The hierarchical STrucTure of The DimenSional aSSeSSmenT of PerSonaliTy PaThology (DaPP-BQ)
advertisement
")
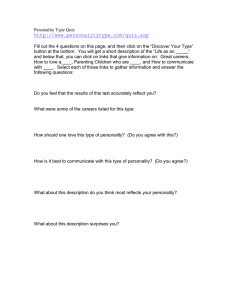
Journal of Personality Disorders, 25(4), 504–516, 2011 © 2011 The Guilford Press The Hierarchical Structure of the Dimensional Assessment of Personality Pathology (DAPP-BQ) Shauna C. Kushner, MA, Lena C. Quilty, PhD, CPsych, Jennifer L. Tackett, PhD, and R. Michael Bagby, PhD, CPsych Hierarchical personality models have the potential to identify common and specific components of DSM-IV personality disorders (PDs), and may offer a solution for the re-tooling of personality pathology in future versions of the DSM. In this paper, we examined the hierarchical structure of the Dimensional Assessment of Personality Pathology—Basic Questionnaire (DAPP-BQ; Livesley & Jackson, 2009) and the capacity of various trait components at different levels to predict DSM-IV PD symptoms. Participants were 275 psychiatric outpatients and 365 undergraduate students. Goldberg’s (2006) bass-ackwards method was used to investigate the hierarchical structure of the DAPP-BQ. The predictive capacity of hierarchy components was assessed. We found that Level 5 of the hierarchy enhanced the capacity of the DAPP-BQ for predicting DSM PD symptoms beyond a four-factor structure, particularly for borderline PD. The predominant model of personality pathology in psychiatry and clinical psychology is the DSM Axis II personality disorder (PD) classification system. This system, as codified in the DSM-IV-TR, uses a categorical approach to diagnosis and is composed of 10 ostensibly distinct disorders. The categorical model of PDs has been the subject of much criticism, including excessive diagnostic co-morbidity between disorders, diagnostic heterogeneity within disorders, inadequate symptom representation of personality pathology most generally, and arbitrary diagnostic thresholds (Widiger & Trull, 2007). These criticisms are well substantiated empirically, and in turn have prompted the development of alternative conceptualizations or approaches to understanding personality pathology (Trull & Durrett, 2005). Common among these various alternatives is the contention that a dimensional model better represents personality pathology than the current categorical system (Widiger, Simonsen, Krueger, Livesley, & Verheul, 2005). In the current investigation, we examine the hierarchiFrom University of Toronto. Address correspondence to Dr. R. Michael Bagby, Centre for Addiction and Mental Health, 250 College Street, Suite 647A, Toronto, Ontario, M5T 1R8, Canada; E-mail: michael_bagby@ camh.net 504 HIERARCHICAL STRUCTURE 505 cal structure of one of these alternative models—Livesley’s dimensional model of personality pathology (Livesley, 2005)—and attempt to demonstrate its validity at various hierarchical levels (e.g., Markon, Krueger, & Watson, 2005; Tackett, Quilty, Sellbom, Rector, & Bagby, 2008). Livesley’s Dimensional Model of Personality Pathology Livesley, Jackson, and Schroeder (1989) delineated a dimensional model for classifying personality pathology using a two-staged procedure. In the first stage, a pool of self-report questionnaire items was generated; these items were derived from several sources, including DSM-III descriptions of PD symptoms and features, an extensive literature review of personality pathology, and clinical opinion. At the second stage, these items were subjected to factor analysis, the latent factors from which formed the foundation for the development of personality scales that form the Dimensional Assessment of Personality Pathology-Basic Questionnaire (DAPP-BQ; Livesley & Jackson, 2009; Livesley, Jang, & Vernon, 1998). The DAPP-BQ scales assess 18 lower-order dimensions of personality pathology, including Affective Instability, Anxiousness, Callousness, Cognitive Distortions, Compulsivity, Conduct Problems, Identity Problems, Insecure Attachment, Intimacy Problems, Narcissism, Oppositionality, Rejection, Restricted Expression, Self-harming Behavior, Social Avoidance, Stimulus Seeking, Submissiveness, and Suspiciousness. These dimensions have been found to distinguish between samples with and without PDs (Gutiérrez-Zotes et al., 2008), and between samples