Curr. Pharm. Biotechnol. 4 21-37 (2003).doc
.doc")
Current Pharmaceutical Biotechnology (IN PRESS)
Inhibiting Cyclin-Dependent Kinase/Cyclin Activity for the Treatment of Cancer and Cardiovascular Disease.
C. Ivorra, H. Samyn, M. D. Edo, C. Castro, S. M. Sanz-González, A. Díez-Juan and V.
Andrés*
Unit of Vascular Biology, Instituto de Biomedicina de Valencia (IBV-CSIC), Spanish
Council for Scientific Research, Valencia, Spain.
*Author for correspondence:
Instituto de Biomedicina de Valencia (IBV-CSIC)
C/ Jaime Roig, 11
46010 Valencia (Spain)
Tel: +34-96-3391752
FAX: +34-96-3690800
E-mail: vandres@ibv.csic.es
1
ABSTRACT
Excessive cell proliferation contributes to the pathobiology of human diseases with a high health and socio-economic impact, including cancer and vascular occlusive diseases (e. g., atherosclerosis, in-stent restenosis, transplant vasculopathy, and vessel bypass graft failure).
Recent advances in the understanding of the molecular networks governing the hyperplastic growth of tumors and vascular obstructive neointimal lesions have provided new perspectives for preventive and therapeutic strategies against these disorders.
Mammalian cell proliferation requires the activation of several cyclin-dependent protein kinases (CDKs). Postranslational activation of CDKs is a complex process that involves their association with regulatory subunits called cyclins. The activity of CDK/cyclin holoenzymes is negatively regulated through their interaction with members of the CDK family of inhibitory proteins (CKIs). Moreover, over fifty low molecular weight pharmacological CDK inhibitors that target the ATP-binding pocket of the catalytic site of CDKs have been identified. In this review, we will discuss the use of pharmacological and gene therapy strategies against
CDK/cyclins in animal models and clinical trials of cancer and cardiovascular disease.
2
1. INTRODUCTION
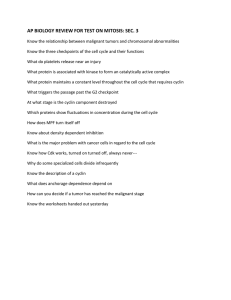
Tight control of cellular growth is essential to ensure normal tissue patterning during embryonic and postnatal development. Several cell proliferation regulatory networks have been associated with hyperplasia during both cancer progression and vascular occlusive diseases (e. g., atherosclerosis, restenosis after angioplasty, transplant vasculopathy, and graft atherosclerosis after bypass) [1-4]. Cell cycle progression is controlled by several CDKs that associate with regulatory subunits called cyclins [5,6]. Different CDK/cyclin complexes are orderly activated at specific phases of the cell cycle (Fig. 1). Progression through the first gap-phase (G
1
) requires both cyclin D- and cyclin E-associated CDK activity. Functional CDK2/cyclin A complexes are required for DNA synthesis (S-phase) and, subsequently, CDC2/cyclin A and CDC2/cyclin B pairs are assembled and activated during the second gap-phase (G
2
) and mitosis (M-phase), respectively. The requirement of CDK2 for entry into mitosis as a positive regulator of
CDC2/cyclin B activity as been suggested [7]. Aside from tight control of cyclin gene expression and protein turnover, the activity of CDK/cyclin pairs is regulated via their phosporylation and dephosphorylation at specific residues.
Active CDK/cyclin holoenzymes are presumed to hyperphosphorylate the retinoblastoma protein (pRb) and the related pocket proteins p107 and p130 from mid G1 to mitosis. The interaction among members of the E2F family of transcription factors and individual pocket proteins is a complex regulatory event that determines whether E2F proteins function as transcriptional activators or repressors [8-11]. Phosphorylation of pRb and related pocket proteins contributes to the transactivation of genes with functional E2F-binding sites, including several growth and cell-cycle regulators (i.e., c-myc, pRb, cdc2, cyclin E, cyclin A ), and genes encoding proteins that are required for nucleotide and DNA biosynthesis (i. e., DNA polymerase
, histone
H2A, proliferating cell nuclear antigen, thymidine kinase ) [9,11].
3
CDK/cyclin activity is negatively regulated by the interaction with specific CDK inhibitory proteins (CKIs) [12] (Fig. 1). CKIs of the Cip/Kip family (for CDK interacting protein/Kinase inhibitory protein) (p21
Cip1
, p27
Kip1
and p57
Kip2
) bind to and inhibit a wide spectrum of
CDK/cyclin holoenzymes, while members of the Ink4 family (for inhibitor of CDK4) (p16
Ink4a
, p15
Ink4b
, p18
Ink4c
, p19
Ink4d
) are specific for cyclin D-associated CDKs (CDK4 and CDK6).
Mitogenic and antimitogenic stimuli affect the rates of synthesis and degradation of CKIs, as well as their redistribution among different CDK/cyclin heterodimers.
2. PHARMACOLOGICAL INHIBITORS OF CDKs
2.1. Families of pharmacological CDK inhibitors
In this section, we will review the different families of pharmacological CDK inhibitors
(purines, alkaloids, indirubins, flavonoids, paullones, butyrolactone I, hymenialdisine and pyrazolo[3,4b ]quinoxalines), and their specificity against different protein kinases (Table 1).
These low molecular weight compounds compete with ATP for its binding to the ATP-binding pocket of the catalytic site of CDKs. Structural information on pharmacological CDK inhibitors was recently reviewed [13,14].
Purines
This family includes olomoucine, roscovitine, CVT-313, isopentenyl-adenine, purvalanols and other purine analogues obtained by combinatorial chemistry. Interaction of the purine portion of these inhibitors with the adenine-binding pocket of CDKs prevents the binding of ATP
[15-17].
Purvalanol B is highly specific for CDKs, with an IC
50
value of 6 nM for CDK1 (CDC2),
CDK2 and CDK5 [16]. In contrast, the IC
50
value of purvalanol B when tested against other
4
protein kinases is higher than 10
M [16]. Purvalanol A is a more permeable analog of purvalanol B that potently inhibits CDK2 (IC
50
= 35-70 nM) [16].
Aminopurvalanol is a potent inhibitor of CDK1, CDK2, and CDK5 [18].
The inhibitory effect of roscovitine is 10 times higher than that of olomoucine, with IC
50 values around 600 nM and 7
M, respectively [19-21]. The inhibitory activity of both compounds is high against CDK1, CDK2 and CDK5 as compared with CDK4. Eight new purine analogues show stronger inhibitory activity than olomoucine against CDK1 and CDK2 (IC
50 ranging from 0.03 to 3.8
M) [22].
The relative inhibitory potency of CVT-313 varies from very high for CDK2 (IC
50
= 500 nM), moderate for CDK1 (IC
50
= 4
M), and very low for CDK4 (IC
50
= 215
M) [23].
Isopentenyl-adenine is the weakest and less specific protein kinase inhibitor of the purine family, with IC
50
values for CDKs higher than 40
M [20,21,24].
Recent structure-activity relationship studies have allowed the design of more potent and selective CDK2 inhibitory purine derivates, including 6-benzylamino-2-thiomorpholinyl-9isopropylpurine (IC
50
= 900 nM) [25] and [6-(3-chloroanilino)-2-(2-hydroxypyrrolidyl)-9isopropylpurine] (IC
50
= 300 nM) [26].
Alkaloids
Members of this family (staurosporine, UCN-01 and CGP 41 251) inhibit a broad-spectrum of protein kinases, including protein kinase C (PKC) and CDKs.
Staurosporine is the most potent CDK inhibitory alkaloid, with IC
50
values in the nM range for CDK1, CDK2 and CDK5 [20,24,27]. The binding of staurosporine to CDK2 resembles that of the adenine base of ATP [28].
5
UCN-01 (7-hydroxystaurosporine) shows high affinity for PKC (IC
50
= 20-60 nM) and variable affinity for CDKs (IC
50
= 1
M for CDK1, and in the nM range for other CDKs) [29-
32]. Likewise, CGP 41 251 (4'-N-benzoylstaurosporine) is a potent PKC inhibitor that shows low affinity for CDKs (IC
50
values in the
M range) [33].
Indirubins
Indirubin is the active ingredient of a mixture of plants used in traditional Chinese medicine [34]. Indirubin and its derivatives inhibit the activity of a broad spectrum of CDKs
(high inhibitory activity against CDK1, CDK2 and CDK5, and 10 times lower for CDK4), and the evolutionarily related glycogen synthase kinase-3
(GSK-3
) (IC
50
= 5-50 nM) [35]. These inhibitors act by competing with ATP for binding to the ATP-binding site of CDK2 [34].
Indirubin is the least active member of the family, with IC
50
values in the
M range. The most potent inhibitor of this family is indirubin-5-sulphonic acid, with IC
50
values between 35 nM and
300 nM. Other indirubin derivatives with strong CDK inhibitory activity are 5-chloro-indirubin and indirubin-3’-monoxime, with IC
50
values between 200 nM and 800 nM for CDK1, CDK2 and CDK5, and around 5
M for CDK4 [34].
Flavonoids
Flavopiridol (L86-8275) and its derivative L86-8276 are relatively potent CDK inhibitors
(IC
50
values in the nM range) [36,37]. Crystallographic studies revealed the binding of the aromatic portion of L86-8276 to the adenine-binding pocket of CDK2 [38]. Moreover, the position of the phenyl group of L86-8276 enables this inhibitor to make exclusive contacts with
CDK2 that are not observed in the CDK2-ATP crystals.
Flavopiridol has higher specificity towards CDK4 (IC
50
= 65 nM) than towards CDK1 and
CDK2 (IC
50
values of 500 nM and 100 nM, respectively). The IC
50
values of flavopiridol for
6
other protein kinases are all in the
M range [36,37].
Casagrande et al [39] demonstrated that flavonoids which induced G1 arrest (i. e., quercetin, daidzein and luteolin) inhibited CDK2 activity by 40-60%. In contrast, other flavonoids which caused G2/M arrest (i.e., kaempherol, apigenin and genistein) inhibited CDK1 activity by 50-70%, without affecting CDK2 activity. All these flavonoids are relatively weak
CDK inhibitors (IC
50
> 100
M).
Paullones
Molecular modelling studies have suggested that paullones make contacts in the ATPbinding site of CDKs similar to those observed in the crystal structure of several CDK2-bound inhibitors [40]. Alsterpaullone shows high inhibitory activity against CDK1 (IC
50
= 35 nM) [41].
Although kenpaullone is a less potent CDK1 inhibitor (IC
50
= 400-800 nM), it retains high specificity for this enzyme (its IC
50
value for other protein kinases is in the
M range) [40].
Paullones also act as very potent inhibitors of GSK-3
and the neuronal CDK5/p25 kinase (IC
50 values in the nM range) [42]
Butyrolactone I
Butyrolactone I is a natural compound isolated from Aspergillus which acts as an ATP binding competitor with high specificity for CDK1 (IC
50
= 600 nM) and CDK2 (IC
50
= 1.5
M)
[43,44].
Hymenialdisine
Hymenialdisine is a natural compound isolated from a marine sponge which contains both bromopyrrole and guanidine groups [45]. The crystal structure of the CDK2-hymenialdisine complex shows hydrogen bonds similar to the links observed in other CDK-inhibitor structures.
7
Hymenialdisine is a very potent inhibitor of CDK1, CDK2 and CDK5 (IC
50
= 22-70 nM).
Interestingly, it shows high inhibitory activity against three protein kinases seemingly involved in Alzheimer’s disease (GSK-3
, casein kinase 1 and CDK5, with IC
50
values of 10 nM, 35 nM and 28 nM, respectively) [45].
Pyrazolo[3,4-b]quinoxalines
Members of this new family of synthetic CDK inhibitors have been identified by virtue of their structural similarity with some purine derivates. A preliminary structure-activity relationship study suggests that pyrazolo[3,4b ]quinoxalines can be optimized to inhibit CDKs and GSK-3. The most active compound (R
3
=NH
2
) shows strong inhibitory activity against the brain kinases CDK1, CDK5 and GSK-3 [46].
