ANTERIOR PITUITARY,GROWTH HORMONE

FUNCTIONS & CONTROL
OF ANTERIOR
PITUITARY,GROWTH
HORMONE.
DR.HAROON RASHID.
OBJECTIVES
• List the hormones secreted by the anterior pituitary gland.
• Discuss Physiological actions of growth hormone.
• Outline the role of Somatomedins as mediators of
Growth Hormone actions.
• Describe the mechanisms that regulate GH production & release.
• Describe the sources,actions of somatostatin & relate it to growth hormone control.
• Correlate this knowledge to Clinical conditions related to hypo & hyper of Growth Hormone.
• Hormones
secreted by Anterior Pituitary gland.
• Growth hormone.
• Thyroid Stimulating hormone.
• Aderno Corticotropic hormone.
• Prolactin.
•
•
• Follicle Stimulating Hormone.
• Leuteinizing Hormone.
GH(=Somatotropin)
Structure:
• Polypeptide, unbranched with191AA
• Shows species specificity.
• hGH & monkey’sGH have similar biological activities in humans.
Genes for Gh
• Genes for human growth hormone, known as growth hormone 1 (somatotropin) and growth hormone 2 , are localized in the q22-24 region of chromosome 17 [4][5] and are closely related to human chorionic somatomammotropin (also known as placental lactogen ) genes. GH, human chorionic somatomammotropin, and prolactin belong to a group of homologous hormones with growth-promoting and lactogenic activity
.
Synthesis & secretion
• Somatotrophs of ant.pituitary.
• Released in pulsatile fashion.
• GHRH(of Hypothalamus)binds receptors on somatotroph(of ant.pit)then cAMP & Ca mediate the release of GH.
Plasma level & circulation
• About 2-4ng/ml.(0.2 – 1 mg/day).
• Released in pulses- 10 – 20 pulses / day.
• Level varies with age.
B=at birth
C- Childhood
P= puberty
A= Adult life
O= Old age
• Nocturnal sleep burst: 1-2hrs after sleep, accounts for 70% of secretion ( More you sleep more you grow!!).
• Circulating Gh binds with GH binding protein( is a part of receptor ).
• Half life = 20 min.
• Metabolism: Mainly in liver, also by kidneys.
GH Receptor
• Present on membrane of target cells.
• Has extracellular, transmembrane and intracellular portion.
Mechanism of action of GH
GH
Directly By IGF-I
Produced by Liver
IGF types- IGF-I( = Somatomedin C ) &
IGF-II
Mechanism of action of GH
ACTIONS
GH
On Growth & On Metabolism
• Skeletal tissue * Carbohydrate
(cartilage&bones) * Fat
• Extraskeletal * Proteins
(muscles&visceras) * minerals
Actions.
Skeletal tissue:
1. Cartilage: proliferation of chondrocytes, increased thickness of epiphyseal cartilage.
2. Bones: St. of osteoblasts, convert cartilage to bone till epiphyseal plate fuses with shaft of long bones. In adults: increases girth of bones.
Actions.
Extraskeletal tissue growth:
*St skeletal muscle growth ( not contractile unit ) = bulk without power.
* Visceral growth increases.
On metabolism
On Carbohydrate:
* Hyperglycemic:-increases gluconeogenesis(hepatic ),decresases peripheral utilization of glucose, inhibits glycolysis.
On Fat metabolism
• Gh Adipose tissue Lipolysis
• Increased FFA in circulation.This acts as energy source during hypoglycemia, fasting and stress.
On proteins
• ANABOLIC.
• Promotes protein deposition in tissues by increased uptake of AA,protein synthesis.
• Causes + ve nitrogen balance.
On minerals
• Positive balance of Calcium, phosphates,magnesium.
• Increased renal reabsorption of calcium,phospates,Na.
Other actions
• On milk production: Gh has lactogenic action.
• On erythropoiesis: stimulates erythropoiesis. Increases EP from kidney
• Stimulates growth of lymphocytes.
• Stimulates growth of genitelia.
Regulation of GH secretion
1. Hypothalamic control by release of a. GHRH b. GHIH.
2. Negative feedback control by a. Somatomedins b. GH c. GHRH
Regulation of GH secretion
Hypothalamic control by release of
GHRH
• GHRH
Factors stimulating GHRH secretion and there by increase secretion of GH:
-Hypoglycemia(through glucoreceptors)
-Emotion,exercise,physical stress(nervous)
-Sleep.
-Increased plasmaAA levels.
-Ghrelin(gh Releasing Peptide)
Hypothalamic control by release of
GHIH
• GHIH( = Somatostatin)
Blocks GHRH stimulation
Decreased GH
Factors stimulating GHIHsecretion & GH.
-Hyperglycemia
-Plasma FFA
Applied aspect
GH: Increased Secretion:1. GIGANTISM
2.ACROMEGALY
GH: Decreased secretion: DWARFISM
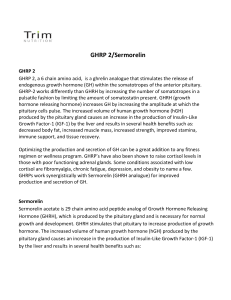
GIGANTISM
• Increased secretion of Gh in children i,.e before closure of epiphysis of long bones.
• Abnormal height(7-8 feet).=gaint.
• Large hands & feets.
• Thick lips.macrogosia.
• Gynaecomastia
• Loss of libido.
• Hyperglycemia- insulin-overactivity of beta cells& degeneration- DM
• If due to tumors- Head ache, visual defects.
Robert Wadlow , the tallest man known to have lived (2.72 metres or 8 feet 11 inches) with his father, Harold
Wadlow (1.82 metres or
6 feet 0 inches)
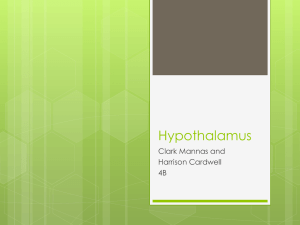
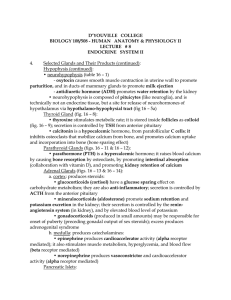
ACROMEGALY
• Increased Gh secretion in adults(after epiphyseal closure)
• Acromegalic face:Thick lips,macroglosia, thick and broadnose,PROGNATHISM.
• Acral part enlargment- hands,feets.
• Excessive growth of internal organshepato,spleeno,renomegaly.
• Poor gonadal function.
Prognathism
Brow ridge and forehead protrusion normal & acromegalic hands
Acromegalic face
DWARFISM
PITUITARY DWARF:
-Decreased Gh secretion at early age.
-Shortness of strature.
-Normal mental activity.
-Sexual maturity- may not be if associated with deficiency of Gonadotropin.
Otherwise sexual maturity present.
AFRICAN PYGMIES
• Short strature due to LACK OF GH
RECEPTORS IN TISSUES.
LARON DWARFISM
• CONGENITAL ABNORMALITY OF GH
RECEPTORS.
Housy Animal
• When pancreatectomy is done it results in
Diabetes. If hypophysectomy is done diabetes is brought under control. This shows that GH is a diabetogenic hormone.