Document 14671337
advertisement

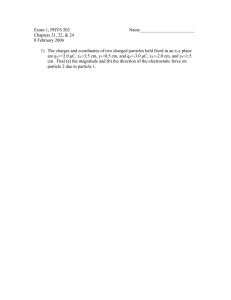
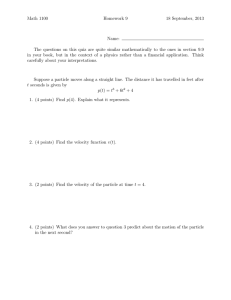
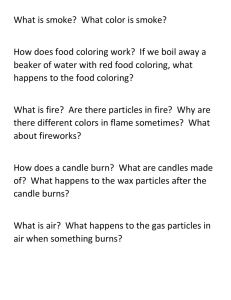
International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 254 Investigation of Performance of Mixing Ventilation Systems for Operating Room in the view of Infection Control Sanjeev B Thool1, Shobha Lata Sinha2 1 (Department of Mechanical Engineering, Rungta College of Engineering, Bhilai, India) sbthool@rediffmail.com 2 (Department of Mechanical Engineering, National Institute of Technology, Raipur, India) shobha_sinha@rediffmail.com Abstract: Effective ventilation system of operating room plays an important role in contamination control resulting in reduced possibility of post operation infection. The best way to treat an infection is to stop it from occurring in the first place. Towards the same objective, traditional mixing ventilation systems have been used since long period. Mixing room air distribution aims for dilution of polluted and warm/cool room air with cleaner and cooler/warmer supply air. In the present investigation, performance of two types of mixing ventilation systems i.e. one with “high supply low exhaust” (HSLE) and another with “low supply high exhaust” (LSHE) have been studied using Computation Fluid Dynamics (CFD) Technique. It have been observed that contaminant control has been found more effective in case of low supply and high exhaust ventilation as thermal plumes are playing the dominant role. Keywords: Mixing ventilation, Air distribution, Infection control, Operating Room, Surgical site. IJOART 1 Introduction One of the stages of design of indoor environment includes identification of the air distribution in room and evolution of its impact on contamination free room environment. Often it is performed in two stages: first, at the design phase air distribution is assessed on the basis of CFD predictions and physical measurements performed under laboratory conditions and then a field survey of air distribution and its impact on occupants is performed at the post occupancy stage. Airflow with different characteristics, including air temperature, mean velocity, turbulence intensity, frequency of velocity fluctuations, flow direction etc., can be generated which affects occupants comfort and indoor air quality. Mixing room air distribution aims for dilution of polluted and warm/cool room air with cleaner and cooler/warmer supply air. The air is supplied to the room with high initial mean velocity and the established velocity gradients generate high turbulence intensity aiming to promote good mixing and uniform temperature and pollution distribution in the occupied zone. Mixing Ventilation is an expression for an air distribution pattern, and not for a ventilation system. It can also be called an air distribution pattern with mixing effect or mixing air distribution. Mixing ventilation is traditional considered to be the air distribution, which is obtained by the use of diffusers with high momentum supply flow. But, by maintaining the proper direction of airflow, proper inlet and outlet orientation, proper inlet area to wall area ratio and distribution of heat source can demonstrate the air distribution pattern controlled by buoyancy from heat source. Selection of air distribution schemes is critical for the whole system performance with regard to the contamination removal effectiveness. Air distribution methods for inlets and outlets located on both opposite sided walls are presented in this study. A model of operating room with surgical staff members, patient, various surgical appliances have been created on which performance of two types of mixing ventilation systems i.e. one with “high supply low exhaust” (Fig. 1 a) and another with “low supply high exhaust” (Fig. 1 b) have been simulated. (a) High Supply Low Exhaust (b) Low Supply High Exhaust IJSER © 2014 http://www.ijser.org International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 255 Figure 1 Mixing Ventilation Configuration 2 CFD Modeling 2.1 Governing equations for turbulent flow Airflow pattern in room is calculated by using Eulerian approach. The airflow and the heat transfer are described mathematically by a set of differential equations for mass, momentum and energy equations based on the solution of the general advection – diffusion