Closing the MGD Gap Through Health Literacy
Working With Civil Society and Communities
Dr Bernhard Schwartländer
ECOSOC Annual Ministerial Review
Regional Ministerial Meeting for Asia and the Pacific
29 & 30 April 2009, Beijing, China
MDG Goal 6: Combat HIV/AIDS, Malaria
and other diseases
• Target 6a: Have halted by 2015 and
begun to reverse the spread of HIV/AIDS
• Target 6b: Achieve by 2010,universal
access to treatment for HIV/AIDS for all
those who need it.
• Target 6c: Have halted by 2015and begun
to reverse the spread of malaria and other
major diseases.
AIDS: Anti Retroviral Treatment in Asia-Pacific
Coverage of those in need
100.0
ART Coverage
2006
2007
60.0
40.0
20.0
0.0
n
ta
hu
h
ng
Ba
s
de
a
l
b
B
C
am
ia
od
C
n
hi
a
ji
Fi
d
In
ia
In
n
do
ia
es
ia
o
La
M
s
ay
al
M
ia
ol
g
on
ar
M
nm
ya
N
a
ep
l
Pa
t
kis
an
Ph
n
pi
li ip
es
PN
a
G
i
Sr
nk
La
Th
la
ai
nd
V
tN
ie
am
UNAIDS/S.NOORANI
Per cent
80.0
AIDS Treatment Literacy in China
Community based approach
• 4 provinces, 35 project sites
• Over 10,000 people on ART (about one quarter of
all PLHIV on ART in China)
• Peer motivators, SMS platform, women’s network
• Positive prevention
• Treatment literacy manual for PLHIV
• ART management software, doctor’s forum
Source: Thomas Cai, AIDS Care China, 2009. Data for 10 Yunnan sites in 2008
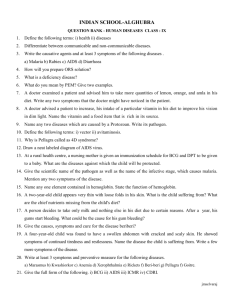
China: AIDS Treatment Literacy
More Than Doubling in Enrollment
25
Before Intervention
After Intervention
20
15
13
13
12
10
5
20
11
11
9
5
5
8
7
7
7
5
4
8
5
4
2
2
Source: Thomas Cai, AIDS Care China, 2009. Data for 10 Yunnan sites in 2008
ag
e
Av
er
Te
ng
ch
on
g
os
ha
n
Ba
u
Ge
ji
le
Mi
g
Lin
gc
ha
n
Da
li
an
iyu
Ka
jia
ng
Yin
g
Ru
ili
0
China: AIDS Treatment Literacy
More Than Two Third Reduction in Drop-Out
16
14.4
14
Before Intervention
After Intervention
12
10
7.7
3.5
1.82.1
1.1 1
1.6
Source: Thomas Cai, AIDS Care China, 2009. Data for 10 Yunnan sites in 2008
ag
e
os
ha
n
Te
ng
ch
on
g
0.6
Ba
an
iyu
Ka
jia
ng
Yin
g
Ru
ili
0
2
u
1
1.6
0.4
4.6
2.6
le
1.1
g
2
2.8
Mi
3.1
Lin
gc
ha
n
3.5
Da
li
4
5.2
Av
er
6
Ge
ji
8
TB prevalence and mortality
Global Targets
Prevalence (cases/100,000)
Mortality (deaths/100,000)
350
35
300
30
250
25
200
20
150
15
100
Target = 148
10
50
5
0
0
1,990
1,995
2,000
2,005
2,010
2,015
1,990
Source: Global Tuberculosis Control 2009, WHO 2009
Target = 14
1,995
2,000
2,005
2,010
2,015
TB DOTS in India
Reaching Patients Through Angan Wari
• Angan Wari: rural community health
workers to improve nutrition of children
and mothers
• Access to communities
• Can be efficiently utilized to increase
health literacy
Source: Singh et al, Indian J Tuberc 2005;15-20
TB DOTS in India
Best Outcome Through Community Approach
Treatment success by delivery model
100%
80%
95%
80%
76%
Gov HW
Commun Volunteer
60%
40%
20%
0%
Angan Wari
Source: Singh et al, Indian J Tuberc 2005;15-20
TB DOTS in Bangla Desh
DOTS more cost effective when CHWs are involved
Total Cost (US$/Patient)
120
Community Health Worker
model could diagnose, treat and
cure 50% more TB patients than
the regular national programme
96
100
80
US$
•
64.2
60
40
20
0
NGO Model
Source: Islam et al, WHO Bulletin 2002, 80(6); 445-450
Government
Malaria Cases per 1000 population
Towards MDG Targets
Target: > 75% Reduction in cases and deaths by 2015 compared to 2005
Source: World Malaria Report 2008, WHO 2008
Teaching Mothers to provide Malaria Treatment
Under 5 mortality/1000 Child Years
More than 40% Reduction in Overall Child Mortality
Two Third Reduction in Malaria Mortality
60
50
Reduction in overall Child Mortality
Randominsed trial in Ethiopia
50.2
40
29.8
30
20
10
0
Controls
Source: Kidane G, Morrow RH. The Lancet, 2000, 356:550-4
Intervention
Malaria in Zambia
Increased Malaria Literacy results in
More Than 50% Reduction in Malaria Mortality
100%
79%
80%
85%
71%
76%
81%
64%
62%
60%
2006
2008
44%
44%
40%
22%
20%
0%
recognising fever
as a symptom
recognising
mosquito bites as
the source
reporting
mosquito nets as
a prevention
method
Source: National Malaria Program Zambia, 2009
HH owning at
least one ITN
children under 5
slept under an ITN
the previous night
Conclusions
•
•
•
•
MDG 6: challenges ahead, but possible
Acceleration is needed
Health Literacy is key
Community approaches are
– Working
– Cost effective
– Equitable (reaching the poorest)
– Sustainable
– Scalable
 0
0