the lever arm in glenohumeral abduction hemiarthroplasty
advertisement

THE
LEVER
ARM
IN GLENOHUMERAL
HEMIARTHROPLASTY
AFTER
A.
BONI
M.
RIETVELD,
HEIN
From
ABDUCTION
A.
the
M.
DAANEN,
University
PIET
Hospital,
M.
ROZING,
Leiden,
The
WILLEM
R. OBERMANN
Netherlands
Fourteen
cases of hemiarthroplasty
for four-part
fractures
of the proximal
humerus
were reviewed.
Pain
relief was satisfactory,
but function
was limited,
mainly
due to loss of glenohumeral
abduction
despite
elecfromyographic
proof of actively
confracting
abductors
in all cases.
Analysis of special radiographs
of nine cases showed a direct relationship
between the clinical results and
the “humeral
offset”, or distance
between the geomefric
cenfre of the humeral
head and the lateral aspect of
the greater
tuberosity.
This
offset affects
the lever arms of the glenohumeral
abductor
muscles.
The
implications
for surgical
technique
and for the design of shoulder
prostheses
are discussed.
After
hemiarthroplasty
of the proximal
be disappointing.
the
shoulders
and
Bancel
Anquin
for displaced
four-part
humerus
the range of movement
Abduction
is usually
limited
become
1978;
1984;
relatively
Lim
painless
et a!. 1983;
DesMarchais
and
fractures
we used
tends to
although
patient.
(Marotte,
Lord
de Anquin
Morais
and
1984;
de
Willems
and Lim 1985). We have studied
the factors
which
influence
this failure of abduction,
in the hope of finding
clues for improvement.
PATIENTS
From
1979
to 1984
four-part
fractures
at the
Hospital
Orthopaedic
in Leiden
humerus
with
were
women
nine
AND
a total
by
of 14 patients
a Neer
and
Type
with
humerus
Department
reconstruction
of
displaced
were
whose
Orthopaedic
Gasthuis,
P. M. Rozing,
MD,
Professor
Department
W. R. Obermann,
MD,
Head
University
Hospital
Leiden,
the
University
of the proximal
mean
(Neer
which
30 for function,
25 for
radiographic
anatomy.
points,
satisfactory
has
70 and failure has below
pain was recorded
as a
the
and passive
shoulder
Laan
of Orthopaedic
22,
scapular
Using
Surgery
of Department
and
of Surgical
Head
A.
Daanen,
studied
Radiographs
and
we
both
active
were
half-abduction
then
in the
of the
throughout
related
humerus
were
EMG
During
recordings
RC
of
movement,
electronic
examination.
and
measured
Elecfromyography.
plane,
the
to the shape
position
and
head
recorded.
abduction
were
Several
of the
made
in the
from
scapular
12 shoulder
were used for the supraspinafor the other muscles.
During
the abduction
angle
was
goniometer
attached
to the
monitored
elbow
(Vink
by an
et al.
1986).
Radiology
10, 2333 AA Leiden,
The
MSc
Correspondence
should
© 1988 British
Editorial
$2.00
0301-620X/88/4106
VOL.
for pain,
RESULTS
M.
Orthopaedic
Laboratory,
State University
2333 VT Leiden,
The Netherlands.
J Bone
to Neer’s
35 points
and
movement.
Netherlands.
H.
according
videofluoroscopy,
plane
abduction
plane
parameters
65.8
2035
was
of each
range of movement
and 10 for
An excellent
result has over 89
over 80, unsatisfactory
has over
70. The presence
of significant
failure.
scapular
at maximal
shoulder
allocates
evaluation.
determined
the
There
age was
Assessment
1970),
muscles.
Wire electrodes
tus,
and surface electrodes
Surgeon
Boerhaave
Rijnsburgerweg
evaluation.
method
contralateral
scapular
plane and with the arm in a dependent
position.
The humerus
was kept in neutral
rotation
in relation
to
years (range 40 to 81 years). Follow-up
times were from
17 months
to 7 years (mean 3.2 years). For control studies
A. B. M. Rietveld,
MD,
St. Elisabeth’s
of Groote
Haarlem,
The Netherlands.
Clinical
taken
treated
I hemiarthroplasty.
five men
unaffected
Radiological
METHODS
of the proximal
the
Joint
70-B,
Surg
No.
[Br]
be sent
to Dr
Society
1988;70-B:561-5.
4, AUGUST
1988
A.
of Bone
Leiden,
B. M.
and
Mezenstraat
Rietveld.
