JOHNS HOPKINS
U
N
I
V
E
R
S
I
T
Y
Department of Pathology
600 N. Wolfe Street / Baltimore MD 21287-7093
(410) 955-5077 / FAX (410) 614-8087
Division of Medical Microbiology
THE JOHNS HOPKINS MICROBIOLOGY NEWSLETTER Vol. 26, No. 04
Tuesday, February 20, 2007
A. Provided by Sharon Wallace, Division of Outbreak Investigation, Maryland Department of
Health and Mental Hygiene.
There is no information available at this time.
B. The Johns Hopkins Hospital, Department of Pathology, Information provided by,
Justin A. Bishop, M.D.
Case presentation:
The patient was a 43-year-old woman with a medical history significant for chronic lymphocytic
leukemia diagnosed in 2001. She was treated with multiple cycles of chemotherapy as well as an
allogenic bone marrow transplant in March 2006. Her post-transplant clinical course was complicated by
ocular, oral, cutaneous, and pulmonary manifestations of graft-versus-host disease for which she received
high-dose corticosteroids. She also had pulmonary radiological changes felt to be consistent with a fungal
pneumonia, for which she was placed on voriconazole. On 12/23/2006, the patient awoke unable to speak.
Imaging of the brain revealed multiple lesions consistent with infection, neoplasm, or vasculitis; the
patient proceeded to brain biopsy. Histological sections revealed angiocentric, aseptate fungal hypae with
wide-angle branching. Cultures of the brain tissue grew Mucor species. The brain lesions were debrided,
and the patient was treated with AmBisome and posaconazole. The patient’s neurological and pulmonary
status continued to decline, however, and the patient expired on 1/7/2007.
Organism:
Mucor is a member of the Zygomycetes, a class of fungi that reproduce sexually by the formation
of zygospores, and produce pauciseptate, wide hyphae. The Zygomycetes are subclassified into the orders
Enthomophthorales and Mucorales, the latter of which Mucor is a member. The Zygomycetes are
ubiquitous in nature, largely saprobic on plant debris and soil, and common contaminants in the lab. Most
of the species known to cause human disease belong to the family Mucoraceae, and are recognized by
their rapid growth rate (filling a Petri dish in 3-5 days, they are colloquially known as “lid lifters”), fluffy,
“cotton candy-like” appearance, and brownish-gray color in culture. The growth of the Zygomycetes is
inhibited by cycloheximide. Other frequently isolated genera of this family include Absidia, Rhizopus
(including the most common isolate, Rhizopus oryzae), Rhizomucor, and Apophysomyces.
Clinical Manifestations:
The Zygomycetes cause a clinical spectrum of illnesses known as zygomycosis (known previously
as phycomycosis and mucormycosis) that results from invasion of the vasculature by hyphae, resulting in
thrombosis and infarction of the surrounding tissue. Infection in the immunocompetent host is rare, and is
usually limited to a subcutaneous infection resulting from a traumatic implantation of spores. These cases
respond well to debridement and antifungal therapy. Progressive infection in an immunocompetent
individual is very, very rare. Conversely, infection in the immunocompromised host results in the most
severe, fulminant infection known. Host risk factors include diabetes mellitus, neutropenia,
immunosuppressive therapy, chronic corticosteroid administration, iron chelation therapy, broad-spectrum
antibiotic use, severe malnutrition, and breakdown of the cutaneous barrier by way of trauma, surgical
wounds, needle sticks, or burns.
Rhinocerebral syndromes are the most common clinical presentation, and are the result of the
inhalation of spores into the paranasal sinuses of susceptible hosts. Acidotic diabetes is the most common
underlying condition in these cases. The infection usually presents initially as an acute sinusitis, with fever,
purulent nasal discharge, and facial pain. Spread of the infection to contiguous structures occurs very
quickly. The hallmarks of spread beyond the sinuses are tissue necrosis of the palate resulting in palatal
eschars, destruction of the turbinates, perinasal swelling, erythema and cyanosis of the overlying facial skin,
facial palsy, and proptosis.
Pulmonary zygomycosis is a rapidly progressive infection that occurs after the inhalation of spores
into the bronchioles and alveoli. A diffuse pneumonia with infarction and necrosis results and the infection
can spread to contiguous structures such as the mediastinum and heart. Pulmonary zygomycosis is the most
common syndrome that precedes systemic spread of the disease.
Gastrointestinal zygomycosis is a rare entity that results from the ingestion of zygomycetous spores.
Patients present with abdominal pain and hematemesis. The gastrointestinal lesions are necrotic ulcers that
can lead to perforation and peritonitis. Bowel infarctions and hemorrhagic shock can result, and the
prognosis is very poor.
Infection of the skin and soft tissues results from traumatic inoculation of the spores into the dermis.
The trauma leading to implantation can include venipuncture, spider bites, insulin injection, burns, and
surgical wounds, dressings, or splints. Nosocomial outbreaks of zygomycosis have occurred associated with
the use of contaminated elastic dressings. Cutaneous zygomycosis usually presents as a single, painful,
indurated area of cellulitis that quickly progresses to tissue necrosis. Dissemination can occur, but is an
infrequent complication of this disease.
