Musculoskeletal Injuries Temple College EMS Professions ECA
advertisement

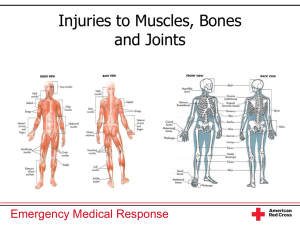
Musculoskeletal Injuries Temple College EMS Professions ECA Muscles • Maintain posture, allow movement • 3 types: – Skeletal (Striated) – Smooth (Involuntary) – Cardiac Bones •Support against gravity •Movement •Protection •Production of blood cells •Storage of minerals Joints • Motion • Flexibility Musculoskeletal Injuries • Fracture – Break in bones continuity • Dislocation – Displacement of bone ends from joint • Sprain – Tearing of ligaments • Strain – Tearing of muscle Forces of MOI •Direct •Indirect •Twisting •High-energy Fractures •Closed/simple •Open/compound •Non-displaced •Displaced Types of Fractures •Greenstick –Fraying •Comminuted –Shattered •Pathologic –Disease •Epiphyseal –Growth plate Types of Fractures • Open - break in the continuity of the skin • Closed - no break in the continuity of the skin Signs and Symptoms • • • • • • • Deformity or angulation Pain and tenderness Grating Swelling Bruising Exposed bone ends Joint locked into position General Rules • Determine if problem with circulation or nerves • Immobilize the joint above and below the injury. • Remove or cut away clothing. • Cover open wounds with a sterile dressing. • If there is a severe deformity or the distal extremity is cyanotic or lacks pulses, align with gentle traction before splinting. General Rules • Do not intentionally replace the protruding bones. • Pad each splint • Splint the patient before moving when feasible and no life threats. • When in doubt, splint the injury • If in shock, immobilize using long board Reasons to Immobilize • Prevent motion of bone fragments, bone ends or joints. • Minimize the following complications: – Damage to muscles, nerves, or blood vessels caused by broken bones. – Conversion of a closed fracture to open fracture – Interruption of blood flow – Excessive bleeding – Increased pain – Paralysis of extremities Hazards of Improper Splinting • Compression of nerves, tissues and blood vessels • Delay in transport of a patient with life threatening injury • Reduced Distal Circulation • Aggravation of the injured area • Cause or aggravate tissue, nerve, vessel or muscle Equipment • • • • Rigid splints Traction splints Pneumatic splints (air, vacuum) Improvised splints, pillow Long Bone Splinting Procedure • Take Body substance isolation • Apply manual stabilization to bone. • Assess pulse, motor and sensory function. • If severe deformity or the distal extremity is cyanotic or lacks pulses, align with gentle traction before splinting. Splinting Procedure • Measure splint. • Apply splint immobilizing the bone and joint above and below the injury. • Secure entire injured extremity. • Immobilize hand/foot in position of function. • Reassess pulse, motor, and sensation after application of splint and record. Splinting a Joint • • • • Body substance isolation Apply manual stabilization to joint Assess pulse, motor and sensory function. Align with gentle traction if distal extremity is cyanotic or lacks pulses and no resistance is met. • Immobilize the site of injury. • Immobilize bone above and below the site of injury. • Reassess pulse, motor and sensation Traction Splinting • Indications – Mid Shaft Femur Fracture – Open or Closed • Contraindications – Injury is close to the knee – Injury to the knee exists – Injury to the hip – Injured pelvis – Partial amputation – Lower leg or ankle injury. Traction Splint Ischial pad Length-adjustment sleeve Ischial strap Support straps Winch “S”-hook Ankle harness Heel stand “D”-ring Traction Splinting Procedures • Assess pulse, motor, and sensation distal to the injury • Body substance isolation • Perform manual stabilization of the Femur • Apply manual traction • Prepare/adjust splint to proper length. • Position splint under injured leg. Traction Splint Procedures • • • • • • Apply proximal securing device (ischial strap). Apply distal securing device (ankle hitch). Apply mechanical traction. Position/secure support straps. Re-evaluate proximal/distal securing devices. Reassess pulses, motor, sensation distal to the injury • Secure torso to the longboard to immobilize hip. • Secure splint to the long board to prevent General Management • • • • • • Body substance isolation Manage life threats Oxygen (NRB @ 15 lpm) Splint Injured Area Application of cold pack Elevate the extremity.