Unusual association of diseases/symptoms
advertisement

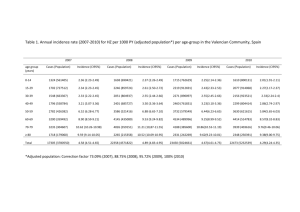
Published 28 April 2009 Cite this as: BMJ Case Reports 2009 [doi:10.1136/bcr.07.2008.0525] Copyright © 2009 by the BMJ Publishing Group Ltd. Unusual association of diseases/symptoms Reactivation of herpes zoster along the trigeminal nerve with intractable pain after facial trauma: a case report and literature review K-C Lin1, Che-Chuan Wang2, Kai-Yuan Wang3, Yi-Chen Liao4 and Jinn-Rung Kuo2 1 Chi-Mei Medical Center, Neurology, 901, Jong-Hwa Rd, Tainan, 710, Taiwan 2 Chi-Mei Medical Center, Neurosurgery, 901, Jong-Hwa Rd, Tainan, 710, Taiwan 3 Chi-Mei Medical Center, Emergency Medicine, 901, Jong-Hwa Rd, Tainan, 710, Taiwan 4 Chi-Mei Medical Center, Dermatologist, 901, Jong-Hwa Rd, Tainan, 710, Taiwan Correspondence to: Jinn-Rung Kuo, cmh7520@mail.chimei.org.tw SUMMARY We report the rare occurrence of herpes zoster reactivation after facial trauma. Herpes zoster appeared in painful groups of distended vesicles containing clear fluid on an erythematous base within the secondary division of the trigeminal nerve. The patient was treated with acyclovir (intravenous, 250 mg, every 8 hours) combined with topical steroids and anti-neuropathic pain medication. The zoster-associated neuralgia subsided gradually 1.5 months after diagnosis. We illustrate this unique case to highlight the fact that reactivation of the varicella zoster virus from childhood chicken pox can reappear at a traumatic site in late adulthood. BACKGROUND This case presenting with mixed facial bony fracture associated with neuropathic pain related to secondary herpes zoster reactivation is rare. The zoster associated neuropathic pain on the traumatic site is often misdiagnosed as tissue injury with nociceptive pain. The early diagnosis and prompt treatment of zoster-related symptoms/signs with antiviral treatment or anti-neuropathic medications will have better outcomes and less sequels of developing intolerable post-herpetic neuralgia. CASE PRESENTATION A 54-year-old male patient with facial abrasions was sent to our emergency room (ER) because of a motorcycle accident. The initial examination at the ER showed his blood pressure was 140/90 mmHg, pulse 78 beats/minute, body temperature 36.8 °C and random blood sugar level of 158 mg. The patient had a contusion swelling on the right cheek with tenderness. The neurological examination did not reveal any abnormalities. He received brain CT (fig 1), and a right maxillary bony fracture and bilateral maxillary sinus blood accumulation were shown. Tracing his past medical history, chicken pox in early childhood, herpes zoster in the right thoracic area at the age of 20, diabetes mellitus for 2 years with regular medication control and squamous cell carcinoma in the left cheek with surgical removal and radiation therapy for 6 weeks was noted. The patient received palliative treatment and was discharged 10 days later with facial swelling and local tenderness remaining. Unfortunately, he returned to the ER due to severe sharp and lightening pain over the right part of his face and teeth on the 17th day after the accident. The pain lasted for 1–2 minutes and recurred intermittently, even making it difficult for him to open his mouth due to the severe pain (visual analogue scale=10). A swollen cheek with erythematous change was noted. The patient had used ice packing to relieve the pain, but in vain. He was given cephazolin sodium (intravenous form, 1 g, every 8 hours) for possible secondary infection. On the 20th day, multiple vesicles appeared along the dermatome of the trigeminal V2 branch without eye or corneal involvement (fig 2). The reactivation of herpes zoster with neuropathic pain was impressed and the antibiotic was switched to acyclovir (intravenous form, 250 mg, every 8 hours) combined with a topical rinderon VA cream (0.06%) and lidocaine jelly (2%) for 7 days. Anti-neuropathic drugs were tried, with gabapentin being effective with a titrated dose from 300 mg to 900 mg. He was discharged with antiviral treatment for another 5 days. The vesicles subsided gradually (fig 3) although the neuropathic pain still occurred off and on. The pain finally diminished 1.5 months after the traumatic event. INVESTIGATIONS Observational case report. DIFFERENTIAL DIAGNOSIS Allergic skin reaction; traumatic inflammatory pain. TREATMENT Anti-viral, steroids and anti-neuropathic medications. OUTCOME AND FOLLOW-UP Good outcomes on early diagnosis and proper treatment. DISCUSSION Reactivation of latent varicella zoster virus (herpes zoster or shingles) is a painful, cutaneous eruption, dermatomal in distribution, and is associated with the risk of dissemination. The risk factors include advanced age, diabetes mellitus, malignancy, HIV infections, organ transplantation, immunodeficiency, and treatment with immunosuppressive medications1–3 have been mentioned on some occasions. Case reports and case series depict that mechanical trauma can precipitate herpes zoster eruptions at sites of traumatised dermatomes following liver biopsy,4 cryosurgery,5,6 intubation,7 axillary nerve block,8 spinal surgery,9 massage,10 orofacial surgery,11,12 and after thoracic sympathectomy for hyperhidrosis.13 Herpes zoster is the result of reactivation of the latent varicella zoster virus following poor immunity in the host. In the ganglia latency phase, the varicella zoster virus travels by centripetal axonal transport through the sensory nerve fibres of the skin and mucous membranes to the spinal and cranial ganglia and remains latent there