Joint
Surgery
2A,
The
results
According
of clinical
to the
an excellent
result,
four failures ; the
patients,
both
evaluation
Neer
scoring
eight
given
two
were satisfactory
average
failures,
are
system,
had
score
moderate
was
in Table
patients
and there
I.
had
were
76
points.
Two
pain.
Even
in the
561
A. B. M. RIETvELD,
562
H. A. M. DAANEN,
best results,
abduction
and flexion
were
somewhat
restricted,
while the cases recorded
as failures
had very
poor abduction
and flexion.
Despite
this disappointing
range
of movement
eating
and
toilet
all 14 patients
hygiene.
to use the arm
Only
were
seven
in an overhead
independent
ofthe
position
Degrees
\
6O
Nine
patients
studies
had detailed
; this
radiological
group
their
the
two
excel-
lent results, three of the eight satisfactory
results
four
failures
(Table
II). Active
movement
and all
of the
glenohurneral
all
joint
was
operated
shoulders
three of the failures
glenohurneral
Ankylosis
less
than
(Freedman
there was
angle
during
of the glenohumeral
normal
in
in all
the
clinical
result
and
the range
of active
glenohumeral
abduction
(Figs
1 and 2 and Table
I). Most
abduction
was achieved
by lateral
rotation
of the scapula
which
appeared
normal
humeral
to be normal
relationship
movements
individual
1944).
The
parameters
radiographs
were
in all cases,
between
and
variation
disturbing
scapulothoracic
producing
(Inman,
of head
assessed
thus
shape
in
and
relation
the
and glenoconsiderable
Saunders
and
Abbott
position
to
on the
medial
line
of the
lateral
projection
interval
(A in Fig.
of the humeral
hurneral
shaft
of the
hurneral
head
(B in Fig.
head
S
fracture.
rotation.
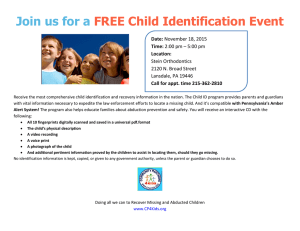
1 . Maximal
There
abduction
is limited
-
30
N
E
S
F
Fig. lb
Relation
between
range
Glenohumeral
abduction
rotation
during
abduction
excellent
result
of movement
and clinical
result.
Figure
1a in the scapular
plane.
Figure
1 b - Scapular
in the scapular
plane.
N, normal
shoulder;
E,
of a Neer
hemiarthroplasty;
5, satisfactory
result;
F,
(C
in
failure.
tuberosity
in relation
Fig. 3) were
the operated
correlate
shoulders
to the
markedly
shoulders,
with
the
the greater
tip
of the
acromion
different
between
the normal
and
but the measurements
did not
clinical
tuberosity
results.
projected
In
the
normal
an average
of
16 mm laterally,
but after arthroplasty
the line of the
greater
tuberosity
was medial to the tip of the acromion.
The distance
between
the geometric
centre
of the
humeral
tuberosity,
head
and
the
lateral
which
we termed
showed
a strong
humeral
abduction
relationship
and
side
of the
the
“humeral
with
therefore
the
with
range
the
clinical
greater
offset”,
of glenoresult
(Figs
beyond
the
3) and
the
upward
clinical
3) showed
at the
greater
not
relate
migration
in all the
to the clinical
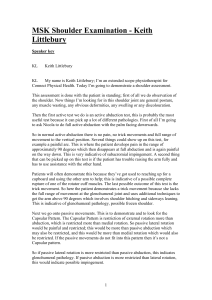
Fig. 2a
Case
F
la
4, 5 and 6, Table II).
The vertical
movement
of the geometric
centre
of
the humeral
head during active abduction
in relation
to
an axis perpendicular
to the glenoid (Poppen
and Walker
1976; DesMarchais
and Morais
1984) showed
excessive
the
results.
The acromiohumeral
no correlation.
Medial
projection
E
Fig.
In
of
at abduction.
excluded
since
some passive glenohumeral
movement
was possible
cases.
There
was a remarkable
relationship
between
N
30
the
and Munro
1966).
an actual
reduction
attempts
joint
was
.\
\
30
and electro-
included
60
able
or to comb
hair.
myographic
W. R. OBERMANN
rees
Deg
for
14 were
P. M. ROZING,
in the scapular
plane
glenohumeral
abduction
replaced
shoulders,
but
did
result.
