BNP Ordering UC Irvine Medical Center Department of Internal Medicine DSR2 Cost-Conscious Project

BNP Ordering
UC Irvine Medical Center
Department of Internal Medicine
DSR2 Cost-Conscious Project
4/6/15
Brain natriuretic peptide (BNP)
• Hormone initially identified in the brain but released primarily from the heart, particularly the ventricles
• Cleavage of the pro-hormone proBNP produces biologically active BNP as well as biologically inert N-terminal pro-BNP (NT-proBNP)
BNP Assay Purity
• Available commercial assays for plasma BNP or NTproBNP actually measure mixtures of peptides
• Plasma BNP assays appear to detect various degradation products of BNP as well as proBNP
• Assays for NT-proBNP likely also detect proBNP
• The relative contribution of individual natriuretic peptides has not yet been elucidated
Causes of Elevated BNP
1.
Cardiac conditions:
• Left or right ventricular heart failure
• Valvular disease
• Left ventricular hypertrophy
• Myocarditis
• Coronary artery disease
• Myocardial trauma (contusion, cardiac surgery, cardioversion)
• Atrial fibrillation
• Pericardial disease
Causes of Elevated BNP
2.
Pulmonary disease:
Acute pulmonary embolism (i.e. RV failure)
Pulmonary hypertension
Obstructive sleep apnea
Infection
Chronic obstructive lung disease
Causes of Elevated BNP
3.
Neurologic disorders: CVA (ischemic or hemorrhagic)
4.
Critical illness:
Sepsis
Burns
Transfusion associated circulatory overload (TACO)
5.
Toxins:
Chemotherapy
Snake bites
Causes of Elevated BNP
6.
Renal insufficiency
7.
Anemia
8.
Cirrhosis
9.
Hyperaldosteronism
10.
Hypertension
Class I Indications for BNP Testing
• To support clinical decision-making regarding the diagnosis of HF in the setting of dyspnea
• To support clinical judgment for the diagnosis of acutely decompensated HF
• Establishing prognosis or disease severity in both acutely decompensated and chronic HF
Class IIa Indication for BNP Testing
As a guide to achieve optimal dosing of HF therapy in select euvolemic patients followed in a well-structured HF disease management program
BNP Ordering on Presentation
• Study population: 21 UCI inpatients
• Teams: Medicine ward teams, CCU, MICU
• Time period: 1 week in March 2015
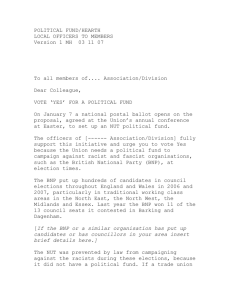
BNP Ordering on Presentation
Indication
Decompensated heart failure
Atrial fibrillation
Sepsis
CKD
Pneumonia
Pulmonary embolism
Cor pulmonale
Cardiac arrest
Anemia
Altered mental status
Pancreatitis
Pleural effusion
Vascular insufficiency
Number Ordered
5
1
1
1
2
2
2
2
1
1
1
1
1
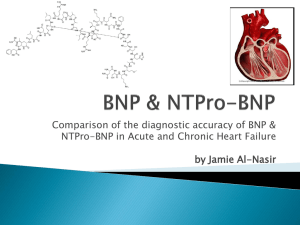
BNP Ordering on Presentation
Test Indicated
Test Not Indicated
Potentially Indicated
Number
7
3
11
Diagnoses
Decompensated HF, A-Fib
Pancreatitis, cardiac arrest,
AMS
CKD, PNA, PE, cor pulmonale, sepsis, anemia, pleural effusion, vascular insufficiency
Cost of BNP Test
• Average cost of BNP assay alone = $32
• Estimated cost per test (including cost of phlebotomy, technician, reagent, calibration, equipment rental) = $100
• Cost of ordering tests not indicated or only potentially indicated = $1400 per week
• Extrapolated to cost per year = $72,800
Conclusions
• Physicians should be educated about the indications for
BNP ordering
• However, indications can be construed as vague
• Clinical impact of ordering BNPs is unclear
• Medical personnel should be made aware of the cumulative cost of ordering BNPs as every extraneous order increases our overall high cost of healthcare
Limitations
• Snap shot of 1 week (variability of providers, symptoms, diagnoses)
• Extrapolation is not really a valid representation
• Small sample size
• Patients limited to medicine services though it was not clear whether ER or Medicine physician ordered BNP
• Poor/inadequate documentation?
References
Colucci WS, Chen HH. Natriuretic peptide measurement in heart failure. In: UpToDate,
Post TW (Ed), UpToDate, Waltham, MA. (Accessed in April 2015.)
Heidenreich PA, Gubens MA, Fonarow GC, et al. Cost-effectiveness of screening with Btype natriuretic peptide to identify patients with reduced left ventricular ejection fraction. J Am Coll Cardiol. 2004;43(6):1019-1026.
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary. A report of the American college of cardiology foundation/American heart association task force on practice guidelines. J Am Coll
Cardiol. 2013;62(16): 1495-1539.