A Numerical Simulation of Flow in a Two-Dimensional End-to
advertisement

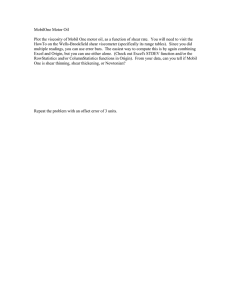
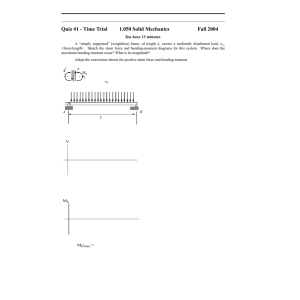
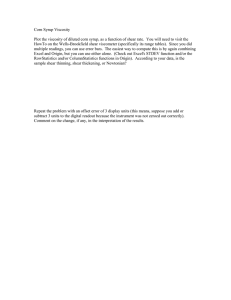
D. A. Steinman Department of Mechanical Engineering. Bach Vinh C. Ross Ethier Department of Mechanical Engineering and Institute for Biomedical Engineering. M. Ojha !!. S. C. Cobbold K. W. Johnston Institute for Biomedical Engineering. University of Toronto, Toronto, Canada A Numerical Simulation of Flow in a Two-Dimensional End-to-Side Anastomosis Model In order to understand the possible role that hemodynamic factors may play in the pathogenesis of distal anastomotic intimal hyperplasia, we carried out numerical simulations of the flow field within a two-dimensional 45 degree rigid-walled endto-side model anastomosis. The numerical code was tested and compared with experimental (photochromic dye tracer) studies using steady and near-sinusoidal waveforms, and agreement was generally very good. Using a normal human superficial femoral artery waveform, numerical simulations indicated elevated instantaneous wall shear stress magnitudes at the toe and heel of the graft-host junction and along the host artery bed. These sites also experienced highly variable wall shear stress behavior over the cardiac cycle, as well as elevated spatial gradients of wall shear stress. These observations provide additional evidence that intimal hyperplasia may be correlated to wall shear stresses over the cardiac cycle, high wall shear stress gradients, or a combination of the three. The limitations of the present work (especially in regard to the two-dimensional nature of the flow simulations) are discussed, and results are compared to previous observations about distal anastomotic intimal hyperplasia. Introduction The long-term success of bypass graft surgery is frequently limited by the development of intimal hyperplasia, a progressive thickening of the pseudointima or neointima that eventually leads to occlusion of the graft lumen (DeWeese, 1985; Dilley et al., 1988; Suggs et al., 1988). Intimal hyperplasia occurs preferentially at graft-vessel anastomoses, and is most commonly seen in distal anastomoses, in end-to-side anastomoses, and in synthetic rather than vein grafts (DeWeese, 1985). Sottiurai and co-workers (1983, 1984) reported that anastomotic intimal hyperplasia tends to occur preferentially at the heel and toe of the graft and on the bed of the parent vessel for the end-to-side configuration (Fig. 1). The mechanisms most commonly advanced to explain this intimal thickening are mechanical mismatch, hemodynamic factors, or some combination of both factors (DeWeese, 1985). In the hemodynamic theory, it has been proposed that intimal hyperplasia is promoted by abnormal blood flow patterns, such as recirculating zones, turbulence, and/or abnormal wall shear stress. LoGerfo et al. (1979) hypothesized that platelets "trapped" in recirculating zones will tend to aggregate and release platelet-derived growth factor, leading to myocyte proliferation, while Morinaga et al. (1985) stated that unphysiological variation in wall shear stress promotes intimal thickening at the distal anastomosis. Hemodynamic mechanisms have also been proposed by Crawshaw et al. (1980), Matsuzaki (1988), Contributed by the Bioengineering Division for publication in the JOURNAL OF BIOMECHANICAL ENGINEERING. Manuscript received by the Bioengineering Division July 24, 1991; revised manuscript received May 2, 1992. Associate Technical Editor: L. Talbot. 112 / V o l . 115, F E B R U A R Y and Fujiwara et al. (1988). Recently our group reported the results of a 3D experimental model study of flow in an endto-side anastomosis (Ojha et al., 1990). Evidence was presented that suggests a correlation exists between low and fluctuating wall shear stress and intimal hyperplasia. Flow in a 2-D endto-side anatomosis has been numerically simulated by Pietrabissa et al. (1990), who limited their attention to steady flow. Although the number of elements (and hence the resolution) in their study was somewhat limited, they observed a separated region at the toe of the anastomosis. In spite of the studies mentioned above, at present there does not appear to be a sufficiently detailed understanding of the flow field in an end-to-side anastomosis to permit a careful evaluation of the hemodynamic hypothesis for the development of intimal hyperplasia. One possible means of addressing host artery intimal hyperplasia after Sottiurai etal., 1984 Fig. 1 The distribution of intimal hyperplasia in an end-to-side anastomosis (after Sottiurai et al., 1984) 1993 T r a n s a c t i o n s of t h e A S M E Copyright © 1993 by ASME Downloaded 17 May 2008 to 128.100.48.224. Redistribution subject to ASME license or copyright; see http://www.asme.org/terms/Terms_Use.cfm were solved by applying Galerkin finite element discretization in conjunction with penalty function decoupling. Briefly, in the penalty function method (Reddy, 1982a, 1982b; Cuvelier et al., 1986; van de Vosse et al., 1986), the continuity equation has added to it a term involving the pressure: V-u + ep = Q (4) where e is a small parameter of order 10~6. This modification 1 allows the continuity and momentum equations to be decouhost artery hee ? toe pled, while introducing a small error of order < e ' / 2 (Reddy, 1982b). Cuvelier et al. (1986) indicate that the penalty function approach yields an approximate 10-fold decrease in computational requirements. The general solution method was that described by van de Vosse et al. (1986), and quadrilateral Q£ - P . enriched CrouFig. 