NHS 111 and the Summary Care Record
advertisement

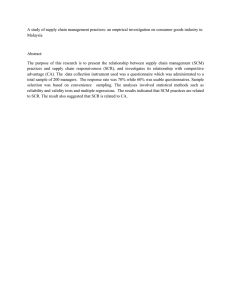
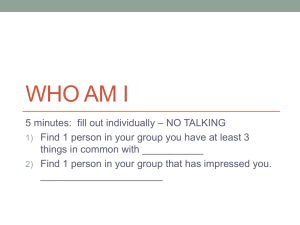
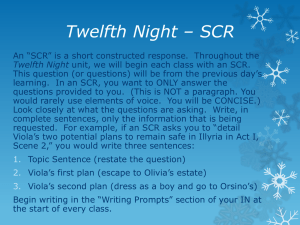
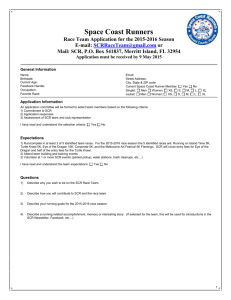
Summary Care Record Viewer Guidance Including Additional Information Version 0.37 – June 2015 For further information or to request support: scr.comms@hscic.gov.uk The Summary Care Record and Additional Information 1. What is the Summary Care Record (SCR)? 1.1. The SCR is an electronic patient record containing up to date key information from the patient’s GP record. It is available throughout England and as of June 2015 over 96% of people in England have an SCR. 1.2. Currently, most patients have an SCR containing the core dataset SCR (medication, allergies and adverse reactions as a minimum) - see Fig.1. SCRs can also contain Additional Information over and above the core dataset where patients provide their explicit consent for this to happen. 2. Interpreting the SCR (Fig.1) 2.1. The core SCR dataset present in all records is: Allergies and adverse reactions to medication; Current repeat medication; 12 months of acute medication (or 6 months if stated); 6 months of discontinued repeat medication (unless otherwise stated). 2.2. The SCR is sourced from the patient’s GP record only. Therefore, it may not include the entire list of the patient’s over the counter medications or items prescribed outside of the GP practice, unless the practice has manually entered these items into their GP system or the information is part of a wider shared record from another organisation. These items will be labelled on the SCR (under Type) as ‘Prescribed Elsewhere’. 2.3. The SCR is marked with the last date and time that an update was sent by the GP practice. Viewers should check this to ensure that they understand when the record was last updated – see Fig. 1 – Note 1.2. 2.4. A message will be displayed if a patient has recently changed their GP practice, as this could indicate that the SCR content is not yet fully up to date – see Fig.1 – Note 1.1. This message will be displayed if the SCR has been newly created or has not yet been created by the patient’s new GP practice; either because the new GP practice does not yet hold information to overwrite the existing SCR, or because they have not yet started uploading SCRs. These messages, in conjunction with the date and time stamp, should be used to assess how current the SCR information is (see Fig. 1). 2.5. A message will be displayed when items have been withheld from the SCR. This may be because GP system privacy settings have been used to restrict the sharing of certain information from the patient’s GP record. 3. Additional Information Content in the Summary Care Record (Fig. 2) 3.1. Functionality is being enabled in GP systems during spring and summer 2015 to provide an improved mechanism for Additional Information to be added. This will include: Reason for medication Significant medical history (past and present) Significant procedures (past and present) Anticipatory care information – such as information about the management of long term conditions Communication preferences – as per the ISB-1605 dataset End of life care information – as per the ISB-1580 dataset Immunisations For further information or to request support: scr.comms@hscic.gov.uk Page 1 of 8 Items are identified for inclusion due to their presence above either as part of a key dataset (e.g. End of Life care) or because they appear in a relevant section of the GP record, e.g. items appearing as ‘significant problems’ within the GP system are likely to be automatically included. GP practices may also manually add further information, in accordance with patient wishes. 3.2. As this improved functionality is enabled and utilised, Additional Information will slowly become more widespread – particularly for those patients who will benefit most – such as patients approaching the end of life, the “frailest 2%” and those with long term conditions and/or communication problems such as patients with learning disabilities or dementia. 3.3. There are differences in the underlying GP record format, supplier implementation, local data quality and patient preferences. As a result, the content of SCRs with Additional Information will vary from record to record but will follow a broadly consistent presentation format explained below. 3.4. SCR content is limited to information held in GP systems but may include information from shared records. Therefore, the SCR Additional Information may include relevant content recorded by other organisations and shared with the GP practice. 3.5. The data included in the SCR consists of coded items from the GP system together with any supporting free text. The codes are translated to SNOMED terminology1 and presented to the SCR viewer. Some of the primary care terminology may not be familiar to emergency and other secondary care clinicians – see 3.22 below. There is no standard for the recording of supporting free text and its quality will vary, but when present in the SCR it generally provides additional useful detail to supplement the coded information. This may also include information that may be considered sensitive or relate to un-necessary third party information – see sensitive information below (3.14 and 3.15). 3.6. The SCR with Additional Information is generally larger - typically 2-3 times the size of the core SCR (3-16 pages). 3.7. The SCR with Additional Information follows the existing SCR format with the core dataset of the record containing medications, allergies and adverse reactions remaining at the top of the SCR. When Additional Information has been added, Reason for Medication will appear against relevant medication if this has been recorded by the GP practice. 