2.2. Biological effects of pharmacological CDK inhibitors on cultured cells
Table 2 summarizes representative studies of the biological effects of pharmacological
CDK inhibitors on cultured cells, which include cytostatic and cytotoxic effects, and induction of phenotypic differentiation. It is noteworthy that growth arrest by CVT-313 and alkaloids requires slightly higher concentrations than those needed to inhibit CDK activity in vitro . This disparity is even more pronounced for olomoucine, roscovitine, indirubins and butyrolactone I, whose effective in vivo concentrations are 10-100 times higher than those required to inhibit CDK activity in vitro . Poor membrane permeability of these compounds, and/or differences in the ATP concentrations used in the in vitro experiments compared to cellular conditions might account for these differences.
Pharmacological CDK inhibitors generally cause G1 and/or G2/M arrest, consistent with their potent inhibitory activity against both CDK2 and CDK1 (see Table 1). G1 arrest in cells treated with CDK inhibitory agents correlates with decreased pRb protein levels and/or
8
accumulation of hypophosphorylated pRb [31,34,37,47-49]. Interestingly, pRB status influenced the ability of UCN-01 to induce G1 blockade in several cancer cell lines [50]. Likewise, staurosporine failed to induce G1 arrest in the bladder carcinoma cell line 5637 that lacks a functional pRB, and restoration of pRb function in these cells by retroviral infection led to staurosporine-induced G1 arrest [51]. Nishi et al. examined the effect of staurosporine on the growth of several human tumor cell lines and oncogene-transformed NIH3T3 cell lines [52].
While all the cell lines that underwent G1 arrest in response to staurosporine contained functional pRB, this agent induced growth arrest in embryonic fibroblasts derived from pRb-null mice. Interestingly, staurosporine led to p27 kip1
accumulation regardless of whether it induced or not growth suppression. Collectively, these results suggest that pRb inactivation alone is not sufficient for the abrogation of staurosporine-induced G1 arrest, and that the antiproliferative potential of staurosporine depends on the integrity of cell cycle regulators which operate downstream of p27 kip1
.
Some inhibitors, like olomoucine [53,54], roscovitine [54], staurosporine [55,56], indirubin
[34], CVT-313 [23] and flavopiridol [37,57], can cause blockade in different cell cycle phases depending on both the concentration of the drug and the cell line analyzed. Cells treated with butyrolactone I accumulate mainly in G2/M, perhaps due to its higher affinity for CDK1 [58-61].
Evidence has been presented indicating that the kinase(s) involved in the regulation of cell exit from G1 and G2, respectively, in normal and leukemic lymphocytes may have different sensitivities to staurosporine, which suggests that the mechanisms controlling exit from G1 in these cells may be different [56].
Consistent with the observation that differentiation and proliferation are mutually exclusive processes in many cell types, treatment of cultured cells with agents that block cell cycle progression can simultaneously induce phenotypic differentiation. For instance, roscovitine and
9
flavopiridol caused mucinous differentiation of non-small cell lung cancer cells [62]. Likewise,
PC12 cells [27] and neuro2a cells [63] underwent neuronal differentiation when treated with staurosporine and butyrolactone I, respectively. Staurosporine can induce morphological and biochemical maturation in mouse keratinocyte cell lines [64], and might induce neuronal differentiation of human prostate cancer TSU-Pr1 cells [65]. Distinctive features of neuronal differentiation have been also observed upon exposure of PC12 cells to butyrolactone I or olomoucin, including the appearance of neurite extensions and induction of microtubuleassociated protein 2 expression [66].
During development and morphogenesis of multicellular organisms, physiological mechanisms of cell death operate to control cell number, and as a protective strategy to remove infected, mutated or damaged cells [67]. In many instances, programmed cell death (apoptosis) is associated with changes in CDK activity [68,69]. While cell death can be blocked by several pharmacological CDK inhibitors (i. e., butyrolactone I, olomoucine and roscovitine) [70,71], many tumor-derived cells respond to these agents with increased apoptosis (Table 2). Treatment of several bladder cancer cell lines with flavopiridol for 24 hours resulted in marked G2/M arrest
[72]. Although modest apoptosis was also observed, it required 72 hours of continuous drug exposure to become evident. Although “conflicting” signals resulting from forced inhibition of
CDKs under conditions of deregulated proliferation might be proposed as a general mechanism leading to apoptosis, different CDK inhibitors induce apoptosis via distinct molecular mechanisms [73].
2.3. Therapeutic use of pharmacological CDK inhibitors in animal models of cancer and vascular proliferative disease.
Table 3 summarizes some therapeutic applications of synthetic CDK inhibitors in animal models of cancer and neointimal thickening after balloon angioplastia.
10
Hyperplastic neointimal lesion growth is thought to contribute to restenosis after angioplasty, the recurrence of arterial narrowing at the site of intervention that occurs in 20-40% of coronary artery disease patients after successful revascularization [74-76]. The rat carotid model of balloon angioplasty has been used to assess the therapeutical efficacy of CVT-313 and flavopiridol. CVT-313 reduced neointimal lesion formation by 80 % when delivered at a dose of
1.25 mg/kg for 15 minutes under pressure at the site of balloon angioplasty [23]. Likewise, flavopiridol at 5 mg/kg administered orally for 5 days beginning at the day of balloon angioplasty reduced neointima formation by 35 % and by 39 % at day 7 and 14 after intervention, respectively [77].
The antitumor activity of pharmacological CDK inhibitors has been extensively investigated in experimental models of cancer. UCN-01 elicited antitumor activity in several murine xenogratft models using different human tumor cells (epidermoid carcinoma A431, fibrosarcoma HT1080, acute myeloid leukemia HL-60, and pancreatic tumor cells) [78,79]. Koh et al. investigated the therapeutic activity of UCN-01 against 3 human breast carcinoma cell lines
(MCF-7, Br-10, and MX-1) serially transplanted into nude mice [80]. UCN-01 had antitumor activity against MCF-7 and Br-10, while MX-1 was resistant to UCN-01. Although UCN-01 induced p21
Cip1
in the 3 cell lines in culture, little dephosphorylated pRb protein was expressed in MX-1 compared with Br-10 and MCF-7. Pharmacokinetic studies in mice, rats and dogs demonstrated high total clearance values of UCN-01 and higher concentrations of the drug in tumor tissue compared with those found in the plasma [79].
Ikegami et al. have demonstrated broad antitumor activity of CGP 41 251 in various types of murine and human tumor models [81]. When administered at a dose of 75 mg/kg 3 times daily for 9 days, this staurosporine derivative prolonged the life span of mice bearing B16 melanoma.
However, oral administration of CGP 41 251 at doses of 25-225 mg/kg once daily for 9 days was
11
ineffective in 4 kinds of murine tumor models. Oral administration of CGP 41 251 at a dose of
200 mg/kg once daily for 4 weeks showed antitumor activity (inhibition rates of 58-80%) in mice subcutaneously inoculated with several human tumor cells (gastric H-55, colorectal H-26, breast
H-31, lung H-74 and LC-376 cancer)
Several studies with murine models have shown antitumor activity of flavopiridol, including different human xenografted tumors (head and neck squamous cell carcinoma, colon carcinoma, prostate cancer, and leukemia and lymphoma xenografts) [82-85]. Treatment of mice bearing human head and neck squamous cell carcinoma xenografts with flavopiridol given as a daily intraperitoneal injection for 5 consecutive days at a concentration of 5 mg/kg resulted in a
23% reduction in tumor growth, reaching a 60% reduction 10 weeks after the end of the treatment [84]. In this study, flavopiridol induced apoptosis in tumor cells. In murine models using human tumors of lymphohematopoietic origin, including HL-60 and SUDHL-4 subcutaneous xenografts and Nalm/6 and AS283 disseminated disease models, intravenous injection of flavopiridol at a concentration of 7.5 mg/kg induced tumor regression [82].
Flavopiridol promoted apoptosis in these tumor models and in lymphoid organs (i. e., spleen, thymus and intestinal lymphoid tissues) of healthy mice [82].
Antitumor activity of some pharmacological CDK inhibitors may result from the combination of growth suppression and anti-angiogenic activity. For example, flavopiridol decreased blood vessel formation in a mouse Matrigel model of angiogenesis [83]. Likewise, the anticancer agent UFT, which is widely used in Japan to treat cancer patients requiring a longterm chemotherapy, inhibited angiogenesis induced by RENCA cells (murine renal carcinoma) in a dorsal air sac assay [86]. This inhibitory effect on angiogenesis was also elicited by the butyrolactone analogues
-hydroxybutyric acid (GHB) and
-butyrolactone (GBL), 2 UFTspecific metabolites. Interestingly, the antiangiogenic effects of GHB and GBL were increased
12
with administration by continuous infusion, providing a suitable pharmacokinetic profile.
3. GENE THERAPY STRATEGIES BASED ON CDK INHIBITION IN ANIMAL
MODELS OF CANCER AND CARDIOVASCULAR DISEASE.
Gene therapy approaches aimed at inhibiting CDK/cyclin activity attenuated both tumor progression and vascular occlusive lesion growth in experimental animals. These studies included antisense strategies and overexpression of CKIs using viral and non-viral vector systems (Table 4).
The efficacy of ex vivo genetic manipulation of tumor cells to inactivate CDK/cyclin activity followed by inoculation of these cells into the animal (i.e., xenograft in nude mice) ranges from different degrees of retardation of tumor growth and reduction of tumor size to complete loss of tumorigenicity. Inhibition of tumor growth can also take place when gene transfer occurs in vivo into pre-established tumors, whether or not this is followed by tumor regression. In some instances, prolongation of survival of the treated animal compared with controls has been demonstrated.
3.1. Antisense strategies to inhibit CDK/cyclin activity
The efficacy of antisense oligodeoxynucleotide strategies targeting CDKs and cyclins to reduce neointimal lesion formation has been demonstrated in several animal models of balloon angioplasty. These studies include antisense oligodeoxynucleotides against CDK2 [87,88],
CDC2 [87,89,90], and cyclin B1 [90]. Likewise, downregulation of cyclin G1 expression by retrovirus-mediated antisense gene transfer inhibited vascular smooth muscle cell proliferation and neointima formation after balloon angioplasty [91]. Attenuated graft atherosclerosis has been also observed upon inactivation of CDC2/PCNA [92] and CDK2 [93] with antisense
13
oligodeoxynucleotides.
Antisense cyclin D1 strategies have proven effective in inhibiting tumor growth in a variety of cancers xenograft models, including nude mice transplanted with human esophageal [94,95], colon [96] and pancreatic [97] cancer cells. Loss of tumorigenicity has been also observed with antisense cyclin D1 strategies in a murine neuT-transformed mammary adenocarcinoma [98], and in a K1735 melanoma [99] model of cancer. Moreover, antisense cyclin D1 reduced tumor size in experimental models of squamous cell tumors [100,101] and cutaneous melanoma [102].
Uto et al. reported inhibition of tumor growth and prolonged animal survival in a rat hepatoma xenograft model using a two-step gene transfer approach [103]. Cells were first infected with an adenovirus expressing the retrovirus receptor MCAT-1, and this was followed by retrovirus-mediated gene transduction of antisense cyclin D1.
Using retroviral vectors bearing antisense cyclin G1, Skotzko et al. demonstrated that cyclin G1 is essential for the survival and/or growth of cultured human osteosarcoma cells [104].
Moreover, delivery of concentrated high titer supernatants containing the antisense cyclin G1 retrovirus into rapidly growing subcutaneous tumors derived from human osteosarcoma cells inhibited tumor growth in athymic mice [105]. Histological examination showed diminished mitotic indexes and increased stroma formation within the residual treated tumors, which disclosed concomitant accumulation of cells in the G1 phase.
3.2. Overexpression of CKIs
Adenoviral and retroviral vectors are the most frequent delivery systems to assess the therapeutic efficacy of CKI overexpression for the treatment of experimental cancer and cardiovascular disease.
14
Overexpression of CKIs reduced neointimal lesion growth in animal models of balloon angioplasty, including adenovirus-mediated overexpression of p21
Cip1
[106-108] and p27
Kip1
[109,110] in normocholesterolemic animals. Likewise, overexpression of p21
Cip1 attenuated neointimal lesion development in balloon-injured arteries of hypercholesterolemic mice [111].
Neointimal thickening also contributes to graft atherosclerosis after vessel bypass. Using a plasmidic expression vector, Bai et al. reported reduced neointimal hyperplasia after vein grafting by in vivo transfer of human p21
Cip1
[112].