2 The finite element mesh used in numerical simulations of steady flow (Re = 136) and near-sinusoidal unsteady flow in an end-to-side an- zeix-Raviart elements (quadratic in velocity, linear in pressure) astomosis, in which a host artery (horizontal) is joined by a graft at 45 were employed. Time-stepping was treated in an implicit mandegrees, (a) Overview of entire mesh; (b) Close up of boxed region from ner, using the first-order accurate Euler Backward scheme, (a). Note terminology. and the resulting nonlinear equations were solved by Newton iteration. A skyline storage and factorization algorithm (Dhatt this deficiency is through numerical modeling and in vitro and Touzot, 1984) was used to minimize storage and comexperiments. Our group has therefore undertaken a detailed putational requirements. The quadrilateral element mesh and nomenclature used for study of flow in an end-to-side anastomosis, with the goal of identifying those hemodynamic patterns that could potentially the simulations are shown in Fig. 2. For the steady and nearlead to intimal hyperplasia. It is the purpose of the present sinusoidal code verification studies, the mesh consisted of 752 study to use numerical techniques to gain a qualitative un- elements and 4766 velocity degrees of freedom. The compuderstanding of the flow and wall shear stress behavior in a 2- tational domain extended 16 channel heights downstream along D model end-to-side anastomosis for a physiologically relevant the host artery from the toe of the anastomosis, 10 channel heights upstream from the anastomosis heel, and 4 channel flow waveform. heights upstream along the graft from the toe of the anastomosis. For all simulations, the graft and host were assumed Materials and Methods to have the same channel height. For the physiological waveOverview. In this preliminary study we have considered form simulations, the mesh shown in Fig. 2(a) was enlarged the idealized case of unsteady laminar flow of a Newtonian by extending the downstream outlet and graft inlet to 32 and fluid in a two-dimensional rigid-walled model of an anasto- 10 channel heights respectively, thereby increasing the number mosis. The assumption of laminar and Newtonian behavior is of elements to 1008. This was necessary to accurately handle approximately correct for the vessels sizes and flow rates of the larger Reynolds numbers and negative flow rates encouninterest, and synthetic grafts and diseased arteries are expected tered when using the physiological waveform. to be relatively stiff, partially justifying our rigid wall asNo-slip boundary conditions were imposed on all solid sursumption. As well, Ku and Liepsch (1986) have noted that faces, and fully developed flow at the outlet plane was enforced vessel wall elasticity only slightly modifies the flow field, so by assuming zero traction, which corresponds to zero pressure we feel that a rigid wall simulation should be an adequate and zero axial velocity gradient at the outlet plane. Finally, a approximation. We have also assumed that there is no flow prescribed velocity profile entering the upstream (proximal) through the proximal end of the host artery, corresponding to portion of the graft was applied, based upon a series of 2-D the case of graft implantation in a severely stenosed artery. Womersley velocity profiles (Currie, 1974) weighted by the For code validation studies steady and near-sinusoidal flow Fourier components of the flow waveform. Thus, inlet boundwaveforms were employed. Further numerical studies used a ary conditions in the anastomosis model corresponded to fullyflow waveform based on in vivo measurements of flow in the developed flow in a straight graft. superficial femoral artery using Doppler ultrasound, as deSimulations were carried out on a Cray XMP and on a Sun scribed below. This flow waveform and geometry were chosen SPARCStation II. For the unsteady cases, 60 time-steps per to simulate the conditions that might be seen in an end-to-side cardiac cycle were used, and the resulting simulation took anastomosis of the human femoral artery. approximately one Cray CPU hour per cardiac cycle. For simulations of unsteady (periodic) flow, numerical convergence Numerical. After appropriate nondimensionalization, the was considered to have occurred when the Euclidean vector 2-D Navier-Stokes equations in primitive variable form may norms of the velocity field at all corresponding times in two be written