Soft Tissue Injury and Postoperative Treatment
advertisement

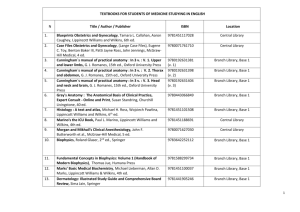
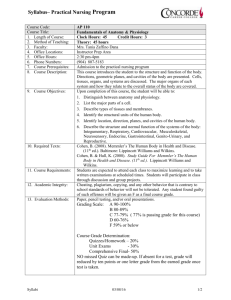
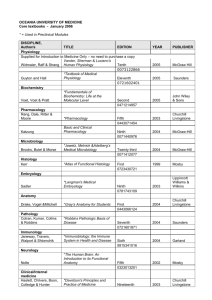
Chapter 11 Soft Tissue Injury and Postoperative Treatment Copyright 2005 Lippincott Williams & Wilkins Physiology of Connective Tissue Repair Ligaments Tendon Cartilage Respond to injury predictably Some repair variability between tissues (e.g., bone) Copyright 2005 Lippincott Williams & Wilkins Microstructure of Connective Tissues Fibers (collagen, elastin) Ground substance (glycosaminoglycans) Cellular substances (fibroblasts, fibrocytes) Function of connective tissues depends on portions of intracellular and extracellular components. Copyright 2005 Lippincott Williams & Wilkins Collagen Distribution of Joint Tissues Copyright 2005 Lippincott Williams & Wilkins Response to Loading Tensile loads – primarily resisted by collagen fibers. If tissue is elongated beyond 4%, plastic changes begin to occur (X-links begin to fail). Yield point is where increase in strain occurs w/o an increase in stress. Cyclic loading produces microstructural damage that accumulates with each loading cycle. Failure from cyclic loading = fatigue failure. Copyright 2005 Lippincott Williams & Wilkins Stress-Strain Curve Showing Elastic Limit Copyright 2005 Lippincott Williams & Wilkins Stress-Strain Curve of Cortical Bone Copyright 2005 Lippincott Williams & Wilkins Viscoelastic Properties Creep Tissue lengthens in response to a constant load. Relaxation Amount of force necessary to maintain new length decreases. Creep and relaxation allow connective tissues to adapt and function in a variety of loading conditions without being damaged. Copyright 2005 Lippincott Williams & Wilkins Phases of Healing Needed to formulate a plan of care. Allows for matching the loading capability to intervention. Understanding provides the tools to treat a variety of injury and surgical conditions. Copyright 2005 Lippincott Williams & Wilkins Phase I – Inflammatory Response Characteristics 3–5 days Palpable pain, tenderness, swelling Release of chemical substances (prostaglandins, bradykinin) Treatment Decrease pain and inflammation Maintain mobility and strength of adjacent joints and soft tissues if possible Copyright 2005 Lippincott Williams & Wilkins Repair and Regeneration (Phase II) Characteristics Treatment Up to 8 weeks New collagen forming (primarily type III) Edema is resolved during this phase Bone – Callus phase Focus on normal tissue relationships, optimal loading Changes become habitual in this stage ROM exercises and joint mobilization End of this stage – Mobility and strength base should be established Bone – Limited activity allowed Copyright 2005 Lippincott Williams & Wilkins Remodeling and Maturation (Phase III) Characteristics Treatment Deposition of type I collagen (end of phase II) Decreased synthetic activity and extracellularity Tension/resistance becomes more important in orientation of collagen Normal loading is necessary for bone remodeling Copyright 2005 Lippincott Williams & Wilkins Stage of Ligament Healing Copyright 2005 Lippincott Williams & Wilkins Restoration of Normal Tissue Relationships After connective tissue injury, relationship and integrity of tissues are altered. Possible Interventions: Active muscle contractions Passive joint motion Mobilization Stretching Copyright 2005 Lippincott Williams & Wilkins Optimal Loading Choose treatment procedures that don’t disrupt the healing process. Requires: 1. Choosing a load that doesn’t under- or overload the tissue. 2. Considering biomechanical effects of daily activities. 3. Understanding of mechanism of injured tissue loading. Copyright 2005 Lippincott Williams & Wilkins Optimal Loading Copyright 2005 Lippincott Williams & Wilkins Signs of Overload 1. 2. 3. 