were to observe the effects of repeat dosing with sufotidine 600 mg bd on 24 hour intragastric acidity and plasma gastrin concentration in subjects with a history of duodenal ulceration. Methods PATI ENTS Seven male subjects with a history of endoscopically confirmed duodenal ulceration completed the study; their median age was 53 years (range 26 to 63 years), their median weight was 76 kg (68 to 99-9 kg), their median height was 178 cm (164 to 189 cm), and two of the seven subjects smoked cigarettes (10 to 20 cigarettes per day). Two other subjects withdrew from the study, but both had been dosed only with placebo. The subjects were in symptomatic remission, and not taking antisecretory therapy. The study was double blind, and dosing was given in a predetermined random order. The subjects were studied twice, on the fifth day of dosing with either sufotidine 600 mg bd or placebo. There was a nine day washout period between the studies, when the subjects received no treatment. Dosing was in the form of six identical tablets taken twice a day - at 0935 and 1935 hours. Compliance with the dosing regimen before the study day was encouraged by the use of a long range paging system (British Telecom); each subject was paged at the recommended time of every dose to remind him to take the tablets. The study was approved by the Ethics Committee of the Royal Free Hospital and written consent was obtained from each patient. Routine safety studies were performed before and after treatment with both drugs. The subjects were studied using the Royal Free Hospital standard protocol for 24 hour studies.'6 They were admitted for each study to a research ward after an overnight fast. A 10 French gauge salem sump nasogastric tube (Argyle Medical) was positioned in the stomach. Aliquots (5-10 ml) of intragastric contents were aspirated hourly throughout the study (except at 1000 and 2000 hours), and the pH of each aliquot measured immediately to the nearest 0-01 pH unit by means of a glass electrode and digital pH meter (Radiometer, Copenhagen). The electrode was calibrated with standard buffers (pH 7-00, 4-01, and 1-09: Radiometer, Copenhagen) before and halfway through each hourly batch of samples. Every hour from 0900 to 2400 hours, and two hourly thereafter, blood was taken through a venous cannula for assay of plasma gasrin concentration. The blood was collected in lithiumheparin tubes which contained 0-2 ml aprotinin (Trasylol, Bayer). The tubes were centrifuged immediately, the plasma transferred to plastic tubes and frozen to -20°C. All the plasma samples from each subject were analysed for gastrin in one batch, by radioimmunoassay using antibody GAS 179 in Professor Bloom's laboratory at the Hammersmith Hospital, London. 17 During the study the subjects were fully ambulant around the ward. The food and environmental conditions for both studies were identical to those used in earlier experiments at the Royal Free Hospital.'6 The following meals were served: breakfast, coffee, lunch, tea, dinner Downloaded from http://gut.bmj.com/ on September 30, 2016 - Published by group.bmj.com 292 Smith, Pounder and plasma gastrin concentration was tested using Spearman rank correlation. Differences occurring with a probability of 5% of less were considered significant. Results Two subjects withdrew from the study, but both were found to be taking placebo. The remaining seven subjects completed each part of the study, and no clinically significant abnormality was observed in any of the routine haematology or biochemistry profiles, before or after dosing with either placebo or sufotidine. E E : 9 10 11 12 13 14 2021 22 23 24 1 Time (h) 2 15 16 17 18 19 3 4 6 7 5 8 INTRAGASTRIC ACIDITY Figure 1: Median hourly 24 hour intragastric acidity profile in seven subjects with a history of duodenal ulcer on the fifth day of dosing with placebo (-O* or sufotidine 600 mg bd (O-O). B=breakfast; C=coffee; L =lunch; T=tea; D=dinner; N=nightcap. and a bedtime snack at 0915, 1115, 1315, 1615, 1915, and 2215 hours, respectively. STATISTICAL ANALYSIS 1600 n=7 1400 P<0 001 1200\ 1000 1000 E 600- 400- 200 51 0- Placebo Suf 600mg bd Figure 2: Twenty four hour integrated intragastric acidity in seven subjects on the fifth day ofdosing with placebo or sufotidine 600 mg bd. Twenty four hour profiles of intragastric acidity and plasma gastrin concentration were obtained for every subject in each study period. No gastric aspirates were taken at 1000 or 2000 hours to avoid aspirating drug