Orofacial pain I
advertisement

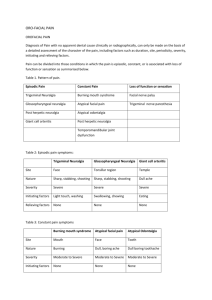
OROFACIAL PAIN-1 DEFINITION According to International association for the study of pain (IASP) pain is defined as :- “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” Dr.S.Karthiga Kannan Porfessor Oral Medicine & Radiology SPECIFIC LEARNING OBJECTIVES • To know the pathophysiology of orofacial pain • To know the classification of orofacial pain • To know the clinical characteristics treatment of – Trigeminal Neuralgia (TN) – Glossopharyngeal Neuralgia (GN) – Post Herpetic Neuralgia (PHN) and PAIN PATHWAYS CLASSIFICATION OF OROFACIAL PAIN LOCAL DISEASES ☞ Dental causes Pulpal Pulpitis Dentin hypersensitivity Cracked tooth syndrome Apical periodontitis Periapical Abcess Gingivitis/Periodontitis ANUG Pericoronitis /pericoronal abcess Oral ulcers Oral Cancers ☞ ENT diseases like sinusitis, otitis media Pharygitis, ☞ Eye diseases – Conjunctivitis CHORNIC OROFACIAL PAIN ☞Musculoskeletal diseases Temporomandibular disorder(TMD) Myofacial pain dysfunction syndrome (MPDS) Eagle’s syndrome ☞ Vascular diseases Migraine Cluster headach Temporal or Giant cell arteritis ☞ Neurologic disorders Trigeminal neuralgia Glossopharyngeal neuralgia Post herpetic neuralgia ☞ Psychogenic Pain Atypical facial pain Burning mouth syndrome Atypical odontalgia Episodic pain ☛ Trigeminal neuralgia ☛ Glossopharyngeal neuralgia ☛ Post-herpetic neuralgia ☛ Giant cell arteritis Pattern of pain Constant pain ☛ Burning mouth syndrome ☛ Atypical facial pain ☛ Atypical odontalgia ☛ Post-herpetic neuralgia ☛ Temporomandibular joint dysfunction Loss of function or sensation ☛ Facial nerve palsy ☛ Trigeminal nerve paresthesia Category rating scale Numeric rating scale TRIGEMINAL NEURALGIA (TN) Synonym – ☛ Tic douloureux, ☛ Fothergill’s neuralgia Types ☛ Classical TN (85%) – caused by compression of sensory root by vascular anurysm. ☛ Secondary TN – caused by tumors, viralinfection, trauma, and multiple sclerosis. ☛ Is the most common of the cranial neuralgias ☛ Age predilection - older than 50 years of age. CLINICAL FEATURES ☛ NATURE – Unilateral, Paroxysmal (occurs in episodes) awakes from sleep. ☛ QUALITY – Sharp, stabbing,electric piercing. shock like, ☛ INTESITY – Severe ☛ AGGRAVATING FACTORS – shaving, eating, washing face, speaking, exposure to wind. ☛ DURATION – from seconds to 2 minutes. ☛ SITE – Maillary, mandibular, Opthalmic dermatome in decending order, usually right side. Clinical features ☛ TRIGGER ZONE - Pain in TN is precipitated by a light touch on a “trigger zone”(Allodynia) present on the skin or mucosa within the distribution of the involved nerve branch. ☛ Common sites for trigger zones include the nasolabial fold and the corner of the lip. ☛ REFRACTORY PERIOD - Just after an attack, touching the trigger zone will not precipitate pain. ☛ PAIN BEHAVIOR – spasm of ipsilateral facial muscles, Patient protects / cover that area. DIFFERENTIAL DIAGNOSIS ☛ Cracked tooth Syndrome ☛ TN pain will be triggered by touching the soft tissue around the trigger zone, whereas pressure on the tooth is required to cause pain from a cracked tooth. INVESTIGATIONS ☛Local anesthetic blocks, which temporarily eliminate the trigger zone, may also be helpful in diagnosis. ☛ CT scan,MRI of the brain is indicated to rule out