Illinois Health Record
advertisement

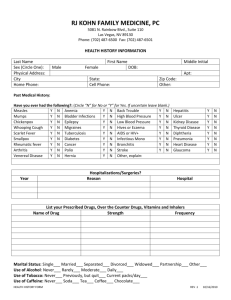
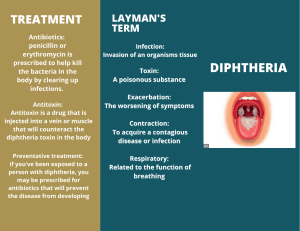
Illinois Health Record Name: Club: YOUR FAMILY’S HEALTH HISTORY Parents Name Birthdate Birthplace Nationality Occupation Height at age 25 Weight at age 25 Weight now General Physical Condition Father: Mother: Year: YOUR OWN HEALTH HISTORY Diseases Diphtheria Measles Mumps Pnuemonia Scarlet Fever Strep sore throat Whooping cough Polio Rhuematic fever Heart disease Other Age Nature and Effect Major Diseases and illnesses of parents Immunizations Tuberculosis Diabetes Anemia Cancer Rheumatic Fever Heart disease Disease of nervous system Overweight Underweight Others If not living, give date and cause of death Brother and Sisters Name: Date of birth: Serious illnesses: Date: Date: Date: Smallpox Diphtheria Whooping cough Tetanus Polio Typhoid Tests Test: Schick (Diphtheria) Tuberculin X-ray Laboratory Examination Other Blood Type: Date: Results: Rh Factor: Allergies: Operations and Accidents Accident/Operation Date: Serious Aftereffects: