Unit 13 Investigation of a Positive DAT and Immune Hemolysis
advertisement

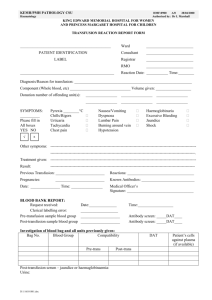
Unit 13 Investigation of a Positive DAT and Immune Hemolysis Terry Kotrla, MS, MT(ASCP)BB Significance of Positive DAT Positive Direct Antiglobulin Test (DAT) does NOT mean that RBCs will have shortened survival. Positive DAT without clinical problems occur in 1:1000-1:14,000 blood donors and 1-15% of hospital patients. IgG and C3d Coating of RBCs Healthy individuals can have 5-90 molecules if IgG/RBC and 5- 40 C3d/RBC, this is below threshold of detection. DAT can detect 100-500 IgG/RBC and 400-1100 C3d/RBC Causes of Positive DAT Autoantibodies Alloantibodies - HTR Passively acquired alloantibodies (plasma, derivatives) Maternal alloantibodies Nonspecifically adsorbed proteins or membrane modification. Drug induced antibodies. Antibodies produced by passenger lymphocytes Complement activation due to bacterial infection, autoantibodies or alloantibodies. Autocontrol versus DAT Autocontrol (AC) run as part of antibody work up and is not the same as DAT. Autocontrol treated like screen or panel cells. Add serum/plasma and enhancement reagent. Incubated and taken to AHG. May be positive due to testing procedure, may detect in-vitro sensitization If AC positive perform DAT, may be negative. DAT cells are taken directly to AHG, no adding of serum or enhancement, no incubation, detects IN-VIVO sensitization. DAT Test freshly washed cells with antiglobulin reagents (anti-IgG and/or anti-C3d) to detect IN-VIVO coated of RBCs. The 2 Fab sites on the antiglobulin molecule bind to the Fc portion of sensitizing antibody or complement on 2 adjacent RBCs, bridging gap and causing visible agglutination. Strength of agglutination proportional to amount of bound protein. Reasons for Performing DAT Screen for clinically unexpected autoimmune phenomena Detect early manifestation of immune response to recent transfusion. Assist in diagnosis of HDFN. Collection of Blood Sample To verify in-vivo sensitization EDTA sample should be used. EDTA sample will provide RBCs for elution if necessary. If cold hemagglutinin suspected keep sample at 37C. False Positive DAT Want to detect IN-VIVO sensitization not in-vitro. False positive most often associated with using refrigerated or clotted samples. Any positive obtained on clotted sample should be confirmed with EDTA sample. EDTA will be provide RBCs for elution if necessary. Patient History Crucial to investigation. Is there: History of recent transfusion. Administration of drugs previously associated with immune hemolysis. History of hematopoietic progenitor cell or organ transplantation. Administration of IVIG or IV anti-D. Serologic Investigation Perform DAT on RBCs with anti-IgG and anti-C3d to characterize protein(s) coating RBCs. Test serum/plasma to detect and identify clinically significant antibodies to red cell antigens, may have to distinguish autofrom allo-antibodies, if present. Prepare and test eluate from DAT positive RBCs to define whether coating protein has red cell antibody specificity. Eluate from complement only coated cells should be tested if clinical evidence of hemolysis. Concentrates IgG, if present, which may not be present in patient serum/plasma. Elution Removes antibody from sensitized RBCs and recovers antibody in usable form. Many types of elution procedures available, no single method is ideal in all situations. Thorough washing of the RBCs ESSENTIAL to ensure that antibody detected in eluate is only RBC bound antibody. Last wash will detect Elution (whenever DAT is positive) Elution techniques “free” antibodies from the sensitized red cells so that the antibodies can be identified Y Y Y Positive DAT Y Y Sensitized RBC Elution Frees antibody Antibody ID Once antibody is freed from RBC test against panel to ID. Anti-e Anti-e Anti-e Anti-e Anti-e e e e e e e Anti-e e Anti-e Anti-e eeAnti-e e ee eAnti-e Anti-e e e e Anti-e e Anti-e Anti-e e e e Anti-e Anti-e Anti-e e e ee e e e ee e e e e e e e e Further Studies No further testing if: No unexpected antibodies present in serum/plasma. Only autoantibody detected in eluate. No recent transfusion Confirm specificity of alloantibody if present. If DAT positive but serum/plasma and elution studies are negative suspect drug induced hemolysis – reference lab. If ABO incompatible components