4. Increased pain that does not resolve within the next 12 hours. Pain that is increased over the previous session or comes on earlier in the exercise session. Increased swelling, warmth, or redness in the injury area. Decreased ability to use the part. Copyright 2005 Lippincott Williams & Wilkins Specific Adaptations to Imposed Demands (SAID) Includes quantity and type of activity. Extension of Wolff’s law. Guides exercise prescription parameters. Stage of healing and optimal loading parameters closely reflect the specific demands on the patient’s functional tasks. Copyright 2005 Lippincott Williams & Wilkins Prevention of Complications Goal – Minimize effects of immobilization while an injury is healing. Electrical stimulation or isometric contractions. AROM at joints above and below injury sites. Weight-bearing exercises when feasible to load articular cartilage and prevent degradation. Copyright 2005 Lippincott Williams & Wilkins Management of Impairments Associated with Connective Tissue Dysfunction Sprain – Acute injury to a ligament or joint capsule without dislocation. May resolve with short-term immobilization, controlled activity, and rehab exercises. Copyright 2005 Lippincott Williams & Wilkins Sprain Classification 1. Grade I – Mild, ligament is stretched, no discontinuity. 2. Grade II – Moderate, some fibers stretched/torn, some joint laxity. 3. Grade III – Severe, complete ligament disruption with resultant laxity. Copyright 2005 Lippincott Williams & Wilkins Examination and Evaluation Observation to assess ecchymosis and edema. Observe functional ROM, AROM, and PROM. Assess joint integrity and mobility. Palpation to identify primary and secondary injuries. Copyright 2005 Lippincott Williams & Wilkins Strain: Musculotendinous Injury Strain – An acute injury to the muscle or tendon from an abrupt or excessive muscle contraction. Usually a result of a quick overload to the muscle– tendon unit whereby the tension generated > tissue’s capacity. Copyright 2005 Lippincott Williams & Wilkins Strain Classification 1. Mild 2. Moderate 3. Severe Based on clinical examination – Pain, edema, loss of motion, tenderness. Contributing factors – Poor flexibility, poor warm-up exercise, insufficient strength or endurance, poor coordination. Copyright 2005 Lippincott Williams & Wilkins Examination and Evaluation Thorough history. Reproduce clinically through active or resisted contraction. Muscle may need to be put on stretch during active or resisted contraction. Localized swelling and warmth may be observed. Copyright 2005 Lippincott Williams & Wilkins Application of Treatment Principles Phase I Phase II Phase III Principle Optimal loading Prevent secondary complications Restore normal tissue relationships Prevent complications Fine Tune. Convert baseline strength and mobility into functional movement patterns Loading Zone Balance of rest and loading Loading is important– orientation of collagen fibers Graded, progressive exercise is necessary to maintain improvements Modalities Cryotherapy with compression/ elevation Joint mobilization Stretching, massage, postural education Patient maintenance program. Postural education, stretching, strengthening, etc. Exercise Intervention Isometric contractions Contraction of lengthened muscle in shortened range More whole body patterns and functional activity Copyright 2005 Lippincott Williams & Wilkins Tendinitis and Tendon Injuries Failure occurs due to micro- or macrotrauma. Outcomes are lengthy BUT predictable. Categories/classifications have evolved. Copyright 2005 Lippincott Williams & Wilkins Classification of Tendon Injuries 1. Macrotrauma – Commonly occur at musculotendinous junction. 2. Microtrauma – Paratendinitis (inflamation of outer layer of tendon). 3. Tendinosis – Degeneration without inflammatory response. 4. Tendinitis – Symptomatic degeneration of tendon with vascular disruption and an inflammatory response. Copyright 2005 Lippincott Williams & Wilkins Examination and Evaluation History and subjective symptoms are of primary importance. ROM, muscle performance, posture, joint integrity, mobility tests. Observe structural or postural abnormality. Document nodules, palpable defects, crepitus. Copyright 2005 Lippincott Williams & Wilkins Treatment Principles and Procedures Treatment based on specific tendon injury. Restoring length, strength: fundamental. If inflammation is present – consider cold packs, electrotherapeutic modalities. Stretching (low load) if muscle length is inadequate. Appropriate rehabilitation activities (w/ appropriate modifications). Copyright 2005 Lippincott Williams & Wilkins Management of Cartilage Injury Classification of Cartilage Injuries Mechanical Nonmechanical – Infection, inflammatory conditions, prolonged joint immobilization Copyright 2005 Lippincott Williams & Wilkins Examination and Evaluation Cause of damage Area of damage Classification/health of cartilage General health Lifestyle factors Body weight Joint alignment ROM Muscle performance Joint integrity Mobility Copyright 2005 Lippincott Williams & Wilkins Treatment Principles Primary goal – Restoration of motion Freedom of motion Equitable load distribution Stability Increased muscle performance Copyright 2005 Lippincott Williams & Wilkins Management of Impairments Associated with Localized Inflammation Contusion Results from a blow and can occur in any area of the body. Blood vessels below skin become damaged. Accumulation in deeper tissues (hematoma) may develop. If untreated, may progress to myositis ossifications. Copyright 2005 Lippincott Williams & Wilkins Examination and Evaluation History of a “blow” provides best information. Size, location, and direction lend a window into location and extent of soft tissue injuries. Palpation, joint mobility, muscle performance, flexibility, and function tests help guide treatment procedures. Copyright 2005 Lippincott Williams & Wilkins Treatment Principles Simple contusions resolve in a timely manner. Use measures of pain, muscle length, muscle performance to guide aggressiveness of treatment. ROM must be restored as quickly as possible. Use ice to control swelling and local inflammation. Restore muscle performance. Submaximal isometrics may be initiated in early stages. Copyright 2005 Lippincott Williams & Wilkins Management of Impairments Associated with Fractures Fracture – Break in the continuity of the bone. Copyright 2005 Lippincott Williams & Wilkins Classification of Fractures 1. Open fractures – Breaking the skin’s surface. 2. Closed fractures – Does not break through the skin. 3. Nondisplaced – All sides of fracture remain in anatomic alignment. 4. Displaced – The ends of the bones are not in anatomic alignment. Copyright 2005 Lippincott Williams & Wilkins Types of Fractures Copyright 2005 Lippincott Williams & Wilkins Application of Treatment Principles Consider associated soft tissues. Healing of fracture is primary. Rehabilitation of soft tissue may be more challenging. Copyright 2005 Lippincott Williams & Wilkins Fracture Intervention Treatment focuses on recovery of initial trauma, rehabilitating tissues that were immobilized. Initially, gentle joint mobilization, stretching. Decrease loading when indicated (e.g., stress fracture). Gentle strengthening (isometrics, etc.). NMES, SEMG – Feedback for atrophy. As impairments improve, incorporate activities to alleviate remaining functional limitations. Copyright 2005 Lippincott Williams & Wilkins Soft Tissue Procedures Ligament reconstruction Tendon surgery Debridement Synovectomy Decompression Soft tissue stabilization and realignment Meniscal and labral repairs Copyright 2005 Lippincott Williams & Wilkins Bony Procedures Debridement/abrasion chondroplasty Osteochondral autograft transplantation (OAT) Autologous chondrocyte implantation Open reduction and internal fixation Fusion Osteotomy Copyright 2005 Lippincott Williams & Wilkins Summary Composition and structure of connective tissues provide information regarding mechanical properties and function. Unique viscoelastic characteristics are the result of fluid and solid constituent materials. When connective tissues are loaded, the stress or change per unit length gives information about the tissue’s ability to withstand loads. Copyright 2005 Lippincott Williams & Wilkins Summary (cont.) Stages of healing & knowledge of injury give clinician guidelines for intervention throughout care. Restoration of tissue relationships, SAID principle, prevention of secondary complications – Guide treatment. Acute soft tissue injuries necessitate early intervention to avoid secondary complications. Copyright 2005 Lippincott Williams & Wilkins Summary (cont.) Management of tendon injuries and prognosis varies according to injury classification. Interventions used in treatment of bony or surgical procedures should have foundations in basic science and require an understanding in anatomy and kinesiology of the area. Copyright 2005 Lippincott Williams & Wilkins