5 CL. III
advertisement

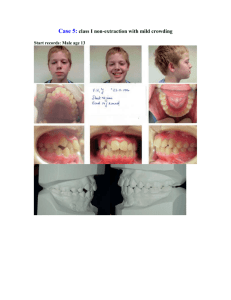
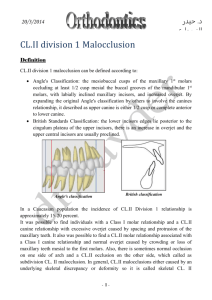
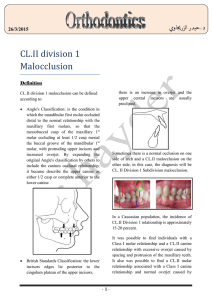
حيدر الزرجياوي.د 16/4/2015 CL.III malocclusion Definition A CL. III malocclusion is rare as compared to other type of malocclusions, with an incidence of possibly less than 5 %. Individual CL. III cases are characterized as having a retruded maxilla or a prognathic mandible and in some cases by a combination of both. It is of special interest to the orthodontist because it offers a therapeutic challenge. CL.III malocclusion can be defined according to: Angle's classification: the mesiobuccal cusps of the maxillary 1st molars occluding at least 1/2 cusp distal the buccal grooves of the mandibular 1st molars, and the canines relationship, it described as upper canine is either 1/2 cusp or complete posterior to lower canine. In other words, the lower teeth occlude mesial to their normal relationship with the upper. In CL. III cases, the lower incisors and canines are inclined lingually because of the pressure of the lower lip in its effort to close the mouth. The disharmony between maxilla and mandible may be of lesser degree with a normal occlusion on one side of the arches and a CL. III occlusion on the other, so it is called CL. III subdivision malocclusion. Clinical Features of skeletal CL.III Extra-Oral Features British standards classification: the lower incisors edges lie anterior to the cingulum plateau of the upper incisors. -1- A concave facial profile. Anteriorly divergent profile. Long face (increased lower face height), which may be pointed at the chin. Mandible appears to be well developed (with an obtuse gonial angle). Orthodontics……….…………………………………………….....……..…............... Cl. III Malocclusion Intra-Oral Features that distinct characteristics of a CL.III malocclusion due to prognathic mandible were related to genetic inheritance. A CL.III molar relationship. A CL.III canine relationship. A reverse overjet with possibly labially inclined lower incisors and lingually inclined upper incisions. A posterior cross-bite unilateral or bilateral (or functional) due to a constricted maxillary arch or a more forward positioned mandibular arch. Soft tissue and habits The soft tissues have minor influences on the CL. III malocclusion pattern. In fact, the reverse is often the case, with the soft tissues tending to tilt the upper and lower incisors towards each other so that the incisor relationship is often less severe than the underlying skeletal pattern. Macroglossia, or anteriorly tongue posture, which lies low in the oral cavity, are to be a local factors in CL.III development. Dental factor Occlusal forces created by the abnormal eruption may produce unfavorable incisal guidance and promote a CL.III incisors relationship. This may present initially as a pseudo CL. III but if unattended can lead to a true CL.III malocclusion. Premature loss of second primary molars can lead to forward drifting of permanent molars; the mandibular first permanent molar assumes a more mesial position, resulting in a dental CL.III permanent molar relationship. Classification In evaluating the CL.III relationship, it is important to consider whether the problem is dentoalveolar or skeletal in origin. In the diagnosis of CL.III malocclusions, patients may present with CL.III symptoms such as multiple teeth in anterior crossbite, minimal overjet, or lingually inclined lower incisors. In summary, anterior crossbites may be caused by the improper inclination of the maxillary and mandibular incisors (dentoalveolar), occlusal interferences (functional), or skeletal discrepancies of the maxilla and/or the mandible. Etiology Skeletal factor Skeletal relationship is the most important factor in the etiology of most CL.III malocclusion, and the majority of CL.III incisor relationships are associated with an underlying CL.III skeletal relationship. The growth pattern and the size of the jaws are affected by heredity. Many studies showed Premature loss of deciduous molars may also cause anterior mandibular displacement. If the mandible loses it's posterior proprioceptive and functional support in habitual occlusion it is often positioned anteriorly in an attempt to establish full occlusal contact during chewing. -2- Orthodontics……….…………………………………………….....……..…............... Cl. III Malocclusion Congenital Abnormalities 3. To simplify phase II comprehensive treatment. In mild and moderate Class III patients, early treatment may eliminate the necessity for orthognathic surgery treatment. 4. To improve occlusal function, especially if it is accompanied by a functional shift. 5. To provide more pleasing facial esthetics, thus improving the psychosocial development of a child. A transverse as well as anteroposterior restriction of the mid-face growth can occur in cases of cleft lip and palate with a normal mandible, markedly when the patient has undergone the surgical repair. This can be attributed to restraining effect of scar tissue following surgical intervention. Limitation in vertical growth of the maxilla can also be seen. Treatment of Dentoalveolar Functional CL.III Malocclusion & Early treatment should be considered in these cases, in order to avoid potential adverse growth influences in the maxilla and mandible, and to improve upper lip posture and facial appearance. Correction of multiple teeth in anterior crossbite has been accomplished by using a fixed or removable appliance. During mixed dentition stage, the removable appliance with springs can be used successfully to tip one or more of upper incisors labially. In addition, a mandibular Hawley appliance with an anterior labial bow can be used to tip the lower incisors lingually. Correction of CL. III malocclusion using removable appliance to change the upper and/or lower incisors inclination can be considered in cases with following features: Management CL.III malocclusion can be classified as Dentoalveolar, Functional, or Skeletal, which will determine the treatment approach and prognosis. It is known that Class III malocclusion exacerbates during growth, mainly starting at adolescence. There are three main treatment options for skeletal class III malocclusion: growth modification, dentoalveolar compensation (orthodontic camouflage), and orthognathic surgery. Growth modification should be commenced before the pubertal growth spurt, after this spurt, only the latter two options are possible. The goals of early interceptive treatment of CL. III malocclusion may include the following: 1. To improve skeletal discrepancies and provide a more favorable environment for future growth. 