Adenovirus-mediated overexpression of p16
Ink4a
in mesothelioma cells, which display absence of p16
Ink4a
expression, resulted in inhibition of tumor formation, tumor growth arrest and diminished tumor size and spread in a murine xenograft model [113]. This strategy has been also used to deliver the p21 Cip1 or p27 Kip1 genes into p53-null human astrocytoma cells, which suppressed tumor formation in a peripheral murine xenograft model, and in an intracerebral model [114,115]. Adenovirus-mediated delivery of p21
Cip1 into murine renal carcinoma Renca cells followed by inoculation into nude mice completely suppressed tumorigenicity, and also inhibited the growth of established Renca tumors [116]. Repetitive injections of the p21
Cip1 expression vector induced tumor regression and prolonged animal survival. Retrovirus-mediated overexpression of human p16
Ink4a
and p21
Cip1 in RT-2 rat glioma cells suppressed tumorigenicity after intracranial implantation of infected cells, and also suppressed the growth of preestablished tumor infected in situ [117-119].
Several studies have shown significant dissimilarities in the efficacy of different CKIs in vitro and in vivo . Schreiber et al. investigated the effectiveness of adenovirus-mediated overexpression of p16
Ink4a
, p18
Ink4c
, p21
Cip1 and p27
Kip1
in inhibiting tumor formation in a polyomavirus middle T antigen model of murine breast carcinoma [120]. While all tested CKIs delayed tumor progression, the latency period varied from 5 weeks for the p19 Ink4d expression
15
vector to greater than 25 weeks for the p27 Kip1 expression vector. However, when preestablished tumors were injected directly with the adenoviral vectors, only the p16
Ink4a
expression vector delayed tumor growth. In contrast, as determined by their effects on in vitro colony formation assays, tumor growth in vivo and animal survival, Wang et al. demonstrated comparable tumor suppressor effects of p21
Cip1 and p16
Ink4a in the rat glioblastoma cell line RT-2 after retrovirus mediated gene delivery [119]. These authors also showed reduced tumor suppressor efficacy of p53 compared to p21
Cip1 and p16
Ink4a
. In an in vitro study with human breast cancer MDA-MB-
231 and MCF-7 cells infected with recombinant adenovirus expressing p27
Kip1
and p21
Cip1
, a markedly more (up to 56-fold) potent cytotoxic effect of p27
Kip1
was observed [121].
Combination gene transfer strategies to induce tumor regression have been assessed in animal models of cancer, some of which have demonstrated synergistic effects. For example, simultaneous overexpression of p21
Cip1 and H-2K b with adenoviral vectors resulted in a trend toward a reduced tumor growth greater than with either vector alone in an in vivo murine model
[122]. Likewise, simultaneous adenoviral transfer of p53 and p16
Ink4a
, but not p53 on its own, induced apoptotic death in tumor cells [123]. Moreover, combination of p16
Ink4a
and p53 overexpression led to significant growth suppression in hepatocellular carcinoma [123] and pancreatic [124] cancer models. In another study, a bicistronic replication-deficient adenovirus vector containing antisense urokinase-type plasminogen activator receptor and sense p16
Ink4a sequences suppressed the growth of tumors derived from glioblastoma cell lines in an ex vivo intracerebral tumor model and an in vivo subcutaneous tumor model [125].
It is noteworthy that antisense-mediated ablation of CKIs might be an efficient approach for the treatment of cancer when combined with other therapeutic agents. For example, p21
Cip1 antisense therapy radiosensitized human colon cancer cells by converting growth arrest to apoptosis [126]. Likewise, p27 Kip1 inactivation with antisense oligodeoxynucleotides sensitized
16
cultured tumor cells to several chemotherapeutic drugs, including flavopiridol [127]. Compared with each single treatment, the combination of flavopiridol and p27
Kip1
inactivation showed synergistic effects in vivo with respect to both the induction of apoptosis and the inhibition of tumor growth. Importantly, p27
Kip1
antisense treatment alone did not provoke any detectable tumor enhancement.
The use of nonviral vector systems for gene delivery into different tumor models has been described. For example, transfection of human breast cancer cells transfected with a p27
Kip1 expression plasmid prior to injection into nude mice increased the latency period before tumors became detectable, and reduced tumor size [128]. Plasmid-mediated transfer of p27
Kip1 into
HER/neu-transformed tumor cells also inhibited tumor growth [129]. In a xenograft model, combined gene transfer of p21 Cip1 and GM-CSF using a a nonviral gene delivery system was more effective than the transfer of each single gene, as indicated by greater inhibition of the growth of preestablished tumors and prolonged survival time of hepatoma-bearing mice [130].
Two studies have investigated the effect of chimeric CKI proteins. Patel et al. assessed the therapeutic activity of an adenovirus vector expressing a p27
Kip1
-p16
Ink4a
fusion molecule
(termed AV-W9) in a wide range of tumor cell types [131]. When assayed in cultured cells, AV-
W9 elicited a 5- to 50-fold greater tumoricidal activity than either of the parental molecules p16
Ink4a
and p27
Kip1
, and this effect was independent of the p53 and pRb status of the tumor cells.
Likewise, AV-W9 demonstrated p53-independent antitumor activity in several murine tumor models, whereas the parental molecules only elicited partial protection. AV-W9 also was the most potent inhibitor of human primary vascular smooth muscle and endothelial cell proliferation when compared to the parental p16
Ink4a and p27
Kip1
, p27
Kip1
derivatives, or several alternative p27
Kip1
-p16
Ink4a
chimeric molecules [132]. Moreover, AV-W9 was more effective in inhibiting neointimal thickening after balloon angioplasty in cholesterol-fed rabbits compared to
17
the parental AV-p16 Ink4a and AV-p27 Kip1 adenoviral vectors [133]. These studies suggest that combining the activities of different CKIs might increase the therapeutical activity in the treatment of cancer and restenosis postangioplasty.
4. CLINICAL DEVELOPMENT OF CDK INHIBITORY STRATEGIES FOR THE
TREATMENT OF CANCER AND CARDIOVASCULAR DISEASE PATIENTS
The efficacy of CDK inhibitory approaches in reducing tumor growth and vascular occlusive lesion formation in animal models of cancer and cardiovascular disease has encouraged clinical trials in patients with cancer and vascular obstructive disease. Despite the success of gene therapy strategies based on CKI overexpression in animal models (see above), future improvements are required to override the practical barriers and limitations placed on most clinical trials before these approaches exhibit wide application in clinic.
The clinical use of CDK inhibitory drugs in cancer and cardiovascular disease patients is discussed below. Indirubin, the active constituent of a traditional Chinese antileukaemia medicine, is the first example of a pharmacological CDK inhibitor being used to treat human cancer [34]. Flavopiridol was the first synthetic CDK inhibitor to enter clinical trials [134]. The clinical pharmacokinetics of flavopiridol and clinical trials of these compound have been recently reviewed [135,136]. Briefly, Phase I trials have been conducted in cancer patients to determine the maximum-tolerated dose, toxicity profile and pharmacology of flavopiridol give as a daily 1-hour infusion every 3 weeks, or as a 72-hour continuous infusion every 2 weeks
[135,137,138]. Despite the promising results of preclinical and Phase I clinical trials, flavopiridol was ineffective in several Phase II trials conducted in patients with refractory renal carcinoma
[139], metastatic non-small cell lung cancer [140], mantle cell lymphoma and chronic lymphocytic leukemia [136], and advanced gastric carcinoma [141]. Therefore, future
18
development of flavopiridol as an antitumor agent might depend on other doses and schedules of administration in combination with chemotherapy. Of note in this regard, Schwartz et al. reported recently the results of a Phase
clinical trial of flavopiridol in combination with paclitaxel (taxol), an agent that promotes microtubule assembly and inhibits microtubule disassembly [142]. Clinical activity was observed in patients with advanced esophageal, lung, and prostate tumors, including patients who had progressed on paclitaxel.
Results from a Phase
clinical trial in patients with refractory neoplasms indicated that
UCN-01 can be administered safely as an initial 72-hour continuous intravenous infusion with subsequent monthly doses administered as 36-hour infusions [143]. In this trial, one partial response was observed in a patient with melanoma, and one protracted period ( > 2.5 years) of disease stability was observed in a patient with alk-positive anaplastic large-cell lymphoma.
Evidence from one 68-year-old patient has been presented suggesting that UCN-01 can sensitize large B cell lymphoma to the cytotoxic effects of EPOCH II (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin) chemotherapy [144]. Concentrations of UCN-01 10-fold greater than maximum tolerated doses in rat and dogs are well tolerated in humans [145].
Additional distinctive features of the clinical pharmacokinetics of UCN-01 in contrast to experimental animals include unpredicted long elimination half-life, and extremely low distribution volumes and systemic clearance values [146]. These unusual pharmacokinetics in humans could be due, at least in part, to high-affinity binding of UCN-01 to
1-acid glycoprotein
[145,146]
The antiproliferative approaches used so far for the treatment of cardiovascular disease have focused on restenosis and graft atherosclerosis, during which neointimal hyperplasia is rapid and localized. These disorders remain the major limitation of revascularization by angioplasty and bypass. In general, systemic pharmacological approaches that proved effective
19
in animal models have been unsuccessful in reducing the incidence of clinical restenosis, including antiplatelet, anticoagulant, antithrombotic, antiproliferative, antioxidant, and antiinflammatory agents [147-150]. The lack of correlation between animal studies and clinical trials is likely the result of distinct vascular responses to mechanical injury, and/or dissimilar pharmacokinetics in diverse animal species. Owing that coronary stents represent almost 80% of the contemporary interventional procedures for revascularization, stent-based pharmacologic therapy to enhance local delivery of antiproliferative agents is the focus of active research.
Rapamycin (sirolimus) is a bacterial macrolide that potently inhibits vascular smooth muscle cell proliferation and migration, at least in part via upregulation of p27
Kip1
[151-154]. Preclinical studies have demonstrated the efficacy of rapamycin in inhibiting primary and metastatic tumor growth [155], and neointimal thickening in angioplasty and graft atherosclerosis models [156-
163]. Aside from p27
Kip1
upregulation, additional mechanisms might contribute to these beneficial effects, including the potent immunosuppressant activity and inhibition of protein translation elicited by rapamycin. Recent clinical trials using rapamycin-coated stents showed promising results for the prevention of neointimal proliferation, restenosis, and associated clinical events in patients undergoing coronary angioplasty [164,165].
E2F participates in the transcriptional activation of several growth and cell-cycle regulators
(i.e., c-myc, pRb, cdc2, cyclin E, cyclin A ), and genes encoding proteins that are required for nucleotide and DNA biosynthesis (i. e., DNA polymerase
, histone H2A, proliferating cell nuclear antigen, thymidine kinase ) [9,10]. Activation of E2F is triggered by CDK-dependent phosphorylation of pRb and pocket proteins. Thus, a common mechanism by which different
CDK/cyclin inhibitory strategies reduce tumor growth and neointimal thickening maybe blockade of E2F function. Indeed, inactivation of E2F directly using synthetic oligodeoxynucleotides containing an E2F consensus binding site prevented neointimal thickening after balloon angioplasty and vein grafting in experimental animals [166,167].
20
Application of this E2F ‘decoy’ strategy appears to be safe and can achieve sequence-specific inhibition of cell-cycle gene expression and DNA replication in patients receiving bypass vein grafts [168,169].
5. CONCLUDING REMARKS
Excessive cell proliferation is a hallmark of cancer and vascular obstructive disease (e. g., atherosclerosis, in-stent restenosis, transplant vasculopathy, and vessel bypass graft failure).
Substantial efforts over the last years have led to the development of antiproliferative strategies based on the inactivation of CDKs/cyclins that efficiently attenuated experimental cancer and cardiovascular disease, including the use of chemical inhibitors and gene therapy strategies based on antisense-mediated inactivation of CDKs and cyclins and overexpression of CKIs. These preclinical studies have encouraged clinical trials in patients with cancer and cardiovascular disease. Despite some encouraging results, a great effort is still necessary before these strategies exhibit wide application in clinic. Optimisation of synthetic CDK inhibitors might rely on improved selectivity and a thorough characterisation of their cellular targets. Regarding the use of gene therapy approaches, technical improvements are required to override the current practical barriers and limitations placed on most clinical trials. Combination of synthetic CDK inhibitors and gene therapy strategies with more conventional approaches (e. eg., chemotherapy and radiotherapy) should also help develop effective therapies against cancer and cardiovascular disease.
21
ACKNOWLEDGMENTS
Work in the laboratory of V. Andrés is currently supported by grants from the Spanish
Ministry of Science and Technology and Fondo Europeo de Desarrollo Regional (SAF2001-
2358, SAF2002-1443), and from Generalitat Valenciana (GV01-488). C. Ivorra, M. D. Edo, C.
