Overview of Glomerulonephritidies Madeleine V. Pahl, M.D. University of California, Irvine
advertisement

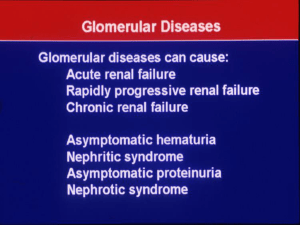
Overview of Glomerulonephritidies Madeleine V. Pahl, M.D. University of California, Irvine Objectives • To define common primary and secondary glomerular disorders • To discuss involved pathophysiology • To review their clinical presentation • To review clinical course and therapy Definition (R. J. Glassock) • A primary GN is a disease where the sole organ involved is the kidney (the glomeruli) • Clinical manifestations due to the consequences or pathophysiologic derangements that resulted in glomerular damage • In contrast secondary GNs have manifestations due to systemic disease and glomerular injury Presentation: Clinical Syndromes • Asymptomatic: hematuria (gross or microscopic) and/or proteinuria (< 3g/day) • Acute glomerulonephritis (AGN) • Rapidly progressive glomerulonephritis (RPGN) • Chronic glomerulonephritis (CGN) • Nephrotic Syndrome (NS) Clinical Syndromes: AGN • Abrupt onset of variable degrees of hematuria, proteinuria, reduced GFR, sodium and fluid retention, HTN and oliguria • Tendency to spontaneous recovery • Association with proliferative GN, ie. bacterial infection Clinical Syndromes: RPGN • • • • More insidious onset, not abrupt Dominated by progressive loss of GFR and oliguria Little tendency for spontaneous recovery Classification and terminology of this group of disorders (Type I, II, II) Clinical Syndromes: CGN • Clinical expression of a wide variety of glomerular diseases • Vague, all inclusive term refers to progressive reduction in GFR • Varying degrees of hematuria, proteinuria, HTN • Course may be protracted but usually relentless Composite plot of reciprocal serum creatinine versus time in six patients with chronic kidney disease. Clinical Syndromes: NS • • • • • • Heavy proteinuria (> 3-3.5g/day ) Reduced serum albumin Edema HTN Hyperlipidemia Lipiduria Pathology • Minimal change • Focal and segmental glomerulosclerosis • Proliferative GN o o o o Pure mesangial proliferative Endocapillary proliferative Extra-capillary proliferative (crescenteric) Membrano-proliferative • Membranous GN • Fibrillary/ Immunotactoid GN, Collageno-fibrotic GN, Lipoprotein GN (deposits of Apo E Nephron 83: 193, 1999) Normal Glomerular Histology From tutorial: J. Charles Jennette, M.D. Common Primary Glomerulonephritidies • • • • • Minimal Change Disease Focal Segmental Glomerulosclerosis (FSGS) IgA Nephropathy (Bergèr’s Disease) Membranoproliferative GN (Types I, II, III) Membranous GN Case #1 • 20 yo Caucasian male develops frothy urine and notes ankle edema. He takes no medication or drugs. • On exam he has a BP 180/98 and pitting lower extremity edema. • He has a Cr = 2mg/dl and 12g/day urinary protein excretion. • HIV, HBSAg, and Hepatitis C negative. FSGS • Incidence among all biopsied patients rising, up to 25% of all adults • Most common pattern among African Americans, some secondary forms more common in whites (obesity and hereditary) • Children usually present with NS, adults with asymptomatic proteinuria UpToDate® FSGS UpToDate® FSGS: Histopathologic Variants • Glomerular “tip” lesion: o epithelial cell proliferation and sclerosis in segment adjacent to origin of proximal tubule, o common in whites with heavier proteinuria, preserved GFR, good response to treatment and outcome • “Collapsing/malignant” variant: o global collapse of capillary loops with visceral epithelial cell proliferation (similar to HIV), o