12640814_ISICEM2012-Revie-PE_SS_ID.pptx (507.5Kb)
advertisement
")
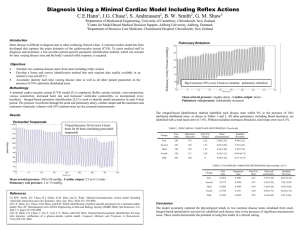
Computer-based monitoring of global cardiovascular dynamics during acute pulmonary embolism and septic shock in swine JA Revie, J Stevenson, JG Chase, BC Lambermont, A Ghuysen, P Kolh, GM Shaw, T Desaive. Objective Retrospectively test a model-based monitoring method on porcine measurements. Fit subject-specific cardiovascular models from available or inferable ICU data. Track hemodynamic changes due to acute pulmonary embolism (APE) and septic shock. (SS). Retrospectively identify pig-specific cardiovascular models for improved monitoring of common ICU diseases. Experimental Protocol 9 pigs were pre-medicated , ventilated, and anesthetised as explained in Lambermont et al (2003). Cardiovascular model In 5 pigs 3 autologous blood clots were inserted at t0, t120, and t240 minutes into the trials to simulate APE. Measurement ABPsys (mmHg) ABPdia (mmHg) PAPsys (mmHg) PAPdia (mmHg) SV (ml) GEDV (ml) CVPmean (mmHg) ECGtpeak (msec) In the other 4 pigs, and endotoxin infusion over t0-t30 was used to induce SS. 6 main cardiac measurement were recorded: • • • Left and right ventricular volume waveforms (open heart catheterisation) Left and right ventricular pressure waveforms (open heart catheterisation) Aortic and pulmonary artery pressure waveforms Measurements were recorded every 30 minutes for up to 4.5 hours. . Model Fitting 80 subject-specific models of the cardiovascular system were identified. Model identification was achieved using only equivalent measurements of readily available or inferable ICU data: • • • • • Value 120 80 40 15 70 Aorta Lung Capillaries Pulmonary artery Pulmonary vein Left Right ventricle ventricle Vena Cava Body Capillaries Features of the aortic and pulmonary artery pressure waveforms SV Global end diastolic volume (GEDV) CVP ECG Aortic pressure Parameter trends were tracked to monitor the progression of SS and APE. Left ventricle P-V loop 125 120 Modeled maximum left and right ventricular pressure were identified to median errors of <7%. In APE pulmonary afterload tracked experimentally derived afterload to R2 = 081 In SS pulmonary afterload tracked experimentally derived afterload to R2 = 0.95 In both studies RVEDV increased significantly and LVEDV decreased indicating a leftward shift in the intra-ventricular septum 110 Pmean 105 100 dPmax This model-based method shows clinical potential. Hemodynamic measurements, from different monitoring devices, can be aggregated into an easy to understand physiological form, to assist with diagnosis and real-time monitoring of cardiac and circulatory state. However, further human clinical trials are required to test the technology, which are currently underway at the Christchurch Hospital ICU. Ea 60 Measured 40 Model 20 90 85 0 0.1 0.2 0.3 0.4 0.5 0 0.6 0 10 20 30 40 Time (s) 50 60 70 80 Volume (ml) Systemic vascular resistance Pulmonary vascular resistance 1.6 3.2 3 Resistance (mmHg.s/ml) All trends derived from the subject-specific cardiovascular models were consistent with known trends of septic shock and pulmonary embolism, including an increase in pulmonary vascular resistance in both diseases, and a decrease in systemic resistance in septic shock. Ees 95 Discussions The model matched independent measures (LVEDV, RVEDV, and max left and right ventricle pressures), not used during identification, to median errors of less than 10%, which is smaller than most measurement errors. PP 80 1.4 APE Resistance (mmHg.s/ml) Modeled LVEDV and RVEDV matched measured values to median errors of <7.5%. Measured 115 100 Model Pressure (mmHg) Results Aortic pressure (mmHg) 120 2.8 2.6 2.4 2.2 2 1.8 SS 1.2 1 0.8 0.6 0.4 1.6 1.4 0.2 0 50 100 150 Time (sec) 200 250 0 50 100 150 Time (sec) 200 250 90