Castro, and S. M. Sanz-González received salary support from the Spanish Ministry of Science and Technology, Generalitat Valenciana, Agencia Española de Cooperación Internacional, and
Fondo de Investigaciones Sanitarias, respectively. A. Díez-Juan was partially supported from the
Spanish DGESIC and Fondo Europeo de Desarrollo Regional (grant 1FD97-1035-C02-02), and from Fondo Social Europeo (CSIC-Programa I3P fellowship).
22
FIGURE LEGENDS
Figure 1: Mammalian cell cycle control by CDK/cyclin holoenzymes and members of the
CKI family of growth suppressors.
Sequential activation of specific CDK/cyclin complexes drives progression through the different phases of the cell cycle (CDK1 = CDC2). CDK/cyclin activity is negatively regulated by interacting inhibitory proteins of the CKI family (Cip/Kip and
Ink4 subfamilies). Mitogenic and antimitogenic stimuli affect the rates of synthesis and degradation of CKIs, as well as their redistribution among different CDK/cyclin heterodimers.
Additional mechanisms of cell cycle control include regulation of the synthesis and degradation of cyclins, and phosporylation/dephosphorylation of CDKs and cyclins.
23
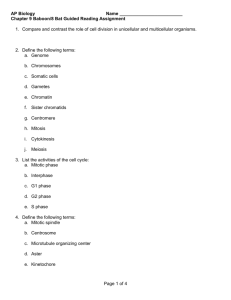
Table 1. Families of pharmacological CDK inhibitors.
The IC
50
value for each compound is shown. References are in square brackets.
PURINES
Olomoucine
Roscovitine
CVT-313
Isopentenyl-adenine
Purvalanol B
Purvalanol A
Aminopurvalanol
ALKALOIDS
Staurosporine
UCN-01
CGP 41 251
INDIRUBINS
Indirubin
5-Chloro indirubin
Indirubin-3’-monoxime
CDK1 (CDC2) CDK2
7
M [21]
650 nM [19]
4
M [23]
40
M [21] [24] 50
M [21]
6 nM [16]
33 nM [23]
20 nM [27]
1
1
M [29]
M [33]
10
M [34]
400 nM [34]
180 nM [34]
Indirubin-5-sulphonic acid 55 nM [34]
FLAVONOIDS
Flavopiridol 500 nM [36]
7
M [21]
700 nM [19]
500 nM [23]
6 nM [16]
35-70 nM [16]
28-33 nM [23]
3.2 nM [24]
600 nM [29] [30]
42 nM [31]
1
M [33]
32 nM [31]
2.2-7.5
M [34] 12
M [34] 5.5
M [34]
750-550 nM [34] 6.5
M [34] 800 nM [34]
440-250 nM [34] 3.33
M [34] 100 nM [34]
35-150 nM [34] 300 nM [34] 65 nM [34]
100 nM [37]
CDK4 CDK5 Other kinases
>1 mM [21] 8
M [20] [21] ERK1=25
M [21]
>100
M
[19]
200 nM [19] ERK1=34
M [19]
ERK2=14
M [19]
215
M [23]
200
M [21] 80
M [20] [21] CDK6>100
M [21]
6 nM [16]
PKC=43-100
M [21]
Other >10
M [16]
75 nM [16]
20 nM [23] CK1=3
M [23]
ERK2= 3.1
M [23]
ERK1=12
M [23]
75 nM [27]
65 nM [37]
39 nM [20]
CDK6=58 nM [31]
PKC=20-60 nM [170]
GSK3=0.6
M [35]
GSK3=50 nM [35]
GSK3=22 nM [35]
GSK3=33nM [35]
CDK6=60 nM [170]
CDK7=110-300 nM [170]
PAULLONES
Kenpaullone
Alsterpaullone
BUTYROLACTONE I
HYMENIALDISINE
PYRAZOLO[4,3-b]
QUINOXALINES
400 nM [40]
35 nM [41]
600 nM [44]
22 nM [45]
0.6
M [46]
680 nM [40]
15-200 nM [42]
1.5
M [43]
40-70 nM [45] 600 nM [45]
850 nM [40]
40 nM [42]
28 nM [45]
0.4
M [46]
ERK2>ERK1 [40]
GSK3=23 nM [42]
GSK3
/
=4 nM [42]
GSK3-
=10 nM [45]
CK1=35 nM [45]
GSK3=1
M [46]
24
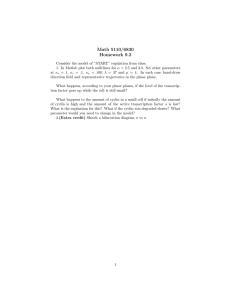
Table 2. Biological effects of pharmacological CDK inhibitors on cultured cells.
Olomoucine
Roscovitine
Cell Type Effects
Normal and tumor cell lines Growth arrest
Tumor cell lines Growth arrest, apoptosis
Normal and tumor cell lines Growth arrest
Tumor cell lines Growth arrest, apoptosis
Tumor cell lines Growth arrest, apoptosis, differentiation
References
[21,171-174]
[53,54]
[19,171,172,174-176]
[177-179]
[54,62]
CVT-313
HNSC carcinoma Apoptosis
Normal and tumor cell lines Growth arrest
[180]
[23] [221]
Staurosporine Tumor cell lines
Non-small cell lung cancer
Growth arrest
Growth arrest, apoptosis
Tumor cell lines Polyploidy
Human prostate cancer cells Differentiation
[47,49,51,56,181-185]
[49,56]
[55,186]
[65]
Normal and tumor cell lines Apoptosis
PC12 cells
[187-189]
Growth arrest, differentiation [27]
UCN-01 Normal and tumor cell lines Growth arrest [30-32,47,49,50,55,181,190-193]
Tumor cell lines
Tumor cell lines
Apoptosis
Growth arrest, apoptosis
[73,187,194-200]
[29,201,202]
CGP 41 251 Epidermoid carcinoma Poliploidy
-monoxime
Glioblastoma and gliosarcoma Growth arrest
Indirubin-3’-
Tumor and normal cell lines Apoptosis
Tumor and normal cell lines Growth arrest
[47]
[33,181,183,203]
[204,205]
[34,206,207]
Flavopiridol Tumor and normal cell lines Growth arrest
Tumor and normal cell lines Apoptosis
Non-small cell lung cancer
[37,48,57,72,77,208]
[73,209-215]
Growth arrest, differentiation [62]
Tumor cell lines Growth arrest, apoptosis [84,216-218]
Butyrolactone I Tumor cell lines
Colon carcinoma
Pancreatic cancer
Neuro 2a cells
Growth arrest
Growth arrest, apoptosis
Apoptosis
[58-61]
[219]
[220]
Growth arrest, differentiation [63]
25
Table 3. Pharmacological CDK inhibitors with beneficial effects in animal models of cancer and cardiovascular disease.
Experimental Model Dose References
CVT-313
UCN-01
Balloon angioplasty 1.25 mg/kg
Epidermoid carcinoma xenograft 5 mg/kg
[23]
[78]
Fibrosarcoma xenograft 7 mg/kg
Acute myeloid leukemia xenograft 7 mg/kg
Pancreatic tumor xenograft
Glioma xenograft
9 mg/kg
1-2 mg/kg/daily
[78]
[78]
[79]
[32]
Murine fibrosarcoma
HN12 xenograft
Breast carcinoma xenograft
7.5 mg/kg
7.5 mg/kg (5 days)
7.5 mg/kg/day
(5 days/week, 2 weeks)
[78]
[222]
[80]
CGP 41 251 Gastric, colorectal, breast and lung cancer xenografts
Murine melanoma
Flavopiridol Head and neck squamous cell carcinoma xenograft
200 mg/kg/day [81]
75 mg/kg (3 times daily) [81]
5 mg/kg/day [84]
Colon carcinoma xenograft
Prostate cancer xenograft
5 mg/kg (every other day) [83]
10 mg/kg/day [85]
Leukemia and lymphoma xenograft 7.5 mg/kg/day
Balloon angioplasty 5 mg/kg/day
[82]
[77]
26
Table 4. Gene therapy strategies targeting CDK/cyclin activity with beneficial effects in animal models of cancer and cardiovascular disease.
Strategy
1) Antisense-
mediated
inactivation
Targeted Gene Delivery System Animal Model cyclin D1 Retrovirus Cancer 1 cyclin D1 cyclin D1 cyclin G1
Plasmid
Adenovirus
Retrovirus
Cancer 2
Cancer 3
Cancer 4
CDK2
CDK2
References
[95,96,99,103]
[94,97,98]
[100-102]
Oligonucleotide Angioplasty
[105]
[87,88]
Oligonucleotide Graft atherosclerosis [93]
CDC2 cyclin B1
Oligonucleotide
Oligonucleotide
Balloon angioplasty
Balloon angioplasty
[87,89,90]
[90]. cyclin G1 Retrovirus Balloon angioplasty [91]
CDC2/PCNA Oligonucleotide Graft atherosclerosis [92]
2) Overexpression p16 Ink4a Retrovirus Cancer 5 [118,119]
of CKIs p16 Ink4a p16 Ink4a
Plasmid
Adenovirus
Cancer
Cancer
6
7
[223]
[113,120,123,124,224-227] p21 Cip1 p21 Cip1 p21 Cip1 p21 Cip1
Retrovirus
Plasmid
Adenovirus
Oligopeptide-
Cancer
Cancer
Cancer
Cancer
8
9
10
11
[117,119,228]
[229]
[114,116,120,122,230-232]
[130]
DNA polyplex p21 Cip1 p21 Cip1 p27 Kip1 p27 Kip1
Adenovirus
Plasmid
Plasmid
Adenovirus p27 Kip1 Adenovirus
3) Overexpression p27 Kip1 -p16 Ink4a Adenovirus
of CKI chimera p27 Kip1 -p16 Ink4a Adenovirus
Balloon angioplasty [106-108,110,111]
Graft atherosclerosis [112].
Cancer 12
Cancer 13
Cancer
Balloon angioplasty
Balloon angioplasty
[128]
[114,120,233,234]
[109,110]
[131]
[133]
1 Murine melanoma and tumor xenografts (esophageal cancer, colon cancer, and hepatoma).
2 Murine mammary adenocarcinoma and tumor xenografts (pancreatic carcinoma, and esophageal cancer).
3 Squamous carcinoma and melanoma xenografts.
4 Osteosarcoma xenograft.
5 Rat glioblastoma.
6 Nasopharyngeal carcinoma xenograft.
7 Murine mammary adenocarcinoma and tumor xenografts (lung cancer, hepatocelular carcinoma, mesothelioma, prostate cancer, glioma, colorectal cancer, pancreatic cancer, and breast cancer).
8 Rat glioblastoma and murine mammary cancer.
9 Colon carcinoma xenograft.
10 Murine tumors (renal carcinoma, prostate cancer, mammary adenocarcinoma), and tumor xenografts (astrocytoma, non small cell lung cancer, and cervical cancer).
11 Murine hepatoma.
12 Mammary epithelial cell xenograft, and HER2/neu-transformed cancer.
13 Murine mammary adenocarcinoma and tumor xenografts (astrocytoma, lung cancer, and renal carcinoma).
27
REFERENCES
[1] Ross, J.S.; Stagliano, N.E.; Donovan, M.J.; Breitbart, R.E. and Ginsburg, G.S. (2001)
Ann. N. Y. Acad. Sci., 947 , 271-292.
[2] Ross, R. (1999) N. Engl. J. Med., 340 , 115-126.
[3] Steinberg, D. (2002) Nat. Med., 8 , 1211-1217.
[4] Dzau, V.J.; Braun-Dullaeus, R.C. and Sedding, D.G. (2002) Nat. Med., 8 , 1249-1256.
[5] Morgan, D.O. (1995) Nature, 374 , 131-134.
[6] Nurse, P. (1994) Cell, 79 , 547-550.
[7] Guadagno, T.M. and Newport, J.W. (1996) Cell, 84 , 73-82.
[8] Weinberg, R.A. (1995) Cell, 81 , 323-330.
[9] Lavia, P. and Jansen-Durr, P. (1999) Bioessays, 21 , 221-230.
[10] Dyson, N. (1998) Genes Dev., 12 , 2245-2262.
