Garg.Gaurav - Exclusive Breastfeeding for improving child health in Sierra Leone
advertisement

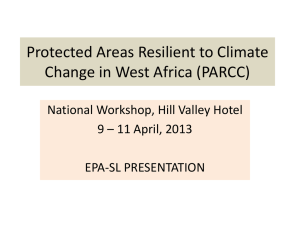
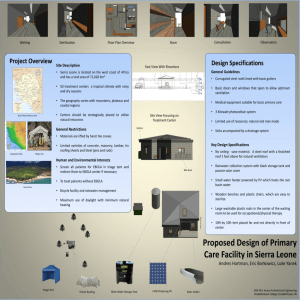
Gaurav Garg 07/16/2010 Exclusive Breastfeeding for improving child health in Sierra Leone Background Despite some recent progress, Sierra Leone continues to have extremely high rates of infant and child mortality.1 In the 2009 Human Development Report (HDR), Sierra Leone was ranked 180 out of 182 countries. Recently, the Government of Sierra Leone (GoSL) with the help of development partners has taken steps to strengthen health systems and improve access to and quality of curative care through the launch of the Free Health Care services for pregnant women, lactating mothers and children under five years on April 27, 2010. The preventive side of public health is equally if not more important. Figure 1: Map of Sierra Leone Evidence has shown that exclusive breastfeeding (EBF) for the first six months is one of the most effective interventions to reduce child malnutrition and morbidity. This is because 1 The Lancet (Vol 375, Issue 9730, pg. 1988-2008, 5 June 2010) reported Sierra Leone was one of the 34 countries in which between 2000-10 rates of decline in child mortality have increased by more than 1%. According to the SLDHS 2008, infant mortality and child mortality stood at 89 and 140 per 1000 live birth, a reduction from corresponding figures of158 and 267 according to MICS 2005. 1 Gaurav Garg 07/16/2010 breastfeeding is a low cost and high impact intervention (as are handwashing and use of bed nets) that can improve nutrition and immunological status of children and also reduce incidence of diarrhoea, which is the second leading causes of child mortality worldwide.2 Although breastfeeding is very common in Sierra Leone with 95% of children ever breastfed, EBF is only 11% (DHS 2008). The UNICEF Sierra Leone Country Programme objective is that by 2012, 60% of the lactating mothers are aware of the benefits and practice EBF. Identifying the script Within Sierra Leonean society and across all ethno-tribal groups (Krio, Mende, Limba, Temne, Kono, Madingo and others) grandmothers, mothers-in-law, Traditional Birth Attendants (TBAs) and community elders are held as custodians of traditions, knowledge and best practices on child care. For this, they are accorded a high degree of respect in the community. In Sierra Leone, credible information about healthcare and childcare information is minimal across all demographic groups and this is further compounded by the women’s low literacy levels – only 43% of the women aged between 15-24 years are literate according to SLDHS 2008. In this scenario, new and/or young mothers are often thought of as being inexperienced, “dumb”, unaware and largely incapable of making decisions about child feeding and care. The social structure within the communities and the power hierarchy within women systematically marginalise young mothers. The high incidence of teenage pregnancy and early marriage in Sierra Leone has further entrenched these attitudes in the country. 3 According to Bicchieri (2006), social norms are embedded in scripts, and thus are part of a 2 WHO, Learning from Large-scale Community-based Programmes to Improve Breastfeeding Practices, 2008, pg 47. 3 According to the SLDHS 2008, 25% of women (15-49 years) are married before age 15, and 69% of women (20-49 years) are married before age 18. 2 Gaurav Garg 07/16/2010 complex network of values, practices etc”.4 In this paper, I focus on precisely this, the “young mother” script which is activated in issues of EBF in Sierra Leone. A recent qualitative study undertaken by UNICEF Sierra Leone shows that there exist several social norm influenced barriers to the adoption of exclusive breastfeeding practices. These barriers include limited autonomy on the part of the woman/mother (subject to the directives of her husband, her mother-in-law, and even some ill-informed health advisors); mistrust of the information source; fear of violence or embarrassment; cost of adoption of the new practice; and the distance to acquire the information, skills, or materials to undertake it. The study also highlights the issue of work overload which blocks women from taking on new, recommended practices is another key barrier to exclusive breastfeeding. However, “women’s workload” can be understood as another script in the EBF and broader nutrition scenario (across the world and not only in Sierra Leone), and a detailed discussion on its complexities is beyond the scope of this paper. Traditional practice and customs on EBF, under the custodianship of older women, grandmothers and community elders, often outweigh the perceived positive benefits of changing behaviour. Some of the traditional practices, customs and beliefs