Fig. 2b
for both arms after a left
on the operated
side with
hemiarthroplasty
symmetrical,
THE
JOURNAL
for four-part
normal
scapular
OF BONE
AND
JOINT
SURGERY
THE
LEVER
ARM
IN GLENOHUMERAL
ABDUCTION
AFTER
HEMIARTHROPLASTY
563
mm
.
30
N
20
10
N
E
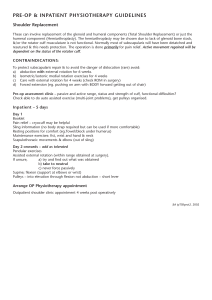
Fig.
Fig.
Figure
4a
humeral
Mean
Fig. 3
offset
-
measured
from
E Excellent
S Satisfactory
F Failure
the geometric
edge of the greater
in millimetres
N Normal
Parameters
of position
and
shape : A,
acromio-humeral
interval
; B, medial
projection
of humeral
head ; C, lateral
projection of greater
tuberosity
in relation
to the
S
F
4b
4a
Humeral
offset
head to the lateral
humeral
N
shoulder
result
result
-
related
-
33 mm
26.5 mm
-
19 mm
12.5 mm
centre
tuberosity.
to the
clinical
of the
Figure
4b
-
result.
(9 cases)
(2 cases)
(3 cases)
(4 cases)
acromion.
Humeral
offset
Lever
.-.-.-.-.-.-.-.
Lever
Diagrams
Line
to show
glenohumeral
arm
of deltoid
arm
of supraspinatus
of muscle
(see
5
action
the influence
abduction
Fig.
of the humeral
offset
on the lever
arm of the deltoid
(D) and the supraspinatus
(5) at various
angles
of
text).
Fig. 6
Examples
failure.
VOL.
70-B,
of humeral
No.
offset.
4, AUGUST
From
1988
left
to right,
normal
shoulder
; Case
1 1 , excellent
result
of Neer
arthroplasty
; Case
2, satisfactory
result
; Case
1,
A.
564
The
B. M.
electromyographic
traction
of the
rotators
of the scapula
RIETVELD,
results
glenohumeral
H. A.
showed
abductors
M.
DAANEN,
active
and
P. M.
con-
the
The
lateral
deltoid
and
the
result
I. Clinical
results
in
14 cases
(Weiner
after
Casenumber
Neer
3
and
can
of the
The
lever
for
2
13
it is lateral
to
the
tip
of
the
acromion
exert
only
an upward
action,
possible
Monastyrski
some
(Van
force.
But
for the lever
helpful,
because
glenohumeral
even
abduction
Linge
and
Mulder
and Stener
1985 ; Howell
estimate
not
shear
glenohumeral
be
1963 ; Markhede,
et al. 1986).
An
arm of the supraspinatus
the
without
should
supraspinatus
is
would
the
only
be
other
abductor.
Although
represent
abductors,
influence
the humeral
offset shown in Figure 4 does
the actual
lever arm of the glenohumeral
the diagrams
on the
lever
(especially
above
in Figure
5 show
arms
of both
30#{176}
glenohumeral
its important
supraspinatus
abduction)
and
deltoid
(especially
below 60#{176}
glenohumeral
abduction).
In the functionally
important
range
of 30 to 60#{176}
of
glenohumeral
abduction,
it seems that the humeral
offset
is closely related
to the lever arms of both muscles.
A
reduced
humeral
offset greatly
reduces
glenohumeral
abduction
power,
and therefore
the range of abduction
four-part
8
fracture
6
1
9
7
4
5
10
12
14
82
81
63
60
49
44
86
80
81
81
87
E
E
S
S
S
F
F
F
F
S
S
S
S
S
M
M
M
F
F
F
M
F
F
F
M
F
F
F
40
65
57
69
69
56
71
72
71
59
56
75
80
81
49
25
67
19
33
39
86
30
37
42
41
28
25
17
120
140
130
150
100
90
125
45
80
30
15
90
80
100
110
125
60
100
100
60
100
90
100
170
100
130
100
120
120
130
100
140
140
100
80
90
100
100
55
60
80
90
50
90
30
60
80
80
80
100
100
100
110
140
80
90
70
90
70
50
70
50
50
70
30
70
70
30
70
70
60
25
30
40
30
15
30
30
25
30
10
20
30
45
of the
operated
AND
JOINT
(months)
in degrees
active
passive
Abductionactive
passive
Medial
rotation
Lateral
rotation
E excellent,
fibres
86
(years)
Flexion
of the posterior
the tip of the acromion.
92
Sex
Movement
some
93
Result
Follow-up
and
from
that
deltoid
Macnab
hemiarthroplasty
11
Neenscore
Age
R. OBERMANN
(Fig. 5). If the greater
tuberosity
is medial
to the line of
the tip of the acromion
as in all our hemiarthroplasties,
the lever arm for the deltoid
is reduced
to zero and this
1970). Furthermore,
arthrography
in one of our failures
showed
an intact
rotator
cuff, so its integrity
does not
seem to be an important
factor.
Table
middle
originate
provided
The average
score of 76 points in our series is in the same
range as the scores reported
for other series (Neer 1970;
Marotte
et a!. 1978; DesMarchais
and Morais
1984;
Stableforth
1984), results which have been described
as
“satisfactory,
but imperfect”
(Neer 1970). We found that
the Neer prosthesis
gave a reasonably
painless
shoulder
and found no new clinical
factors
which influenced
the
result
(Kraulis
and Hunter
1976; DesMarchais
and
Morais
1984; Stableforth
1984). The Neer score gives
most points for lack of pain, and it was obvious,
even in
our best cases, that loss of points for range of movement
was mainly
due to limited
glenohumeral
abduction
(Table
I). The EMG
analysis
showed
that, even in our
worse cases, contracting
glenohumeral
abductors
were
present.
Ifa cufftear
was the cause ofthe poor abduction,
we
would expect a clear relationship
between
the acromiointerval
W.
arm through
which
these
act depends
on the lateral
projection
of the greater
tuberosity,
especially
in the first
60#{176}
of glenohumeral
abduction
(Howell
et a!. 1986)
in all cases.
DISCUSSION
humeral
ROZING,
S satisfactory,
Table
F failure.
II.
Detailed
radiological
Casenumber
Active
movement
Glenohumeral
Scapular
rotation
Humeral
offset
in degrees
operated
normal
operated
normal
in mm
operated
normal
evaluation
and
normal
sides
in nine
patients
3
11
2
13
8
6
1
9
7
36
118
48
61
2
80
1
47
13
34
-1
97
18
80
-23
99
-17
76
48
42
78
69
57
69
67
65
68
46
41
44
52
43
63
28
38
26
39
27
37.5
21.5
31
14.5
32
22
31
14
29.5
17
33.5
6.5
33
15
30.5
THE
JOURNAL
OF BONE
106
SURGERY
THE
LEVER
ARM
IN GLENOHUMERAL
ABDUCTION
AFTER
REFERENCES
and the quality
of the clinical
result. When the offset is
small, the supraspinatus,
in the important
range of 30 to
60#{176}
of abduction,
will
produce
a compressive
force
at the
glenohumeral
joint,
and the deltoid
will produce
an
upward
shear force (Poppen
and Walker
1978). These
abnormal
forces result in loss ofglenohumeral
abduction,
dynamic
fixation
of the glenohumeral
joint and upward
migration
of the humeral
head,
as was seen in our
hemiarthroplasty
patients.
The
lever
arm
principle
applies
to other
be restored
may
the
with
bone
be necessary.
humeral
grafts
When
offset
then
a more
bulky
then
total
force
of the deltoid,
though
this
may
give
HA III, Ranawat
CS, Warren
RF, Inglis AE. Long term results
of
Neer total shoulder
replacement.
In : Bateman
JE, Welsh
RP, eds.
Surgeryoftheshoulder.
Philadelphia,
etc : BC Decker
Inc. St Louis,
etc: CV Mosby
Co, 1984:294-302.
Freedman
a greater
risk
SM, Imobersteg
AM,
the role of the supraspinatus
Joint Surg [Am]
1986;68-A
Inman
VT,
function
Lim
TE, Ochsner
of comminuted
humerus.
Linge
humeral
function.
offset
will improve
these
levers
Fraterman
and
of
and allow
the
thanks
for
their
Jolanda
de Pol
are
technical
to Mr
a commercial
Hans
assistance
Hofman-Hulsink
for his enthusiastic
No benefits
from
due
in any form
party
in the
for her secretarial
co-operation.
have
related
this article.
VOL.
70-B,
No. 4, AUGUST
1988
been
directly
Mr
Wim
orthopaedic
work
received
or indirectly
to Mr
Peter
JH,
S
or will be received
to the
subject
of
Holscher
and fracture
l983;35(4):139-43.
II. Displaced
of three-part
replacement
in fracturethe
humerus.
Injury
of the supraspinatus
muscle
syndrome
: an experimental
1963;45-B:750-4.
etc : CV Mosby
J, Stener
Orthop
and
proximal
J Bone
Co,
and
study
its
in
1984;60-2.