hence, to calculate the 24 hour integrated acidity profiles, intragastric acidity values of 1-30 and 0 13 mmol/l were used at these times, respectively. The 1 30 and 0-13 mmol/l values represent the median intragastric acidity at 1000 and 2000 hours in 46 healthy subjects, studied under identical conditions when receiving placebo at the Royal Free Hospital. The area under the time-concentration curve for each profile was calculated by the trapezoid rule, with integrated acidity expressed as mmollhIl and integrated plasma gastrin as pmoIIhIl. To make these values comparable with single point measurements of either acidity or gastrin, each value should be divided by 23. The significance of the difference between the integrated 24 hour values were assessed using Wilcoxon's matched-pair signed rank test. The correlation between integrated 24 hour acidity 80 70- B C L 6050- ,' 40- / , (D 30 01 PLASMA GASTRIN CONCENTRATION The 24 hour profiles of median plasma gastrin concentration on the fifth day of dosing with either placebo or sufotidine 600 mg bd are shown in Figure 3, which shows a consistent rise of median plasma gastrin concentration throughout the 24 hours during dosing with sufotidine. Figure 4 shows that the median integrated 24 hour plasma gastrin concentration for the seven subjects during dosing with placebo was 416 pmoIIhIl (range 208-947 pmol/h/l); the concentratons on the fifth day of dosing with sufotidine 600 mg bd had risen in every subject to a median of 927 pmol/h/Il (range 629-1951 pmol/h/l; p 0-001). Figure 5 shows a non-significant inverse correlation between integrated 24 hour intragastric acidity and integrated 24 hour plasma gastrin concentration in the 14 paired data sets from this study (r,=0 4418; p=0 1 14). C , . 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Time (h) range of 8-33%. RELATIONSHIPS BETWEEN INTRAGASTRIC ACIDITY AND PLASMA GASTRIN CONCENTRATIONS 0 a Figure 1 shows the hourly median intragastric acidity on the fifth day of dosing with either placebo or sufotidine 600 mg bd. It shows that during dosing with sufotidine 600 mg bd there was a consistent and profound decrease of acidity throughout the 24 hours. Figure 2 shows that the median integrated 24 hour intragastric acidity for the seven duodenal ulcer subjects with a history of duodenal ulceration during dosing with placebo was 1000 mmol/h/l (range 618-1449 mmol/h/l). On the fifth day of dosing with sufotidine 600 mg bd, integrated 24 hour intragastric acidity was decreased in every subject to a median value of 51 mmolIhIl (range 5-158 mmol/h/l; 95%; p 0-001). For the seven subjects the decreases of 24 hour intragastric acidity ranged from 74% to 99%. The median intragastric acidity was above pH 3 for 17% of the study, with an inter-subject 1 2 3 4 5 I I 6 7 I 8 Figure 3: Median 24 hour plasma gastrin concentration profile in seven subjects on the fifth day of dosing with placebo (- or sufotidine 600 mg bd (O----0). B=breakfast; C=coffee; L =lunch; T=tea; D=dinner; N=nightcap. Discussion This study shows that a twice daily regimen using an H2-blocker is capable of produc- Downloaded from http://gut.bmj.com/ on September 30, 2016 - Published by group.bmj.com Acid inhibition with sufotidine 293 2000 2500 n=7 p< 0.001 n=7 p=0-114 1500- 2000 0 0 E X 0 927 1000 (9~~~~~~~2 500- 1500 E 416 *' o 1000 0Placebo Suf 600mg bd Figure 4: Twenty four hour integrated plasma gastrin concentration in seven subjects on thefifth day of dosing with placebo or sufotidine 600 mg bd. @0 0000 0 0 500 O *. X . 0 200 400 600 800 1000 1200 1400 1600 Acidity (mmol/h/l) Figure 5: Correlation between 24 hour integrated intragastric acidity and 24 hour integrated plasma gastrin concentration in seven subjects, during dosing with placebo (0) or sufotidine 600 mgbd(O). ing virtual elimination of intragastric acidity throughout the day and night in subjects with a history of duodenal ulceration. Hitherto, studies using twice daily regimens of H2-blockers have failed to control day time acidity, particularly in the late afternoon.' 