around EBF in Sierra Leone include - child given salt mixed with palm oil and kola nut because this is what the relatives eat and the child should learn right way how to eat like adults; water is the child's first meal in the world, and colostrums is discoloured so should be discarded; water promotes growth and cleans the stomach; wife discouraged by husband to breastfeed because of the belief that sexual intercourse with the wife/mother while she is breastfeeding will 4 Bicchieri, C. (2006), The Grammer of Society: The Nature and Dynamics of Social Norms, Cambridge; Cambridge University Press pg. 57 3 Gaurav Garg 07/16/2010 poison the breastmilk (sexual intercourse ranks above EBF of child in the preference ordering). Social norm analysis – expectations and payoffs Using Bicchieri’s social norm framework to explore and analyse the “young mother” script reveals useful details. There exist conditional preferences for a social norm to exist which are a combination of empirical expectations (young mothers believe that a sufficiently large part of the relevant population conforms to non-exclusive breastfeeding behaviours) and normative expectations (young mothers believe that a sufficiently large part of the relevant population expect them to conform to non-exclusive breastfeeding behaviours).5 The normative expectations of young mothers are managed and enforced by the respect relationship and power hierarchy among women and elders in the community. Nonconformity with the norm could lead to ostracisation, loss of respect and standing and also to domestic violence. Changing these expectations is the key to enhancing young mothers’ decision making about EBF and for them to adopt the favourable EBF behaviours. For this to happen, the collective empirical expectations of the reference group need to be changed, in a participatory manner with the full participation and involvement of the community members to ensure that the change is socialised and sustainable. This is not to say that positive deviants for exclusive breastfeeding do not exist in communities. UNICEF Sierra Leone’s monitoring of community nutrition activities has revealed that in certain communities pregnant and lactating women’s understand, adopt and maintain favourable exclusive breastfeeding practices. This “change” has been largely 5 Bicchieri, C. (2006) 4 Gaurav Garg 07/16/2010 attributed to regular counselling and outreach by a long serving health worker who over a period of time has been able to convince community members and mothers about the value of EBF and importantly, make mothers believe that it is indeed possible to practice EBF and support them in the adoption and maintenance of the practice. Within the social norms framework, it can thus be said that these positive deviants have strong personal normative beliefs which clash with the normative expectations, which means that mothers practice EBF without worrying about the sanctions (ostracisation, rejection, shame etc). This EBF scenario in Sierra Leone presented in the “young mothers” script represents a pure coordination game with two Nash equilibria, which implies that if a young mother “knows a cooperative norm exists and expects a sizeable part of the population to follow it, then provided she also believes she is expected to follow such a norm, she will have a preference to conform to the norm in a situation in which she has the choice to cooperate or to defect”.6 In the figure below, conforming to EBF when everyone else also does so, is represented by a payoff of 10 for the young mother with 10, 10 representing the ideal/desired situation where due to existing collective empirical expectations everyone exclusively breastfeeds. Conforming to the traditional practices reinforced by elders would result in a payoff of 5 to the young mother. This is less desirable than 10, 10 state but conforming would save the young mother from sanctions and punishments so she is likely to adopt unfavourable EBF practices. When others in the reference group are practicing EBF and there exist empirical and normative expectations for the young mother to do so as well, not doing it would mean that the infant would miss out on the health benefits of the practice which is represented by 0,3. The -1, 0 state represents the young mother practicing EBF (3) but in the absence of 6 Bicchieri, C. (2006), pg. 26. 