1.0. DISEASE SURVEILLANCE – AND EWARN

WHO SOUTHERN SUDAN
HEALTH UPDATE
September 2001
HIGHLIGHTS
Surveillance program enlists support of Veterinary workers.
EWARN strategy reviewed by external experts
An unusual “nodding disease investigated in Mundri’
TB strategy developed for southern Sudan
Polio eradication in south Sudan on course with global targets.
1.0. DISEASE SURVEILLANCE –
AND EWARN
1.1.1.
EWARN orientation extends to veterinary health workers and remote areas
WHO, in collaboration with VSF-B and
GOAL/Ireland conducted an orientation for a total of
48 participants, including veterinary health workers on outbreak diseases Early Warning and Response
Network. These participants were from EQA, BGZ,
UNL and SBN.
Community-level NGO staff can support
EWARN in remote areas
The orientations were aimed at improving awareness on when to suspect disease outbreaks, how and when to support timely reporting, investigation and response. This extension is expected to improve timely detection, reporting, and awareness on suspected outbreaks, which are either not detected or often reported late among remote communities with no access to health NGOs.
1.1.2.
Consultation to strengthen EWARN with
Counties
Consultation was held at Maridi County Health department on ways of improving the local EWARN team. At present any suspected disease outbreak is reported to the county through the PHCUs. Most
PHCUs have community health workers who directly report to Health Centers and from there to County
Health Department. When required, the CHD and its team support investigation and response. It was agreed to give training to the Team to improve timely detection, reporting, and investigation and response.
Similarly, a total of 36 participants at Rumbek discussed on the roles of WHO in health services.
Among these were support to strengthen laboratories, enhancing EWARN, and local capacity building for detection and responding to outbreaks.
Preliminary investigation guidelines, case definitions, and weekly surveillance formats were discussed.
Participants were urged to continue to strengthen
EWARN by improving awareness among community health workers and village health committees, and by strengthening Payam (sub-district) level EWARN teams.
1
1.2.
EWARN reviewed by experts
A team from WHO HQ, and WHO south Sudan office conducted field assessment and review of the
EWARN program which has been in operation for almost one and a half years now. The team held consultations with partners at Nairobi, Loki, and in southern Sudan with partners, program coordinators and EWARN team members. Activity plans, performances, outcomes, and field reports were reviewed. Field and facility visits were conducted.
Discussions with EWARN Teams (Yambio) and local partners, including SRRA and county health departments (Maridi and Yambio), were conducted to complement field visits and activity reports.
The mission observed encouraging progress and suggested ways of further strengthening local
EWARN. Considering difficult access in southern
Sudan, strengthening of county-level EWARN teams is appropriate for timely reporting and responding to outbreaks of diseases. The county EWARN team members are convinced that it is possible to detect, report, investigate and respond to common disease outbreaks occurring in their county. They cited examples of their experiences by comparing to previous years. According to one observant
“ building local EWARN is feasible and has reduced considerably the need for expensive and often late deployment of external investigation and response teams
”. The supervision and technical support is essential to enhance capacity building efforts. It was observed that local partners are motivated to participate in strengthening EWARN activities.
Communication, shortage of essential drugs and supplies, inadequate number and mix of local health workers were identified challenges.
Based on the observations, it was agreed to continue training, and orientation of health workers, establishing of EWARN teams in all strategic locations and to continue supervision and follow-up.
Similarly, ways of improving timely detection and reporting of outbreaks to support EWARN teams are recommended.
1.2.1 Unusual ‘nodding disease ‘ investigated
A mysterious disease characterized by nodding and progressive mental disorientation affecting children was reported to WHO in August. Preliminary investigations with Samaritan Purse, Oxfam and
Malteser confirmed these reports. Two WHO experts joined the investigation this month and confirmed that over 200 children had been affected by this condition which seemed to affect children between 2-15 years.
This condition seems to have stated and continued undetected since 1994. Samples have been collected from those affected and a more in depth investigation has been launched.
1.3. Outbreaks Forecasting, Preparedness
Verification/Response
1.3.1.
Forecasting and Preparedness
Weekly monitoring of selected outbreak–prone diseases in Kapoeta (at Narus by SMC) for August and September, shows that there are no indications suggesting outbreaks. Service data, and key informants for any rumors of suspected outbreaks at community-level are on use.
WHO and AMREF, and on experiences from all health NGOs and partners who were involved in
EWARN activities, briefed the quarterly health coordination meeting at Nairobi on likely outbreaks, challenges, and areas of collaboration. It was emphasized that AMREF, through WHO, will continue to provide laboratory services to strengthen outbreaks detection and response.
1.3.2. Outbreak verification and Response
A total of two suspected outbreaks were reported and responded to. NCA at Alek, Bahr El Ghazal region, reported ARI among 17 under two children, with five reported deaths. All presented with shortness of breath, mild fever and cough. Case management was done with a diagnosis of RSV bronchiolitis. A measles outbreak was reported and investigated by MSF-B at
Midel in Bahr El Ghazal region.