with different PDs (Bagge & Trull, 2003). The pattern of correlations between the DAPP-BQ dimensions and PD symptom counts has also been examined, the results from which are interpreted to provide support for the validity of the DAPP-BQ (Bagge & Trull, 2003; Gutiérrez-Zotes et al., 2008; Pukrop, Gentil, Steinbring, & Steinmeyer, 2001). The factor structure of the DAPP-BQ has been extensively investigated. Livesley et al. (1998) initially reported that the DAPP-BQ lower order ­personality scales cluster into four higher-order latent factors or ­domains: (1) Emotional Dysregulation, (2) Dissocial Behavior (3) Inhibitedness, and (4) Compulsivity. These factors have been extracted in subsequent factor analytic investigations, which have used diverse samples and different language groups (Bagge & Trull, 2003; Brezo, Paris, Tremblay, Vitaro, & Turecki, 2008; Gutiérrez-Zotes et al., 2008; Pukrop et al., 2001; Simonsen & Simonsen, 2009). Other investigators examining the underlying latent structure of the DAPP-BQ, however, have recovered a five-factor solution (Clark, Livesley, Schroeder, & Irish, 1996; Goldner, Srikam­es­waran, Schroeder, Livesley, & Birmingham, 1999; Gutiérrez-Zotes et al., 2008; Larstone, Jang, Vernon, & Wolfe, 2002; Jang, Livesley, & Vernon, 1999; Schroeder, Wormworth, & Livesley, 1992; Wang, Du, Wang, Livesley, & Jang, 2004), in which the Dissocial Behavior domain parses into two separate domains. For example, Schroeder et al. reported two dissocial be- 506 KUSHNER ET AL. havior factors, one related primarily to high levels of extraversion and another related to low agreeableness. Goldner et al. also recovered two dissocial factors, which they labeled as psychopathy and behavioral disturbance. To date, no studies have reported on the capacity of the DAPPBQ higher-order factors to predict DSM-IV PD symptom counts. The Hierarchical Structure of Personality and Enhanced Validity The different factor solutions of the DAPP-BQ may be interpreted to reflect different levels in the hierarchical structure of personality. Using both meta-analytical and empirical data, Markon and colleagues (2005) illustrated that different models of personality can be integrated into a single hierarchical structure. The authors were silent on the matter of which level of the hierarchy is ideal. The answer for this issue likely differs depending on the specific domain of interest. Using the trait domains of the five-factor model (FFM), Tackett, Quilty, et al. (2008) demonstrated that the higher-order levels of the personality hierarchy successfully differentiated individuals with and without internalizing disorders and individuals with different internalizing disorders. Based on these results, Tackett and colleagues revealed the potential applicability of hierarchical models to the development of a new, re-modeled psychiatric nosological system as well as to the enhancement of differential diagnosis in the current system. Again, the level of the hierarchy providing maximal explanatory power may differ for diagnostic groups as well as specific diagnoses. Applying this to a specific diagnostic group, PDs, is the focus of the present study. The Current Investigation In the current investigation, our aims were two-fold: (1) to delineate the hierarchical structure of personality pathology as measured by the DAPPBQ, and (2) to examine the capacity of the components of the DAPP-BQ hierarchy to predict PD symptoms. Because as many as six factors have been extracted in previous factor analytic investigations of the DAPP-BQ, we extracted one through six factors from the 18 lower-order dimensions. To maximize statistical power in the analyses and expand the distributional variance of the constructs at hand, hierarchy components were extracted using data from both clinical and nonclinical samples. Given the replicability of the four factor solution of the DAPP-BQ (Bagge & Trull, 2003; Brezo et al., 2008; Gutiérrez-Zotes et al., 2008; Livesley et al., 1998; Pukrop et al., 2001; Simonsen & Simonsen, 2009), we hypothesized that Emotional Dysregulation, Dissocial Behavior, Inhibitedness, and Compulsivity would clearly represent the four-factor solution in these analyses. Based on previous investigations (Bagge & Trull, 