Unit 7 Hematology System Group D (Meg, Kristy, Marla and Carol)
advertisement
")
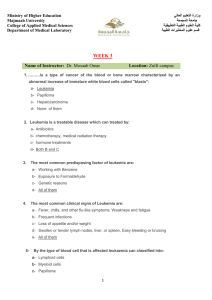
Unit 7 Hematology System Group D (Meg, Kristy, Marla and Carol) Mr. D. presents to you with fatigue. He had surgery for obesity about 1 year ago that involved bypassing part of his stomach and he has done well controlling his weight since then. He has also been on a prescription "antacid" for about 9 months. After your investigations, you find that Mr. D. is anemic. What are the major etiologies of acute and chronic leukemia and what is the major pathologic deficiency in these diseases? (Group D) Answer the above two questions (major etiologies and presentations) for platelet disorders: thrombocytopenia presentation (Group D) Leukemia: Leukemia is a "clonal malignant disorder of the blood..." and primarily it is a disorder of the bone marrow (Mansen & McCance, 2006). Thus leukemia leads to an accumulation of dysfunctional cells. Leukemia affects white blood cells; the form of leukemia depends upon the type of white cells affected i.e. lymphoid or myeloid (Canadian Cancer Society, 2006). There are four main types of leukemia’s which, are broken down into two groups acute or chronic (Medline Plus, 2007; Wikipedia, 2008). Acute leukemia’s are either acute lymphocytic (Mansen & McCance, 2006) or lymphoblastic leukemia (ALL) and acute myeloid or myelogenous leukemia (AML). Chronic leukemias are either chronic myelogenous leukemia (CML) or chronic lymphocytic leukemia (CLL) (Mansen & McCance, 2006; Wikipedia, 2008). Acute Leukemia: The most common types of acute leukemia are acute lymphocytic or lymphoblastic leukemia (ALL) and acute myeloid or myelogenous leukemia (AML)(Medline Plus, 2007). AML is the "excessive number of immature myeloid cells in the blood and bone marrow" (McCance & Huether, 2006 p. 1681). AML are the most common type of leukemia among adults over the age of 40 and usually developing around 65 (Medline Plus, 2007). ALL is the "excessive production and continuous multiplication of malignant and immature white blood cells in the bone marrow" (McCance & Huether, 2006 p. 1681). ALL is commonly seen in children under the age of 10. The onset of ALL and AML is rapid and the blast cells are usually either immature or undifferentiated (McCance & Huether, 2006). Prognosis for ALL is better in children less than 5 years of age and worsens in adults to an average 64.8% survival rate (Mansen & McCance, 2006). Etiology: The direct cause of acute leukemia is unknown but several things have been linked to the onset (Medline Plus, 2007). Possible causes of both AML and ALL Radiation exposure Age - some types are more common in children and others more common in adults Chemicals (benzene and alkylating agents) Medications (chemotherapy, etoposide and immunosuppressant) Blood disorders (polycythemia, thrombocythemia and myelodyplasia) (Canadian Cancer Society, 2006; Mansen & McCance, 2006; Medline Plus, 2007). Possible Causes of AML Genetics may predispose an individual for example, Down syndrome Fanconi aplastic anemia, Bloom syndrone, ataxiatelangiectasis, trisomy 13, Patau Syndrome, Wiskott-Aldrich syndrome and agammaglobulinemia Risk increases with age and reaches a peak at about age 60 years (Canadian Cancer Society, 2006; Mansen & McCance, 2006) Possible Causes of ALL Life-style Environmental factors (Mansen & McCance, 2006; Medline Plus, 2006). Major Pathology Deficiency: The deficiency of normally functioning mature hematopoietic cells (source for all blood cells) is a major cause of mortality and morbidity relating to acute leukemia, rather than the number of malignant cells in circulation. Acute leukemia begins with a mature hematopoietic cell that transforms and becomes incapable of normal differentiation, lacks the property of apoptosis, and does not respond to normal growth regulation or constraints; producing many abnormal (malignant) blood cells (Weinblatt, 2007). These transformed hematopoietic cells compete with normal hematopoietic cell function. Bone marrow and blood have increasing leukocyte and blast cell presence which replace normal erythrocytes, megakaryocytes (source of