as: successive cycles differed by less than 10~ 3 . In general, three cycles were required to satisfy this criterion. AOL du 1 , „ (1) Experimental. The photochromic dye tracer method (Ojha where Re is the Reynolds number and a is the Womersley et al., 1988a, 1988b, 1990) was used for flow visualization. In parameter: this technique, a normally colorless indicator dye (0.01 percent by weight l',3',3'-trimethyl-6-nitrobenzospiropyran) is disHU Re = (2) solved in deodorized kerosene. The dye is rapidly ( < 1 \ii) turned dark blue by intense ultraviolet light, such as that produced by a nitrogen laser. Up to seven traces were produced (3) simultaneously by firing a laser across the test section, and these were photographed 20 ms after formation to determine U, the inlet mean velocity, is a characteristic velocity scale and a set of flow displacement profiles which were digitized to H, the channel height, is the characteristic length scale. The produce quantitative velocity data. A schematic of the optical momentum and continuity equations in primitive variable form arrangement is shown in Fig. 3. j a= l Journal of Biomechanical Engineering FEBRUARY 1993, Vol. 115 /113 Downloaded 17 May 2008 to 128.100.48.224. Redistribution subject to ASME license or copyright; see http://www.asme.org/terms/Terms_Use.cfm (b) laser beam 5 mm • 50 t mm • Fig. 3 Schematic of optical arrangement used in experimental studies. (a) Side view of experimental setup; (b) end view of experimental setup at section A-A, showing flow channel dimensions. nominal sinusoidal data points spline lit Fig. 4 Plot of Reynolds number Re and volumetric flow rate Q(ml/min) versus time fraction (defined as time divided by the flow period 7) for the near sinusoidal flow waveform used in numerical simulations. Dashed line: nominal sinusoidal flow waveform; bullets: data points, measured as described in text; solid line: spline fit to data points used for numerical simulations. The experimental test section consisted of a "two-dimensional" flow channel constructed from UV-transparent Plexiglas. The model had a channel height i f of 5 mm, a width of 50 mm (10:1 aspect ratio), an entrance length of 190 mm, and a graft-vessel angle of 45 degrees (Fig. 3). A flow straightener was positioned immediately downstream of the test-section inlet, and thus boundary layers can be expected to develop on the bottom and top walls, and on both side walls in the test section. The aspect ratio and entrance length upstream of the test section were chosen so that boundary layers on the channel side walls would be thin in comparison to the channel depth of 10H, and so that the flow would be fully developed across the channel height i f in the measurement region. The dye traces were formed and then photographed at the center of the channel (i.e., 25 mm from each side wall), so as to minimize threedimensional effects. Both steady and unsteady flow experiments were performed. Unsteady flow was produced by superimposing a nominally sinusoidal flow from a calibrated piston pump on the mean flow. For steady flow, volumetric flow rate was determined in two ways: (i) the time required to collect a calibrated volume was measured (bucket and stopwatch method); and (ii) a ve114 / Vol. 115, FEBRUARY 1993 locity profile obtained at the channel midplane at a distance 22H from the toe of the junction was digitized, numerically integrated, and multiplied by the channel depth (5 cm). We note that these approaches will only produce identical results in the absence of sidewall effects, and defer further consideration of this point to the Discussion section. Under steady flow conditions the instantaneous flow rate was estimated as described in (ii) above. This approach was necessary because compliance effects in the experimental system caused the flow waveform delivered to the test section to be slightly different from the nominal flow waveform produced by the pump system. We therefore refer to this as "near-sinusoidal" flow. All experimental Reynolds numbers reported in the present study are based on channel height H-5 mm, mean velocity U (flow rate/channel cross-sectional area), and a kinematic viscosity v = 1.89 cStokes. For steady flow, a Reynolds number (as determined by method (i) above) of 130 was used, while for pulsatile flow the nominal conditions were: mean Reynolds number of 125, one half peak-to-peak or modulation Reynolds number of 96, and Womersley parameter a of 7.74. Photographs of the dye traces were taken at 40 ms intervals throughout the pulsatile flow cycle duration of 345 ms. Since limitations of the measurement system did not enable more than one photograph to be taken per flow cycle, a complete set was obtained from different flow cycles by incrementing the delay between the start of the cycle and the laser firing by 40 ms for each successive photograph. Photographic negatives were digitized using a COHU CCD camera (640 X 480 pixels) equipped with a Canon 100 mm macro lens plus extension tubes and interfaced to an IBM AT computer. A minimum