2003; Gutiérrez-Zotes et al., 2008; Pukrop et al., 2001), we also hypothesized that HIERARCHICAL STRUCTURE 507 higher-order components of the hierarchy would account for considerable variability in DSM-IV PD symptoms. Given the exploratory nature of our analyses, only tentative a priori hypotheses were made concerning the nature of the components beyond Level 4 of the hierarchy. Based on previous investigations suggesting a five-factor solution have typically delineated two dissocial behavior factors, we did hypothesize that the dissocial behavior factor would parse into two at Level 5 of the DAPP-BQ hierarchy. As only one study has previously extracted six factors from the DAPP-BQ (Gutiérrez-Zotes et al., 2008), no predictions about Level 6 were made. Method Participants Clinical Sample. Participants in the clinical sample were 275 psychiatric outpatients (100 male, 175 female) enrolled in a clinical research study of mood disorders and behavior. Participant lifetime diagnoses included bipolar I disorder (n = 110), bipolar II disorder (n = 20), bipolar disorder not otherwise specified (NOS; n = 6), cyclothymic disorder (n = 1), major depressive disorder (n = 119), dysthymic disorder (n = 18), and depressive disorder NOS (n = 1). The mean age of the sample was 43.02 years (SD = 11.58). Ethnoracial status was self-reported by all participants: 238 were Caucasian; 11 were Asian; 10 were Black Canadians of Caribbean descent; 6 were Arabic/Islamic African; 4 were Latin American; 4 were East Indian; 1 was an Aboriginal Canadian; and 1 reported belonging to multiple visible minorities.1 Nonclinical Sample. Participants in the nonclinical sample were 365 undergraduate psychology students (69 male, 293 female). The mean age of the sample was 21.86 years (SD = 4.98). Ethnoracial status was selfreported by 358 participants: 197 were Caucasian; 101 were Asian; 22 were Black Canadians of Caribbean descent; 13 were Arabic/Islamic African; 4 were Latin American; and 21 reported belonging to other visible minorities. Procedure Participants in each sample were recruited as part of two separate data collection protocols. Participants in the clinical sample were solicited from the community by advertisement, and attended a clinical research laboratory where they completed two days of extensive assessment of personality and psychopathology as part of a larger investigation. Participants in the nonclinical sample were solicited by a research assistant, and were given a battery of questionnaires to be returned after completion. All participants received financial compensation. Participation in the clinical sample was limited to individuals who met DSM-IV criteria for a lifetime mood 1. These categories approximate the ethnoracial classifications of Statistics Canada. 508 KUSHNER ET AL. disorder as assessed by the SCID-I/P (First, Spitzer, Gibbon, & Williams, 1995); exclusion criteria included severe mania, active psychotic symptoms, and/or diagnoses of schizophrenia or schizoaffective disorder. ­Participation in the nonclinical sample was not subject to pre-specified inclusion/exclusion criteria. There were significant differences between participants in the clinical and nonclinical samples for age, t(637) = 31.26, p < .01, and sex, χ2(1) = 24.00, p < .01. Measures Dimensional Assessment of Personality Pathology—Basic Questionnaire (DAPP-BQ; Livesley & Jackson, 2009). The DAPP-BQ is a 290-item selfreport questionnaire assessing characteristic feelings and behaviors. Items are rated on a five-point Likert scale, ranging from “very unlike me” to “very like me.” Scoring for the DAPP-BQ generates scores for the 18 lower order dimensions, as described above. Scale reliability as assessed by Cronbach’s alpha for the DAPP-BQ dimensions ranged from .90 (Rejection) to .95 (Self-Harm), with an average of .92. Diagnostic Interview for DSM-IV Personality Disorders (DIPD-IV; Zanarini, Frankenburg, Sickel, & Yong, 1996). The DIPD-IV is a semi-structured interview for assessing the criteria of DSM-IV Axis II disorders. To obtain an Axis II diagnosis for a given PD on the DIPD-IV, a threshold number of criteria must be coded as present and clinically significant. The DIPD-IV was administered only to the clinical sample. The