common in AA with massive proteinuria, worse prognosis • Obesity: o fewer glomeruli with FSGS but remaining with glomerulomegaly. o Increasing in prevalence, likely white, less likely NS, progression slower FSGS-Pathophysiology • Podocyte injury (JASN 2012; 23:381-99) • Unknown: increased glomerular permeability factor Suggested by studies demonstrating in-vitro glomerular permeabiliy (NEJM 334:878, 1996) o Certain forms of the soluble urokinase plasminogen activating receptor (suPAR) (Nat Med. 2011;17(8):952) o Expression of a specific microRNA called miR193a produced FSGS in mice (Nat Med. 2013 Apr;19(4):481-7) • Controversial role of Parvovirus B-19 (KI 59:2126, 2001) • Evidence for hyperfiltration: Glomerulomegaly and obesity, sleep apnea, or remnant kidney • Genetic Defect: role of MYH9 or APOL1 in African Americans (Nat Genetics. 2008 Oct;40(10):1185-92; Science. 2010 Aug 13;329(5993):841-5) FSGS: Clinical Course • Tendency for progressive renal failure, ESRD in 5-20 yrs • Factors associated with progression: o magnitude of proteinuria, higher serum Cr, o AA ethnicity, response to corticosteroids, o degree of sclerosis, TI damage, “collapsing” variety • Recurrence in allograft in up to 30%. Treatment with plasmapheresis (Clin Nephrol 56:271, 2001) and Rituximab (Transplantation. 2009 Aug 15;88(3):41720) FSGS: Treatment • Prednisone 0.5-2.0 mg/kg/day. Total duration of 6 month before declaring pt steroid resistant, then alternate day. Complete and partial response rate 50-60% ( JASN 9:1333, 1998) • Cytotoxic therapy (cyclophosphamide, chlorambucil, MMF) may be useful but not proven (KI 55(S70): S26, 1999). • CsA at 5 mg/kg/day may be effective, relapses common, long term use may be required (KI 55(S70): S26, 1999). • Synthetic ACTH (Am J Kidney Dis. 2006;47(2):233) • Rituximab (Intern Med. 2012;51(7):759-62) • Plamapheresis, in recurrent disease in transplant patients (Semin Nephrol. 2000;20(3):309) Common Secondary Glomerulonephritidies • • • • • • • Infection Malignancy Drugs and toxins Metabolic Rheumatologic Disorders Vasculitidies Hereditary/Familial GLOMERULAR DISEASES ASSOCIATED WITH INFECTIOUS AGENTS, TUMORS OR DRUGS Infection Glomerular disease Bacteria of all types MCGN, diffuse proliferative GN E coli and Shigella species HUS Malaria Membranous GN, MCGN Syphilis Membranous GN Leprosy, schistosomiasis, TB Amyloidosis Hepatitis B virus FSGS, MCGN, Membranous Hepatitis C virus FSGS, MCGN, Membranous HIV FSGS (collapsing variant), IgA nephropathy, immune complex GN, HUS Parvovirus FSGS Tumor Glomerular Disease Lymphoma and leukemia Minimal change disease, Membranous, MCGN Myeloma Amyloidosis, light chain nephropathy Carcinoma (lung, gastrointestinal, uterine, prostate, etc) Membranous, MCGN, HUS Drug Glomerular Disease Heroin FSGS, MCGN NSAIDs Minimal change disease, Membranous Penicillamine, captopril Membranous Tacrolimus, cyclosporine HUS Bisphosphonates FSGS Case #2 • 28 yo woman with known SLE for 1 year and history of arthralgias develops proteinuria and hematuria • BP 138/86, faint malar rash, mild pitting edema • Cr 0.7 • 24 hr: 2.5 g of protein • DS-DNA positive high titer and low C3 Classification of Lupus Nephritis ISN Classification • • • • • • • KI 2004;65(2):521 Minimal mesangial lupus nephritis (class I) Mesangial proliferative lupus nephritis (class II) Focal lupus nephritis (class III) Diffuse lupus nephritis (class IV) Membranous lupus nephritis (class V) Sclerosing lupus nephritis (class VI) a healing /scarring of prior injury; advanced