magnification of 15 was used, and each digitized image consisted of two to three traces of a given photographic frame. By curve-fitting to the digitized profiles, the velocity gradient at the channel wall was determined, whose product with the dynamic viscosity (1.43 cPoise) enabled the wall shear stress to be calculated. Doppler Ultrasonography. In order to obtain representative flow waveforms to be used as input for the numerical model, pulsed Doppler recordings of blood flow were made from the superficial femoral artery on three ostensibly normal subjects using an Acuson 128 colour Doppler flow imaging system. Vessel diameters were measured in two orthogonal planes using B-mode imaging, and Doppler flow measurements were made with the sample volume filling the arterial lumen as completely as possible. The instantaneous flow was computed by multiplying vessel cross-sectional area by the instantaneous mean velocity. Results Experimental/Numerical Comparison. In order to compare experimental data with the results of our 2-D numerical simulations it was desirable to verify that flow in the model anatomosis was effectively two-dimensional. Accordingly, a series of dye traces were formed at 22 channel heights downstream from the toe (i.e., Z = 22, where Z i s the axial distance downstream from the toe, made dimensionless with respect to H). At this location, velocity profiles were observed to be essentially independent of cross-sectional position, with the exception of a thin layer (thickness <0.5if) adjacent to the channel side wall, confirming the essentially 2-D nature of the flow field downstream of the toe. However, when similar tests were performed within 0.5H of the heel, transverse (i.e., in the plane of Fig. 3(b)) velocity components were observed, indicating that some 3-D flow effects were present in the neighborhood of the junction. The accuracy of the digitization and integration procedure for estimating flow rates was tested under steady flow conditions. For measured flow rates yielding Reynolds numbers of 130 and 160, the digitization procedure yielded Reynolds Transactions of the ASME Downloaded 17 May 2008 to 128.100.48.224. Redistribution subject to ASME license or copyright; see http://www.asme.org/terms/Terms_Use.cfm (a) 0.3 2.3 3.9 dimensionless axial distance downslream (ram toe (Z) Fig. 7 Mid-femoral flow waveform calculated from Doppler ultrasonography and used in numerical simulations Table 1 Fourier coefficients a,„ b„ used in Eq. (5) to produce the physiological flow waveform shape seen in Fig. 7 a„ 1.466328 0.296833 1.713260 0.370048 0.087783 Fig. 5 Comparison between experimentally determined and numerically calculated dimensionless velocity profiles in 2-0 model anastomosis at axial locations Z=0.3, 2.3, and 3.9. Solid lines: experimental results; dotted lines: numerical predictions. Note velocity calibration vectors, (a) Steady flow (Re = 136); (b) near-sinusoidal unsteady velocity profiles for selected times throughout the flow cycle. 2 0,4 0.6 0.8 traction of period 1 0 0.2 0.4 0.6 0.8 1 0 fraction of period 0.2 0.4 0.6 0 fractkin of period Fig. 6 Comparison between experimentally determined and numerically calculated dimensionless wall shear stress (r) at axial locations Z = 0.3,2.3, and 3.9 throughout the near-sinusoidal flow cycle. Solid lines: numerical predictions, near wall; dotted lines: numerical predictions, far wall; squares: experimental data, near wall; bullets: experimental data, far wall. numbers of 136 and 160, respectively, confirming the 2-D nature of the flow field far from the toe. We therefore estimate that the error involved in this procedure is <5 percent. For unsteady flow, instantaneous volumetric flow rates were measured in this manner at 11 instants throughout the flow cycle. By spline-fitting these experimentally measured flow rates, a "near-sinusoidal" waveform was determined, and is compared to the nominal sinusoidal waveform in Fig. 4. The near-sinusoidal waveform was used in subsequent code validation studies. Velocity profiles obtained from the numerical simulations under steady flow conditions in the model anastomosis are Journal of Biomechanical Engineering b„ 0.797575 2.932334 0.010294 -0.441529 -0.152390 compared to the corresponding experimental data at Z = 0.3, 2.3, and 3.9 in Fig. 5(a). Similar profiles for unsteady flow are shown in Fig. 5(b). Generally excellent agreement between numerical and experimental results is seen, with the exception that there are slight differences between numerical and experimental results very near the toe of the anastomosis (i.e., at Z = 0.3) on the lower wall of the host artery. Finally, in Fig. 6, we compare experimentally measured and numerically computed wall shear stresses throughout the flow cycle at Z = 0.3, 2.3 and 3.9. Generally, fair to good agreement is noted, with discrepancies most evident near the toe and along the near wall of the host artery. Physiological Flow Waveform. In Fig. 7 we show a measured mid-femoral flow waveform shape as measured by Doppler