DIPD-IV was administered by experienced research assistants trained in diagnostic interviewing and the administration of the DIPD-IV. Although interrater reliability was not formally assessed for the current study, all interviewers completed a structured training protocol, and attended biweekly case conference meetings to ensure assessment consistency. Results The Hierarchical Structure of the DAPP-BQ Goldberg’s (2006) bass-ackwards method was used to explore the hierarchical structure of the DAPP-BQ. This method involves the top-down extraction of higher order traits from a set of variables to derive a hierarchical structure. Following the application employed by Tackett et al. (2008), the dimensions of the DAPP-BQ were subjected to principal components analyses with varimax rotation, beginning with the first principal component and iteratively extracting successive levels of the hierarchy. Regression-based factor scores at each level were correlated to provide path estimates between factors at contiguous levels of the hierarchy. Figure 1 displays the six levels of the hierarchy delineated using the bass-ackwards method. For each hierarchy component, dimensions with loadings greater than the absolute value of .60 and below .40 on the remaining factors were considered in the interpretation of the component. Complete factor loading matrices are available upon request. HIERARCHICAL STRUCTURE 509 FIGURE 1.Structure of the DAPP-BQ hierarchy delineated using the bass-ackwards method. Level 2. At Level 2, the first component was defined primarily by high loadings of the Identity Problems, Social Avoidance, Anxiousness, Oppositionality, Cognitive Distortion, Submissiveness, Restricted Expression and Self-harming Behavior dimensions, and labeled Emotional Dysregulation. The second component was defined by high loadings of the Rejection, Narcissism, Callousness, and Stimulus Seeking dimensions, and labeled Dissocial Behavior. Level 3. At Level 3, Emotional Dysregulation split into an Emotional Dysregulation component (Anxiousness, Identity Problems, Affective Instability, Submissiveness, Social Avoidance, Oppositionality, Cognitive Distortion, and Insecure Attachment) and an Inhibitedness component (Intimacy Problems and Restricted Expression). Dissocial Behavior (Rejection, Callousness, Conduct Problems, and Stimulus Seeking) was replicated at Level 3. Level 4. At Level 4, four components emerged resembling those reported in previous investigations (Bagge & Trull, 2003; Brezo et al., 2008; Gutiérrez-Zotes et al., 2008; Livesley et al., 1998; Pukrop et al., 2001; Simonsen & Simonsen, 2009). Emotional Dysregulation (Anxiousness, Identity Problems, Submissiveness, Affective Instability, Social Avoidance, Cognitive Distortion, Oppositionality, and Insecure Attachment), Dissocial Behavior (Callousness, Conduct Problems, Stimulus Seeking, and Rejection), and Inhibitedness (Intimacy Problems and Restricted Expressiveness) were 510 KUSHNER ET AL. replicated at Level 4. The fourth component was defined by a high loading of the Compulsivity dimension, and split off of the Dissocial Behavior component at Level 3. Level 5. At Level 5, Emotional Dysregulation split into Emotional Dysregulation (Affective Instability, Self-harming Behavior, Identity Problems, Anxiousness, and Cognitive Distortion) and a component defined by high loadings of the Insecure Attachment, Narcissism, and Submissiveness dimensions, resembling Clark and colleagues’ (1996) ‘Need for Approval’ factor, and labeled accordingly. Inhibitedness (Restricted Expressiveness and Intimacy Problems), Dissocial Behavior (Callousness, Conduct Problems, Stimulus Seeking, and Rejection), and Compulsivity (Compulsivity) were replicated at Level 5. Level 6. Emotional Dysregulation (Affective Instability, Anxiousness, Identity Problems, Cognitive Distortion, Self-harming Behavior, and Oppositionality), Inhibitedness (Restricted Expressiveness and Intimacy Problems), Need for Approval (Insecure Attachment, Submissiveness, and Narcissism), and Compulsivity (Compulsivity) were replicated at Level 6. Dissocial Behavior and Compulsivity both split to contribute to the sixth component, defined primarily by high loadings of the Rejection and Callousness