tumors, multiple sclerosis. ☛ Magnetic resonance tomographic angiography (MRTA) for vascular lesions. MANAGEMENT OF TN MEDICAL ☛ Carbamazepine – 100 -200 mg / twice a day can be increased slowly ☛ Baclofen – 5-10mg thrice a day ☛ Oxcarbamazepine – 300mg/ thrice a day ☛ Gabapentin – 200-300mg/twice a day ☛ Phenytoin – 300 -600mg /day ☛ Lamotrigine 25mg/1-2 time perday SURGICAL ☛ Pheripheral Neurectomy ☛ Percutaneous Trigeminal Rhizotomy – TN ganglion level -Glycerol injection -Ballon compression -Radiofrequency rhizolysis ☛ Microvascular decompression (MVD) – Brainstem level ☛ Gamma knife stereotactic radiosurgery (GKS) – 70-90 Gy radiation. GLOSSOPHARYNGEAL NEURALGIA (GN) ☛ ETIOLOGY – compression of nerve root by blood vessel or anurysm. ☛ TYPES ☛Pharyngeal GN Pharynx, posterior tongue are involved and radiate to ear, eyes, nose, maxilla, shoulder and even tip of tongue. ☛Tymphanic GN Ear pain radiating to pharynx ☛ NATURE OF PAIN -Paroxysmal, unilateral, moderate to severe pain ☛ QUALITY – Sharp, stabbing, shooting or lancinating. ☛ DURATION – Fraction of second to 2 minutes ☛ FREQUENCY – 5-12 every hour and may occur in cluster lasting for weeks to months. ☛ TRIGGER POINTS - Tonsillar region, posterior pharynx. ☛ AGGRAVATING FACTORS – swallowing, chewing, talking, coughing and yawning, sneezing and rubbing ear. ☛ COMPLICATIONS – GN may induce uncontrollable coughing, seizures, and cardiac arrythmias, bradycardia and syncope. ☛ TREATMENT ♐MEDICAL - Carbamazepin, baclofen, oxcarbazepin, gabapentin, lamotrigine and phenytoin. ♐SURGICAL – Microvacular decompression and Gamma knife stereotactic radiosurgery POST HERPETIC NEURALGIA (PHN) ☛ PHN- Pain of herpes zoster that persists three or more months. ☛ AGE – common in > 50 yrs ☛ SITE - 22% - Opthalmic nerve commonly affected. is ☛NATURE OF PAIN - Burning constant pain & superimposed flashes of pain ☛QUALITY – burning, sharp, shooting, throbbing , stabbing. ☛AGGRAVATING FACTOR – Hypo pigmented scar acts as trigger points – Allodynia. ☛ COMPLICATION - Paresthesialoss of sensation MANAGEMENT ☛ Prevention by use of varicella zoster vaccine ☛ For those with active Herpes Zoster use of antiviral drugs early in the course of the disease For those who develop PHN ☛ Topical therapy such as lidocaine. ☛ Topical application of Capsaicin , a selective c-fiber neurotoxin that deplete the substance P ☛ Acyclovir: 800 mg 5 times / day for 2 Weeks. ☛ Famcyclovir 250 mg 3 times a day ☛ Tricyclic antidepressant therapy Amitriptyline 25-100 mg daily divided doses. ☛ Systemic Corticosteroid Prednisolone - 60 mg / day for 1st week 30mg / day for for 3rd week 2nd week and 15mg / day Treatment should be started within 10days and continued for three weeks ☛ Gabapentin 200-300 mg twice daily ☛ TENS - Trans Cutaneous Electrical Nerve Stimulation ☛ Opioids, Tramadol CLINICAL CHARARECTERISTICS Trigeminal neuralgia 1.Site Face Glossopharyngeal neuralgia Throat, tonsillar region Postherpetic neuralgia Forehead,eyes – opthalmic dermatome Burning constant pain & superimposed flashes of pain 2.Nature Sharp, stabbing, shooting Sharp, stabbing, shooting 3.Severity Worst pain experienced Worst pain experienced 4.Initiating factors Light touch, washing Swallowing, chewing Allodynia – light touch 5.Relieving factors None None None Moderate to Severe Thank you