ultrasonography. This physiological flow waveform is characterized by a rapid acceleration to a peak systolic flow of approximately eight times the mean, and an equally rapid deceleration through zero flow to a peak reverse flow rate approximately three times the mean. A period of less intense acceleration then leads to a post diastolic peak, followed by a return to zero flow and the start of the next cardiac cycle. The flow waveform shape was obtained by digitizing a representative flow waveform from the pulsed Doppler recordings , and then smoothed by considering only its first five Fourier components, defined by: - = 1 + 2 (a„ cos 2wnt/T+ b„sin limt/T) Qn, (5) where / is the time, T\s the period of the flow cycle, Qmean is the mean (cycle-averaged) flow rate, and the Fourier coefficients a„ and b„ are listed in Table 1. The measured mean (cycle-averaged) flow rate was 195 ml/ min, and the measured artery diameter was 6.5 mm. To better represent flow conditions in typical bypass graft patients, we chose to scale the measured flow waveform to give a mean flow rate of 135 ml/min, which is well within the range of typical femoral bypass graft flow rates (Shearman et al., 1990; Lee and Baird, 1990; Levy et al., 1981; Stabile and Wilson, 1977; Albrechtsen, 1976). The resulting mean and peak Reynolds numbers were 125 and 980, and the Womersley number was 4.7, obtained by assuming a pulse rate of 70 beats/min and a blood viscosity of 3.5 cStokes. FEBRUARY 1993, Vol. 115 /115 Downloaded 17 May 2008 to 128.100.48.224. Redistribution subject to ASME license or copyright; see http://www.asme.org/terms/Terms_Use.cfm (b) (b) minium (c) llllIMM iiiimiiiiiiiiiiiiiiiillillillllliti ' III'IIIII I (c) mim "wiiiiiiiiiiiiiiiiiiiiiiiiiiiiimiiiiiiiiiiiiiiiiuiiiii Fig. 8 Numerically calculated velocity vector and wall shear stress plots for physiological unsteady flow at peak forward flow, (a) Location of peak forward in flow cycle; (b) velocity vector plot; (c) wall shear stress plot. Fig. 10 Numerically calculated velocity vector and wall shear stress plots for physiological unsteady flow at peak reverse flow, (a) Location of peak reverse in flow cycle; (b) velocity vector plot; (c) wall shear stress plot. (a) graft inlet, as well as a very small recirculating region just distal to the toe of the graft-host junction. The locations of the recirculation zones are mirrored in the wall shear stress plot (Fig. 8(c)), in the form of negative wall shear stresses in the host artery slightly distal to the toe and on the bed of the (b) host artery. The wall shear stress plot indicates the presence of elevated shear stresses just at the toe of the graft-host junction, and on the bed of the host artery. Here we note that the term "elevated" refers to wall shear stress magnitudes noticeably larger than those which would be observed for flow in a straight channel (or, equivalently, flow far downstream of the toe in the host artery) for the same flow rate. At zero flow (Fig. 9(b)), we note a more complicated flow pattern, as flow is now entering the junction through the center of the graft, but leaving near the walls. The slowly rotating m ""ll Illlllllllllllllll vortex on the bed noted above has now enlarged and moved (c) over the graft inlet, while the small recirculation zone in the host artery has also increased in size to form another vortex further downstream. This complicated flow pattern appears in the wall shear stress plot (Fig. 9(c)) as highly variable, mostly negative, wall shear stresses in the host artery. Note the presence of elevated shear stresses distal to the toe and on the bed, where the strong vortices are present. Also note the highly elevated shear stresses at the heel, a result of some of the reverse Fig. 9 Numerically calculated velocity vector and wall shear stress plots for physiological unsteady flow at zero flow, (a) Location of zero flow dividing as it hits the sharp corner of the heel. in flow cycle; (b) velocity vector plot; (c) wall shear stress plot. At peak reverse flow (Fig. 10(b)), a more regular flow pattern is seen, with flow now entering the junction through the Numerical. Figures 8-10 show plots of the computed di- host artery and leaving through the graft. The two distal vormensionless velocity vectors and corresponding dimensionless tices present downstream in the host artery at zero flow have wall shear stresses in the junction at three different times in now been washed away; however, the proximal vortex has the flow cycle. In the wall shear stress plots, the length of the ' moved from the graft inlet back to the proximal portion of lines normal to the graft geometry indicate the magnitude of the host artery. The wall shear stress plot (Fig. 10(c)) indicates the wall shear stress at the given location, made dimensionless uniform wall shear stress around most of the junction, except with respect to pU2. Lines pointing away from the geometry for some elevated shear stresses as flow rounds the toe, and indicate positive wall shear stresses, while lines pointing