NEW PATIENT ASTHMA/ALLERGY Past Medical History Date
advertisement

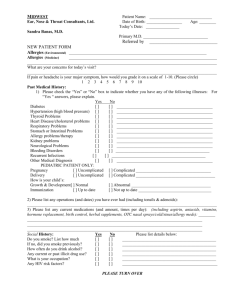
NEW PATIENT ASTHMA/ALLERGY Past Medical History Date Comment Past Surgical History/Hospitalizations Date Comments Medications Allergies FAMILY HISTORY Problem Relation Name Comments Social History Tobacco Use Alcohol Use Drug Use Y/N Marital Status S/M/D/W Y/N Spouse Name Y/N # of children Sexual Activity Y/N Years of Education Occupation ADULT Environmental History Type of home Type of Heating and cooling Where is the carpet in the home Pets Smokers in house Allergy Proof bed Pillow type House Central Bedroom Dog Yes Yes Cotton Apartment Window unit Whole house Cat No no Feather Condo Living space Bird Modular Home none Reptile Mouse Rat None Foam Review of System Eyes itching Eyes discharge Eyes Redness Eyes Swelling Glasses/Contacts Ear pain Ear Drainage Ear Swelling Ear Infection Nasal Congestion Nose Bleeds Nasal itching Drainage Yes Y Y Clear Colored Y Y Y Y Y Clear Colored Y Y Y Clear Colored Y Y Clear Colored Y N Nasal Sneezing Headaches Sore Throat Throat swelling Throat redness Hoarseness Throat Itching Tongue Swelling Chest Pain Palpitations High Blood Pressure Swelling in hands or feet Difficulty Lying flat Cough Sputum/Mucous Wheezing Shortness of Breath Chest Tightness Change in appetite Nausea Vomiting Indigestion Sour Taste Diarrhea Constipation Acne Hives Skin Itching Skin Dryness Skin Redness Moles Rash Scaly skin Diabetes Thyroid problems Cold or heat intolerance Excessive Thirst Fever/Chills/Sweats/Diarrhea/Fatigue/Weight loss Y No N N N N N N N N N N N N Clear Colored Comments Y N Throat Y Y Y Y Y Y Y Y Y Y Y Y Y Y Clear Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Colored N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N N If yes, please circle