5 Gaurav Garg 07/16/2010 empirical and normative expectations for her to do so which means that sanctions would be imposed on her (-4). Figure 1: Coordination game with young mother The figure below represents the case of the positive deviance in practicing EBF. All other figures being the same as in the figure above, since the young mother does not worry for the sanctions and has enough belief in her own capacity to practice EBF and is also supported by some key influencers in the community ( combination of health worker, maybe some health volunteers, religious leaders etc), her payoff is 3. EBF EBF O T H E R Non-EBF 10,10 3,0 0,3 5,5 SELF Non-EBF Figure 2: Coordination game with positive deviance 6 Gaurav Garg 07/16/2010 Strategies to promote EBF in Sierra Leone Since the end of the war in 2002, Sierra Leone has taken small but assured steps in moving from an emergency to a more structured development phase. In the past, health promotion strategies have been limited to one-way information dissemination campaigns. Other problems exist. For example, while radio is the most popular source of information in the country, social customs and informal asset ownership rules dictate that radios be owned by men. Also as recent Sierra Leone polio communication evaluation has confirmed, information heard on the radio by men is not always shared with their wives, mothers and sisters. UNICEF Sierra Leone studies have shown that women’s access to credible information remains limited and information when received, does not translate into desired behaviour due to the lack of support from community members and the overwhelming importance of customs and traditional practices and low levels of education. Following the qualitative baseline study on barriers to infant and young child feeding practices in 2009, a detailed network analysis was undertaken to understand the flow of information - who talks to whom in a typical community in Sierra Leone. In the figure below the young mother (blue) receives information from her peers (green) and the health worker (black), grandmothers and older women (yellow) and the TBA (orange). Older women’s and TBA’s experience and position in society heavily mediate this relationship. The young mother’s peers receive information from/talk to grandmothers and the health worker. As mentioned earlier, in cases of the positive deviance in Sierra Leonean communities the tie between the young mother and the health worker is very strong and the health worker’s influence in the community is able to override the traditional practices and marginalization of young mothers. The husband (pink) in the community receives 7 Gaurav Garg 07/16/2010 information from the religious leader and also from the grandmothers but has there is little transfer of information between the husband and the young mother. Figure 3: Network Analysis on flow of information on EBF to a young mother in a typical community Based on the network analysis and qualitative data available, since 2009, UNICEF Sierra Leone has put in place a two pronged strategy which aims to support a collective transformation within communities not only on EBF but on child health (with EBF and nutrition being a core component of it). The first step in this approach is to share (learn and provide) with communities knowledge about EBF within the broader framework of child health. A broader discussion on child health is a useful tool to trigger the aspirations of the community members for their respective communities and identify their role in supporting positive health outcomes in their community. This is done with a wide variety of community members and stakeholders – women and men, women leaders, religious and traditional leaders, youth groups, farming groups, market women leaders. 8 Gaurav Garg 07/16/2010 The second step is the setting up of We Pikin (Our Children in Krio) mother to mother support groups across the country. We Pikin groups are constituted by pregnant women, lactating mothers and other women members of the community. If there are cases of positive deviance in the respective communities, these mothers also form part of the group as agents of change. Each group has a democratically elected leader and We Pikin groups use dialogue and deliberation to identify barriers to exclusive breastfeeding and young child feeding practices, and also other health issues (immunisation, handwashing, malaria prevention). Partner NGO facilitators introduce counselling techniques and the We Pikin group members are encouraged to use these techniques to discuss EBF issues and suggest supportive actions and measures. Recently in some communities men have also started attending the meetings out of curiosity and due to advocacy from key influencers in the community. The groups are free to meet anywhere they want, under a mango tree in the village, in the veranda of the mosque or church or by the water point or any other location. The design of the group meetings is flexible and participants are free to talk about anything they want, with the NGO facilitator’s role being to bring up and direct the conversation towards EBF and health issues. Apart from this the NGO facilitator is largely non-visible in the discussions. A supporting component is UNICEF led advocacy with religious