into highly elevated shear stresses as flow divides around the heel. the geometry indicate negative wall shear stresses. Note the Also note the low wall shear stresses on the bed of the host artery. calibration line at the downstream end of the host artery. Figure 11 shows the behavior of the wall shear stress over At peak forward flow (Fig. 8(b)), flow is coming up through the graft and out through the host artery. There is a large, the entire flow cycle. The cycle-averaged wall shear stress, slowly rotating vortex in the host artery just proximal to the defined as: 116 / Vol. 115, FEBRUARY 1993 Transactions of the ASME Downloaded 17 May 2008 to 128.100.48.224. Redistribution subject to ASME license or copyright; see http://www.asme.org/terms/Terms_Use.cfm iiiiiiwiiiifcLiMH^.., (a) Fig. 11 Cycle mean and limit wall shear stress plots for physiological unsteady flow. See text for definition of terms. Note scaling for mean wall shear stress plot, which is different than that for limit wall shear stress plot, (a) Mean; (b) limits. 7-avg = ^,J Tdt (6) where r is the instantaneous dimensionless wall shear stress, is shown in Fig. 11(a). This plot indicates the presence of elevated average wall shear stresses at both the toe and heel of the graft-host junction, and on the bed of the host artery. Another useful representation of the overall behavior of the wall shear stresses is the limit plot (Fig. 11(6)). In this plot, the maximum possible wall shear stress at a given location is represented by a line pointing away from the domain, while lines pointing into the domain indicate the maximum negative wall shear stress. Taken together, the length of a line at a given point represents the maximum variation in wall shear stress over the flow cycle. This plot indicates that elevated temporal variations in wall shear stress (i.e., over the cardiac cycle) are present at the toe, heel and distal bed. We also note a large spatial variation in wall shear stress in these same areas. Discussion Numerical/Experimental Comparison. Comparison of numerical and experimental results for steady and near-sinusoidal flows shows generally very good agreement, with some small discrepancies as described in the Results section. We feel that these discrepancies are most likely attributable to experimental causes. For example, the experimentally measured flow waveform indicates that a perfect sinusoidal variation in the flow rate was not achieved, perhaps due to unavoidable compliance effects in connecting tubing and the flow circuit. For the purposes of the numerical simulation, a spline fit of the experimentally measured flow rates was used to model the flow waveform, rather than assuming a purely sinusoidal variation; however, differences between the real experimental and fitted numerical waveforms, caused by the limited amount of data available for the spline fit, are likely the cause of the slight disagreement between profiles at the three axial locations shown in Fig. 5(b). With regard to the differences observed near the toe of the junction, we feel that these are most likely due (at least in part) to unavoidable three-dimensional flows in the experimental studies. There will in general be secondary flows created at the anastomotic junction, which appear to have been minimized Journal of Biomechanical Engineering but not completely eliminated in our experiment. Such flows will be strongest in the near vicinity of the graft toe, which is where maximum discrepancies were noted. As well, grid refinement studies indicate that the flow in this area of the model is numerically well-resolved. Thus, it seems likely that discrepancies seen near the toe are due to experimentally occurring secondary flows. These differences are of course magnified in the comparison of numerically computed and experimentally measured wall shear stresses, since the derivative of the velocity profile is sensitive to small variations in the velocity profile near the wall. Flow Patterns and Physiological Implications. Simulations of unsteady physiological flow clearly indicate the presence of elevated wall shear stress magnitudes at the toe and heel of the junction, as well as the on the bed of the host artery, at different times during the flow cycle. The large magnitudes of the wall shear stresses at the heel and toe can be partially attributed to the (unphysiological) sharpness of the corners of the mesh, which are effectively singular points. However, these singular points were eliminated in a subsequent mesh by rounding the corners and eliminating all slope-discontinuities around the toe and heel (approximate radii of curvature at the toe and heel were 0.08// and 0.01//, respectively), and results (not shown) indicated similar behavior of the wall shear stresses, except with a slight overall decrease in magnitude of the elevated wall shear stresses. These results suggest a correlation between locations of high instantaneous (as opposed to cycle-averaged) wall shear stresses, and sites known to be susceptible to the development