B. Shoulder
function
Scand
1985 ;56:242-4.
L’arthroplastie
complexes
humeral
fractures.
Joint Surg [Am]
proximal
humeral
four-part
displacement.
NK,
Walker
Joint
PS.
Surg
Normal
[Am]
and
fractures.
Part
J Bone
abnormal
les
de
motion
II. Treatment
Joint
Surg
[Am]
osteoarthritis.
of the
shoulder.
1976;58-A:195-201.
PG. Four-part
fractures
Surg [Br] 1984;66-B:l04-8.
DS, Macnab
I. Superior
radiological
aid in the diagnosis
Joint Surg [Br] 1970;52-B:524-7.
of the
neck
migration
of tears
Neer
arthroplasty
l985;56:394-5.
TEA.
deltoid
Part I. Classifica1970;52-A:1077-89.
NK, Walker
PS. Forces
at the glenohumeraljoint
Clin Orthop l978;135:165-70.
Wifiems
WJ, Lim
Orthop Scand
after
de Neer
dams
de l’#{233}paule: a propos
1970;5l-A :1090-103.
Neer CS II. Replacement
arthroplasty
for glenohumeral
J Bone Joint Surg [Am]
l974;56-A:l-13.
Weiner
the
:1-30.
AA. The results
of treatment
dislocations
of the proximal
RK,
Lord G, Bancel
P.
et fractures-luxations
Chirurgie 1978;104:816-2l.
Neer CS II. Displaced
Joint
van
St Louis,
tion and evaluation.
Poppen
Mrs
Neth
Inc.
12 cas.
Deegenaars
laboratory,
and
fractures
J Surg
G, Monastyrski
removal.
Acta
fractures
Neer
Marti
PE,
on
JE, Morais
G. Treatment
of complex
fractures
of the
humerus
by Neer
hemiarthroplasty.
In : Bateman
JE,
RP, eds. Surgery
of the Shoulder.
Philadelphia,
etc : BC
Markbede
muscle
Stableforth
Our
Marone
PJ. Clarification
of
in shoulder
function.
J Bone
JBdeCM,
AbbOtt
LC.
Observations
shoulder
joint.
J Bone Joint
Surg
1944;28
B, Mulder
J Bone
better
DH,
muscle
:398-404.
JD. Function
relation
to the supraspinatus
man.
J Bone Joint Surg [Br]
Poppen
Restoration
Seger
J, Hunter
G. The results
of prosthetic
dislocations
of
the
upper
end
of
1976;8 :129-3 1.
for
supraspinatus.
of the arm in the scapular
plane:
movements
: a roentgenographic
I966;48-A:1503-10.
Kraulis
Marotte
and
Saunders
of the
Decker
of
RR. Abduction
glenohumeral
Joint Surg [Am]
and
J Bone
Howell
glenoid
loosening.
An oversized
glenoid
component
will
tend to hold the remains
of the greater
tuberosity
out
laterally
so restoring
the lever arm of the deltoid,
and its
abduction
power.
But an oversized
glenoid
component
does not restore
the lever arm of the supraspinatus,
so
some weakness
will remain.
We conclude
that poor function
after hemiarthroplasty for four-part
fractures
is due to reduced
lever arms
deltoid
L, Munro
scapular
study.
DesMarchais
proximal
Welsh
replacement,
using
a superiorly
extended,
oversized
glenoid
component
may be indicated
(Bade et al. 1984).
Such a superior
extension
will oppose
the upward
shear
de Anquin CA. Prosthetic
replacement
in the treatment
fractures
of the proximal
humerus.
In : Bayley
I, Kessel
Shoulder
surgery.
Berlin,
etc : Springer-Verlag,
1982:207-17.
Bade
to restore
hemiarthroplasty,
CE,
of serious
L,
eds.
Van
prosthesis
it is not practicable
during
de Anquin
shoulder
conditions
including
osteosynthesis,
other hemiarthroplastics
and total shoulder
replacements.
Hemiarthroplasty for osteoarthritis
of the shoulder
may give better
results than those after four-part
fractures,
because
there
is no bone
loss, the integrity
of the tuberosity
is
maintained
and humeral
offset is preserved
(Neer 1974;
de Anquin
and de Anquin
1982). The principle
of
humeral
offset has important
implications
for prosthetic
design.
Where there is severe loss of bone which cannot
565
HEMIARTHROPLASTY
of the
in abduction.
humerus.
J Bone
of the humeral
head : a
of the rotator
cuff. J Bone
for
humeral
fracture.
Acta