Preceptors Pearls One

PRECEPTOR PEARLS
Sonoma State University
Family Nurse Practitioner Program
Dr. Wendy Smith and Dr. Mary Ellen Wilkosz
Objectives
• 1. Develop knowledge and understanding of the history and current status of the preceptor role.
• 2. Develop an understanding of three learning theories/models that support the preceptor role and learning styles.
• 3. Have a clearer understanding of the:
• Student and Program responsibilities
• Preceptor and Clinical Faculty responsibilities
History and Background
• Guided experience = preceptorship
• Goal = manage care with optimal health outcomes
• Preceptorship highly useful strategy for clinical education
• Education is individualized
• Create link with classroom knowledge and patient care
• Role modeling
Requirements for Accredited NP
Programs
• > 500 hours of supervised clinical practice
• Preceptors must be experienced NPs or MDs in same specialty
• One-to-one relationship
Expectations
• Expectation Student = SOAP
• Expectation Preceptor = plan development, implications, reflections
I
L
S
K
L
E
D
G
E
K
N
O
W
L
National Organization for Nurse Practitioners, 2000
Pitfalls of TEACHING “On the Job”
Rapid pace Multiple demands
Limited time for teaching
TEACHING IN CLINICAL SETTING
Variable teaching/learning opportunities
Limited time for feedback
Irby, 1995
Pitfalls of LEARNING “On the Job”
Not collaborative
Rapid pace
Multiple demands
TEACHING IN CLINICAL SETTING
Not optimal pace for learning
Limited time for teaching
Variable teaching/learning opportunities
Lack opportunity for reflection
Limited time for feedback
Irby, 1995
Why Am I Here?????
• Help you to identify students learning style
You can do it!!
Why Am I Here?????
• Help you identify your leadership style
VS
Whip cracker
Nurturing
Rewards of Precepting
• Enjoy teaching and being a preceptor
• Giving back
• Ensuring capable and competent HCP
• Adjunct faculty status
• CEUs
• Letters for recertification
Ø
Connection With Program
• Understand expectations of the program
• Regular communication between program and preceptor
• Clinical faculty site visit
• Student evaluation
• Participate in final grade decision
Program Preceptor
Benefits of Having a Student
• Molding a student into the perfect fit for your office
• They add value
• Currency
• Extra attention for patients
• Fresh perspective
Catherine Burns, PhD, RN, CPNP, FAAN, Michelle Beauchesne, DNSc, RN, CPNP,
Patricia Ryan-Krause, MS, MSN, RN, PNP, Kathleen Sawin, DNS, CPNP, FAAN.
J Pediatr Health Care. 2006;20(3):172-183. Retrieved 12/27/2014: http://www.medscape.com/viewarticle/532189_1
Clinical Placements at SSU
• Who can our students precept with?
• MDs, DOs, NPs, PAs*, CNS, CNM
• How do our students find preceptors?
• Clinical coordinator, word of mouth, prior students, friends, acquaintances
• Legal Contracts?
• Agency contract and/or LOA
• Do students carry liability? ABSOLUTELY!
• Certified Background
• Background check, drug test, immunizations, current licensure,
CPR, TB,
Agency Responsibility
• Student attends:
• EHR training
• HIPPA training specific to agency
Preceptors Perspective
• Check Paperwork is complete, MAKE COPIES for file
• Introductions to Manager/s, other providers, support staff
• Set positive manner of your role and the experience with
Manager and staff.
• What if you are ill or unable to attend clinic on student day is there a back-up preceptor that can be designated?
• How will you introduce student to patient, if teaching is commonplace in your practice then a brief statement about your having a student work with you is all that is needed. If not will you ask patients if willing to have student see them.
• Maintaining your relationship and rapport with your patients.
• How will you manage the stress of a student and the impact on your flow?
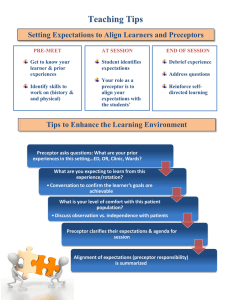
Setting the Learning Environment
• Have a plan and discuss with the student how the process of patient visits will take a directive coaching role.
• A place to discuss performance issues and give teaching/feedback? – privacy, “safe place”
• Discuss time elements, what are your parameters
( depending of level of student and complexity of patient) consider variance.
• A place for student to sit/how will you work with them on the HER/charting, Checking each entry?
• Note about shadow charting?
• Logistics - number of exam rooms and your plan for student role/pt visits
Adult Learning Theory
• Adult learning ≠ Children and Teen learning
• Adults have special needs/requirements
• New area of study
• Malcom Knowles in 1978
Knowles, M (1978) The Adult Learner : A Neglected Species. Tampa, FL: Gulf Publishing
Adults as Learners
• Autonomous and self-directed
• Life experiences and knowledge
• Relevancy oriented
• Practical
• Respect
Kolb’s Experiential Learning Theory
• Different ways of taking in and processing information
4 Stages of Kolb’s Experiential learning theory
• 1. Concrete experiences
• 2. Observational/reflection
• 3. Forming abstract concepts
• 4. Testing in new situations
Built on Knowles Theory, Kolb’s Experiential Learning Theory.
Kolb, DA (1984) Experiential Learning: Experience as the Source of Learning and Development.