dimensions. This new component was labeled Dissocial Behavior/Disagreeable; the previous Dissocial component, now defined by Conduct Problems and Stimulus Seeking dimensions, was renamed Dissocial/ Externalizing Behavior. Multiple Regression Analyses of DIPD-IV PD Symptoms Multiple regression analyses were conducted for each level of the personality hierarchy to assess the extent to which components of the DAPP-BQ hierarchy differentially predict DSM-IV PD symptom counts, using DIPDIV data from the clinical sample. Table 1 displays the variance in personality pathology for each DSM-IV-TR PD that was accounted for by components at each level of the hierarchy.2 The components of the DAPP-BQ hierarchy accounted for considerable variance in PD clusters, ranging from 32% to 39% across levels. Variance for specific PDs predicted by the hierarchy components ranged from 9% to 39% across levels. Emotional Dysregulation significantly predicted most, but not all of the PDs. Dissocial Behavior significantly predicted all cluster B PDs, and intermittently paranoid, schizotypal, and obsessive-compulsive PDs. Dissocial Behavior/Externalizing significantly predicted several cluster B PDs, whereas Dissocial Behavior/Disagreeableness significantly predicted PDs across all clusters. Inhibitedness significantly predicted all cluster A PDs, and 2. Given the significant differences in age and sex observed between the clinical and nonclinical samples, hierarchical regression analyses controlling for age and sex were also conducted for each level of the personality hierarchy. These analyses revealed the same pattern of results and were therefore omitted from the manuscript for clarity. Results are available upon request. 511 Note: ED = Emotional Dysfunction; DB = Dissocial Behavior; IN = Inhibitedness; CO = Compulsivity; NA = Need for Approval; DB/E = Dissocial Behavior/Externalizing; DB/D = Dissocial Behavior/Disagreeableness; PAR = Paranoid; SZD = Schizoid; SZT = Schizotypal; HIS = Histrionic; NAR = Narcissistic; BDL = Borderline; ASL = Antisocial; DPN = Dependent; OC = Obsessive-Compulsive. * p < .005; ** p < .001. TABLE 1. Results from Multiple Regression Examining the Ability of the Components of the DAPP-BQ Hierarchy in Predicting DIPD-IV Symptom Counts for DSM-IV Axis II Disorders. Cluster ACluster BCluster C PAR SZD SZT TotalHISNAR BDLASL TotalAVD DPNOC Total Level 1 Personality .47** .44** .46** .57** .42** .33** .56** .25** .56** .51** .41** .33** .54** R2 .22 .19 .21 .32 .18 .11 .31 .06 .31 .26 .17 .11 .30 Level 2 ED .38** .47** .43** .53** .24** .12 .43** .12 .35** .60** .42** .24** .55** DB .27** .07 .17* .22** .42** .44** .36** .28** .51** –.01 .11 .24** .13 2 R .22 .22 .22 .33 .24 .20 .32 .09 .38 .36 .18 .12 .32 Level 3 ED .31** .30** .38** .40** .30** .18* .46** .15 .40** .51** .50** .21** .53** DB .25** .09 .11 .19** .36** .41** .26** .26** .43** –.11 –.06 .23** .01 IN .29** .41** .25** .39** .08 .05 .17* .06 .13** .30** .01 .18* .23** R2 .24 .26 .22 .35 .24 .21 .32 .10 .38 .36 .25 .13 .33 Level 4 ED .32** .31** .38** .42** .29** .18* .45** .14 .40** .52** .50** .22** .53** DB .23** .10 .10 .18** .35** .32** .31** .28** .43** –.08 –.03 .16* .01 IN .27** .41** .25** .39** .04 .03 .12 .02 .08 .31** .01 .18* .24** CO .15* .08 .11 .15** .09 .27** –.05 –.03 .08 .01 –.08 .23** .07 R2 .25 .27 .23 .37 .24 .24 .33 .11 .38 .37 .25 .17 .34 Level 5 ED .32** .34** .40** .43** .21** .09 .53** .13 .38** .35** .31** .20** .37** IN .27** .40** .24** .38** .08 .07 .08 .02 .09 .40** .09 .19* .32** DB .21** .08 .06 .15* .33** .32** .24** .27** .39** –.09 –.06 .15 –.01 NA .12 .05 .13 .12 .24** .21** .14* .09 .22** .30** .37** .12 .33** CO .15 .08 .11 .15* .06 .24** –.04 –.04 .07 –.02 –.11 .22** .04 .26 .28 .25 .39 .24 .24 .39 .11 .39 .37 .26 .17 .34 R2 Level 6 ED .34** .35** .42** .46** .21** .14 .50** .12 .38** .42** .37** .26** .45** IN .25** .38** .23** .36** .10 .06 .09 .04 .10 .37** .07 .14 .27** DB/E .13 .08 .08 .12 .26** .11 .33** .24** .33** –.06 –.01 –.02 –.05 NA .05 –.02 .06 .04 .21** .15 .09 .08 .17* .22** .30** .03 .23** DB/D .21** .06 .06 .15* .24** .41** .06 .14 .27** –.07 –.06 .30** .07 CO .10 .08 .12 .12 .03 .12 .00 –.05 .03 –.02 –.13 .10 –.02 R2 .26 .28 .25 .39 .24 .25 .39 .11 .39 .37 .26 .19 .35 512 