1. 4. WHO TB experts recommend DOTS in south
Sudan
A three-persons TB mission conducted an in-depth evaluation of TB activities in south Sudan in
September. The findings of the mission, among others, include:
Different regimens are on use, the 6 months
(2HRZE/4HR) is considered appropriate and is in use in 2 facilities;
Fairly well equipped laboratories are present in all facilities with TB programs BUT with poorly trained staff.
NGOs provide drugs, but high cost limits expansion of services; and
The need for training and specific training in
TB was identified as high priority.
WHO will support the implementation of these recommendations.
2
2.
POLIO ERADICATION
2.1 Acute Flaccid Paralysis (AFP) surveillance summary for southern Sudan, How are we doing?
The table below summarizes our indicators.
1998 1999 2000 2001
----------------------------------------------------
Number of AFP cases investigated 8 31 59 53
Number of clinically confirmed polio cases 6 17 23 11
Number of confirmed cases with isolation
of wild poliovirus 0 1 0 1
Number of discarded polio cases
(i.e. non-polio AFP) 2 13 36 24
Number of cases pending classification 0 0 0 17
Annual non-polio AFP rate in children
<15 years (includes pending classification) 1 (0.04) 11 (0.46) 36 (1.21) 41 (1.86)*
AFP cases with 2 stool specimens collected
<= 14 days since paralysis onset
and at least 1 day apart (adequate specs) 1 ( 13%) 13 ( 42%) 23 ( 39%) 23 ( 43%)**
AFP cases with inadequate specimens
receiving a follow-up exam at least
60 days after paralysis onset 7 (100%) 17 ( 94%) 33 ( 92%) 16 (
53%)**
Cases with stool specimens arriving at
laboratory <= 3 days after collection 4 ( 50%) 7 ( 23%) 8 ( 14%) 10 (
23%)**
Cases with stool specimens arriving in
good condition 8 (100%) 31 (100%) 59 (100%) 43 (
98%)**
Cases with stool specimens with laboratory
results <= 28 days after specimen receipt 8 (100%) 30 ( 97%) 56 ( 95%) 40 (
91%)**
Cases with stool specimens from which
non-polio enteroviruses (NPEV) isolated 1 ( 13%) 3 ( 10%) 10 ( 17%) 6 ( 14%)***
*Target = 1.00
**Target = 80%
Despite wet and rainy conditions, a mopping-up campaign was implemented in Ruweng County, Upper Nile in response to the isolation of wild P1 poliovirus from a two year old girl. As per previous reports, in early May a
MedAir mobile team investigated this case. A stool specimen was sent to the WHO office in Loki for further investigation. Subsequently, wild P1 poliovirus was isolated from the stool specimen, confirming the ongoing circulation of poliovirus in Ruweng County. In response to this information a team of 9 WHO polio eradication staff went on ground in Ruweng County in August to conduct a more detailed epidemiological investigation of the index case and plan a mopping-up campaign. A similar investigation was also organized from the GOS side and results of these investigations shared. The epidemiological investigations were greatly hampered by the fighting that was going on in the area between the SPLA and the GOS. A process of negotiation of corridors of tranquillity was also initiated through top UNICEF and WHO leadership.
The mopping-up campaign originally scheduled for 27-30 August in order to synchronize with a similar campaign by the GOS was delayed due to inaccessibility to Ruweng County caused by flooding and insecurity.
The campaign was conducted from 2-5 September after obtaining assurances and clearances from both sides of
3
the conflict. One new Polio County Supervisor, 4 new Polio Field Assistants, 106 vaccinators, 26 team supervisors, 15 independent supervisors and 12 social mobilizers were trained and 8,893 under 5 years children were immunized. In addition, 6,402 doses of vitamin A were administered to children 6-59 months. Two additional rounds will be implemented in October and November 2001.
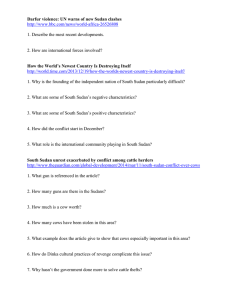
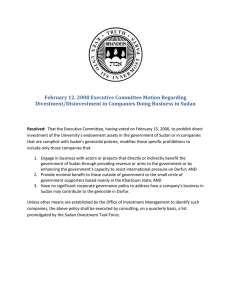
2.3 Global Overview of Progress towards Polio Eradication WHERE DO WE STAND?
The map and graph below show the number of wild polioviruses isolated globally from May 2000 to May
2001. It is encouraging to note that the global number of wild viruses in 2001 is less than 100 (with only 8 endemic countries) as of 1 October 2001. Only 59 cases with wild poliovirus have been identified in the
WHO Eastern Mediterranean Region. From this analysis, southern Sudan is on course to interrupt transmission by 2002.
NB as of 1st October 2001. The one case from Sudan is the one detected in
Ruweng.
NIDs and SNIDs 2001 Dates
Bahr el Ghazal/Lakes
1
st
Round:
15-18 October 2001
2
nd
Round
12-15 November 2001
Upper Nile/Jonglei/Equatorias
1
st
Round:
22-25 October 2001
2
nd
Round:
19-22 November 2001
4
5