Subject Payment Schedule-Participant Payment Form
advertisement

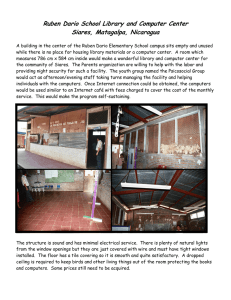
SUBJECT PAYMENT SCHEDULE / PARTICIPANT PAYMENT FORM UTHSCSA Tracking Number: Section 1: Payment Schedule ☐ Yes ☐ No Will Subjects be compensated the same amount for Each Study Visit? IF Yes to section 1: Number of Visits: Type of Payment Fee Type Select an item Select an item Total Compensation per patient: Timing of Payment: MAX Amount per Occurrence (USD) (USD) Select an item IF No to section 1: Please specify Payment Schedule below Visit or Event Description Fee Type Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Select an item Select an item (USD) Total Compensation per patient: Timing of Payment: Compensation Amount Type of Payment (USD) Select an item If you need additional Space please attach additional pages Version 1.2, 07/25/2014 Clinical Trials Office UT Health Science Center at San Antonio Page 1 of 2 SUBJECT PAYMENT SCHEDULE / PARTICIPANT PAYMENT FORM Section 2: Additional Reimbursement (i.e., Airfare, Lodging, Meals, Mileage, Parking, Taxi Voucher/Fare, etc.) For “Additional Reimbursement” that is variable, please provide the Maximum amount per Occurrence. Additional Reimbursement Type Fee Type Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Select an item Timing of Payment: TOTAL MAX Additional Reimbursement Amount, per/Subject: ☐ N/A MAX Amount per Occurrence (USD) (USD) (USD) (USD) (USD) (USD) ☐ N/A Section 3: Gifts ☐ Will Subjects be provided Gifts or other items of limited or no monetary value? (Please Specify: Type and Approximate Value) Section 4: Screen Failures ☐ Yes ☐ No Will Screen Failures be compensated for visits completed? Approximately how many Screen Fails do you expect locally? Up to which Visit can a Subject Screen Fail? Section 5: Unscheduled Visits ☐ Yes ☐ No Will Subjects receive additional compensation for Unscheduled Visits? Compensation amount per/visit: (USD) Section 6: Incomplete Visit Payment How will Subjects who do not complete their Visit be compensated? Select an item Section 7: Incomplete Study Payment How will Subjects who do not complete the Study be compensated? Select an item Section 8: Study Scope Will UTHSCSA funds be used to pay participants? (This would include any funds that are used from a “Project Account,” or that are deposited into a “Project Account,” to pay participant payments) ☐ Yes ☐ No Will UTHSCSA employees manage or handle the participant payments? ☐ Yes ☐ No Version 1.2, 07/25/2014 Clinical Trials Office UT Health Science Center at San Antonio Page 2 of 2