KUSHNER ET AL. intermittently borderline, avoidant and obsessive-compulsive PDs. Compulsivity variably predicted paranoid, narcissistic, and obsessive-compulsive PDs. Need for Approval intermittently predicted histrionic, narcissistic, borderline, avoidant and dependent PDs. Discussion The current analyses provide support for the validity of components of the DAPP-BQ hierarchy. Specifically, variance in symptom counts for all PDs was significantly predicted by components at each level of the hierarchy. As hypothesized, the components at the fourth level of the hierarchy were similar to those recovered in previous factor analytic investigations of the DAPP-BQ components, with Emotional Dysregulation, Dissocial Behavior, Inhibitedness, and Compulsivity emerging as robust domains across most levels of the hierarchy. At Level 5, a component representing Need for Approval separated from Emotional Dysregulation and appeared similar in content to that reported previously by Clark et al. (1996). The five extracted components were associated with a six percent increase in the prediction of borderline PD symptoms, suggesting an improvement in the predictive capacity of Level 5 components beyond those of Level 4. Interestingly, Emotional Dysregulation actually became more predictive at Level 5 when differentiated from Need for Approval, also emerging as a significant predictor. Furthermore, the differentiation of Emotional Dysregulation and Need for Approval held important information for other Cluster B disorders as well. Emotional Dysregulation and Dissocial Behavior became slightly less predictive of Histrionic Disorder with Need for Approval predicting additional unique variance. Emotional Dysregulation further moved from a significant predictor of Narcissistic PD at Level 4 to not significant at all at Level 5, with Need for Approval taking over that predictive power. This shift in the personality pathology profile for Narcissistic PD is perhaps better aligned with theoretical conceptualizations of the disorder with Need for Approval, rather than Emotional Dysregulation, reflecting a core aspect of the ­pathology. Although overall explained variance did not substantially improve between Levels 4 and 5 for Cluster C disorders, similar evidence for the potential importance of Need for Approval emerged. Specifically, predictive power of Emotional Dysregulation decreased for Cluster C PDs when Need for Approval was differentiated. Importantly, both of the factors continued to offer unique prediction of Avoidant and Dependent PD, suggesting that they capture distinct but relevant information. Taken together, prediction of both Cluster B and Cluster C disorders demonstrated a potentially important role for Need for Approval and supported distinguishing between Need for Approval and a more salient Emotional Dysregulation component. Despite overlap, it is likely that these components have distinct correlates and consequences relating to impairment and interpersonal prob- HIERARCHICAL STRUCTURE 513 lems; as such, these features warrant careful assessment and consideration in clinical practice (e.g., Miller & Pilkonis, 2006). At Level 6, the Dissocial Behavior component decomposed into externalizing (i.e., Conduct Problems, Stimulus Seeking) and disagreeable (i.e., Rejection, Callousness) components, also reported previously (Goldner et al., 1999; Jang et al., 1999; Larstone et al., 2002; Wang et al., 2004). No specific improvements in the prediction of variance across PDs were observed, with negligible increases in R2 for narcissistic PD (1%) and obsessive-compulsive PD (2%) likely resulting from the addition of predictors to the regression model. Moreover, Compulsivity at Level 6 did not significantly explain the symptom counts for individual PDs or for overall clusters. The current results suggest that the addition of Need for Approval at Level 5 of the DAPP-BQ hierarchy provides additional information of PD symptoms beyond components at Level 4, while the division of Dissocial Behavior at Level 6 provides no considerable improvements in symptom prediction. Based on these results, we think that Level 5 represents a crucial level of analysis for PD symptoms. These results are largely in line with those