transfused test for anti-A and anti-B. If patient an infant perform appropriate testing on maternal sample and elution on cord cells. Immune Hemolysis Causes shortened RBC survival due to immune reaction. Diagnosis of hemolysis : H&H reticulocytes LDH haptoglobin bilirubin Hemoglobinemia and/or hemoglobinuria may indicate acute hemolysis. Classification Hemolytic Anemia Autoimmune Warm autoimmune hemolytic anemia (WAIHA) Cold agglutinin syndrome (CAS) Mixed type – both warm and cold autoantibodies present Paroxysmal cold hemoglobinuria (PCH) Alloimmune Hemolytic transfusion reaction Hemolytic disease of the fetus and newborn Drug induced Drug dependent Drug independent Warm Autoimmune Hemolytic Anemia (WAIHA) Most common type of AIHA and most difficult problem encountered in the transfusion service. DAT 67% of the cases, RBCs are coated with both IgG and complement. 20% of the cases, RBCs are coated with IgG alone. 3) 13% of the cases, RBCs are coated with complement alone. WAIHA Serum/Plasma testing May have little free autoantibody, may all be on RBCs Once all antigen sites coated, detectable Approximately 50% of WAIHA will have autoantibody reactive with ALL CELLS TESTED. DANGER – alloantibody may be present also Eluate Usually reactive with all cells tested. Negative reactions due to complement only OR presence of drug induced antibody WAIHA – Antibody Specificity May be very complex. Often initially directed against Rh antigen complex. Specificity against simple Rh or other blood group antigens occasionally seen. If simple specificity, give antigen negative, if high frequency or complex antibody, antigen negative not practical. WAIHA – Autoadsorption - MEMORIZE If patient NOT recently transfused perform WARM autoadsorption. If RBCs heavily coated may need to pretreat with ZZAP to remove Ig. Incubate patient serum/plasma with patient RBCs. Antibody directed against patient RBCs Incubate at 37C for 60 minutes Will attach and be removed from serum/plasma Separate (harvest) adsorbed serum/plasma Test adsorbed serum/plasma against screen cells. Negative – autoantibody only Negative AND positive reactions – alloantibody present perform panel on adsorbed serum and identify. All positive – procedure unsuccessful, repeat entire process with 1X adsorbed serum. Remove serum and test for alloantibody 2 tubes Wash x3 after incubation Centrifuge after incubating; and transfer serum to 2nd tube of treated cells; incubate and centrifuge again WAIHA Blood Bank Investigation Warm Autoadsorption To ensure that no alloantibodies are being masked by autoanibodies Remove plasma Patient plasma 37oC 1 hour ZZAP Repeat Spin Alloantibody Autoantibody Patient RBC DAT neg WAIHA – Transfusion Considerations Best to AVOID transfusing if possible. If transfusion essential give smallest volume of RBCs necessary to maintain oxygen transport. If allo- plus autoantibody present blood must be negative for antigen to which alloantibody is directed. Serologically compatible blood may not be found. Some facilities perform the following, be aware may lead to false sense of security. MUST prove presence/absence of alloantibodies first! Crossmatch with adsorbed serum. Perform electronic crossmatch. Crossmatch with serum/plasma and select those units which react the weakest. WAIHA Blood Bank Investigation Autoantibody may still be present Look for reaction strength patterns Issue “least incompatible” XM blood Recipient's plasma Donor's cells 1 Reaction wk 2 2+ 3 wk WAIHA – Transfusion Considerations Patients with no apparent hemolysis do quite well. Difficulty is with pretransfusion testing. Survival of transfused RBCs is about the same as the patient’s own RBCs. Patients with active hemolysis – challenging Transfused RBCs may be destroyed more rapidly. May increase hemoglobinemia and hemoglobinuria May cause DIC Transfusion is a clinical decision and should not be withheld due to serological incompatility. Cold Agglutinin Syndrome (CAS) Less common BUT most common type associated with cold reactive autoantibodies. Accounts for approximately 16% of immune hemolysis. Occurs as acute or chronic form. Acute secondary to lymphproliferative diseases or Mycoplasma pneumoniae infections. Chronic seen in elderly and may result in Raynaud’s phenomena and hemoglobinuria if exposed to extreme cold. Often characterized by RT agglutination of