for years. The thoracic and trigeminal nerve ganglia are most commonly affected. In certain conditions, the reactivated virus travels over the axon centrifugally to the dermatome corresponding to its ganglion of origin producing the typical dermatomal rash of shingles. This phenomenon implies that recurrence of the herpes zoster can happen at different ages and in different locations in the same person as verified in our patient. Our patient had a history of chicken pox in childhood, reactivated herpes zoster in the thoracic wall when he was 20 and the current reactivation of herpes zoster in the trigeminal nerve. Several precipitating factors for shingles have been reported.1–13 The cause of herpes zoster in our patient was most likely multifactorial, including his diabetic condition, skin cancer history and recent trauma. The zoster occurred after facial trauma and at the site of the trigeminal nerve of the secondary branch corresponding to the reactivation of zoster-related symptoms. The mechanism by which trauma might reactivate the zoster virus is unknown, but reflex irritation and hyperaemia of ganglions have been proposed.9 In 2004, Thoms et al14 reported that a recent trauma was associated with an adjusted 12-fold increased risk of herpes zoster. They indicated that trauma increases the risk of herpes zoster at a trauma site within 1 month of the onset of skin rash but not elsewhere. These observations highlight the fact that traumatic stimulation of a nerve could trigger viral activation in the dorsal root ganglion of the nerve. The reactivation of herpes zoster in our patient, whose skin rash appeared on the 20th day after facial trauma, was correlated with recent trauma. The explanation for the elicitation of herpes zoster is direct pressure or stimulation on the trigeminal nerve bundle or ganglia during the trauma event. Post-traumatic craniocollar pain after facial trauma involving simple bony or soft tissue abnormalities can be mimicked by various stages of herpes zoster. It is difficult to consider zoster reactivation in a traumatic area before vesicles appeared until the neuralgia characteristic occurred. The earlier consideration of this possibility raised the opportunity for prompt management with good results. Antiviral agents should be given within 72 hours to improve the outcome and prevent post-herpetic neuralgia,15 although the timing is still in debate. Corticosteroids are effective to decrease the inflammatory reaction and shorten the disease process.16 Gabapentin with specific voltage-gated calcium channel blocker to relieve neuropathic pain has been well documented in pre-herpetic or post-herpetic neuralgia with the adverse effects being dizziness and drowsiness; therefore, a slow titration of the dose is needed in the treatment course.17 To the best of our knowledge, there have not been any cases of reactivated herpes zoster with zoster-associated neuropathic pain along the traumatic trigeminal lesion reported in the literature previously. (In total, there are less than 10 reports about zoster reactivation in traumatic lesion.) Competing interests: none. Patient consent: Patient/guardian consent was obtained for publication. REFERENCES 1. Schimpff, S, Serpick, A, Stoler, B, et al. Varicella-zoster infection in patients with cancer. Ann Intern Med 1972; 76: 241–54.[Abstract/Free Full Text] 2. Gnann, JW, & Whitley, RJ. Clinical practice. Herpes zoster. N Engl J Med 2002; 347: 340–6.[Free Full Text] 3. Thomas, SL, & Hall, AJ. What does epidemiology tell us about risk factors for herpes zoster. Lancet Infect Dis 2004; 4: 26–33.[CrossRef][Medline] 4. Levy, JM, & Smyth, SH. Reactivation of herpes zoster after liver biopsy. J Vasc Interv Radiol 2002; 13: 209–10.[CrossRef][Medline] 5. Lee, MR, & Ryman, W. Herpes zoster following cryosurgery. Austral J Dermatol 2005; 46: 42–3.[CrossRef] 6. Wood, JR, & Anderson, RL. Complications of cryosurgery. Arch Ophthalmol 1981; 99: 460–3.[Abstract/Free Full Text] 7. Wackym, PA, Gray, GF, & Avant, GR. Herpes zoster of the larynx after intubational trauma. J Laryngol Otol 1986; 100: 839–41.[Medline] 8. Percival, NJ. Shingles following axillary nerve block: a case report. J Hand Surg 1986; 11: 115–16.[Abstract/Free Full Text] 9. Weiss, R. Herpes zoster following spinal surgery. Clin Exp Dermatol 1989; 14: 56–7.[CrossRef][Medline] 10. Mumm, AH, Morens, DM, Elm, JL, et al. Zoster after shiatsu massage (Letter). Lancet 1993; 341: 447.[Medline] 11. Bailey, MH, & McKinney, P. Herpes zoster as a complication of face lift. Anesthetic Plast Surg 1988; 12: 23–4.[CrossRef][Medline] 12. Furuta, Y, Ohtani, F, Fukuda, S, et al. Reactivation of varicella-zoster virus in delayed facial palsy after dental treatment and oro-facial surgery. J Med Virol 2000; 62: 42–5.[CrossRef][Medline] 13. Massad, MG, Navarro, RA, Rubeiz, H, et al. Acute postoperative shingles after thoracic sympathectomy for hyperhidrosis. Ann Thorac Surg 2004; 78: 2159–61.[Abstract/Free Full Text] 14. Thoms, SL, Wheeler, JG, & Hall, AJ. Case-control study of the effect of mechanical trauma on the risk of herpes zoster. BMJ 2004; 328: 439–40.[Free Full Text] 15. Ormrod, D, & Goa, K: Valaciclovir: a review of its use in the management of herpes zoster. Drugs 2000; 59: 1317–40.[CrossRef][Medline] 16. Kawasaki, A, & Borruat, F. An unusual presentation of herpes zoster ophthalmicus: orbital myositis preceding vesicular eruption. Am J Ophthalmol 2003; 136: 574–5.[CrossRef][Medline] 17. Johnson, RW. Zoster-associated pain: what is known, who is at risk and how can it be managed? Herpes 2007; 14: 30–4.[Medline]