leaders, town and village chiefs to ensure their support and leverage their authority to mobilise the community (especially elders and men). Recently UNICEF Sierra Leone has signed a MoU with the Inter Religious Council of Sierra Leone to promote EBF and other essential practices for child survival and development. Towards this end chiefdom level consultation meetings are being organised with imams and pastors, so they can carry the messages to their congregations and also organise, take part in and lead discussion sessions on their premises and during outreach visits. UNICEF Sierra Leone is also planning to restart the Chiefs as Champions programme, 9 Gaurav Garg 07/16/2010 so Paramount Chiefs of chiefdoms in the country can take on the leadership roles in improving the child survival and education outcomes and enhancing the protective environment for children. The well documented success of the Community Led Total Sanitation (CLTS) intervention in many communities in Sierra Leone and their being declared open defecation free (ODF) has provided UNICEF Sierra Leone with a “foot in the door” to engage the same communities on other child health issues. In the next stage of expansion of the We Pikin groups, new groups will be set up in the ODF communities where community deliberation and action is at an advanced stage and propensity for collective transformation is high. Positive incentives and sanctions Programme activities do not provide monetary incentives for social transformation and behaviour change, rather the focus is on incentivising and regulating action through social recognition, leadership and moral obligation (especially with religious leaders) around EBF and child health issues. In its next scale of expansion, We Pikin will be expanded to also include UNICEF Sierra Leone’s education supported mothers groups (called Mothers Clubs) in order to scale up, consolidate gains and establish a stronger presence at the community level with a shared identity (concept of imagined communities by Benedict Anderson). Better health of children through exclusive breastfeeding ceteris paribus (made visible through Baby Shows), a shared sense of identity of a nationwide and growing women’s network and greater participation and mobilisation are some of the positive incentives to advance behaviour and social change. 10 Gaurav Garg 07/16/2010 Another positive incentive is linking up We Pikin groups the community radio which will give them an opportunity to have their voices and discussions heard beyond their villages and hamlets, a step towards advancing common knowledge on EBF and child health. These positive incentives are not only limited to the pregnant women and lactating mothers but also to the older women, grandmothers and the community elders and represents a step towards the re-categorisation of their role from being obstacles to being enablers and leaders in the development of the country and its children. In a recent consultation meeting with religious leaders for example, some of them said that being able to talk about EBF and take health related information to the communities (many admitted that information about the benefits of EBF was new to them) would make them “aware” and “champion” leaders. Sierra Leone yet being a centralised state, with ongoing decentralisation being a slow and tedious process, there exists a real hunger for information and willingness to assume leadership at the community level. This needs to be built on. Going forward – the need for attention to detail As the programme moves ahead, special attention needs to be given to ensure that We Pikin group discussions do not become one way information transfer sessions relying solely on message delivery through the partner NGO. Not all NGOs have the capacity to adopt and undertake a dialogue based pedagogy to the work, so this area will require capacity strengthening. The discussion between traditions and new information can be potentially fraught, so greater attention needs to be paid to how the rights based discourse is linked to people’s everyday lives (as in Tostan and also in the case of Mockus-Bogota). Also solely addressing EBF might limit the scope and the potential impact of the intervention, so this needs to be placed within the larger framework of child health and wellbeing therefore other 11 Gaurav Garg 07/16/2010 key health, protection and education issues need to be linked in, but without being forced on the communities. It needs to be a process of constant development and iteration. Links needs to be made between community radios, religious and traditional leaders and folk theatre groups, and the We Pikin groups and participants so each and everyone in the community has a potential stake in the collective transformation and this can be communicated even to external audiences. 12