EDTA cells to the extent the sample appears clotted. Cold Agglutinin Syndrome (CAS) DAT - Only complement is detected on the RBCs Why is complement the only protein present? Antibody is IgM, which in-vivo binds to RBCs in peripheral circulation where temperature falls to 32C or less. IgM causes binding of complement in the cold. When RBCs return to warmer circulation IgM dissociates leaving RBCs coated with complement only. Eluate will be negative as only complement is binding to the RBC. Cold Agglutinin Syndrome (CAS) Serum/Plasma IgM reactive antibody associated with immune hemolysis react at > 30C and 60% have titers 1000> when tested at 4C. May show high thermal amplitude. Anti-I specificity, less commonly anti-i associated with IM. Antibody specificity NOT diagnostic as anti-I seen in healthy patients and rarely reacts at titers above 64. Pre-warmed testing may eliminate reactivity. May cause false positive forward and reverse typing Forward – cells so heavily coated spontaneously agglutinate. Reverse cells have I antigen and will agglutinate. CAS – Two Types of Autoadsorptions Rabbit Erythrocyte Stroma Test (REST) Cold auto adsorpiton Rabbit Erythrocyte Stroma Test (REST) For patients who have been recently transfused. Rabbit cells have I antigen. Procedure Incubate patient serum/plasma with rabbit stroma at 4C. I antibody absorbed out. Remove (harvest) serum/plasma Test absorbed serum against screen cells. Use with caution: may adsorb out clinically significant antibodies to D, E, Vel antigens and IgM antibodies regardless of specificity. Cold Autoadsorption Test CANNOT be performed on recently transfused patients. Collect EDTA sample, keep warm. Separate plasma from RBCs. Wash RBCs with warm saline. Add aliquot of plasma/serum to RBCs incubate at 4C for 1 hour. Harvest serum/plasma and test against screen cells. Negative – no alloantibody. Positive and negative – alloantibody present, run panel. All positive, unsuccessful, repeat with 1X adsorbed sample. CAIHA Blood Bank Investigation Cold Autoabsorption Spin Alloantibody autoantibody Supernatant used for IgM Warm saline Wash Spin Spin Incubate patient’s cell and serum @ 4oC Ab screen Reverse grouping cells Autocontrol Limitation: Will not remove a high titer cold agglutinin completely CAS – Transfusion Considerations Rarely require transfusion. Use prewarmed technique for compatibility tests or use cold autoadsorbed serum. Transfuse blood through blood warmer. Warm versus Cold Autoantibodies WARM Reacts at 37C COLD Reacts at RT or below Broad antibody specificity Titer > 1000 IgG and C3d coating RBCs Complement only coating RBCs Insidious to acute Anti-I most common Anemia severe Fever, jaundice frequent Intravascular not common Splenomegaly Hematomegaly Adenopathy Use great caution when transfusing. Often chronic anemia 9-12 g/dL (less severe) Autoagglutination Hemoglobinuria, acrocyanosis and raynaud’s with cold exposure No organomegaly Transfusion well tolerated, use blood warmer Mixed Type Autoantibodies One-third of patients with WAIHA have nonpathologic IgM antibodies reactive at RT Further divided Patients with high-titer, high thermal amplitude IgM Patients with normal titer (<64), high thermal amplitude IgM Often present with hemolysis and complex serum reactivity present in all phases of the testing. DAT Both IgG and C3d detectable. IgG due to warm autoantibody. C3d bound due to IgM autoantibody Mixed Type Autoantibodies Serum/Plasma Cold – can have anti-I or-i, but often has no specificity Warm – serologically indistinguishable from WAIHA Eluate activity indistinguishable from WAIHA. Adsorptions – may be necessary to perform at both 37C and 4C. Transfusion considerations identical to those described for WAIHA. Paroxysmal Cold Hemoglobinuria (PCH) DIFFERENT from Paroxysmal Nocturnal Hemoglobinuria in which hemolysis is caused by acid produced during sleep. RAREST form of DAT positive AIHA. Presents as acute transient condition secondary to viral infections particularly in young children. Caused by a biphasic hemolysin which induces hemolysis after exposure to cold. Results in hemoglobinuria and hemoglobinemia. PCH – DAT and Eluate DAT Autoantibody is IgG which acts as cold agglutinin. IgG binds to RBCs in colder parts of body. Causes complement to be bound irreversibly. IgG elutes off of RBCs in warmer parts of the body. ONLY