equation: 𝜕 𝜕𝑡 (𝜌𝜙) + 𝑑𝑖𝑣(𝜌𝑉𝜙) = 𝑑𝑖𝑣�𝛤𝜙 𝑔𝑟𝑎𝑑𝜙� + 𝑆𝜙 ………. (1) where, ϕ represents the independent variables: time averaged velocity components V (i.e. u, v, w), turbulent kinetic energy, k, dissipation rate of turbulent kinetic energy, ε, and enthalpy H. When ϕ is unity, the equation represents the conservation of mass. Expressions for the effective diffusivity, 𝛤𝜙 and source term, 𝑆𝜙 for each variable and the corresponding empirical numbers are described by Launder and Spalding (1972) [1]. In order to model the random feature of turbulent flows, a time decomposition (also called Reynolds decomposition) of the instantaneous flow variables ϕ(t) is introduced into the governing flows. 𝜙 (𝑡) = 𝜙� + 𝜙′(𝑡) ………. (2) The mean value of ϕ(t) is obtained by integrating ϕ(t) over a period of time dt that is much longer than the fluctuating duration: IJOART 1 𝑡+𝑑𝑡 𝜙� = 𝜏 ∫𝑡 𝜙(𝑡1 ) 𝑑𝑡1 ………. (3) Using “Reynolds rules”, all instantaneous flow equations are time averaged. In this case, time averaging will be presented by considering a three-dimensional flow (x, y and z directions) located in a gravity field opposed to y direction and assuming flow to be Newtonian, incompressible under nonisothermal condition Boussinesq hypothesis is employed, which neglects the variations of physical characteristics of the fluid in all equations, except for the density in the buoyancy term of the vertical momentum conservation equation (the density variations in the buoyancy term induce the vertical motion of the fluid in natural convection). Thus the various terms of the momentum conservation equations could be divided by the density ρ i of the fluid in reference conditions. 2.2 Equations for particle motion and dynamics Particle motion in carrier fluid is affected by various forces such as viscous drag force, gravity force, added mass force (virtual mass force), Brownian force, and pressure force. In this study, Brownian force has been ignored due to the large size of particle. The added mass force was considered in a few simulations and was found to have negligible influence on particle trajectory [2]. Thus in this study, steady viscous drag force, gravity force and pressure force have been considered. The methodology for predicting turbulent particle dispersion used in this study is originally laid out by Gosman and Ioammides [3] and validated by Ormancey and Martinon [4]. Turbulence was incorporated into the Stochastic model via the k – ε turbulence model (Alaniet al.) [5]. The Lagrangian particle tracking method is used to calculate individual trajectories by solving the momentum equation. By equating the particle inertia with external forces, the momentum equations can be expressed as: 𝑚𝑝 𝑚𝑝 𝑑𝑢𝑝 1 2 2 2 1 2 2 2 𝑑𝑡 = 2 𝐶𝐷 𝐴𝑝 𝜌�𝑢 − 𝑢𝑝 ���𝑢 − 𝑢𝑝 � + �𝑣 − 𝑣𝑝 � + �𝑤 − 𝑤𝑝 � + 𝑚𝑝 𝑔𝑥 ………. (4) 𝑑𝑡 = 2 𝐶𝐷 𝐴𝑝 𝜌�𝑣 − 𝑣𝑝 ���𝑢 − 𝑢𝑝 � + �𝑣 − 𝑣𝑝 � + �𝑤 − 𝑤𝑝 � + 𝑚𝑝 𝑔𝑦 ………. (5) 𝑑𝑣𝑝 IJSER © 2014 http://www.ijser.org International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 𝑚𝑝 𝑑𝑤𝑝 2 1 2 256 2 = 2 𝐶𝐷 𝐴𝑝 𝜌�𝑤 − 𝑤𝑝 ���𝑢 − 𝑢𝑝 � + �𝑣 − 𝑣𝑝 � + �𝑤 − 𝑤𝑝 � + 𝑚𝑝 𝑔𝑧 ………. (6) 𝑑𝑡 where u, v, w u p , v p , wp x p , y p , zp gx, gy, gz Ap mp - instantaneous velocity of air in x, y and z directions; particle velocity in x, y and z direction; movement of particle in x, y and z direction; acceleration due to gravity gravity in x, y and z directions; cross-sectional area of the particle; mass of particle; density of the particle; drag coefficient; time interval. - ρ CD dt where 24 3 𝐶𝐷 = 𝑅𝑒 �1 + 16 𝑅𝑒� 0.5 for Re ≤ 560; ………. (7) and 𝐶𝐷 = 0.44 …. for Re > 560 The Reynolds number of the particle is based on the relative velocity between particle and air. In laminar flow, particles released from a point source with the same weight would initially follow the airstream in the same path and then fall under the effect of gravity. Unlike laminar flow, the random nature of turbulence indicates that the particles released from the same point source will be randomly affected by turbulent eddies. As a result, it will be diffused away from the streamline at different fluctuating levels. In order to model the turbulent diffusion, the instantaneous fluid velocities in the three Cartesian directions u, v and w are decomposed into the mean velocity component and the turbulent fluctuating component as: 𝑢 = 𝑢� + 𝑢′ ; IJOART 𝑣 = 𝑣̅ + 𝑣 ′ ; 𝑤=𝑤 � + 𝑤′ where, 𝑢� and u’ are the mean