Comprehensive Geriatric Assessment in Nottinghamshire (Jo Harvey)
advertisement
")
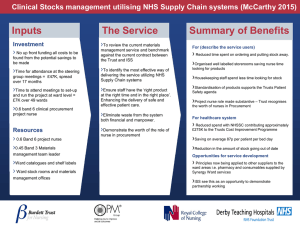
4th December 2013 Comprehensive Geriatric Assessment in Nottinghamshire The Community Programme Better Together The Community Programme 2 Better Together Identifying Seniors at Risk (ISAR) ISAR tool involves answering the following questions in yes/no manner: 1) 2) 3) 4) 5) 6) Does the patient have carers? Have the carers found it more difficult to care? Does the patient have any memory problems? Does the patient have any visual problems? Does the patient take more than 3 medications? Has the patient been in hospital for more than 1 night in the past 6 months? Every ‘yes’ response equates to 1 mark. The higher the score the higher the frailty of the patient/citizen. The Community Programme 3 Better Together Project 1 – Jackie Butterworth Hospital Threshold CGA - Comprehensive Geriatric Assessment at the Front Door Trial - Develop a multi-disciplinary team to provide CGA to Patients on Ward D57 Aim: • To improve service user, carer and staff experience • To reduce the likelihood of future crisis and readmission to the acute setting • To expedite transfer of care to a community setting (where appropriate) and reduce the time that frail older people, admitted as medical emergencies, spend in hospital unnecessarily “Having the CGA team to focus on the frail older people on our ward and help us to plan their care and assist with discharge planning is great.” Staff Nurse – Ward D57 The Community Programme 4 Better Together Strengthening our links for Dementia patients through CGA Project 1 During the initial trials links with the B47 team were made Attendance by Mental Health Nurse at Delivery Group meetings During the trials links with the Liaison Psychiatry Team were made Referral process used for advise / assessment of D57 patients Project 2 Links to Dementia Outreach Team when letters specify dementia diagnoses Mental Health Specialist Nurse working on “Triage to CGA” as part of the Integrated Health and Social Care Team Links to Mental Health Intermediate Care The Community Programme 5 Better Together