2. To prevent progressive irreversible soft tissue or bony changes. Anterior crossbite is often accompanied with Class III malocclusion can lead to thinning of the labial alveolar plate and/or gingival recession. -3- A CL.I and mild CL.III skeletal pattern. The upper incisors are not already proclined and the lower not already retroclined. Well aligned teeth. Sufficient overbite should be present at the end of treatment, to retain the corrected incisors position. Orthodontics……….…………………………………………….....……..…............... Cl. III Malocclusion of the pressure of the appliance on the lower lip and dentition. The lower anterior facial height tends to increase so it is contraindicated for a child who has excessive lower face height. Treatment of Malocclusion Skeletal CL. III Treatment of Growing Patient The developing skeletal Class III malocclusion is one of the most challenging problems confronting the orthodontists. Differentiate between midface deficient Class III patients that would benefit from early treatment vs. a true mandibular prognathism that may require surgical correction later. Class III malocclusions are growth related problems that often become severe if left untreated, so the treatment could be beneficial if initiated early. For a mild to moderate skeletal CL.III malocclusion, among the approaches for treatment is the growth modification by using of orthopedic appliances, such as chincup, facial masks, and functional appliances. On the other hands, for the cases with severe skeletal prognathism, no treatment until orthognathic surgery can be done at the end of the growth period may be the best treatment. Functional Appliance Therapy The Frankel III appliance is used in treatment of cases with mild maxillary deficiency, and can be effective if the case is diagnosed early. The biggest problem is of patient cooperation. The Frankel III appliance possible action is made with labial (vestibular) pads to stretch the upper lip in addition to the periosteum forward, in a way that stimulates forward growth of the maxilla. At the same time, it does not allow the mandible to advance forward. Actually, most of the improvement is from dental changes. The appliance allows the maxillary molars to erupt and move mesially while holding the lower molars in place vertically and anteroposteriorly tips the Chin Cup Therapy CL.III malocclusion with a relatively normal maxilla and a moderately protrusive mandible may be treated with the use of chin-cup. Chin cup is used to apply forces (450 gm per side), which are directed along the direction of growth of the condyle. Therefore it's action are accomplished to lesser extent by restraining the forward growth of the mandible, and to larger extent by change in the direction of mandibular growth, rotating the chin down and back. In addition, lingual tipping of the lower incisors occurs as a result -4- Orthodontics……….…………………………………………….....……..…............... Cl. III Malocclusion maxillary anterior teeth facially and retracts the mandibular anterior teeth. Vertical movement of maxillary molar will help in rotating the chin down, back, and improve facial appearance. canine-primary molar area above the occlusal plane. Approximately 350-450 grams of force per side is applied via the elastics for 12-14 hours per day. Treatment of adolescent growing patients and non- Treatment in the adolescent age is limited to Orthodontic Camouflage or orthodontic decompensation in an effort to prepare the patient for surgery. Camouflage can be achieved by proclining the maxillary incisors and tipping the mandibular incisors lingually. Single arch extractions, 1st premolars extraction only in the mandibular arch, are frequently done to create space for the retraction of the mandibular anterior segment. CL.III elastics in combination with fixed appliance are frequently used in an effort to tip/retract the mandibular incisors. Facemask (Delaire Mask) Therapy The facemask can be used in growing patients with Class III malocclusions due to both anteroposterior and vertical maxillary deficiency, to help provide the impetus for the maxilla to grow anteriorly and/or rotate downwards. This causes a reciprocal downward and backward rotation of the mandible. It. is a very effective appliance if the patient is cooperative. The facemask obtains anchorage from the forehead and chin. The forward force on the maxilla is generated via elastics that attach to an intra-oral maxillary appliance (either fixed or removable). The removable appliance if used, it is preferred to be as splint to make the upper arch a single unit for maxillary protraction. The maxillary appliance must have hooks for attachment located in the In a more severe cases and after the growth is ceased, Orthognathic Surgery is indicated. It is suggested for patients with an ANB angle of greater than -4°. The most commonly used surgical procedures are the bilateral sagittal -5- Orthodontics……….…………………………………………….....……..…............... Cl. III Malocclusion split osteotomy with retraction of the mandible in cases of mandibular prognathism, in cases of maxillary deficiency a Le-Fort I down positioning may be attempted. -6-