stage of chronic class III, IV, or V Overlap of SLE and ANCA GNs — ANCA found in 20% of SLE and some have superimposed ANCA GN, with prominent necrosis and crescent with minimal endocapillary proliferation or subendothelial deposits Comparison to WHO Class IV • Most common and severe (historically 50% developed ESRD in 5 yrs) • Class IV showed higher rate of ESRD compared to I, II, III or V—14.5% vs 4.6% • Present with hematuria and proteinuria /nephrotic syndrome, frequent HTN and reduced GFR. • Serology: reduced C3, positive anti-DNA • Histology: > 50 % glomeruli with endocapillary GN. • Subclasses: o Diffuse segmental or global proliferative nephritis, active vs chronic and/or sclerosing o Active disease: necrotizing changes, crescents and marked IgG and C3 deposition with thickening of GN capillary wall like MPGN. Histology: Class IV Severe Lupus Nephritis: “Optimal” Therapy • There is no universally agreed upon “optimal therapy” for severe proliferative lupus nephritis • Therapeutic approaches are divided into “Induction” therapy (first 6-12 months of treatment) and “Maintenance” therapy (beyond 6-12 months • Generally, the earlier intensive “Induction” therapy is begun the better the response • Combined therapy (cytotoxic agents and steroids) are indicated in most cases • Complete and/or partial remissions are the goal of induction therapy, accompanied the minimum amount of untoward side-effects (particularly infection) Lupus Nephritis: “Induction” therapy choices Probability of developing ESRD (prepared by R. Glassock, 2007) • Oral cyclophosphamide 2.0mg/kg/d for 3-6 months, with daily or alternate-day oral prednisone (±or 3 IV MP pulses) • IV Cyclophosphamide 5001000mg/m2 monthly for 3-6 months (mini-dose or maxidose) with daily or alternate-day oral prednisone (± monthly IV MP pulses) • Oral Mycophenolate mofetil 2-3gms/d, with oral daily oral alternate-day prednisone (± IV MP pulses) • Oral Tacrolimus (±MMF) ALMS Trial: MMF v IV CP Induction Therapy • Largest prospective randomized trial in SLE, 88 centers, 370 patients with Class III, IV, V • At the end of a 6 months induction: no difference in remission rate for oral MMF compared to “maxi-dose” IV CP in patients with “severe” lupus nephritis (neither superior or inferior)- about a 60% remission rate overall • During a 6 months course of induction the adverse event rates were similar for oral MMF and IV CP (leukopenia, alopecia, amenorhea, infection in CP; anemia, diarrhea, infections in MMF) (Appel G, et al JASN, 2009 May;20(5):1103-12) Lupus Nephritis: Maintenance Therapy • The primary goals of maintenance therapy in LN are: 1) to prevent or minimize relapses (“renal flares” ) 2) to reduce the side-effects of the therapy; 3) to improve quality of life 4) to reduce the risk of ESRD and death • Evaluation of efficacy and safety of maintenance therapy requires long-term follow up (perhaps 5 years minimum) Clinical Trial in Maintenance Therapy • ALMS trial: after 3 yrs regardless of induction therapy, MMF (16.4% flare) was superior to AZA (32.4% flare), irrespective of race, gender,region and more AE with AZA (NEJM 2011; 365:1886-95) • MAINTAIN nephritis trial (EURO-lupus nephritis trial high vs low dose cyclophosphamide) at 48 mo. no statistical difference between AZA (25% flare) and MMF (19% flare). (Ann Rheum Dis 2010; 69:2083-89) • Recent review concludes that maintenance therapy with either MMF or AZA is overall well tolerated and leads to excellent results (Nephrol. Dial. Transplant. (2013) 28 (6): 1371-1376).