Quantitative Determination of ER:
Adding Clarity to Your Patients’ ER Status
•
•
Accurate and reproducible methods for evaluating Estrogen Receptor status are essential for making the appropriate hormonal treatment decisions for breast cancer patients.
Our quantitative ER score determined by RT-PCR is another measure determining ER status, and provides further insight into an individual’s breast cancer biology and their magnitude of tamoxifen benefit.
Facilitating Identification of Patients Who Are ER-positive
An Oncotype DX® Recurrence Score® will automatically be generated if
the ER status is:
1) positive by IHC or
2) positive by RT-PCR. The patient’s insurance company will be billed in this case.
If the sample is ER-negative by both IHC and RT-PCR, Genomic Health will not provide the Oncotype DX Recurrence Score or
quantitative single gene results, but will provide a qualitative report
confirming the patient’s ER-negative status. The patient’s insurance company will not be billed in this case.
www.oncotypeDX.com
(866) ONCOTYPE • (866) 662-6897
Continuous Measurement & Wide Range of Expression
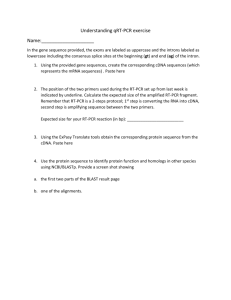
•Breast cancers show a broad range of hormone receptor expression, and RT-PCR is able to measure ER as a continuous variable and capture this wide range of gene expression.
Overall Range
of PR 1000-fold
Range of ER for
ER+ 200-fold
Continuous Measurement of ER and PR1
NSABP B-14 (n = 668)
12
ER-PR+
ER+PR+
ER-PR-
ER+PR-
PR Expression by RT-PCR
11
10
9
8
7
6
5
4
3
2
2
3
4
5
6
7
8
9
10
11
12
13
14
ER Expression by RT-PCR
Overall Range
of ER 3000-fold
•Delay to fixation, duration of fixation and choice of fixative may affect accurate hormone receptor assessment.
•Our RT-PCR employs a wide range of controls and calibrators including reference gene
normalization to reduce this impact and to enhance accuracy and reproducibility in quantitative
single gene assessment.
1
Data on file compiled from Paik, et al.
Data from ECOG & Kaiser Studies
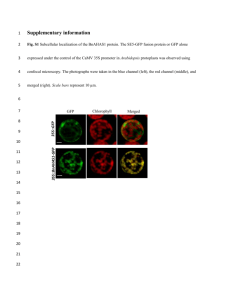
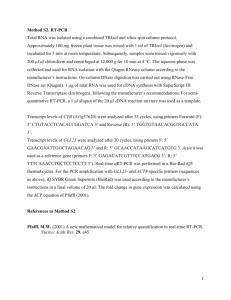
•Studies have demonstrated a high degree of concordance between ER status determined through our quantitative RT-PCR and IHC:
• 9
3% concordance for ER status: E2197 (769 patient samples)2
• 9
6% concordance for ER status: Northern California Kaiser Permanente (607 patient samples)3
ER Measurement: IHC x RT-PCR2
8
ER
Central IHC Allred Score
7
6
IHC-,
RT-PCR+
Discordant
Cases
5
4
3
2
1
0
2
3
4
5
6
7
8
9
10
11
12
13
14
ER Expression by RT-PCR
•Although concordance was high, IHC ER-negative cases that were RT-PCR positive were more common than IHC ER-positive cases that were RT-PCR negative.
• In one study, 14% (central IHC) and 13% (local IHC) of samples classified as ER-negative by
IHC are ER-positive by central RT-PCR.2
J Clin Oncol. 2008;26(25). Badve SS, Baehner FL, Gray R, et al. Estrogen- and progesterone-receptor status in ECOG 2197: comparison of immunohistochemistry by local and central laboratories and quantitative reverse transcription polymerase chain reaction by central laboratory. J Clin Oncol.
2008;26(15):2473-2481.
2
Baehner FL, Maddala T, Alexander C, et al. A Kaiser Permanente population-based study of ER and PR expression by the standard method, immunohistochemistry (IHC), compared to a new method, quantitative reverse transcription polymerase chain reaction (RT-PCR). Presented at the ASCO Breast
Cancer Symposium. September 7-8, 2007; San Francisco, CA. Abstract #88.
3
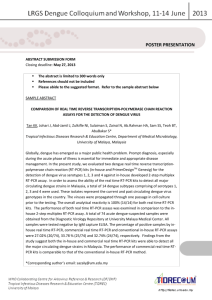
Accurate, Precise and Reproducible
Now Accepting All Appropriate* Early Stage Breast Cancer Samples
Please designate your patient’s ER-negative status on the Requisition Form
in the Exception Criteria box in the Physician Signature area.
Analysis by IHC
(or Unknown)
Quantitative Analysis
by RT-PCR
Report Generation
ER-negative
ER-positive
ER-negative
by RT-PCR
ER-positive
by RT-PCR
ER-positive
by RT-PCR
ER-negative
by RT-PCR
YES
Y ES
Y ES
NO
Oncotype DX:
Recurrence
Score
Oncotype DX:
Recurrence
Score
Oncotype DX:
Recurrence
Score
FAILED
SPECIMEN:
No Recurrence
Score
Page 1
of 4
Inc.
c Health,
Genomi obscot Drive
63
-6897)
301 Pen City, CA 940
d
(866-662
Redwoo ONCOTYPE
)
Tel (866 otypeDX.com
www.onc
PORT
ENT RE
PATI
, Jane
t: Doe
Patien
ale
Sex: Fem 1950
677771
01/01/
t #: 556
DOB:
/Patien
Record
008
Medical
y: 9/25/2
-0001
Surger
SURG
Date of
lock ID:
en ID/B
Specim
PATIEN
G
R00003
T REPO
8
ition:
Patien
15/200
RT
Requis
t: Doe
ed: 10/
, Jane
8
Receiv
Sex: Fem
Order
10/23/200
ter
ale
orted:
DO
dical Cen
ithB: 01/01/
Date Rep
nity Me
ry D Sm
s 1950
Commu
Dr. Har
:
William
Client:
P
ian
n
g Physic ogist: Dr. Joh QUAN
Treatin
Jones TITATI
hol
M
ly
Pat
The
VE SIN
Sal
ting
Onc
nt: Dr.
Submit
®
results otype DX ass
is GLE
l Recipie
reported
aySco
usere
s RT-PCR
usin
Additiona
urrence
The
g
Genomi
c
301 Pen Health, Inc.
Page 3
of 3
Redwoo obscot Drive
d
Tel (866 City, CA 940
63
)
www.onc ONCOTYPE
(866-662
otypeDX
-6897)
.com
GENE
Requis
ition:
R00003
Order
G
Receiv
ed: 10/
Date Rep
15/200
orted:
8
10/23/
REPORT
other met
ER, The
to
PR, Rec
hods or determine the
2008
and HER
or tissue.
reported
RNA exp
2 Scores
es in tum
by othe
are also
21 gen
r laborato ression of the
include
panel of
genes
ries. 1
d in the
ion of a 0.
below.
report
calculat
express
ER Sc
These
0-10
ion of the
results
ore = contained in this
as
rmine the range is from
Recurre
may diffe
ION
to dete
tion
re
features
nce Sco
r from
informa
clinical marized in the
SCRIPT Assay uses RT-PCRRecurrence Sco
ER, PR,
re.
erience with specific
DE
Pos
sum
Y
Exp
The
or HER
itiv
ings
ical
ions
e
ASSA ® Breast Cancerression results.
2
g the Clin
populat whether the finde described.
ted usin lving patient
e exp
e DX
thos
nown
interpre
Oncotyp from the gen
rent from
uld be ical studies invoerience. It is unk The
ed
ures diffeER
ults sho
TIENTS
clin
calculat
ical Exp ents with feat and 607 Score pos
E PA
Test Res derived from
/negativ
sam
pati
of the Clin
SITIVitive
S
which is each section applicable to
cut-off
siteive
g -Po
, ER-PO ples usin
the SP1
of 6.5 unit
RESULT
are
VE
ER
TI
nce
noted in
anti
e,
body (imm s was vali
Experie
NEGA
ClinicalNegativ
=
dated from
Clinical
unohist
de Experie Score of 6
NODE
No
Score
och
R
II,
e
a
e
stud
emi
nce
or
nc
FO
For
I
stry). The
y of
ER currenc :
SIS
itive brea
standard 761 samples
h Stage
Recurre
a Repos
OGNO
Plea
d
usin
deviatio
nts wit
who harece se note: The Avest cancer, the mag7-26.
CE: PR
n for the g the 1D5 anti
ale patie
ived 5
ER Sco
bod
patients
: 281 nitude
PERIEN
years of rage Rat
ed fem
re is less y (immuno
of tamoxif
e of Dist
Those
2004; 351
AL EX
includ
tamoxif
histoch
-7%)
than 0.5
l J Med
en trea
oxifen.