2 The subjects in this study responded to dosing with sufotidine with a median 95% decrease of 24 hour acidity, ranging from 74% to 99%. When 12 duodenal ulcer patients were dosed with omeprazole 20 mg daily for a month under identical conditions at the Royal Free Hospital, they showed a median 97% decrease of 24 hour acidity, but their individual responses ranged from 30% to 100%.9 When higher doses of omeprazole are given (30 mg/day, or more), all patients respond with a consistency similar to that seen with sufotidine 600 mg bd.5 Five days of dosing with sufotidine 600 mg bd were tolerated without any adverse reaction by the seven subjects. The present regimen and lower dose regimens are suitable for testing by clinical trial for their use in the treatment of resistant peptic ulceration, and severe oesophagitis. Supplies of sufotidine and placebo, and financial support, were provided by Glaxo Group Research Ltd. Ms Doris Elliott prepared this manuscript. Technical assistance for this study was provided by D Smart, J Sercombe, P Braidley, J Coward, D Dalgleish, A Jackson, R Walker. 1 Pounder RE, Williams JG, Milton-Thompson GJ, Misiewicz JJ. Twenty-four hour control of intragastric acidity by cimetidine in duodenal ulcer patients. Lancet 1975; ii: 106972. 2 Walt RP, Male PJ, Rawlings J, Hunt RN, Milton-Thompson GJ, Misiewicz Jj. Comparison of the effects of ranitidine, cimetidine and placebo on the 24 hour intragastric acidity and nocturnal acid secretion in patients with duodenal ulcer. Gut 1981; 22: 49-54. 3 Gledhill T, Howard OM, Buck M, Paul A, Hunt RH. Single nocturnal doses of an H2-receptor antagonist for the treatment of duodenal ulcer. Gut 1983; 24: 904-8. 4 Lanzon-Miller S, Pounder RE, Ball SG, Dalgleish DJ, Coward J, Jackson AO. The effects of famotidine, 40 mg at night, on 24-hour intragastric acidity and plasma gastrin concentration in healthy subjects. Scand J Gastroenterol 1988; 23: 244-50. 5 Lanzon-Miller S, Pounder RE, Chronos NAF, Raymond F, Hamilton MR, Dalgleish D. 24-hour intragastric acidity and plasma gastrin concentration in healthy volunteers taking nizatidine 150 mg, nizatidine 300 mg, ranitidine 300 mg, or placebo at 2100h. Gut 1988; 29: 1364-9. 6 Jones DB, Howden CW, Burget DW, Kerr GD, Hunt RH. Acid suppression in duodenal ulcer: a meta-analysis to define optimal dosing with antisecretory drugs. Gut 1987; 28: 1120-7. 7 Chiverton SG, Burget DW, Hunt RH. A meta-analysis to predict duodenal ulcer healing from acid suppression [Abstract]. Gastroenterology 1988; 94: A68. 8 Pounder RE. The pharmacological control of gastric acid secretion. In: Pounder RE, ed. Recent advances in gastroenterology - 7. Edinburgh: Churchill Livingstone, 1988: 245-60. 9 Sharma BK, Walt RP, Pounder RE, Gomes M de FA, Wood EC, Logan LH. Optimal dose of oral omeprazole for maximal 24 hour decrease of intragastric acidity. Gut 1984; 25: 957-64. 10 Lanzon-Miller S, Pounder RE, Hamilton MR, et al. Twentyfour hour intragastric acidity and plasma gastrin concentration before and during treatment with either ranitidine or omeprazole. Aliment Pharnacol Therap 1987; 1: 23952. 11 Tytgat GNJ, Lamers CBHW, Hameeteman W, Jansen JMBJ, Wilson JA. Omeprazole in peptic ulcers resistant to histamine H2-receptor antagonists. Aliment Pharnacol Therap 1987; 1: 31-8. 12 Hinchliffe RFC, Thompson M, Morris P, Daly MJ, Carroll NJH, Walan A. Treatment of refractory peptic ulcer with omeprazole [Abstract]. Gut 1988; 29: A724. 13 Hetzel DJ, Dent J. Oesophageal disease. In: Pounder RE, ed. Recent advances in gastroenterology - 7. Edinburgh: Churchill Livingstone, 1988: 261-89. 14 Lloyd-Davies KA, Rutgersson K, Solvell L. Omeprazole in the treatment of Zollinger-Ellison syndrome: a 4-year international study. Aliment Pharmacol Therap 1982; 2: 1332. 15 Humphray JM, Bays DE, Brittain, RT, Reaves JJ, Stables R. Sufotidine: a competitive and long-acting H2-antagonist [Abstract]. Br Pharmnacol Soc 1988: C54. 16 Lanzon-Miller S, Pounder RE, Hamilton MR, et al. Twentyfour hour intragastric acidity and plasma gastrin concentration in healthy subjects and patients with duodenal or gastric ulcer, or pernicious anaemia. Aliment Pharmacol Therap 1987; 1: 228-38. 17 Bryant MG, Adrian TE. Gastrin. In: Bloom SR, Long RG, eds. Radioimmunoassay of gut regulatory peptides. London: Saunders, 1982: 51-9. Downloaded from http://gut.bmj.com/ on September 30, 2016 - Published by group.bmj.com Sufotidine 600 mg bd virtually eliminates 24 hour intragastric acidity in duodenal ulcer subjects. J T Smith and R E Pounder Gut 1990 31: 291-293 doi: 10.1136/gut.31.3.291 Updated information and services can be found at: http://gut.bmj.com/content/31/3/291 These include: Email alerting service Topic Collections Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Articles on similar topics can be found in the following collections Stomach and duodenum (1688) Gastrointestinal hormones (848) Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/