platelets), and myelocytes (source of neutrophils) (Mansen & McCance, 2006). Presentation: Common Signs and Symptoms for both ALL and AML: Fatigue (caused by bone marrow depression and anemia). Bleeding bruising and Disseminated Intravascular Coagulation (DIC) (caused by decreased platelet production) Persistent fevers and infections (caused by decreased available normal leukocytes) Anorexia and weight loss (caused by changes is taste and swallowing difficulties from oral infections) Bone and joint pain Elevated uric acid (increased protein catabolism) Anemia Pallor Pinpoint red rash (petechiae) Shortness of breath with exertion Loss of appetite and weight loss (Mansen & McCance, 2006; Medline Plus, 2007) Unique Signs and Symptoms of ALL Liver, spleen and lymph node enlargement. Joint pain Infection Palpitations Infected gums (Canadian Cancer Society, 2006; Medline Plus, 2007) Unique Signs and Symptoms of AML: Typically no symptoms Early signs are rare and similar to flu like symptoms Tumor development outside the bone marrow (chloroma) (Medline Plus, 2007) Chronic Leukemia: There are two types of chronic leukemia: chronic myelogenous leukemia (CML) and chronic lymphocytic leukemia (CLL) (Medline Plus, 2006) . In CLL, the main problem is a failure of the B cells to mature. However, occasionally T cells will be associated with CLL when they are overproduced in the bone marrow (Mansen & McCance, 2006). CML is an overproduction of myeloid cells in the bone marrow which is caused by the Philadelphia chromosome (Mansen & McCance, 2006). The onset of CML and CLL is gradual and cells are mature but function abnormally. Survival rate of CML is 36.7% overall which is almost twice that of ALL (Mansen & McCance, 2006). Etiology: CLL: Damage to the DNA of cells in the bone marrow causes CLL. Oncogenes may be turned on or tumor suppressor genes may be turned off. In some cases the affected person has an extra chromosome or another chromosome abnormality. The changes in the genes cause the bone marrow to produce faulty lymphocytes. These lymphocytes interfere with normal blood cell production, and accumulate in the blood and some organs. Some insecticides and pesticides may be associated with increased risk of developing CLL. CLL tends to affect older adults. (Mayo Clinic, 2008) CML: The cause of CML is unknown, but is believed to be associated with exposure to ionizing radiation, as it is seen in those who have suffered exposure to the atomic bombs of Hiroshima and Nagasaki. Another source that is being studied is the chemical benzene (Besa & Woermann, 2006; Medline Plus, 2007). Major Pathology Deficiency: Chronic leukemia’s are progressive and insidious. The key problem with chronic leukemia is that the cells are mature but do not function as they should (Mansen & McCance, 2006). This leads to a decreased number of functioning B-cells and therefore an inability to produce antibodies. Leukemic cells build up in the bone marrow, but don't interfere with the production of other blood cells, interfering only with the maturation cycle of the B-lymphocytes and suppressing the humoral immunity of the host (Mansen & McCance, 2006). Presentation: Signs and symptoms of CLL: fever weight loss decreased appetite, night sweats, lethargy & fatigue - particularly with physical activity. bone & joint pain, swollen liver & spleen and lymph node enlargement. (Mayo Clinic, 2008; Medline Plus, 2007) Signs and symptoms of CML depend on the phase the disease is at: The chronic phase little to no signs or symptoms for several months to years The accelerated phase fever bone pain swollen spleen and pressure under left lower ribs weakness The blast crisis phase high count of immature white blood cells (leukemia cells) bleeding and infection bone marrow failure. pinpoint red rash (petechiae). (Medline Plus, 2007) Thrombocytopenia: Thrombocytopenia is defined as a platelet count of less then 100,000. A normal platelet count is from 150,000 to 400,000 UL (mean 250,000 UL). A low platelet count increases the risk of bleeding; the lower the count, the higher the risk. Platelets are the basic element of blood that promotes coagulation (clotting). (LeFever Kee, 