3.8. Additional Information will appear below the core SCR, grouped under the following Care Record Element (CRE) headings: 1 For further information on SNOMED CT see the SNOMED CT GP user guide: http://systems.hscic.gov.uk/data/uktc/training/snmdct_gp_userg.pdf For further information or to request support: scr.comms@hscic.gov.uk Page 2 of 8 3.9. The headings are determined by the UK Terminology Centre (UKTC) and are a mechanism to group SCR items within individual patient records. A heading will only appear in an individual SCR if there is relevant information available from the patients GP record for inclusion under that heading. Some headings are only likely to be used in limited circumstances e.g. ’Third Party Correspondence’ will not generally be present, as this information cannot currently be attached to the SCR – although the existence of correspondence in the GP record could be signposted. 3.10. When headings are shown, they always appear in the order above. 3.11. There is no specific ‘End of Life’ heading but End of Life care information will appear under relevant headings e.g. the Resuscitation status (see section 3.12) will always appear under Personal Preferences and diagnoses will appear under Diagnoses. 3.12. Resuscitation Information in the SCR: Resuscitation Codes in the Summary Care Record Only the most recent instance of the Resuscitation (Do Not Attempt Cardio-pulmonary Resuscitation - DNACPR) codes from the GP system is displayed in an SCR with Additional Information (if this information is recorded in the GP system). This always appears under the Personal Preferences heading along with other End of Life preferences such as preferred place of care or death. If the code has been marked in the GP record as an active problem, then it may also appear under the SCR Problems and Issues heading. Resuscitation status in the SCR is only to be treated as a signpost to information that is fully recorded elsewhere and viewers and clinicians are advised to continue to follow their existing processes according to local and national standards 3.13. The quality and completeness of the Additional Information included in an SCR is dependent on a number of factors including the underlying clinical record, data quality and confidentiality issues. As a result, SCR viewers should be aware that the SCR potentially may not be complete and should be seen as an additional clinical tool to support current practices. 3.14. Items defined in the Royal College of GP’s (RCGP) sensitive dataset, found at: http://systems.hscic.gov.uk/scr/gppractices/additional/rcgpexc2015aprv1.xls which specifically relate to in-vitro fertilisation, sexually transmitted diseases, terminations of pregnancy and gender re-assignment are automatically excluded from Additional Information, but can be manually added by the patient’s GP practice, if the patient wishes. However, there may be other items deemed as sensitive which may have been included as codes or referenced in free text i.e. details of abuse or un-necessary information related to third parties. Viewers are reminded to treat the SCR information with sensitivity as for any other clinical records and to take steps to avoid inappropriate disclosure when discussing information with patients, family and carers. 3.15. When an item is excluded from SCR Additional Information because it is in the RCGP sensitive dataset, a message is included in the SCR. As per section 2.4 above a general message is included at the top of the SCR indicating that one or more items have been withheld from the SCR. See Fig. 3. 3.16. There are a number of known causes of duplication and repetition within the SCR with Additional Information. These include duplication of codes from the underlying system, data quality issues, inclusion of repeated vaccinations or different instances of similar information from shared records. Means for filtering these out are being considered. For further information or to request support: scr.comms@hscic.gov.uk Page 3 of 8 3.17. SCRs may contain auto generated text defining problem detail from the GP system. This may be of less relevance for non GP viewers. Examples include Significant Active, Significant Past, Minor Active, Minor Past, End Date, Problem; New – see Fig.2. 3.18. Problems and Issues is a special section that may contain the patient’s active problems, where they have been identified as such in the GP system. Some systems may also include significant past or inactive problems. Any items that appear under this heading will also appear under their respective defined headings as well e.g. heart failure in Figure 3 appears in Diagnoses and also Problems and Issues. 3.19. Immunisations / vaccinations currently appear under Treatments. The placement of these items is being reviewed. 