and fluctuating components of velocity in x – direction. The same applies for y and z directions. The stochastic approach prescribes the use of a random number generator algorithm, which, in this case, is taken from Press et al. [6] to model the fluctuating velocity. It is achieved by using a random sampling of a Gaussian distribution with a mean of zero and a standard deviation of unity. Assuming isotropic turbulence, the instantaneous velocity of air are then calculated from kinetic energy of turbulence: 𝑢 = 𝑢� + 𝑁𝛼 ; 𝑣 = 𝑣̅ + 𝑁𝛼 ; 𝑤=𝑤 � + 𝑁𝛼 Where N is the pseudo-random number, ranging from 0 to 1, with 2𝑘 0.5 𝛼 =�3� ………. (8) The mean velocity, which are the direct output of CFD, determine the convection of the particles along the streamline, while the turbulent fluctuating velocity, Nα, contributes to the turbulent diffusion of the particle. 3 Brief of Operating Room In a typical operating room layout five surgical staff members, lights, machinery, tables and patient is considered for the baseline model for the CFD simulations. The brief description of operating room is given in the Fig. 1 and Table 1. The size of each inlet and exhaust grille is 0.61m x 0.36m. The most suitable operating value of ACH for this system is ranging from 20 h-1 to 25 h-1. The present CFD simulation is done taking ACH as 25 h-1 and air velocity as 0.64 m/s with temperature as 27 C°. IJSER © 2014 http://www.ijser.org International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 257 Figure 1 Baseline model of the operating room Table 1 Dimension of operating room and other available items Item Operating table Surgical lamp Anesthesia machine Back table Monitor stand Monitor Surgical staff (Two surgeon and three nurses) Patient Dimensions 0.64 m x 2.0 m x 0.9 m 0.55 m x 0.55 m x 0.1 m 0.6 m x 0.6 m x 1.1 m 0.64 m x 1.6 m x 0.9 m 0.6 m x 0.5 m x 1.20 m 0.5 m x 0.4 m x 0.6 m 0.46 m x 0.28 m x 1.8 m each 0.46 m x 0.28 m x 1.8 m IJOART 4 Boundary and Initial Conditions The velocity, temperature and turbulent transport quantities over the inlet boundary are prescribed from the experimental data found by Memarzadeh and Manning [7]. Outlet boundary conditions are set as the Neumann boundary condition. No slip boundary condition has been used at the wall. Wall functions are applied to describe the turbulent flow properties in the near wall reason. The initial conditions for particle tracking include the starting position and initial velocities of particles. For this study, the particles are assumed as skin flakes generated from the forehead of the surgical staff having the density of ρP = 850 kg/m3. Particles are equally divided into three size groups of 10, 15 and 20 microns [7]. The representative number of particles generated is 576 for 1 hour of surgery [7]. Other boundary conditions regarding the rate of generation of contaminant particles, heat generation from equipment and human bodies are illustrated in Fig. 2. When particles reach air supply inlets or exhaust outlets, they will escape and the trajectories terminate. When reaching a rigid object, particles may either attach to or rebound from the object’s surface. Particles in a ventilated room are most likely to attach to the surface since they usually cannot accumulate enough rebound energy to overcome adhesion [8]. It is therefore natural to terminate, or “trap”, a particle trajectory after hitting a rigid surface. This treatment was adopted and used in many CFD studies of the indoor environment. Nevertheless, the trap treatment worked well when the near-wall grid was sufficiently fine, like that which was used in the DNS simulation (McLaughlin; Narayanan et al.) [9, 10]. The trap treatment, however, is not suitable for the current situation, which uses a high Reynolds number k-ε model. Instead of using trap treatment, this study set the restitution coefficient to a very small value. By doing so, particles were immediately stopped without being trapped after reaching a surface. When particles acquired sufficient normal velocity, they escaped from the boundary layer and became resuspended. This implies that deposition is neglected. Such manipulation may only be suitable when particle deposition rate is very low. IJSER © 2014 http://www.ijser.org International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 258 Figure 2 Boundary Conditions 5 Particle Tracking