[11] Stevaux, O. and Dyson, N.J. (2002) Curr. Opin. Cell. Biol., 14 , 684-691.
[12] Vidal, A. and Koff, A. (2000) Gene, 247 , 1-15.
[13] Fischer, P.M. (2001) Curr. Opin. Drug Discov. Dev., 4 , 623-634.
[14] Toogood, P.L. (2002) Curr. Opin. Chem. Biol., 6 , 472-478.
[15] De Azevedo, W.F.; Leclerc, S.; Meijer, L.; Havlicek, L.; Strnad, M. and Kim, S.H. (1997)
Eur. J. Biochem., 243 , 518-526.
[16] Gray, N.S.; Wodicka, L.; Thunnissen, A.M.; Norman, T.C.; Kwon, S.; Espinoza, F.H.;
Morgan, D.O.; Barnes, G.; LeClerc, S.; Meijer, L.; Kim, S.H.; Lockhart, D.J. and Schultz,
P.G. (1998) Science, 281 , 533-538.
[17] Schulze-Gahmen, U.; Brandsen, J.; Jones, H.D.; Morgan, D.O.; Meijer, L.; Vesely, J. and
Kim, S.H. (1995) Proteins, 22 , 378-391.
[18] Chang, Y.T.; Gray, N.S.; Rosania, G.R.; Sutherlin, D.P.; Kwon, S.; Norman, T.C.;
Sarohia, R.; Leost, M.; Meijer, L. and Schultz, P.G. (1999) Chem Biol, 6 , 361-375.
[19] Meijer, L.; Borgne, A.; Mulner, O.; Chong, J.P.; Blow, J.J.; Inagaki, N.; Inagaki, M.;
Delcros, J.G. and Moulinoux, J.P. (1997) Eur. J. Biochem., 243 , 527-536.
[20] Veeranna; Shetty, K.T.; Amin, N.; Grant, P.; Albers, R.W. and Pant, H.C. (1996)
Neurochem. Res., 21 , 629-636.
[21] Vesely, J.; Havlicek, L.; Strnad, M.; Blow, J.J.; Donella-Deana, A.; Pinna, L.; Letham,
D.S.; Kato, J.; Detivaud, L.; Leclerc, S. and et al. (1994) Eur. J. Biochem., 224 , 771-786.
28
[22] Vermeulen, K.; Strnad, M.; Krystof, V.; Havlicek, L.; Van der Aa, A.; Lenjou, M.; Nijs,
G.; Rodrigus, I.; Stockman, B.; van Onckelen, H.; Van Bockstaele, D.R. and Berneman,
Z.N. (2002) Leukemia, 16 , 299-305.
[23] Brooks, E.E.; Gray, N.S.; Joly, A.; Kerwar, S.S.; Lum, R.; Mackman, R.L.; Norman, T.C.;
Rosete, J.; Rowe, M.; Schow, S.R.; Schultz, P.G.; Wang, X.; Wick, M.M. and Shiffman,
D. (1997) J. Biol. Chem., 272 , 29207-29211.
[24] Rialet, V. and Meijer, L. (1991) Anticancer Res., 11 , 1581-1590.
[25] Oh, C.H.; Lee, S.C.; Lee, K.S.; Woo, E.R.; Hong, C.Y.; Yang, B.S.; Baek, D.J. and Cho,
J.H. (1999) Arch. Pharm. (Weinheim), 332 , 187-190.
[26] Oh, C.H.; Kim, H.K.; Lee, S.C.; Oh, C.; Yang, B.S.; Rhee, H.J. and Cho, J.H. (2001)
Arch. Pharm. (Weinheim), 334 , 345-350.
[27] Gollapudi, L. and Neet, K.E. (1997) J. Neurosci. Res., 49 , 461-474.
[28] Lawrie, A.M.; Noble, M.E.; Tunnah, P.; Brown, N.R.; Johnson, L.N. and Endicott, J.A.
(1997) Nat. Struct. Biol., 4 , 796-801.
[29] Wang, Q.; Worland, P.J.; Clark, J.L.; Carlson, B.A. and Sausville, E.A. (1995) Cell
Growth Differ., 6 , 927-936.
[30] Akiyama, T.; Yoshida, T.; Tsujita, T.; Shimizu, M.; Mizukami, T.; Okabe, M. and
Akinaga, S. (1997) Cancer Res., 57 , 1495-1501.
[31] Kawakami, K.; Futami, H.; Takahara, J. and Yamaguchi, K. (1996) Biochem. Biophys.
Res. Commun., 219 , 778-783.
[32] Pollack, I.F.; Kawecki, S. and Lazo, J.S. (1996) J. Neurosurg., 84 , 1024-1032.
[33] Begemann, M.; Kashimawo, S.A.; Heitjan, D.F.; Schiff, P.B.; Bruce, J.N. and Weinstein,
I.B. (1998) Anticancer Res., 18 , 2275-2282.
[34] Hoessel, R.; Leclerc, S.; Endicott, J.A.; Nobel, M.E.; Lawrie, A.; Tunnah, P.; Leost, M.;
Damiens, E.; Marie, D.; Marko, D.; Niederberger, E.; Tang, W.; Eisenbrand, G. and
Meijer, L. (1999) Nat. Cell Biol., 1 , 60-67.
[35] Leclerc, S.; Garnier, M.; Hoessel, R.; Marko, D.; Bibb, J.A.; Snyder, G.L.; Greengard, P.;
Biernat, J.; Wu, Y.Z.; Mandelkow, E.M.; Eisenbrand, G. and Meijer, L. (2001) J. Biol.
Chem., 276 , 251-260.
[36] Losiewicz, M.D.; Carlson, B.A.; Kaur, G.; Sausville, E.A. and Worland, P.J. (1994)
Biochem. Biophys. Res. Commun., 201 , 589-595.
[37] Carlson, B.A.; Dubay, M.M.; Sausville, E.A.; Brizuela, L. and Worland, P.J. (1996)
Cancer Res., 56 , 2973-2978.
[38] De Azevedo, W.F., Jr.; Mueller-Dieckmann, H.J.; Schulze-Gahmen, U.; Worland, P.J.;
Sausville, E. and Kim, S.H. (1996) Proc. Natl. Acad. Sci. USA, 93 , 2735-2740.
29
[39] Casagrande, F. and Darbon, J.M. (2001) Biochem. Pharmacol., 61 , 1205-1215.
[40] Zaharevitz, D.W.; Gussio, R.; Leost, M.; Senderowicz, A.M.; Lahusen, T.; Kunick, C.;
Meijer, L. and Sausville, E.A. (1999) Cancer Res., 59 , 2566-2569.
[41] Schultz, C.; Link, A.; Leost, M.; Zaharevitz, D.W.; Gussio, R.; Sausville, E.A.; Meijer, L. and Kunick, C. (1999) J. Med. Chem., 42 , 2909-2919.
[42] Leost, M.; Schultz, C.; Link, A.; Wu, Y.Z.; Biernat, J.; Mandelkow, E.M.; Bibb, J.A.;
Snyder, G.L.; Greengard, P.; Zaharevitz, D.W.; Gussio, R.; Senderowicz, A.M.; Sausville,
E.A.; Kunick, C. and Meijer, L. (2000) Eur. J. Biochem., 267 , 5983-5994.
[43] Kitagawa, M.; Okabe, T.; Ogino, H.; Matsumoto, H.; Suzuki-Takahashi, I.; Kokubo, T.;
Higashi, H.; Saitoh, S.; Taya, Y.; Yasuda, H. and et al. (1993) Oncogene, 8 , 2425-2432.
[44] Someya, A.; Tanaka, N. and Okuyama, A. (1994) Biochem. Biophys. Res. Commun., 198 ,
536-545.
[45] Meijer, L.; Thunnissen, A.-M.; White, A.; Garnier, M.; Nikolic, M.; Tsai, L.-H.; Walter,
J.; Cleverley, K.; Salinas, P.; Wu, Y.-Z.; Biernat, J.; Mandelkow, E.-M.; Kim, S.-H. and
Pettit, G. (1999) Chem. Biol., 7 , 51-63.
[46] Ortega, M.A.; Montoya, M.E.; Zarranz, B.; Jaso, A.; Aldana, I.; Leclerc, S.; Meijer, L. and Monge, A. (2002) Bioorg. Med. Chem., 10 , 2177-2184.
[47] Akiyama, T.; Shimizu, M.; Okabe, M.; Tamaoki, T. and Akinaga, S. (1999) Anticancer
Drugs, 10 , 67-78.
[48] Schrump, D.S.; Matthews, W.; Chen, G.A.; Mixon, A. and Altorki, N.K. (1998) Clin.
Cancer Res., 4 , 2885-2890.
[49] Shimizu, E.; Zhao, M.R.; Nakanishi, H.; Yamamoto, A.; Yoshida, S.; Takada, M.; Ogura,
T. and Sone, S. (1996) Oncology, 53 , 494-504.
[50] Mack, P.C.; Gandara, D.R.; Bowen, C.; Edelman, M.J.; Paglieroni, T.; Schnier, J.B.;
Gelmann, E.P. and Gumerlock, P.H. (1999) Clin. Cancer Res., 5 , 2596-2604.
[51] Schnier, J.B.; Nishi, K.; Goodrich, D.W. and Bradbury, E.M. (1996) Proc. Natl. Acad.
Sci. USA, 93 , 5941-5946.
[52] Nishi, K.; Schnier, J.B. and Bradbury, E.M. (1998) Exp. Cell Res., 243 , 222-231.
[53] Abraham, R.T.; Acquarone, M.; Andersen, A.; Asensi, A.; Belle, R.; Berger, F.;
Bergounioux, C.; Brunn, G.; Buquet-Fagot, C.; Fagot, D. and et al. (1995) Biol. Cell, 83 ,
105-120.
[54] Schutte, B.; Nieland, L.; van Engeland, M.; Henfling, M.E.; Meijer, L. and Ramaekers,
F.C. (1997) Exp. Cell Res., 236 , 4-15.
[55] Akinaga, S.; Nomura, K.; Gomi, K. and Okabe, M. (1994) Cancer Chemother.
Pharmacol., 33 , 273-280.
30
[56] Bruno, S.; Ardelt, B.; Skierski, J.S.; Traganos, F. and Darzynkiewicz, Z. (1992) Cancer
Res., 52 , 470-473.
[57] Kaur, G.; Stetler-Stevenson, M.; Sebers, S.; Worland, P.; Sedlacek, H.; Myers, C.; Czech,
J.; Naik, R. and Sausville, E. (1992) J. Natl. Cancer Inst., 84 , 1736-1740.
[58] Hida, D.; Nakata, K.; Shima, Y.; Migita, K.; Nakao, K.; Kato, Y.; Ishii, N. and Eguchi, K.
(1998) Anticancer Res., 18 , 4317-4322.
[59] Nishio, K.; Ishida, T.; Arioka, H.; Kurokawa, H.; Fukuoka, K.; Nomoto, T.; Fukumoto,
H.; Yokote, H. and Saijo, N. (1996) Anticancer Res., 16 , 3387-3395.
[60] Kitagawa, M.; Higashi, H.; Takahashi, I.S.; Okabe, T.; Ogino, H.; Taya, Y.; Hishimura, S. and Okuyama, A. (1994) Oncogene, 9 , 2549-2557.
[61] Suzuki, M.; Hosaka, Y.; Matsushima, H.; Goto, T.; Kitamura, T. and Kawabe, K. (1999)
Cancer Lett., 138 , 121-130.
[62] Lee, H.R.; Chang, T.H.; Tebalt, M.J., 3rd; Senderowicz, A.M. and Szabo, E. (1999) Int. J.
Oncol., 15 , 161-166.
[63] Inokoshi, J.; Katagiri, M.; Arima, S.; Tanaka, H.; Hayashi, M.; Kim, Y.B.; Furumai, R.;
Yoshida, M.; Horinouchi, S. and Omura, S. (1999) Biochem. Biophys. Res. Commun.,
256 , 372-376.
[64] Dlugosz, A.A. and Yuspa, S.H. (1991) Cancer Res., 51 , 4677-4684.
[65] Takahashi, N.; Shimizu, T. and Takeda, K. (2000) Prostate, 44 , 328-333.
[66] Dobashi, Y.; Shoji, M.; Kitagawa, M.; Noguchi, T. and Kameya, T. (2000) J. Biol. Chem.,
275 , 12572-12580.
[67] Vaux, D.L. and Korsmeyer, S.J. (1999) Cell, 96 , 245-254.
[68] Gil-Gomez, G.; Berns, A. and Brady, H.J. (1998) EMBO J., 17 , 7209-7218.
[69] Harvey, K.J.; Blomquist, J.F. and Ucker, D.S. (1998) Mol. Cell Biol., 18 , 2912-2922.
[70] Furukawa, Y.; Iwase, S.; Terui, Y.; Kikuchi, J.; Sakai, T.; Nakamura, M.; Kitagawa, S. and Kitagawa, M. (1996) J. Biol. Chem., 271 , 28469-28477.
[71] Maas, J.W., Jr.; Horstmann, S.; Borasio, G.D.; Anneser, J.M.; Shooter, E.M. and Kahle,
P.J. (1998) J. Neurochem., 70 , 1401-1410.
[72] Chien, M.; Astumian, M.; Liebowitz, D.; Rinker-Schaeffer, C. and Stadler, W.M. (1999)
Cancer Chemother. Pharmacol., 44 , 81-87.
[73] Kitada, S.; Zapata, J.M.; Andreeff, M. and Reed, J.C. (2000) Blood, 96 , 393-397.
[74]
Andrés, V. (1998)
Int. J. Molec. Med., 2 , 81-89.
[75] Bauters, C. and Isner, J.M. (1997) Prog. Cardiovasc. Dis., 40 , 107-116.
31
[76] Libby, P. and Tanaka, H. (1997) Prog. Cardiovasc. Dis., 40 , 97-106.
[77] Ruef, J.; Meshel, A.S.; Hu, Z.; Horaist, C.; Ballinger, C.A.; Thompson, L.J.; Subbarao,
V.D.; Dumont, J.A. and Patterson, C. (1999) Circulation, 100 , 659-665.
[78] Akinaga, S.; Gomi, K.; Morimoto, M.; Tamaoki, T. and Okabe, M. (1991) Cancer Res.,
51 , 4888-4892.
[79] Kurata, N.; Kuwabara, T.; Tanii, H.; Fuse, E.; Akiyama, T.; Akinaga, S.; Kobayashi, H.;
Yamaguchi, K. and Kobayashi, S. (1999) Cancer Chemother. Pharmacol., 44 , 12-18.
[80] Koh, J.; Kubota, T.; Migita, T.; Abe, S.; Hashimoto, M.; Hosoda, Y. and Kitajima, M.
(2002) Breast Cancer, 1 , 50-54.
[81] Ikegami, Y.; Yano, S.; Nakao, K.; Fujita, F.; Fujita, M.; Sakamoto, Y.; Murata, N. and
Isowa, K. (1995) Arzneimittelforschung, 45 , 1225-1230.
[82] Arguello, F.; Alexander, M.; Sterry, J.A.; Tudor, G.; Smith, E.M.; Kalavar, N.T.; Greene,
J.F., Jr.; Koss, W.; Morgan, C.D.; Stinson, S.F.; Siford, T.J.; Alvord, W.G.; Klabansky,
R.L. and Sausville, E.A. (1998) Blood, 91 , 2482-2490.
[83] Kerr, J.S.; Wexler, R.S.; Mousa, S.A.; Robinson, C.S.; Wexler, E.J.; Mohamed, S.; Voss,
M.E.; Devenny, J.J.; Czerniak, P.M.; Gudzelak, A., Jr. and Slee, A.M. (1999) Anticancer
Res., 19 , 959-968.
[84] Patel, V.; Senderowicz, A.M.; Pinto, D., Jr.; Igishi, T.; Raffeld, M.; Quintanilla-Martinez,
L.; Ensley, J.F.; Sausville, E.A. and Gutkind, J.S. (1998) J. Clin. Invest., 102 , 1674-1681.
[85] Drees, M.; Dengler, W.A.; Roth, T.; Labonte, H.; Mayo, J.; Malspeis, L.; Grever, M.;
Sausville, E.A. and Fiebig, H.H. (1997) Clin. Cancer Res., 3 , 273-279.
[86] Yonekura, K.; Basaki, Y.; Chikahisa, L.; Okabe, S.; Hashimoto, A.; Miyadera, K.;
Wierzba, K. and Yamada, Y. (1999) Clin. Cancer Res., 5 , 2185-2191.
[87] Abe, J.; Zhou, W.; Taguchi, J.; Takuwa, N.; Miki, K.; Okazaki, H.; Kurokawa, K.;
Kumada, M. and Takuwa, Y. (1994) Biochem. Biophys. Res. Commun., 198 , 16-24.
[88] Morishita, R.; Gibbons, G.H.; Ellison, K.E.; Nakajima, M.; von der Leyen, H.; Zhang, L.;
Kaneda, Y.; Ogihara, T. and Dzau, V.J. (1994) J. Clin. Invest., 93 , 1458-1464.
[89] Morishita, R.; Gibbons, G.H.; Ellison, K.E.; Nakajima, M.; Zhang, L.; Kaneda, Y.;
Ogihara, T. and Dzau, V.J. (1993) Proc. Natl. Acad. Sci. USA., 90 , 8474-8478.
[90] Morishita, R.; Gibbons, G.H.; Kaneda, Y.; Ogihara, T. and Dzau, V.J. (1994) Gene, 149 ,
13-19.
[91] Zhu, N.L.; Wu, L.; Liu, P.X.; Gordon, E.M.; Anderson, W.F.; Starnes, V.A. and Hall, F.L.
(1997) Circulation, 96 , 628-635.
[92] Mann, M.; Gibbons, G.H.; Kernoff, R.S.; Diet, F.P.; Tsao, P.S.; Cooke, J.P.; Kaneda, Y. and Dzau, V.J. (1995) Proc. Natl. Acad. Sci. USA, 92 , 4502-4506.
32
[93] Suzuki, J.-I.; Isobe, M.; Morishita, R.; Aoki, M.; Horie, S.; Okubo, Y.; Kaneda, Y.; Sawa,
Y.; Matsuda, H.; Ogihara, T. and Sekiguchi, M. (1997) Nat. Med., 3 , 900-903.
[94] Shintani, M.; Okazaki, A.; Masuda, T.; Kawada, M.; Ishizuka, M.; Doki, Y.; Weinstein,
I.B. and Imoto, M. (2002) Anticancer Res., 22 , 639-647.
[95] Zhou, P.; Jiang, W.; Zhang, Y.J.; Kahn, S.M.; Schieren, I.; Santella, R.M. and Weinstein,
I.B. (1995) Oncogene, 11 , 571-580.
[96] Arber, N.; Doki, Y.; Han, E.K.; Sgambato, A.; Zhou, P.; Kim, N.H.; Delohery, T.; Klein,
M.G.; Holt, P.R. and Weinstein, I.B. (1997) Cancer Res., 57 , 1569-1574.
[97] Kornmann, M.; Arber, N. and Korc, M. (1998) J. Clin. Invest., 101 , 344-352.
[98] Lee, R.J.; Albanese, C.; Fu, M.; D'Amico, M.; Lin, B.; Watanabe, G.; Haines, G.K., 3rd;
Siegel, P.M.; Hung, M.C.; Yarden, Y.; Horowitz, J.M.; Muller, W.J. and Pestell, R.G.
(2000) Mol. Cell Biol., 20 , 672-683.
[99] Rieber, M. and Rieber, M.S. (1999) Cell Death Differ., 6 , 1209-1215.
[100] Sauter, E.R.; Nesbit, M.; Litwin, S.; Klein-Szanto, A.J.; Cheffetz, S. and Herlyn, M.
(1999) Cancer Res., 59 , 4876-4881.
[101] Sauter, E.R.; Herlyn, M.; Liu, S.C.; Litwin, S. and Ridge, J.A. (2000) Clin. Cancer Res.,
6 , 654-660.
[102] Sauter, E.R.; Yeo, U.C.; von Stemm, A.; Zhu, W.; Litwin, S.; Tichansky, D.S.; Pistritto,
G.; Nesbit, M.; Pinkel, D.; Herlyn, M. and Bastian, B.C. (2002) Cancer Res., 62 , 3200-
3206.
[103] Uto, H.; Ido, A.; Moriuchi, A.; Onaga, Y.; Nagata, K.; Onaga, M.; Tahara, Y.; Hori, T.;
Hirono, S.; Hayashi, K. and Tsubouchi, H. (2001) Cancer Res., 61 , 4779-4783.
[104] Skotzko, M.; Wu, L.; Anderson, W.F.; Gordon, E.M. and Hall, F.L. (1995) Cancer Res.,
55 , 5493-5498.
[105] Chen, D.S.; Zhu, N.L.; Hung, G.; Skotzko, M.J.; Hinton, D.R.; Tolo, V.; Hall, F.L.;
Anderson, W.F. and Gordon, E.M. (1997) Hum. Gene Ther., 8 , 1667-1674.
[106] Chang, M.W.; Barr, E.; Lu, M.M.; Barton, K. and Leiden, J.M. (1995) J. Clin. Invest., 96 ,
2260-2268.
[107] Ueno, H.; Masuda, S.; SNishio, S.; Li, J.J.; Yamamoto, H. and Takeshita, A. (1997) Ann.
N. Y. Acad. Sci., 811 , 401-411.
[108] Yang, Z.-Y.; Simari, R.D.; Perkins, N.D.; San, H.; Gordon, D.; Nabel, G.J. and Nabel,
E.G. (1996) Proc. Natl. Acad. Sci. USA, 93 , 7905-7910.
[109] Chen, D.; Krasinski, K.; Chen, D.; Sylvester, A.; Chen, J.; Nisen, P.D. and Andrés, V.
(1997) J. Clin. Invest., 99 , 2334-2341.
[110] Tanner, F.C.; Boehm, M.; Akyürek, L.M.; San, H.; Yang, Z.-Y.; Tashiro, J.; Nabel, G.J.
33
and Nabel, E.G. (2000) Circulation, 101 , 2022-2025.
[111] Condorelli, G.; Aycock, J.K.; Frati, G. and Napoli, C. (2001) FASEB J., 15 , 2162-2170.
[112] Bai, H.; Morishita, R.; Kida, I.; Yamakawa, T.; Zhang, W.; Aoki, M.; Matsushita, H.;
Noda, A.; Nagai, R.; Kaneda, I.; Higaki, J.; Ogihara, T.; Sawa, Y. and Matsuda, H. (1998)
Gene Ther., 5 , 761-769.
[113] Frizelle, S.P.; Grim, J.; Zhou, J.; Gupta, P.; Curiel, D.T.; Geradts, J. and Kratzke, R.A.
(1998) Oncogene, 16 , 3087-3095.
[114] Chen, J.; Willingham, T.; Shuford, M.; Bruce, D.; Rushing, E.; Smith, Y. and Nisen, P.D.
(1996) Oncogene, 13 , 1395-1403.
[115] Chen, J.; Willingham, T.; Shuford, M. and Nisen, P.D. (1996) J. Clin. Invest., 97 , 1983-
1988.
[116] Yang, Z.Y.; Perkins, N.D.; Ohno, T.; Nabel, E.G. and Nabel, G.J. (1995) Nat. Med., 1 ,
1052-1056.
[117] Hsiao, M.; Tse, V.; Carmel, J.; Costanzi, E.; Strauss, B.; Haas, M. and Silverberg, G.D.
(1997) Biochem. Biophys. Res. Commun., 233 , 329-335.
[118] Hung, K.S.; Hong, C.Y.; Lee, J.; Lin, S.K.; Huang, S.C.; Wang, T.M.; Tse, V.; Sliverberg,
G.D.; Weng, S.C. and Hsiao, M. (2000) Biochem. Biophys. Res. Commun., 269 , 718-725.
[119] Wang, T.J.; Huang, M.S.; Hong, C.Y.; Tse, V.; Silverberg, G.D. and Hsiao, M. (2001)
Biochem. Biophys. Res. Commun., 287 , 173-180.
[120] Schreiber, M.; Muller, W.J.; Singh, G. and Graham, F.L. (1999) Oncogene, 18 , 1663-
1676.
[121] Craig, C.; Wersto, R.; Kim, M.; Ohri, E.; Li, Z.; Katayose, D.; Lee, S.J.; Trepel, J.;
Cowan, K. and Seth, P. (1997) Oncogene, 14 , 2283-2289.
[122] Ohno, T.; Yang, Z.; Ling, X.; Jaffe, M.; Nabel, E.G.; Normolle, D. and Nabel, G.J. (1997)
Gene Ther., 4 , 361-366.
[123] Sandig, V.; Brand, K.; Herwig, S.; Lukas, J.; Bartek, J. and Strauss, M. (1997) Nat. Med.,
3 , 313-319.
[124] Ghaneh, P.; Greenhalf, W.; Humphreys, M.; Wilson, D.; Zumstein, L.; Lemoine, N.R. and
Neoptolemos, J.P. (2001) Gene Ther., 8 , 199-208.
[125] Adachi, Y.; Chandrasekar, N.; Kin, Y.; Lakka, S.S.; Mohanam, S.; Yanamandra, N.;
Mohan, P.M.; Fuller, G.N.; Fang, B.; Fueyo, J.; Dinh, D.H.; Olivero, W.C.; Tamiya, T.;
Ohmoto, T.; Kyritsis, A.P. and Rao, J.S. (2002) Oncogene, 21 , 87-95.
[126] Tian, H.; Wittmack, E.K. and Jorgensen, T.J. (2000) Cancer Res., 60 , 679-684.
[127] Achenbach, T.V.; Muller, R. and Slater, E.P. (2000) Clin. Cancer Res., 6 , 3006-3014.
[128] Sgambato, A.; Zhang, Y.J.; Ciaparrone, M.; Soh, J.W.; Cittadini, A.; Santella, R.M. and
34
Weinstein, I.B. (1998) Cancer Res., 58 , 3448-3454.
[129] Yang, H.Y.; Shao, R.; Hung, M.C. and Lee, M.H. (2001) Oncogene, 20 , 3695-3702.
[130] Liu, X.; Tian, P.; Yu, Y.; Yao, M.; Cao, X. and Gu, J. (2002) Cancer Gene Ther., 9 , 100-
108.
[131] Patel, S.D.; Tran, A.C.; Ge, Y.; Moskalenko, M.; Tsui, L.; Banik, G.; Tom, W.; Scott, M.;
Chen, L.; Van Roey, M.; Rivkin, M.; Mendez, M.; Gyuris, J. and McArthur, J.G. (2000)
Mol. Ther., 2 , 161-169.
[132] Lamphere, L.; Tsui, L.; Wick, S.; Nakano, T.; Kilinski, L.; Finer, M.; McArthur, J. and
Gyuris, J. (2000) J. Mol. Med., 78 , 451-459.
[133] McArthur, J.G.; Qian, H.; Citron, D.; Banik, G.G.; Lamphere, L.; Gyuris, J.; Tsui, L. and
George, S.E. (2001) Mol. Ther., 3 , 8-13.
[134] Senderowicz, A.M. (1999) Invest. New Drugs, 17 , 313-320.
[135] Zhai, S.; Senderowicz, A.M.; Sausville, E.A. and Figg, W.D. (2002) Ann. Pharmacother.,
36 , 905-911.
[136] Klasa, R.J.; List, A.F. and Cheson, B.D. (2001) Hematology (Am. Soc. Hematol. Educ.
Program) , 443-462.
[137] Senderowicz, A.M.; Headlee, D.; Stinson, S.F.; Lush, R.M.; Kalil, N.; Villalba, L.; Hill,
K.; Steinberg, S.M.; Figg, W.D.; Tompkins, A.; Arbuck, S.G. and Sausville, E.A. (1998)
J. Clin. Oncol., 16 , 2986-2999.
[138] Tan, A.R.; Headlee, D.; Messmann, R.; Sausville, E.A.; Arbuck, S.G.; Murgo, A.J.;
Melillo, G.; Zhai, S.; Figg, W.D.; Swain, S.M. and Senderowicz, A.M. (2002) J. Clin.
Oncol., 20 , 4074-4082.
[139] Stadler, W.M.; Vogelzang, N.J.; Amato, R.; Sosman, J.; Taber, D.; Liebowitz, D. and
Vokes, E.E. (2000) J. Clin. Oncol., 18 , 371-375.
[140] Shapiro, G.I.; Supko, J.G.; Patterson, A.; Lynch, C.; Lucca, J.; Zacarola, P.F.;
Muzikansky, A.; Wright, J.J.; Lynch, T.J., Jr. and Rollins, B.J. (2001) Clin. Cancer Res.,
7 , 1590-1599.
[141] Schwartz, G.K.; Ilson, D.; Saltz, L.; O'Reilly, E.; Tong, W.; Maslak, P.; Werner, J.;
Perkins, P.; Stoltz, M. and Kelsen, D. (2001) J. Clin. Oncol., 19 , 1985-1992.
[142] Schwartz, G.K.; O'Reilly, E.; Ilson, D.; Saltz, L.; Sharma, S.; Tong, W.; Maslak, P.;
Stoltz, M.; Eden, L.; Perkins, P.; Endres, S.; Barazzoul, J.; Spriggs, D. and Kelsen, D.
(2002) J. Clin. Oncol., 20 , 2157-2170.
[143] Sausville, E.A.; Arbuck, S.G.; Messmann, R.; Headlee, D.; Bauer, K.S.; Lush, R.M.;
Murgo, A.; Figg, W.D.; Lahusen, T.; Jaken, S.; Jing, X.; Roberge, M.; Fuse, E.;
Kuwabara, T. and Senderowicz, A.M. (2001) J. Clin. Oncol., 19 , 2319-2333.
[144] Wilson, W.H.; Sorbara, L.; Figg, W.D.; Mont, E.K.; Sausville, E.; Warren, K.E.; Balis,
35
F.M.; Bauer, K.; Raffeld, M.; Senderowicz, A.M. and Monks, A. (2000) Clin. Cancer
Res., 6 , 415-421.
[145] Sausville, E.A.; Lush, R.D.; Headlee, D.; Smith, A.C.; Figg, W.D.; Arbuck, S.G.;
Senderowicz, A.M.; Fuse, E.; Tanii, H.; Kuwabara, T. and Kobayashi, S. (1998) Cancer
Chemother. Pharmacol., 42 , S54-59.
[146] Fuse, E.; Tanii, H.; Kurata, N.; Kobayashi, H.; Shimada, Y.; Tamura, T.; Sasaki, Y.;
Tanigawara, Y.; Lush, R.D.; Headlee, D.; Figg, W.D.; Arbuck, S.G.; Senderowicz, A.M.;
Sausville, E.A.; Akinaga, S.; Kuwabara, T. and Kobayashi, S. (1998) Cancer Res., 58 ,
3248-3253.
[147] Califf, R.M.; Fortin, D.F.; Frid, D.J.; Harlan, W.R.; Ohman, E.M.; Bengtson, J.R.;
Nelson, C.L.; Tcheng, J.E.; Mark, D.B. and Stack, R.S. (1991) J. Am. Coll. Cardiol., 17 ,
2B-13B.
[148] Franklin, S.M. and Faxon, D.P. (1993) Coronary Artery Dis., 4 , 232-242.
[149] Popma, J.J.; Califf, R.M. and Topol, E.J. (1991) Circulation, 84 , 1426-1436.
[150] Chan, A.W.; Chew, D.P. and Lincoff, A.M. (2001) Curr. Interv. Cardiol. Rep., 3 , 149-
155.
[151] Marx, S.O.; Jayaraman, T.; Go, L.O. and Marks, A.R. (1995) Circ. Res., 76 , 412-417.
[152] Poon, M.; Marx, S.O.; Gallo, R.; Badimon, J.J.; Taubman, M.B. and Marks, A.R. (1996)
J. Clin. Invest., 98 , 2277-2283.
[153] Luo, Y.; Marx, S.O.; Kiyokawa, H.; Koff, A.; Massague, J. and Marks, A.R. (1996) Mol.
Cell. Biol., 16 , 6744-6751.
[154] Sun, J.; Marx, S.O.; Chen, H.-J.; Poon, M.; Marks, A.R. and Rabbani, L.E. (2001)
Circulation, 103 , 2967-2972.
[155] Guba, M.; von Breitenbuch, P.; Steinbauer, M.; Koehl, G.; Flegel, S.; Hornung, M.;
Bruns, C.J.; Zuelke, C.; Farkas, S.; Anthuber, M.; Jauch, K.W. and Geissler, E.K. (2002)
Nat. Med., 8 , 128-135.
[156] Burke, S.E.; Lubbers, N.L.; Chen, Y.W.; Hsieh, G.C.; Mollison, K.W.; Luly, J.R. and
Wegner, C.D. (1999) J. Cardiovasc. Pharmacol., 33 , 829-835.
[157] Gallo, R.; Padurean, A.; Jayaraman, T.; Marx, S.; Rogue, M.; Adelman, S.; Chesebro, J.;
Fallon, J.; Fuster, V.; Marks, A. and Badimón, J.J. (1999)
Circulation, 99 , 2164-2170.
[158] Gregory, C.R.; Huie, P.; Billingham, M.E. and Morris, R.E. (1993) Transplantation, 55 ,
1409-1418.
[159] Gregory, C.R.; Huie, P.; Shorthouse, R.; Wang, J.; Rowan, R.; Billingham, M.E. and
Morris, R.E. (1993) Transplant. Proc., 25 , 120-121.
[160] Meiser, B.M.; Billingham, M.E. and Morris, R.E. (1991) Lancet, 338 , 1297-1298.
36
[161] Poston, R.S.; Billingham, M.; Hoyt, E.G.; Pollard, J.; Shorthouse, R.; Morris, R.E. and
Robbins, R.C. (1999) Circulation, 100 , 67-74.
[162] Roque, M.; Reis, E.D.; Cordon-Cardo, C.; Taubman, M.B.; Fallon, J.T.; Fuster, V. and
Badimon, J.J. (2001) Lab. Invest., 81 , 895-903.
[163] Suzuki, T.; Kopia, G.; Hayashi, S.; Bailey, L.R.; Llanos, G.; Wilensky, R.; Klugherz,
B.D.; Papandreou, G.; Narayan, P.; Leon, M.B.; Yeung, A.C.; Tio, F.; Tsao, P.S.;
Falotico, R. and Carter, A.J. (2001) Circulation, 104 , 1188-1193.
[164] Sousa, J.E.; Costa, M.A.; Abizaid, A.; Abizaid, A.S.; Feres, F.; Pinto, I.M.; Seixas, A.C.;
Staico, R.; Mattos, L.A.; Sousa, A.G.; Falotico, R.; Jaeger, J.; Popma, J.J. and Serruys,
P.W. (2001) Circulation, 103 , 192-195.
[165] Morice, M.C.; Serruys, P.W.; Sousa, J.E.; Fajadet, J.; Ban Hayashi, E.; Perin, M.;
Colombo, A.; Schuler, G.; Barragan, P.; Guagliumi, G.; Molnar, F. and Falotico, R.
(2002) N. Engl. J. Med., 346 , 1773-1780.
[166] Mann, M.J.; Gibbons, G.H.; Tsao, P.S.; von der Leyen, H.E.; Cooke, J.P.; Buitrago, R.;
Kernoff, R. and Dzau, V.J. (1997) J. Clin. Invest., 99 , 1295-1301.
[167] Morishita, R.; Gibbons, G.H.; Horiuchi, M.; Ellison, K.E.; Nakajima, M.; Zhang, L.;
Kaneda, Y.; Ogihara, T. and Dzau, V.J. (1995) Proc. Natl. Acad. Sci. USA, 92 , 5855-
5859.
[168] Mann, M.J.; Whittemore, A.D.; Donaldson, M.C.; Belkin, M.; Conte, M.S.; Polak, J.F.;
Orav, E.J.; Ehsan, A.; Dell'Acqua, G. and Dzau, V.J. (1999) Lancet, 354 , 1493-1498.
[169] Mangi, A.A. and Dzau, V.J. (2001) Ann. Med., 33 , 153-155.
[170] Sedlacek, H.H. (2001) Crit. Rev. Oncol. Hematol., 38 , 139-170.
[171] Iseki, H.; Ko, T.C.; Xue, X.Y.; Seapan, A.; Hellmich, M.R. and Townsend, C.M., Jr.
(1997) Surgery, 122 , 187-194.
[172] Iseki, H.; Ko, T.C.; Xue, X.Y.; Seapan, A. and Townsend, C.M., Jr. (1998) J.
Gastrointest. Surg., 2 , 36-43.
[173] Buquet-Fagot, C.; Lallemand, F.; Montagne, M.N. and Mester, J. (1997) Anticancer
Drugs, 8 , 623-631.
[174] Alessi, F.; Quarta, S.; Savio, M.; Riva, F.; Rossi, L.; Stivala, L.A.; Scovassi, A.I.; Meijer,
L. and Prosperi, E. (1998) Exp. Cell Res., 245 , 8-18.
[175] Yakisich, J.S.; Boethius, J.; Lindblom, I.O.; Wallstedt, L.; Vargas, V.I.; Siden, A. and
Cruz, M.H. (1999) Neuroreport, 10 , 2563-2567.
[176] Vitali, L.; Yakisich, J.S.; Vita, M.F.; Fernandez, A.; Settembrini, L.; Siden, A.; Cruz, M.;
Carminatti, H.; Casas, O. and Idoyaga Vargas, V. (2002) Cancer Lett., 180 , 7-12.
[177] Somerville, L. and Cory, J.G. (2000) Anticancer Res., 20 , 3347-3355.
37
[178] Mgbonyebi, O.P.; Russo, J. and Russo, I.H. (1999) Cancer Res., 59 , 1903-1910.
[179] Mgbonyebi, O.P.; Russo, J. and Russo, I.H. (1998) Anticancer Res., 18 , 751-755.
[180] Mihara, M.; Shintani, S.; Kiyota, A.; Matsumura, T. and Wong, D.T. (2002) Int. J.
Oncol., 21 , 95-101.
[181] Courage, C.; Snowden, R. and Gescher, A. (1996) Br. J. Cancer, 74 , 1199-1205.
[182] Couldwell, W.T.; Uhm, J.H.; Antel, J.P. and Yong, V.W. (1991) Neurosurgery, 29 , 880-
886.
[183] Meyer, T.; Regenass, U.; Fabbro, D.; Alteri, E.; Rosel, J.; Muller, M.; Caravatti, G. and
Matter, A. (1989) Int. J. Cancer, 43 , 851-856.
[184] Kwon, T.K.; Buchholz, M.A.; Chrest, F.J. and Nordin, A.A. (1996) Cell Growth Differ.,
7 , 1305-1313.
[185] Shimizu, T.; Takahashi, N.; Tachibana, K. and Takeda, K. (2001) Anticancer Res., 21 ,
893-898.
[186] Traganos, F.; Gong, J.; Ardelt, B. and Darzynkiewicz, Z. (1994) J. Cell Physiol., 158 ,
535-544.
[187] Harkin, S.T.; Cohen, G.M. and Gescher, A. (1998) Mol. Pharmacol., 54 , 663-670.
[188] Narita, Y.; Asai, A.; Kuchino, Y. and Kirino, T. (2000) Cancer Chemother. Pharmacol.,
45 , 149-156.
[189] Park, J.A.; Kim, K.W.; Kim, S.I. and Lee, S.K. (1998) Eur. J. Biochem., 257 , 242-248.
[190] Chen, X.; Lowe, M. and Keyomarsi, K. (1999) Oncogene, 18 , 5691-5702.
[191] Blagosklonny, M.V.; Dixon, S.C.; Robey, R. and Figg, W.D. (2001) Int. J. Oncol., 18 ,
697-704.
[192] Kohn, E.A.; Ruth, N.D.; Brown, M.K.; Livingstone, M. and Eastman, A. (2002) J. Biol.
Chem., 277 , 26553-26564.
[193] Seynaeve, C.M.; Stetler-Stevenson, M.; Sebers, S.; Kaur, G.; Sausville, E.A. and
Worland, P.J. (1993) Cancer Res., 53 , 2081-2086.
[194] Witham, T.F.; Erff, M.L.; Okada, H.; Chambers, W.H. and Pollack, I.F. (2002)
Neurosurgery, 50 , 1327-1334.
[195] Sugiyama, K.; Akiyama, T.; Shimizu, M.; Tamaoki, T.; Courage, C.; Gescher, A. and
Akinaga, S. (1999) Cancer Res., 59 , 4406-4412.
[196] Shao, R.G.; Shimizu, T. and Pommier, Y. (1997) Exp. Cell Res., 234 , 388-397.
[197] Fukumoto, H.; Tamura, T.; Kamiya, Y.; Usuda, J.; Suzuki, T.; Kanzawa, F.; Kuh, H.J.;
Ohe, Y.; Saijo, N. and Nishio, K. (1999) Invest. New Drugs, 17 , 335-341.
38
[198] Byrd, J.C.; Shinn, C.; Willis, C.R.; Flinn, I.W.; Lehman, T.; Sausville, E.; Lucas, D. and
Grever, M.R. (2001) Exp. Hematol., 29 , 703-708.
[199] Nieves-Neira, W. and Pommier, Y. (1999) Int. J. Cancer, 82 , 396-404.
[200] Bredel, M.; Pollack, I.F.; Freund, J.M.; Rusnak, J. and Lazo, J.S. (1999) J. Neurooncol.,
41 , 9-20.
[201] Senderowicz, A.M. (2001) Leukemia, 15 , 1-9.
[202] Somerville, L. and Cory, J.G. (2000) Int. J. Oncol., 17 , 797-803.
[203] Baltuch, G.H. and Yong, V.W. (1996) Brain Res., 710 , 143-149.
[204] Ganeshaguru, K.; Wickremasinghe, R.G.; Jones, D.T.; Gordon, M.; Hart, S.M.; Virchis,
A.E.; Prentice, H.G.; Hoffbrand, A.V.; Man, A.; Champain, K.; Csermak, K. and Mehta,
A.B. (2002) Haematologica, 87 , 167-176.
[205] Begemann, M.; Kashimawo, S.A.; Choi, Y.A.; Kim, S.; Christiansen, K.M.; Duigou, G.;
Mueller, M.; Schieren, I.; Ghosh, S.; Fabbro, D.; Lampen, N.M.; Heitjan, D.F.; Schiff,
P.B.; Bruce, J.N. and Weinstein, I.B. (1996) Clin Cancer Res, 2 , 1017-1030.
[206] Damiens, E.; Baratte, B.; Marie, D.; Eisenbrand, G. and Meijer, L. (2001) Oncogene, 20 ,
3786-3797.
[207] Marko, D.; Schatzle, S.; Friedel, A.; Genzlinger, A.; Zankl, H.; Meijer, L. and Eisenbrand,
G. (2001) Br. J. Cancer, 84 , 283-289.
[208] Semenov, I.; Akyuz, C.; Roginskaya, V.; Chauhan, D. and Corey, S.J. (2002) Leuk. Res.,
26 , 271-280.
[209] Shapiro, G.I.; Koestner, D.A.; Matranga, C.B. and Rollins, B.J. (1999) Clin. Cancer Res.,
5 , 2925-2938.
[210] Park, D.S.; Farinelli, S.E. and Greene, L.A. (1996) J. Biol. Chem., 271 , 8161-8169.
[211] Parker, B.W.; Kaur, G.; Nieves-Neira, W.; Taimi, M.; Kohlhagen, G.; Shimizu, T.;
Losiewicz, M.D.; Pommier, Y.; Sausville, E.A. and Senderowicz, A.M. (1998) Blood, 91 ,
458-465.
[212] Bible, K.C. and Kaufmann, S.H. (1996) Cancer Res., 56 , 4856-4861.
[213] Brusselbach, S.; Nettelbeck, D.M.; Sedlacek, H.H. and Muller, R. (1998) Int. J. Cancer,
77 , 146-152.
[214] Pepper, C.; Thomas, A.; Hoy, T.; Fegan, C. and Bentley, P. (2001) Br. J. Haematol., 114 ,
70-77.
[215] Li, Y.; Chinni, S.R.; Senderowicz, A.M. and Sarkar, F.H. (2000) Int. J. Oncol., 17 , 755-
759.
[216] Smith, V.; Raynaud, F.; Workman, P. and Kelland, L.R. (2001) Mol. Pharmacol., 60 ,
885-893.
39
[217] Konig, A.; Schwartz, G.K.; Mohammad, R.M.; Al-Katib, A. and Gabrilove, J.L. (1997)
Blood, 90 , 4307-4312.
[218] Byrd, J.C.; Shinn, C.; Waselenko, J.K.; Fuchs, E.J.; Lehman, T.A.; Nguyen, P.L.; Flinn,
I.W.; Diehl, L.F.; Sausville, E. and Grever, M.R. (1998) Blood, 92 , 3804-3816.
[219] Yamamoto, H.; Monden, T.; Miyoshi, H.; Izawa, H.; Ikeda, K.; Tsujie, M.; Ohnishi, T.;
Sekimoto, M.; Tomita, N. and Monden, M. (1998) Int. J. Oncol., 13 , 233-239.
[220] Wada, M.; Hosotani, R.; Lee, J.U.; Doi, R.; Koshiba, T.; Fujimoto, K.; Miyamoto, Y.;
Tsuji, S.; Nakajima, S.; Okuyama, A. and Imamura, M. (1998) Anticancer Res., 18 , 2559-
2566.
[221] Bhattacharjee, R.N.; Banks, G.C.; Trotter, K.W.; Lee, H.L. and Archer, T.K. (2001) Mol.
Cell Biol., 21 , 5417-5425.
[222] Patel, V.; Lahusen, T.; Leethanakul, C.; Igishi, T.; Kremer, M.; Quintanilla-Martinez, L.;
Ensley, J.; Sausville, E.; Gutkind, J. and Senderowicz, A. (2002) Clin. Cancer Res., 11 ,
3549-3560.
[223] Wang, G.L.; Lo, K.W.; Tsang, K.S.; Chung, N.Y.; Tsang, Y.S.; Cheung, S.T.; Lee, J.C. and Huang, D.P. (1999) Br. J. Cancer, 81 , 1122-1126.
[224] Jin, X.; Nguyen, D.; Zhang, W.W.; Kyritsis, A.P. and Roth, J.A. (1995) Cancer Res., 55 ,
3250-3253.
[225] Steiner, M.S.; Zhang, Y.; Farooq, F.; Lerner, J.; Wang, Y. and Lu, Y. (2000) Cancer Gene
Ther., 7 , 360-372.
[226] Tamm, I.; Schumacher, A.; Karawajew, L.; Ruppert, V.; Arnold, W.; Nussler, A.K.;
Neuhaus, P.; Dorken, B. and Wolff, G. (2002) Cancer Gene Ther., 9 , 641-650.
[227] Campbell, I.; Magliocco, A.; Moyana, T.; Zheng, C. and Xiang, J. (2000) Cancer Gene
Ther., 7 , 1270-1278.
[228] Shibata, M.A.; Yoshidome, K.; Shibata, E.; Jorcyk, C.L. and Green, J.E. (2001) Cancer
Gene Ther., 8 , 23-35.
[229] Chen, Y.Q.; Cipriano, S.C.; Arenkiel, J.M. and Miller, F.R. (1995) Cancer Res., 55 , 4536-
4539.
[230] Joshi, U.S.; Chen, Y.Q.; Kalemkerian, G.P.; Adil, M.R.; Kraut, M. and Sarkar, F.H.
(1998) Cancer Gene Ther., 5 , 183-191.
[231] Tsao, Y.P.; Huang, S.J.; Chang, J.L.; Hsieh, J.T.; Pong, R.C. and Chen, S.L. (1999) J.
Virol., 73 , 4983-4990.
[232] Eastham, J.A.; Hall, S.J.; Sehgal, I.; Wang, J.; Timme, T.L.; Yang, G.; Connell-Crowley,
L.; Elledge, S.J.; Zhang, W.W.; Harper, J.W. and et al. (1995) Cancer Res., 55 , 5151-
5155.
[233] Park, K.H.; Seol, J.Y.; Yoo, C.G.; Kim, Y.W.; Han, S.K.; Lee, E.H.; Kim, C.M.; Shim,
40
Y.S. and Lee, C.T. (2001) Lung Cancer, 31 , 149-155.
[234] Katner, A.L.; Gootam, P.; Hoang, Q.B.; Gnarra, J.R. and Rayford, W. (2002) J. Urol.,
168 , 766-773.
41
FIGURE 1
CDK1 Cyclin A
CDK1 Cyclin B
CDK2 Cyclin A
S CDK2 Cyclin E
G2
G1
CDK3 Cyclin E?
Mitosis
CDK
Cyclin
Active
CKIs
Cip / Kip p21 Cip1 p27 Kip1 p57 Kip2
CDK4,6 Cyclin D1,2,3
CKI
CDK
Cyclin
CKI
Inactive
Ink4 p15 Ink4b p16 Ink4a p18 Ink4c p19 Ink4d
42