Urinalysis Orders Among Patients Admitted to the Inpatient General Medicine Service
advertisement

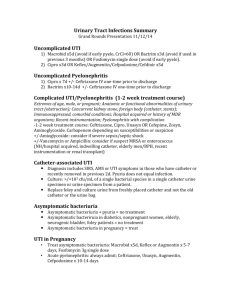
Urinalysis Orders Among Patients Admitted to the Inpatient General Medicine Service Cost Conscious Project Miriam Nojan PGY-2 Are urinlyses being ordered and acted on appropriately among inpatients admitted to the General Internal Medicine wards? Asymptomatic Bacteriuria Asymptomatic Bacteriuria or asymptomatic urinary infection, is isolation of a specified quantitative count of bacteria in an appropriately collected urine specimen obtained from a person without symptoms or signs referable to urinary infection IDSA Guidelines Pyuria accompanying asymptomatic bacteriuria is not an indication for antimicrobial treatment (A-II) Screening for or treatment of asymptomatic bacteriuria is not recommended for the following persons: ◦ ◦ ◦ ◦ ◦ ◦ Premenopausal, nonpregnant women (A-I) Diabetic women (A-I) Older persons living in the community (A-II) Elderly, institutionalized subjects (A-I) Persons with spinal cord injury (A-II) Catheterized patients while the catheter remains in situ (A-I) Evidence Pyuria is evidence of inflammation in the genitourinary tract and is common in subjects with asymptomatic bacteriuria. Pyuria is present with asymptomatic bacteriuria in: ◦ ◦ ◦ ◦ ◦ ◦ ∼32% of young women 30%–70% of pregnant women 70% of diabetic women 90% of elderly institutionalized patients 90% of hemodialysis patients 30%–75% of bacteriuric patients with short-term catheters in place ◦ 50%–100% of individuals with long-term indwelling catheters in place Evidence Asymptomatic bacteriuria is not associated with long-term adverse outcomes, such as hypertension, chronic kidney disease, genitourinary cancer, or decreased duration of survival Treatment of asymptomatic bacteriuria neither decreases the frequency of symptomatic infection nor prevents further episodes of asymptomatic bacteriuria Study Design Retrospective Cohort Study N = 12 Inclusion Criteria: ◦ Adult patients admitted to the inpatient Medicine Service who underwent UA during 04/12 – 04/22 upon admission Exclusion Criteria: ◦ ICU / OSH transfers Appropriate UA: ◦ ◦ ◦ ◦ AKI Dysuria or urinary complaints Fever / Sepsis of unknown origin AMS in elderly Inappropriate UA: ◦ Fever with obvious alternative source (eg. Pneumonia, cellulitis) ◦ Absence of urinary complaints Age Chief Complaint UTI Sx UA Indicated (Y – x / N) Urine Microscopy / Culture (+ / -) Antimicrobial Therapy Initiated Antimicrobial Therapy Indicated 71 BL LE Cellulitiis N N Negative No No 58 Chronic LE Cellulitis / Hypotension / AKI N Y Negative No No 52 Myasthenia w/Cough / Sepsis N Y Negative No No 45 Pulmonary Embolism N N Negative No No 80 Abdominal Pain / Dysuria Y Y Positive Yes Yes 47 Nasopharyngeal CA w/Bilateral Hand Numbess N N Negative No No 55 SVC Syndrome / Incidental leukocytosis N Y Negative No No 85 Cough / Hypoxia N N Negative No No 71 BL LE Cellulitis N N Negative No No 35 RCC w/Fevers / AKI Y Y Negative No No 66 Chest Pain (Hx CKD; Cr at baseline) N N Negative No No 77 Fever / AMS / Dysuria Y Y Positive Yes Yes Results Baseline Characteristics ◦ Mean Age: 61.8; Sex 6 Males / 6 Females UA Indicated in 6/12 (50%) patients UA Culture / Microscopy was positive for infection in 2/12 (17%) patients No instances of inappropriate treatment of asymptomatic bacteriuria Analysis Healthcare Bluebook: ◦ UA: $10 ◦ Urine Culture : $21 ◦ Ceftriaxone (1g/day): $10 After controlling for other variables, those most likely to undergo UA without an appropriate clinical indication had multiple comorbidities. One possible explanation is that patients with complex medical problems are more likely to undergo a broader net of investigations. Discussion Up to 50% of UA’s ordered in the inpatient setting during the study period analysis were done so without indication Treatment of asymptomatic bacteriuria may itself be associated with undesirable outcomes, including subsequent antimicrobial resistance, adverse drug effects, and cost. Positive UA results from these asymptomatic patients significantly increased their probability of receiving additional low-value care, including UC and antibiotics for asymptomatic pyuria or bacteriuria Take Away These findings highlight the harms of UA overuse in this patient population because positive UA results can introduce cognitive biases in favor of a UTI diagnosis even when patients lack accepted guideline-based criteria Limiting indiscriminate UA ordering has the potential to improve resource utilization and antimicrobial prescribing practices among GM patients References Lindsay E. Nicolle, Suzanne Bradley, Richard Colgan, et al. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asymptomatic Bacteriuria in Adults Nicolle LE. Asymptomatic bacteriuria in the elderly. Infect Dis Clin North Am. 1997 Sep;11(3):647-62. Penny Yin, MD; Alex Kiss, PhD; Jerome A. Leis, MD, MSc. Urinalysis Orders Among Patients Admitted to the General Medicine Service. JAMA Intern Med. 2015;175(10):1711-1713.