3.20. Clinical Observations and Findings may include some observation values – such as blood pressure – but only if the GP system adds them systematically (which not all do) or if the GP practice mark the items for inclusion or because they were recorded in a relevant section of the GP record for inclusion in SCR. 3.21. Investigations and Investigation Results only contain items manually added by the GP practice or because they were recorded in a relevant section of the GP record for inclusion in SCR. 3.22. GP systems use different versions of codes to record clinical information1. The information included in the SCR is converted to SNOMED CT codes for display. Some codes may include terminology unfamiliar to non-primary care SCR viewers. Examples of these include: [D]= codes for working diagnoses when a specific diagnosis is not yet ascertained. [M]= related to morphology of neoplasms [EC]= Classified elsewhere in a code, usually referring to an underlying cause of a particular disorder. [NEC]= not elsewhere classified [HFQ]= however further classified [OS]= otherwise specified - only used when a definitive code is not available. [NOS]= not otherwise specified - only used when a definitive code is not available. [SO]= Site of [V]= Supplementary factors influencing health status, but not including illness [X][Q] relate to cross-reference and qualifier information - not important for viewing Other clinical notation that may also be encountered includes: O/E = On examination C/O = Complaining of H/O = History of P/H = Personal history of F/H = Family history of CXR = Chest x-ray NAD = No abnormality detected 3.23. The SCR examples shown in this guidance are screenshots of the SCRa web application. There are some presentation differences between the SCRa and printouts. For further information or to request support: scr.comms@hscic.gov.uk Page 4 of 8 Figure 1: Viewing the core SCR 1.1 If the patient is no longer registered with this GP practice (see 3.4), or if items have been deliberately withheld from the SCR (see 3.4) the relevant message below will be clearly displayed in the SCR: Patient registration ended [date]. GP Summary no longer being updated One or more entries have been deliberately withheld from this GP Summary 1.2. Date and time when the SCR was last updated (see 2.3) 1.3. Items prescribed outside the GP practice will only appear if entered by the GP practice. Their Type will be labelled as Prescribed Elsewhere (See section 3.2) 1.4. Last issued date may not appear for current repeat medication on every SCR. In this case the Date First Added will appear 1.6. If Discontinued Repeat Medications are not being sent by the patient’s GP practice the following message will appear in this section: The Discontinued Repeat Medications are not included in this summary For further information or to request support: scr.comms@hscic.gov.uk 1.5. If an SCR contains Additional Information it will appear under relevant headings beneath the core data (see section 4.7) Page 5 of 8 Figure 2: Viewing Additional Information in the core SCR 2.1. If the patient consents to Additional Information, Reason for Medication will be included if recorded in the GP record 2.2. If the Reason for Medication is recorded in the GP system but is excluded from the SCR, then this is indicated 2.3. Additional Information appears below the core SCR grouped under SNOMED headings. In this example, Diagnoses are the first information to be included in the SCR . 2.4. Additional Information appears as individual rows (in reverse date order), comprising: 1. Date of the event (Date) 2. The SNOMED equivalent of the coded item included from the GP system (Description) 3. Supporting free text (Additional Information sub-heading) In this example, the supporting text includes auto-generated information from the GP system indicating the problem detail of the coded item e.g. it is a Problem and this is the First Episode. The auto-generated information is system specific and will vary depending on which GP system produced that individual SCR. The successive text “end stage” is the supporting free text recorded by the GP practice when this information was recorded For further information or to request support: scr.comms@hscic.gov.uk Page 6 of 8 Figure 3: Viewing Additional Information below the core SCR 3.1 The Diagnoses heading includes the patient’s diagnoses that have been automatically included in the SCR Additional Information. 3.2 Problems and Issues is a special section that contains the patient’s Active and significant past Problem items if they have been identified as Problems in the patient’s GP record. These items also appear elsewhere in the SCR under their own relevant defined headings. 3.3 The supporting free text provides additional useful detail to supplement the coded information. It may include sensitive or third party information – see 3.14 and 3.15 3.4. Clinical Observations and Findings may include some observation values – such as blood pressure – but only if the GP system adds them systematically (which not all do) or if the GP practice mark the items for inclusion or because they were recorded in a relevant section of the GP record for inclusion in SCR. In the example above, some information has been marked as confidential or private in the GP system and is therefore not included in the SCR. When this occurs in the SCR, a message is included indicating that one or more items have been withheld from this SCR. For further information or to request support: scr.comms@hscic.gov.uk Page 7 of 8 Figure 4: Viewing Additional Information below the core SCR 4.1. The Treatments heading includes vaccinations. The example here shows the annual influenza vaccination which can contribute to repetitive information in the SCR. 4.2 Investigations and Investigation Results will only contain items specifically identified in the GP system for inclusion. More detailed information may be available in the GP record but not present in the SCR 4.3. The Personal Preferences section contains patient preferences such as those regarding End of Life care and Resuscitation status – see section 3.12 4.4. This section can include details of Next of Kin Further information can be found at http://systems.hscic.gov.uk/scr/gppractices/additional and any questions can be sent to the Health and Social Care Information Centre (HSCIC) SCR team at scr.comms@hscic.gov.uk. For further information or to request support: scr.comms@hscic.gov.uk Page 8 of 8