Chapter 17 Chronic Leukemias 1
advertisement

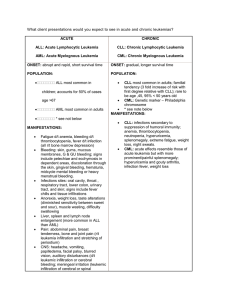
Chapter 17 Chronic Leukemias 1 Chronic Lymphocytic Leukemia 2 CLL ► Chronic – mature cells, signs and symptoms develop gradually, and often discovered accidentally; May not be diagnosed for 1015 years! ► Lymphocytic – lymphoproliferative disorder ► Leukemia – replacement of normal bone marrow with neoplastic cells, causing anemia, thrombocytopenia, and neutropenia 3 CLL ► Most common form of leukemia in older adults ► Patients usually in their 50’s when diagnosed ► Average survival time is 5 years; May take an aggressive course with only 1-2 years of survival time ► Many CLL patients die from infections ► No known specific etiologic agent or cause for CLL ► Most frequently a neoplasm of B-lymphocytes (rarely T cells) ► Lymphocytes are small and have relatively mature, well-differentiated appearance ► Bare nuclei, called “smudge cells” frequently found 4 CLL ► Will develop altered humoral immunity resulting from suppression of all classes of immunoglobulins, leading to hypogammaglobulinemia; Subsequent increase in susceptibility to infections ► Many patients (15-35%) develop autoimmune disorders and produce autoantibodies to neutrophils, platelets (i.e. ITP), or RBCs (WAIHA) ► Have significantly impaired immunologic activity 5 CLL ► Normal adult peripheral blood: B-cell lymphocytes 30% with surface immunoglobulins T-cell lymphocytes 70% without surface immunoglobulins ► Very important to differentiate which type of lymphocytes are involved in the CLL (B cells or T cells) ► Diagnosis of CLL can be done morphologically, but distinguishing between T-cell and B-cell CLL requires testing for cluster differentiation (CD) antigens 6 CLL ► Malignant B cells of CLL do not progress to the final stages of development, the plasma cells; Appear to stop developmentally at earlier Blymphocyte stage of development ► CLL usually presents with elevated WBC count with many lymphocytes ► Not usually curable with available therapy ► Treatments include bone marrow transplants, radiation, chemotherapy, and intravenous gamma globulin to help prevent bacterial infections 7 CLL Laboratory Results ► ► ► ► ► Anemia is usually normochromic, normocytic with a normal to low reticulocyte count Autoimmune hemolytic anemia may develop (positive DAT and elevated indirect bilirubin) Often a decreased PLT count, due to bone marrow replacement of megakaryocytic precursors or platelet antibodies Lymphocytes may be morphologically identical to normal mature lymphocytes, or may have a “soccer-ball” type of staining appearance Immune dysfunction and hypogammaglobulinemia is usually present, with proliferating B-cells 8 Chronic Myelocytic Leukemia 9 CML ► ► ► ► ► ► ► ► ► Also known as Chronic Granulocytic Leukemia (CGL) A clonal myeloproliferative disorder of hematopoietic pluripotent cell transformation characterized by marked leukocytosis and excessive production of granulocytes at all stages of maturation Is associated with chromosomal abnormality called Philadelphia Chromosome; 90-95% of patients with CML carry Philadelphia Chromosome, which is the joining of chromosomes 9 and 22 Usually occurs between ages of 30-50 (“adult leukemia”) CML accounts for 25% of all leukemia cases Often discovered accidentally during routine physical Mean survival is 3-4 years after diagnosis Most patients die from complications arising from blast cell crisis Only treatment is bone marrow transplant 10 CML ►A clonal stem cell disorder ► Causative agents include exposure to ionizing radiation, administration of cytotoxic drugs, and exposure to viruses ► Cause of CML is unknown in 95% of cases ► Not inherited; Appears to be acquired, and the Philadelphia Chromosome is not present in non-hematopoietic tissues 11 Philadelphia Chromosome in CML ► ► ► ► ► ► Philadelphia (Ph) chromosome found in neutrophil, monocyte, erythrocyte, platelet, and basophil precursors from CML patient’s blood and bone marrow Helps in defining translocation that produces Ph chromosome as clonal abnormality Specific notation is t(9;22) Main portion of the long arm of chromosome 22 is deleted and translocated to distal end of long arm of chromosome 9, and a small part of chromosome 9 reciprocally translocates to the broken end of chromosome 22 Provides subsequent progeny with growth advantage over normal cells Also, the expression of the anti-apoptosis gene, which is responsible for cell death, is altered 12 Laboratory Findings in CML Increased load of myeloid cells, often with WBC count over 100 x 109/L ► Will see all stages of maturation, from blasts to mature segs; However, segmented neutrophil and myelocyte are the most numerous forms; Will see left shift ► Eosinophil, basophil and platelet numbers may be increased ► Normochromic, normocytic anemia with Hgb usually < 10 g/dL ► Bone marrow hypercellular with marked myeloid hyperplasia (M:E ratio of 10:1, instead of the normal 3:1) ► Low to absent leukocyte alkaline phosphatase (LAP) ► 13