study
emistry
ncer ant Recurrence en benefit increas
CI: 3%
CLINIC
units. 2
y. N Eng
)
lidation
( 95%
rs of tam
ast Ca tment and take
repo
B-14 stud
ve Bre
of
s into acc rted on Pag es as the ER
h 5 yea
nical Va
NSABP
e 1 bas
Score
-Positi
rrence
ount the
The Cli
ated wit
from the
t Recu
magnitu ed on the Rec increases from
TIVE, ER
cer tre
patients
tan
GA
can
668
de
Dis
PR Sc
urrence
6.5 to�
of tamoxif
y of
of
DE NE
breast
ore =
�
12.5. 3
Sco
on stud
en ben
ge Rate
ce in NO s
validati
era
efit indi re was determin
ical
ren
Av
clin
cur
cate
a
osi
ed
d by the
from
had an
Progn
tant Re
Positiv
lts are
ER Sco in patients who
vs Dis
e
re.
wing resu
ore
Sc
follo
ce
The
The PR
Recurren
Score
(immuno
positive
/negativ
PR Sco histochemistry
e
re is less
) and anocut-off of 5.5
units
than 0.5
ther stud
units. 2
y of 607 was validate
d from
samples
using the a study of
761
PR636
antibod samples usin
g
y (imm
unohist the PR636 anti
HER2
ochemi
Score =
stry). The body
standard
deviatio
Negativ
n for the
e
10.0
6
5%
8.0
9.5
The HER
2 positive
concord
ance stud cut-off of��
11.5 unit
PathVy
sion ® ass ies of 755 sam
s, equivoc
ay (FIS
al rang
H). The ples using the
e from
standard
Her
10.7 to
Referenc
11.4
deviatio cepTest™ ass
es:
n for the
1. ER Sco
ay (imm units, and neg
HER2
re base
based
score is unohistochemi ative cut-off
on quan d on quantitati
of < 10.7
stry
less than
titative
2. ASC
unit
ERBB2 ve ESR1 expr
0.5 unit )4 and another
O Brea
expressi
s.
ession
study of s were validate
st Can
3. ASC
(estrogen
on.
cer Sym
568 sam
d
O Annual
posium
receptor
ples usin from
Meeting
4. ASC
2007 Abs
); PR Sco
g the
O
2005
Breast
tracts #87
re base
Abstract
d on quan
by S.S.
#510 by
Symposi
Badve
titative
S. Paik
um 2008
et al., and 1018272
PGR expr
et al.
Abstract
ession
ber 05D#88 by F.L.
s #13 by
(progest
A Num
ovement Baehner
CLI
F.L.
erone rece
Baehner ratory Impr l or for
et al.
ptor); HER
al.,stigationa
ical Laboet
2 Score
as inve and #41 by F.L.
r the Clin
Baehner
lated unde be regarded
Labora
et al.
ry is regu. It should not
tory Dir
rato
om
This test
The labocal purposes
ector:
lth, Inc.
Pa
clini
typeDX.clth, Inc.
Hea
for
tric
deve
Amendm was
nco
omic
k
lope
used
is
Jos
ents of
, MD
c Hea
test d and its
by Gen
www.o
eph, MD
rese
ed arch
Rev015
1988
perf
ng. This
Joseph
GHI004
. The
determin cal
6897) emarks of Genomi
testi
se resu (CLIA) as qual ormance
62-acte
ristics
clini
char
Patrick
6-6
acte
ity
lts
trad
ified
or:
are adju PE (86
char
plex
ristics
to performstered
ect
nctive
TY
dete
ormance orm high-com 's workup. 301
regi high
are
torethe
tory Dir
its perf
-complex rmined by Gen
ONCO nce Sco
Penob
to perf
ordering
6)
physician
ified
Labora developed and as
(86
ity
ring
sco
omic
©
qual
physician
clini
urre
2004-20
orde
t
was
's work cal testing. ThisHealth, Inc.
94063
(CLIA)
e to the
and Rec Drive
08
up.
The
This test ents of 1988 are adjunctiv
test is
City, CA Oncotype DX Genomic Health, Redwood Cit
lts
used for laboratory is
Amendm . These resu
Inc. All
y,
regu
clinical
Redwood reserved.
CLIA Num
rights rese CA 94063
purposes lated unde
research
ber 05D
t Drive lth, Inc. All rights
r the
. It shou
rved. Onc
(86
101827
nobsco
ld not be Clinical Labo
otype DX 6) ONCO
2
ratory
301 Pe 08 Genomic Hea
regarded
TYPE
Improvem
and Rec
as inve
(866-6
ent
urrence
stigationa
© 2004-20
62-689
Score
l or for
7)
are
Cancer
register
ed trad
www.o
emarks
*Decision to submit
samples for testing based
on medical necessity as
determined by the referring
physician.
ncotyp
of Gen
eDX.com
omic Hea
lth, Inc.
GHI004
Rev015
www.oncotypeDX.com
(866) ONCOTYPE • (866) 662-6897
Genomic Health, Oncotype DX, and Recurrence Score are registered trademarks of Genomic Health, Inc.
© 2009 Genomic Health, Inc. All rights reserved. GHI409 10/09