Vol.1. Englewood Cliffs, NJ: Prentice-Hall.
Kolb, D. A. (1999) Learning style inventory: Version 3 . Boston: McBer & Co.
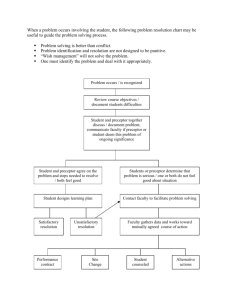
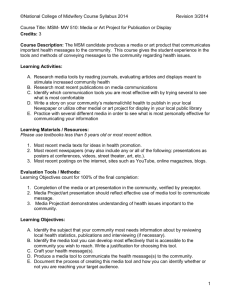
Kolb’s Learning Cycle
Degrees of Preference
Doing ( A ctive
E xperimentation [AE])
Accommodating (CE/AE)
Feeling
( C oncrete
E xperience [CE])
Converging (AC/AE)
Diverging (CE/RO
Watching ( R eflective
O bservation[RO])
Assimilating (AC/RO)
Thinking ( A bstract
C onceptualization [AC])
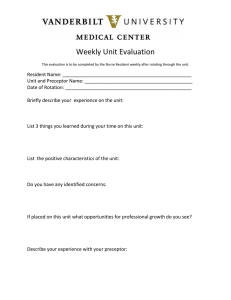
Kolb’s Learning Style Matrix
Feeling (Concrete
Experience (CE))
Doing (Active
Experimentation AE))
Watching (Reflective
Observation (RO))
Accommodating (CE/AE)
Prefer to work in teams to complete tasks, prefers hands-on often relies on intuition rather than logic. Takes practical, experiential approach.
Learn through concrete experience and active manipulation.
Diverging (CE/RO)
These people perform better in situations that require ideageneration. They tend to not jump in like to work in groups and receive personal feedback. Learn through concrete experience and reflection
Thinking (Abstract
Conceptualization (AC))
Converging (AC/AE)
Can solve problems and will use learning to find solutions to practical issue. Prefer technical tasks and less concerned with people and interpersonal aspects. Like to try new ideas and simulate. Learn by thinking (abstract concepts) and doing.
Assimilating (AC/RO)
Less focused on people and more interested in ideas and abstract concepts. Prefer a concise, logical, and linear approach. Like readings, lectures, pictures diagrams, and models and time to think things through. Learn by thinking (abstract concepts) and reflection
From Novice to Expert
• Patricia Benner theorist
• Framework for assessing needs at different stages of professional growth
• Expert nurses develop skills and understanding over time
• Focus on how nurses acquire knowledge
Dr. Benner’s Stages of Clinical Competence
• Stage 1 Novice:
This would be a nursing student in his or her first year of clinical education; behavior in the clinical setting is very limited and inflexible. Novices have a very limited ability to predict what might happen in a particular patient situation.
Signs and symptoms, such as change in mental status, can only be recognized after a novice nurse has had experience with patients with similar symptoms.
Dr. Benner’s Stages of Clinical Competence
• Stage 2 Advanced Beginner:
• Those are the new grads in their first jobs; nurses have had more experiences that enable them to recognize recurrent, meaningful components of a situation. They have the knowledge and the know-how but not enough indepth experience.
Dr. Benner’s Stages of Clinical Competence
• Stage 3 Competent:
• These nurses lack the speed and flexibility of proficient nurses, but they have some mastery and can rely on advance planning and organizational skills. Competent nurses recognize patterns and nature of clinical situations more quickly and accurately than advanced beginners.
Dr. Benner’s Stages of Clinical Competence
• Stage 4 Proficient :
• At this level, nurses are capable to see situations as
"wholes" rather than parts. Proficient nurses learn from experience what events typically occur and are able to modify plans in response to different events
Dr. Benner’s Stages of Clinical Competence
• Stage 5 Expert:
• Nurses who are able to recognize demands and resources in situations and attain their goals. These nurses know what needs to be done. They no longer rely solely on rules to guide their actions under certain situations. They have an intuitive grasp of the situation based on their deep knowledge and experience. Focus is on the most relevant problems and not irrelevant ones.
Analytical tools are used only when they have no experience with an event, or when events don't occur as expected.
Where the Rubber Meets the Road!
• Get to know your preceptee
• Identify learning needs early on
• Assess biases or values
• Ask about other commitments
• Be clear about expectations
Where the Rubber Meets the Road!
• Know preceptee’s level of knowledge
• Huddles and maybe cuddles!
• Communicate strengths, and what still needs work
• Clear up problems ASAP!
• Guide the preceptee in self-direction
But Remember . . .
• It’s not always a match made in heaven!
Group Activity
• What kind of learner are you?
Group Activity #2
• Think of a preceptor you had, what are four attributes/qualities you can recall that made them an effective preceptor, or not so effective preceptor.
Activity #3
• Think about when you began YOUR preceptorship to become an NP and jot down four attributes/qualities YOU felt that you . . .
• 1. Brought to your clinical experience as a student.
• 2. Brought to your very first NP job.
These categories suggest levels of performance in our professional life, however we all experience different levels in different aspects of our life. Identify activities that you currently perform (or have recently performed) that relate to each of these levels
• 1. Novice
• 2. Advanced Beginner
• 3. Competent
• 4. Proficient
• 5. Expert