The methodology is refined to consider different particle outcomes, namely: • The particle is vented from the room via ventilation and • The particle hits one of the two designated targets, namely, the surgical site (patient body put under surgery) or the top surface of the back table. Particles that are neither vented nor strike the target are assumed to remain in the room when the overall particle tracking time limit (1 hour in present case) is reached. IJOART 6 Results of Numerical Simulation Figure 3 and 4 show the numerical simulation results of both the systems obtained by FLUENT software [11]. In both cases, there is no airflow crossing the critical space around the operation table. In case of High Supply and Low Exhaust (HSLE), only curvature downward moment of airflow zones are created at four corners of operating Room. It is also observed that recirculation zones have been formed on both sides of the patient between two surgeons performing surgery. This causes the possibility of trapping of particles generating by surgeons in this region. In case of Low Supply and High Exhausts system (LSHE), only curvature upward moment of air flow zones are created at four corners of operating Room. It is also observed that vertical upward velocity vectors above the patient that is due to the formation thermal plumes. This thermal plumes are experienced due to the fact that there is no counteracting effect of horizontal velocity due to ventilation system on the convective flow of air due to relatively higher temperature of surgical site lamp. 8.67e-01 8.38e-01 8.09e-01 7.80e-01 7.51e-01 7.23e-01 6.94e-01 6.65e-01 6.36e-01 6.07e-01 5.78e-01 5.49e-01 5.20e-01 4.91e-01 4.62e-01 4.34e-01 4.05e-01 3.76e-01 3.47e-01 3.18e-01 2.89e-01 2.60e-01 2.31e-01 2.02e-01 1.73e-01 1.45e-01 1.16e-01 8.67e-02 5.78e-02 2.89e-02 0.00e+00 Y Z X (a) Velocity Contours (at vertical plane at z = 0) IJSER © 2014 http://www.ijser.org International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 2.00e-05 1.95e-05 1.90e-05 1.85e-05 1.80e-05 1.75e-05 1.70e-05 1.65e-05 1.60e-05 1.55e-05 1.50e-05 1.45e-05 1.40e-05 1.35e-05 1.30e-05 1.25e-05 1.20e-05 1.15e-05 1.10e-05 1.05e-05 1.00e-05 Y Z X (b) Stochastic Particle tracks (for size 10, 15 and 20 microns) Figure 3 Numerical Simulation of “High Supply and Low Exhaust” system 8.37e-01 7.95e-01 7.53e-01 7.11e-01 6.69e-01 6.28e-01 5.86e-01 5.44e-01 5.02e-01 4.60e-01 4.18e-01 3.77e-01 3.35e-01 2.93e-01 2.51e-01 2.09e-01 1.67e-01 1.26e-01 8.37e-02 4.18e-02 0.00e+00 IJOART Y Z X (a) Velocity Contours (at vertical plane at z = 0) 2.00e-05 1.90e-05 1.80e-05 1.70e-05 1.60e-05 1.50e-05 1.40e-05 1.30e-05 1.20e-05 1.10e-05 1.00e-05 Y Z X (b) Stochastic Particle tracks (for size 10, 15 and 20 microns) Figure 4 Numerical Simulation of “Low Supply and High Exhaust” system IJSER © 2014 http://www.ijser.org 259 International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 260 7 Particle Trajectory Simulation and Performance Discussion In these systems, the air moves across contaminated personnel and equipment before reaching the patient, resulting in localized areas of turbulent flow and low velocity recirculation zones, thus possibly increase the risk of infection. Figure 2(b) and 3(b) show the tracking path for particles having different diameters for both the cases. Results from the numerical simulation (Table 2, 3 and 4) show the effectiveness of these two cases in removing the particles via ventilation. LSHE system demonstrates better performance in removing the tiny sized particles (10 and 15 micron) from the operating room (Table 2 and 3), even better results demonstrated for particle size of 10 micron. But both systems show same performance in terms of percentage of particles strikes on the back table. LSHE ventilation system works with the thermal plume in the center of the room in driving the particles up to the high level exhausts. There is no noticeable difference between the performances of both systems in terms of percentage of particles removed from the operating room for particle size of 20 micron. However, it is verified that this performance is affected by the heat load in the operating room, which in turn is affected by the amount and type of equipment, people and lights used. Other variable may also affect the efficiency, for example the movement of people in the operating