2001). Low platelet counts can be from either an increase in destruction or a decrease in production of platelets (Mayo Clinic, 2008; Medline Plus, 2006). Etiology: Decreased Production of Platelets: Aplastic anemia Bone marrow cancers Bone infections Medications Vitamin deficiency (B12 or folic acid) Sepsis Genetic syndromes (Fanconi anemia, Grey platelet syndrome and Alport syndrome) Liver failure (inability to produce thrombopoietin) Leukemia Pregnancy (due to increased blood volume) (Mayo Clinic, 2008; Medline Plus, 2006) Increased Destruction of Platelets: Immune thrombocytopenic purpura (ITP) Immune thrombocytopenia Non-immune thrombocytopenia Thrombotic thrombocytopenic purpura Disseminated intravascular coagulation (DIC) Hypersplenism Post transfusion purpura Systemic lupus erythematosus (Mayo Clinic, 2008; Medline Plus, 2006) Presentation: Unexplained bruising Bleeding seen in mouth or nose Red pinpoint rash (petechiae) usually seen on lower legs Gastrointestinal bleeding problems (blood in urine or stools) Intracranial hemorrhage Prolonged bleeding from cuts Unusually heavy menstrual flows (Mayo Clinic, 2008; Medline Plus, 2006) References: Besa, E. & Woermann, U. (2006). Chronic myelogenous leukemia. Emedicine. Accessed online June 17, 2008 from http://www.emedicine.com/med/topic371.htm#section~author_information Canadian Cancer Society. (2006, January). What is leukemia? Accessed June 16, 2008 from http://www.cancer.ca/ccs/internet/standard/0,3182,3225_10175_273209_langId-en,00.html Canadian Cancer Society. (2006, January). Causes of leukemia. Accessed June 16, 2008 from http://www.cancer.ca/ccs/internet/standard/0,3182,3225_10175_272824_langId-en,00.html Canadian Cancer Society. (2006) Leukemia-acute lymphoblastic (ALL). Retrieved June 17, 2008 from http://info.cancer.ca/E/CCE/cceexplorer.asp?tocid=64 LeFever Kee, J. (2001). Handbook of laboratory and diagnostic tests with nursing implications (4th ed.). Upper Saddle River, NJ: Prentice Hall. Mansen, T. J. & McCance, K. L. (2006). Alterations of leukocyte, lymphoid, and hemostatic function. In K. L. McCance & S. E. Huether (Eds.), Pathophysiology: The biologic basis for disease in adults and children (5th ed., pp. 955-995). St. Louis, MI: Elsevier Mosby. Mayo Clinic. (n.d.). Chronic myelogenous leukemia. Accessed June 16, 2008 from http://www.mayoclinic.com/health/chronic-myelogenous-leukemia/DS00564/DSECTION=3 Mayo Clinic. (2008). Chronic lymphocytic leukemia. Retrieved June 14, 2008 from http://www.mayoclinic.com/health/chronic-lymphocytic-leukemia/DS00565/DSECTION=1 Mayo Clinic.(Feb 22, 2008). Diseases and Conditions: Thrombocytopenia (low platelet count). Retrieved June 15, 2008 from http://www.mayoclinic.com/health/thrombocytopenia/DS00691/DSECTION=3 McCance, K. L. & Huether, S. E. (2006). Glossary. In K. L. McCance & S. E. Huether (Eds.), Pathophysiology: The biologic basis for disease in adults and children (5th ed., pp. 1681-1710). St. Louis, MI: Elsevier Mosby. Medline Plus. (2006, April 27). Thrombcytopenia. Retrieved June 15, 2008 from http://www.nlm.nih.gov/medlineplus/ency/article/000586.htm Medline Plus. (2006, September 11). Chronic Myelogenous Leukemia. Retrieved June 17, 2008 from http://www.nlm.nih.gov/medlineplus/ency/article/000570.htm Medline Plus. (2006, September 11). Chronic Lymphocytic Leukemia. Retrieved June 17, 2008 from http://www.nlm.nih.gov/medlineplus/ency/article/000532.htm Medline Plus. (2007, March). Leukemia. Retrieved June 17, 2008 from http://www.nlm.nih.gov/medlineplus/ency/article/001299.htm Medline Plus. (2007, April 1). Acute Myeloid Leukemia. Retrieved June 14, 2008 from http://www.nlm.nih.gov/medlineplus/ency/article/000542.htm Medline Plus. (2007, April 27). Acute Lymphocytic Leukemia. Retrieved June 15, 2008 from http://www.nlm.nih.gov/medlineplus/ency/article/000541.htm Weinblatt, M. E. (2007). Acute Myelocytic Leukemia. Emedicine. (Eds. Sakamoto, K, Windle, M., Cripe, T, Gross, S., & Arceci, R.). Accessed online June 14, 2008 from http://www.emedicine.com/ped/fulltopic/topic1301.htm#section~Introduction Wikipedia (June 14, 2008). Leukemia. Retrieved June 17, 2008 from http://en.wikipedia.org/wiki/Leukemi