Pathogenesis:
Intact mucosal and endothelial barriers serve as structural defenses against tissue and vessel invasion
and by Zygomycetes. If breached, sporangiospores have unique capability for tissue adherence and invasion
of intact endothelial barriers. Surprisingly, viable spores are not essential to cause tissue damage; injection of
heat-killed Rhizopus spp can result in significant mortality in experimental diabetic mice. Once spores are
taken up in the endothelium, phagocytic cells prevent germination of the conidia and kill the hyphal forms.
Phagocytic defects because of cell-number deficiency and functional defects caused by corticosteroids,
hyperglycemia, or acidosis allow proliferation of the fungus.
Iron is required for the growth and virulence of virtually all microbial pathogens; indeed, the ability
to scavenge free iron from the host is clearly an essential component of the pathogenesis of zygomycetes. In
mammalian hosts little serum iron is available to microorganisms because of its strong binding to serum
proteins such as transferrin. Fungi can acquire iron from the host using iron chelators (siderophores) or highaffinity iron permeases such as ferrirhizoferrin. It is thought that acidosis disrupts the capacity of iron
transporter proteins to bind to iron. Also, treatment with deferoxamine has been associated with a markedly
increased incidence of zygomycosis, as these fungi can use this specific chelator as a siderophore to access
iron previously unavailable to them.
Diagnosis:
Direct microscopic examination: Calcoflour white is a fluorescent dye used for rapid morphologic
detection of fungi in the microbiology lab. The dye binds to chitin present in fungal walls and fluoresces
when viewed by a UV microscope. Zygomycetes have a distinctive appearance: sparsely septate, broad (6-25
um), ribbon-like hyphae with irregular branching at right angles. Similarly, the organism may be detected via
tissue biopsy, where similar morphology is seen. Zygomycetes are oserved fairly well with routine
Hemotoxylin and Eosin stains; GMS and PAS may aid in their visualization.
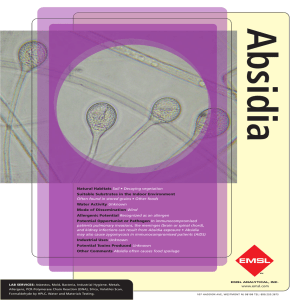
Figure 1 – Mucor
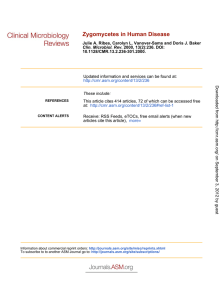
Figure 2 – Rhizopus
Culture: As mentioned above, Zygomycetes grow rapidly in culture. Genus assignment is based on
the arrangement of rhizoids (root-like hyphae) in relation to sporangiophores. Rhizopus is characterized by
sporangiophores arising directly over the rhizoids, while sporangiophores arising between rhizoids are
characteristic of Absidia. Stolons are seen in both Rhizopus and Absidia. Mucor, on the other hand, does not
produce rhizoids or stolons. (See Figures 1 and 2.)
Treatment:
Extensive surgical debridement of the affected tissue, along with antifungal therapy, is
recommended. Successful treatment depends greatly on timely diagnosis. In addition, rapid correction of
underlying conditions, such as appropriate control of hyperglycemia or correction of diabetic ketoacidosis,
immediate tapering of corticosteroids and immunosuppressive drugs, and discontinuation of deferoxaminebased treatment, is critical to outcome. Most of the evidence of the activity of existing antifungal agents has
come from small case series, case reports, and in vivo studies of animal models of zygomycosis. Therefore,
the optimal therapy is uncertain. Currently, the recommended antifungal therapy for zygomycosis includes
Amphotericin B administered at the highest tolerated dosage. Lipid formulations have been used to treat
zygomycosis, although no comparative studies have been performed. Caspofungin lacks significant activity
against zygomycetes in vitro, and most azoles, including fluconazole and voriconazole, have no meaningful
activity. In fact, it has been suggested that a rise in cases of zygomycosis in oncology patients is associated
with increased prophylactic use of voriconazole in this population. Interestingly, posaconazole, however,
does seem to possess potent activity against these fungi.
References:
1. Dennis JE et al. Nosocomical Rhizopus infection (zygomycosis) in children. J Pediatr.
1980;96(5):824-8.
2. Koneman EW at al. Color Atlas and Textbook of Diagnostic Microbiology, 6th ed. New York:
Lippincott-Raven, 2006.
3. Kontoyiannis DP and Lewis RE. Invasive zygomycosis: update on pathogenesis, clinical
manifestations, and management. Infect Dis Clin N Am 20 (2006) 581–607.
4. Larone DH. Medically Important Fungi: A Guide to Identification, 4th ed. Washington, D.C.: ASM
Press, 2002.
5. Merz WG and Hay RJ. Topley and Wilson’s Microbiology and Microbial Infections: Medical
Mycology, 10th ed. Washington, D.C.: ASM Press, 2005.
6. Sanz Alonso MA et al. Epidemiology of invasive fungal infections due to Aspergillus spp. and
Zygomycetes. Clin Microbiol Infect. 2006;12 Suppl 7:2-6.
 0
0