of intimal hyperplasia (compare Figs. 1 and 11). However, locations of high instantaneous wall shear stress are also sites of high temporal and spatial wall shear stress gradients. Thus, any one of these effects, or a combination of the three, may play a role in the development of intimal hyperplasia. The current study does not permit us to isolate these effects and identify the most probable single initiating factor (if in fact intimal hyperplasia is initiated by a single factor). Previous studies (e.g., Bassiounyetal., 1988) have suggested that intimal hyperplasia is correlated with the presence of low wall shear stresses. In the present work, we do not find a strong correlation between sites of low wall shear stress and locations of intimal hyperplasia. In fact, the proximal end of the host artery, which is a very low wall shear stress environment, is not considered to be a site of intimal hyperplasia (see Fig. 1). The fact that this site is a low wall shear stress environment is confirmed by experimental studies (Ojha et al., 1991) and limited numerical studies which include the effects of moderate flow "leakage" through the stenosis (Steinman et al., 1991). Although it would be premature to discount the low wall shear stress theory based upon these observations, we suggest that low wall shear stress may not be the only hemodymamic initiating factor leading to the development of intimal hyperplasia, and that the possibility of high wall shear stress or high wall shear stress (temporal or spatial) gradients as initiating factors needs to be more closely examined. The 2-D Flow Approximation. It is understood that flow in an end-to-side anastomosis is inherently three-dimensional. For example, Ojha et al. (1990), have pointed out that the anastomotic flow field is in some regards similar to that seen in a curved tube, with strong secondary helical flows present. This was indirectly confirmed in the present study, since secondary flows were seen experimentally near the toe of the junction even in our "approximately 2 D " channel. We do note, however, a similarity between some of the flow features observed in this 2-D study, and flow patterns reported by Ojha et al. (1990) for unsteady flow in a 3-D in vitro endto-side anastomosis model. For example, they noted a persistent recirculating zone in the proximal portion of the host artery and mobile stagnation points on the bed of the host FEBRUARY 1993, Vol. 115 /117 Downloaded 17 May 2008 to 128.100.48.224. Redistribution subject to ASME license or copyright; see http://www.asme.org/terms/Terms_Use.cfm artery. They also reported elevated wall shear stresses on the bed of the host artery above the graft inlet, as was seen in the present study. A major difference between the experimental work of Ojha et al. and the present study is our observation of high wall shear stress at the heel, in contrast to experimental observations of low wall shear stress at this location. However, this can be explained by the different flow waveforms used in these two studies; the present work used a waveform with a significant negative flow component (which is required for elevated wall shear stress at the heel), while Ojha et al. used only forward flow. Also, we note that Ojha et al. observed low wall shear stresses in the region of the host artery immediately distal to the toe. This is confirmed in the present study; however, we have also shown the presence of elevated wall shear stresses proximal to and at the toe. Because of the resulting large spatial gradients in wall shear stress, it may be quite difficult to experimentally resolve the wall shear stress behavior at the toe. This may account for the absence of observed elevated wall shear stresses at the toe in the study by Ojha et al. We therefore conclude that many of the major flow characteristics present in the 3-D anastomosis model are also present in the 2-D model, and thus important qualitative information about the flow field in the end-to-side anastomosis can be obtained from the present study. Of course, a 2-D model cannot replicate inherently 3D flow structures; however, the above discussion indicates that they do not markedly affect the major details of the wall shear stress behavior, at least in the Reynolds number range of interest. Finally, it should be noted that the geometry used in the present study, although representative of distal anastomoses, is idealized. For example, the presence of a hood in the anastomosis will likely alter flow patterns at the toe. Such effects, as well as the effects of distensible vessel walls, need to be further examined. Acknowledgment Financial support from the Whitaker Foundation is gratefully acknowledged. References Albrechtsen, D., 1976, "Intra-Operative Haemodynamic Findings and Their Prognostic Significance in Femoropopliteal Reversed Saphenous Vein Graft Bypass Operations," Scand. J. Thorac. Cardiovasc. Surg., Vol. 10, p. 67. Bassiouny, H. S., Lieber, B. B., Giddens, D. P., Xu, C. P., Glagov, S., and Zarins, C. K., 1988, "Quantitative