COMPLEMENT is detected. Eluate Since only complement coats cells eluate is negative. Antibody specificity Anti-P Not necessary to transfuse rare P negative blood. PCH – Serum/Plasma Testing Autoantibody described as “biphasic hemolysin”. Binds to RBCs at low temperatures. Binds complement. As cells warm up hemolysis occurs. Basis of Donath-Landsteiner test. Donath-Landsteiner Usually add fresh complement Antibody binds at cold temperatures Test is warmed to 37C. As warming occurs complement is activated and lysis of RBCs occurs. Donath Landsteiner Test 30’@4ºC 60’@37 ºC 90’@4 ºC 90’@37 ºC Patient Serum + - - Patient Serum + - - - - - Normal fresh serum Normal Fresh PCH – Donath Landsteiner Test Drug Induced Hemolytic Anemia VERY RARE - 1 in a million chance. May induce formation of antibodies either against the drug or red cell antigens. Drugs may act as haptens once firmly bound to RBC. Four theoretical mechanisms Drug adsorption Immune complex formation Autoantibody production Non-specific protein adsorption NOTE: Newest edition of Technical Manual mentions the following categories but also categorizes by activity. Most references still contain the categories listed above. Drug Adsorption Approximately 3% of patients receiving large dose IV penicillin will develop positive DAT. Less than 5% of these will develop hemolytic anemia. Mechanism Drug adsorbed onto RBC in-vivo, becomes a hapten. If patient develops antibodies to penicillin they will bind to penicillin on RBC. Hemolysis occurs extravascularly. Drug Adsorption – Lab Features DAT strongly positive due to IgG coating. Serum/Plasma Antibody screen negative unless alloantibodies coincidentally present. High titer IgG penicillin antibodies present will only react with drug coated RBCs in-vitro. Eluate reactive with drug coated RBCs only – reference lab. Hemolysis is subacute at onset but may become life- threatening if not recognized in time. Discontinue penicillin. Immune Complex Formation Drug binds with antibody in-vivo, in the plasma. Immune drug-antibody complex binds to RBC and initiates complement activation. Leads to INTRAVASCULAR hemolysis. After RBC hemolyzed drug-antibody complex dissociates and attaches to new RBC. Small amounts of drug can results in acute hemolysis. Piperacillin (synthetic penicillin), second and third generation cephalosporins and anti-ceftriaxone have been implicated. Immune Complex Formation DAT – only complement is present on RBCs. Serum/Plasma Antibody screen negative unless alloantibody present. Test serum against RBCs in presence of drug, may cause sensitization, agglutination or hemolysis Eluate – negative, since only complement is coating the RBCs. Autoantibody Production Serological findings indistinguishable from those associated with WAIHA. First case was alpha methyldopa, L-dopa has also been implicated as well as other drugs closely related to alpha methyldopa. Autoantibody Production DAT is Positive in approximately 15% of patients receiving alpha methyldopa. Only 0.5 - 1.0% of patients taking alpha-methyldopa develop hemolytic anemia. RBCs are usually coated only with IgG, but occasionally weak complement coating is also present. DAT usually becomes positive only after 3-6 months of therapy. Development of a positive DAT is dose-dependent; approximately 36% of patients taking 3 g of the drug daily develop a positive DAT compared with 11% of patients receiving 1 g per day. Strength of the positive DAT becomes progressively weaker once alphamethyldopa therapy is discontinued. May take from 1 month to 2 years. Patients with hemolytic anemia due to alpha-methyldopa therapy improve within the first week or so after drug therapy discontinued. Autoantibody Production Serum/Plasma – reactive with all cells tested. Eluate reactive with all cells tested. KEY IS HISTORY – patient taking medication known to cause autoantibody production. Laboratory Investigation When patient has positive DAT history MUST include medications. Perform DAT to classify coating protein. Perform elution if IgG coating detected. Test patient serum/plasma for unexpected antibodies. If drug antibodies suspected send to reference lab. Reference lab has ability to coat cells with drug and/or introduce drug into test system. References http://www.nzma.org.nz/journal/122-1301/3749/ AABB Technical Manual 16th edition, 2008 End of Unit 13