room, and the occurrence of open doors. Cases HSLE LSHE Table 2 Percentage of Particles Vented from Room and Percentage of Particles Strike on Surgical Site and Back Table for HSLE and LSHE for particle size of 10 micron Contaminated particles Contaminated Particles Contaminated Particles Total Number of (Skin flakes) escaped (Skin flakes) Strike on (Skin flakes) Strike on Particle particles from Operating Room Site of Surgery Back Table Source released Nos % Nos % Nos % Surgeons 192*2 = 384 304 79.1 0 0.0 1 0.26 Nurses 192*3 = 576 485 84.2 0 0.0 6 1.0 Surgeons 192*2 = 384 337 87.8 0 0.0 1 0.26 Nurses 192*3 = 576 516 89.5 0 0.0 6 1.0 IJOART Table 3 Percentage of Particles Vented from Room and Percentage of Particles Strike on Surgical Site and Back Table for HSLE and LSHE for particle size of 15 micron Cases HSLE LSHE Cases HSLE LSHE Particle Source Total Number of particles released Surgeons Nurses Surgeons Nurses 192*2 = 384 192*3 = 576 192*2 = 384 192*3 = 576 Contaminated particles (Skin flakes) escaped from Operating Room Nos % 307 79.9 482 83.7 307 79.9 491 85.3 Contaminated Particles (Skin flakes) Strike on Site of Surgery Nos % 0 0.0 0 0.0 0 0.0 0 0.0 Contaminated Particles (Skin flakes) Strike on Back Table Nos % 2 0.52 8 1.4 2 0.52 6 1.0 Table 4 Percentage of Particles Vented from Room and Percentage of Particles Strike on Surgical Site and Back Table for HSLE and LSHE for particle size of 20 micron Contaminated particles Contaminated Particles Contaminated Particles Total Number of (Skin flakes) escaped (Skin flakes) Strike on (Skin flakes) Strike on Particle particles from Operating Room Site of Surgery Back Table Source released Nos % Nos % Nos % Surgeons 192*2 = 384 285 74.2 1 0.26 4 1.00 Nurses 192*3 = 576 279 83.1 2 0.37 11 1.9 Surgeons 192*2 = 384 276 71.9 0 0.00 3 0.78 Nurses 192*3 = 576 681 80.1 1 0.17 8 1.39 IJSER © 2014 http://www.ijser.org International Journal of Advancements in Research & Technology, Volume 3, Issue 4, April-2014 ISSN 2278-7763 261 8. Conclusion From the simulation results, it is concluded that airflow distribution is predominantly control by the thermal plumes induced by the heat generating equipment in case of “Low Supply and High Exhaust” system. This helps in inducing and carrying the minute particles (10 and 15 micron size) along the airflow current formation due to thermal plume and removed out of operating room. Even though there in no noticeable difference in performance in terms of contaminated particles escaped from operating room for relatively large size particles (20 micron), “Low Supply and High Exhaust” system demonstrates better performance in terms of number of particles strike on site of surgery and back table. Acknowledgement This research received no specific grant from any funding agency in the public, commercial, or not-forprofit sectors. References [1] Launder BE, Spalding DB, Lectures in Mathematical Models of Turbulence. Academic Press, London, England, (1972). [2] Sinha SL, Arora RC, and Subhransu Roy, Numerical Simulation of Two Dimensional Room Air Flow with and Without Buoyancy, Energy And Buildings, 32(1), pp. 121–129 (2000). [3] Gosman D and Ioannide E, Aspect of computer simulation of liquid-fuelled combustion. AIAA 19th Aerospace Science Meeting 81-0323, 1 – 10, (1998). [4] Ormancey and Martinon J, Prediction of particle dispersion in turbulent flow, Physico Chemical Hydrodynamics, 5, 229 – 224, (1984). IJOART [5] Alani A Dixon-Hardy D and Seymour M, Contaminants transport modeling. EngD in Environmental Technology Conference, (1984). [6] Press WH, Teukolsky SA, Vetterling WT and Flannary BP, Numerical recipes in FORTRAN, 2d ed. Cambridge, Cambridge University Press, (1992). [7] Farhad Memarzadeh, Andrew P. Manning, Comparison of Operating Room Ventilation Systems in the Protection of the Surgical Site. [8] Hinds WC, Aerosol Technology, Properties, Behavior, and Measurement of Airborne Particles. Wiley, New York, (1982). [9] McLaughlin JB, Aerosol particle deposition in numerically simulated channel flow, Physics of Fluids A 1 (7), 1211–1224, (1989). [10] Narayanan C, Lakehal D, Botto L, Soldati A, Mechanisms of particle deposition in a fully developed turbulent open channel flow. Physics of Fluids 15 (3), 763–775, (2003). [11] FLUENT, Fluent 6.2 User’s guide. Fluent Inc., Lebanon, NH, (2005). IJSER © 2014 http://www.ijser.org