Inverse Correlation of Wall Shear Stress with Experimental Intimai Thickening," Surg. Forum, Vol. 39, p. 328. Crawshaw, H. M., Quist, W. C , Serrallach, E., Valeri, C. R., and LoGerfo, F. W., 1980, "Flow Disturbance at the Distal End-to-End Anastomosis," Arch. Surg., Vol. 123, p. 1280. Currie, I. G., 1974, Fundamental Mechanics of Fluids, McGraw-Hill, New York. Cuvelier, C , Segal, A., and van Steenhoven, A. A., 1986, Finite Element Methods and Navier-Stokes Equations, D. Reidel, Dordrecht. DeWeese, J. A., 1985, "Anastomotic Neointimal Fibrous Hyperplasia," Com- 118 / Vol. 115, FEBRUARY 1993 plications in Vascular Surgery, 2nd ed., Bernhard, V. M., Tourne, J. B., eds., Grune & Stratton, New York. Dhatt, G., andTouzot, G., 1984, The Finite Element Method Displayed, John Wiley & Sons, New York. Dilley, R. J., McGeachie, J. K., and Prendergast, F. J., 1988, "A Review of the Histologic Changes in Vein-to-Artery Grafts, with Particular Reference to Intimai Hyperplasia," Arch. Surg., Vol. 123, p. 691. Fujiwara, T., Fumihiko, K., and Kanazawa, S., et al., 1988, "Comparison of Blood-Flow Velocity Waveforms in Different Coronary Artery Bypass Grafts,'' Circulation, Vol. 78, p. 1210. Ku, D. N., and Liepsch, D., 1986, "The Effects of Non-Newtonian Viscoelasticity and Wall Elasticity on Flow at a 90 Degree Bifurcation," Biorheology, Vol. 23, p. 359. Lee, R. E., and Baird, R. N., 1990, " A Haemodynamic Evaluation of the Femoro-Femorai Cross-Over Bypass," Eur. J. Vase. Surg., Vol. 4, p. 167. Levy, B. I., Michel, J. B., Bailliart, O., and Lagneau, P., 1981, "Etude Hemodynamique par Velocimetrie Ultrasonique a Impulsion des Pontages Axillo-Femoraux," Arch. Mai. Coeur., Vol. 74, p. 979. LoGerfo, F. W., Soncrant, T., Teel, T„ and Dewey, C. F., 1979, "Boundary Layer Separation in Models of Side-to-End Arterial Anastomoses," Arch. Surg., Vol. 114, p. 1369. Matsuzaki, Y., 1988, "Usefulness of Sequential Bypass Technique in Arterial Reconstruction," Nippon Geka Gakkai Zasshi, Vol. 89, p. 443. Morinaga, K., Okadome, K., Kuroki, M., Miyazaki, T., Muto, Y., and Inokuchi, K., 1985, "Effect of Wall Shear Stress on Intimai Thickening of Arterially Transplanted Autogenous Veins in Dogs," J. Vase. Surg., Vol. 2, p. 430. Ojha, M., Cobbold, R. S. C , Johnston, K. W., and Hummel, R. L., 1988a, "High Resolution Photochromic Dye Method for Pulsatile Flow Studies," Proceedings of the International Symposium on Biofluid Mechanics, April 27-29, 1988, Palm Springs, CA. Ojha, M., Hummel, R. L., Cobbold, R. S. C , and Johnston, K. W„ 1988b, '' Development and Evaluation of a High Resolution Photochromic Dye Method for Pulsatile Flow Studies," J. Phys. E: Scientific Instruments, Vol. 21, p. 998. Ojha, M., Ethier, C. R., Johnston, K. W., and Cobbold, R. S. C , 1990, "Steady and Pulsatile Flow Fields in an End-to-Side Arterial Anastomosis Model," J. Vase. Surg., Vol. 12, p. 747. Pietrabissa, R., Inzoli, F., and Fumero, R., 1990, "Simulation Study of the Fluid Dynamics of Aorto-Coronary Bypass,"J. Biomed. Eng., Vol. 12, p. 419. Reddy, J. N., 1982a, "Penalty Function Analysis of 3D Navier-Stokes Equations," Comp. Meth. Appl. Mech. Eng., Vol. 35, p. 87. Reddy, J. N., 1982b, "On Penalty Function Methods in Finite Element Analysis of Flow Problems," Int. J. Nutner. Meth. Fluids, Vol. 2, p. 151. Shearman, C. P., Hickey, N. C , and Simms, M. H., 1990, "Femoro-Distal Graft Flow Augmentation with the Prostacyclin Analogue Iloprost," Eur. J. Vase. Surg., Vol. 4, p. 455. Sottiurai, V. S., Yao, J. S. T., Flinn, W. R., and Batson, R. C , 1983, "Intimai Hyperplasia and Neointima: an Ultrastructural Analysis of Thrombosed Grafts in Humans," Surgery, Vol. 93, p. 809. Sottiurai, V. S., and Batson, R. C , 1984, "Ultrastructural Studies of Arterial Grafts," Evaluation and Treatment of Upper and Lower Extremity Circulatory Disorders, Bergan, J. J., Yao, J. S. T., eds., Grune & Stratton, New York. Stabile, B. E., and Wilson, S. E., 1977, "The Profunda Femoris-Popliteal Artery Bypass," Arch. Surg., Vol. 112, p. 913. Steinman, D. A., Ethier, C. R., and Johnston, K. W., 1991, "Further Studies on Flow in an End-to-Side Anastomosis," 1991 Advances in Bioengineering, Vanderby Jr. R., ed., ASME Press, New York. Suggs, W. D., Henriques, H. F., and DePalma, R. G„ 1988, "Vein Cuff Interposition Prevents Juxtanastomotic Neointimal Hyperplasia," Ann. Surg., Vol. 207, p. 717. van de Vosse, F. N., Vial, F., and van Steenhoven, A. A., 1985, "A Finite Element and Experimental Analysis of Steady and Pulsating Flow Over a TwoDimensional Step," Numerical Methods in Laminar and Turbulent Flow, Taylor, C , Olson, M. D., Gresho, P. M., Habashi, W. G., eds., Pineridge Press, Swansea. van de Vosse, F. N., Segal, A., van Steenhoven, A. A., and Janssen, J. D., 1986, "A Finite Element Approximation of the Unsteady Two-Dimensional Navier-Stokes Equations," Int. J. Numer. Meth. Fluids, Vol. 6, p. 427. Transactions of the ASME Downloaded 17 May 2008 to 128.100.48.224. Redistribution subject to ASME license or copyright; see http://www.asme.org/terms/Terms_Use.cfm