reported by Markon et al. (2005) and Tackett, Quilty, et al. (2008), which highlighted the importance of the five broad personality domains for psychopathology research, although those components were extracted from the FFM. The fifth level in these previous studies, however, is somewhat different from that in the current version. In particular, the DAPP-BQ does not have a clear analog to the typical fifth factor in personality studies, Openness to Experience (Tackett, Silberschmidt, et al., 2008). Furthermore, the differentiation between types of Emotional Dysregulation may be apparent only with a wider breadth of maladaptive items tapping into this domain, such as those found in the DAPP-BQ. Other similarities with previous hierarchies are also seen in these findings. Level 3 of these analyses roughly maps onto a Neuroticism/Negative Affectivity component (Emotional Dysregulation), an Extraversion/Positive Affectivity component (Inhibitedness), and a Disinhibition component (Dissocial Behavior; Clark, 2005). At Level 4, the structure resembles maladaptive variants of Neuroticism, Extraversion, Agreeableness, and Conscientiousness (Markon et al., 2005; Tackett, Quilty, et al., 2008; Widiger & Simonsen, 2005). A more representative sample of items tapping into approach-motivated characteristics, such as those reflected in positive emotionality and Openness to Experience, or unusual sensory and perceptual experiences may be needed to provide full replication of other hierarchies (Tackett, Silberschmidt, Krueger, & Sponheim, 2008). Limitations and Future Directions Although the present results provide support for the validity of the DAPPBQ hierarchy, a number of limitations of the study must be addressed as well. First, the current investigation included patients and students who responded to solicitations for research participants. Given the suggestion 514 KUSHNER ET AL. that individuals who volunteer for research studies may exhibit differing personality characteristics compared to those who do not (Kushner, Quilty, McBride, & Bagby, 2009), we recommend replication using other types of clinical and community samples. Second, the clinical sample consisted of low base-rates for certain PDs. Future research should replicate these results in samples with higher base rates of PDs. A compelling outcome of the current analyses concerns the organization of DAPP-BQ dimensions into hierarchy components. The loadings obtained for Level 4 in the current analyses are generally consistent with those outlined in the technical manual for the DAPP-BQ (Livesley & Jackson, 2009) and replicated in multiple studies (Bagge & Trull, 2003; Brezo et al., 2008; Gutiérrez-Zotes et al., 2008; Livesley et al., 1998; Pukrop et al., 2001; Simonsen & Simonsen, 2009). It is important to note that the resulting components are conceptually counter-intuitive, suggesting outcomes that might be empirically spurious. For example, the interpersonal dimensions of social avoidance and submissiveness fell under the Emotional Dysregulation component rather than the Inhibitedness com­ponent. Oppositionality, which would seem to represent a dimension of Dissocial Behavior, also loaded onto Emotional Dysregulation. This inconsistency poses a challenge for the conceptual validity of empirically derived DAPPBQ dimensions. It is possible that the factors are simply labeled suboptimally, and that the associations between DAPP-BQ dimensions might be better represented by some other label. That is, a more appropriate label for this factor would acknowledge the correlation between emotionally dysregulated and interpersonal dimensions, such as ‘Emotional/Interpersonal Dysregulation.’ Conclusions The current investigation extracted components at six levels of the DAPPBQ hierarchy and investigated the capacity of these components in predicting DSM-IV-TR PD symptoms. Based on these findings, we conclude that Level 5 represents an important level of analysis for predicting personality pathology, with Need for Approval adding important information about symptoms of histrionic, narcissistic, borderline, avoidant, and dependent PD. The results from the current study may contribute to the refinement of the psychiatric nosology and assessment of personality pathology (see Clark, 2005), by identifying common and specific components of PDs. References Bagge, C. L., & Trull, T. J. (2003). DAPP-BQ: Factor structure and relations to personality disorder symptoms in a nonclinical sample. Journal of Personality Disorders, 17, 19–32. Brezo, J., Paris, J., Tremblay, R., Vitaro, F., & Turecki, G. (2008). DAPP-BQ: Factor structure in French Canadians. Journal of Personality Disorders, 22, 538–545. HIERARCHICAL STRUCTURE Clark, L. A. (2005). Temperament as a unifying basis for personality and psychopathology. Journal of Abnormal Psychology, 114, 505–521. Clark, L. A., Livesley, W. J., Schroeder, M. L., & Irish, S. L. (1996). Convergence of two systems for assessing specific traits of personality disorder. Psychological Assessment, 8, 294–303. First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J.B.W. (1995). Structured clinical interview for Axis I DSM-IV disorders–patient version (SCID-I/P version 2.0). New York (NY): New York State Psychiatric Institute Biometric Research Department. Goldberg, L. R. (2006). Doing it all BassAckwards: The development of hierarchical factor structures from the top down. Journal of Research in Personality, 40, 347–358. Goldner, E. M., Srikameswaran, S., Schroeder, M. L., Livesley, W. J., & Birmingham, C. L. (1999). Dimensional assessment of personality pathology in patients with eating disorders. Psychiatry Research, 85, 151–159. Gutiérrez-Zotes, J. A., Gutiérrez, F., Valero, J., Gallego, E., Baillés, E., Torres, X., et al. (2008). Structure of personality pathology in normal and clinical samples: Spanish validation of the DAPPBQ. Journal of Personality Disorders, 22, 389–404. Jang, K. L., Livesley, W. J., & Vernon, P. A. (1999). The relationship between Eysenck’s P-E-N model of personality and traits delineating personality disorder. Personality and Individual Differences, 26, 121–128. Kushner, S. C., Quilty, L. C., McBride, C., & Bagby, R. M. (2009). A comparison of depressed patients in randomized ­versus nonrandomized trials of antidepressant medication and psychotherapy. Depression and Anxiety, 26, 666– 673. Larstone, R. M., Jang, K. L., Livesley, W. J., Vernon, P. A., & Wolfe, H. (2002). The relationship between Eysenck’s P-E-N model of personality, the five-factor model of personality, and traits delineating personality dysfunction. Personality and Individual Differences, 33, 25–37. Livesley, W. J. (2005). Behavioral and molecular genetic contributions to a dimensional classification of personality 515 disorders. Journal of Personality Disorders, 19, 131–155. Livesley, W. J., & Jackson, D. N. (2009). Manual for the Dimensional Assessment of Personality Pathology—Basic Questionnaire. Port Huron, MI: Sigma Press. Livesley, W. J., Jackson, D. N., & Schroeder, M. L. (1989). A study of the factorial structure of personality pathology. Journal of Personality Disorders, 3, 292–306. Livesley, W. J., Jang, K. L., & Vernon, P. A. (1998). Phenotypic and genetic structure of traits delineating personality disorder. Archives of General Psychiatry, 55, 941–948. Markon, K. E., Krueger, R. F., & Watson, D. (2005). Delineating the structure of normal and abnormal personality: An integrative hierarchical approach. Journal of Personality and Social Psychology, 88, 139–157. Miller, J. D., & Pilkonis, P. A. (2006). Neuroticism and affective instability: The same or different? American Journal of Psychiatry, 163, 839–845. Pukrop, R., Gentil, I., Steinbring, I., & Steinmeyer, E. (2001). Factorial structure of the German version of the Dimensional Assessment of Personality Pathology—Basic Questionnaire in clinical and nonclinical samples. Journal of Personality Disorders, 15, 450–456. Schroeder, M. L., Wormworth, J. A., & Livesley, W. J. (1992). Dimensions of personality disorder and their relationships to the Big Five dimensions of personality. Personality Assessment, 4, 47–53. Simonsen, S., & Simonsen, E. (2009). The Danish DAPP-BQ: Reliability, factor structure, and convergence with SCIDII and IIP-C. Journal of Personality Disorders, 23, 629–646. Tackett, J. L., Quilty, L. C., Sellbom, M., Rector, N. A., & Bagby, R. M. (2008). Additional evidence for a quantitative hierarchical model of mood and anxiety disorders for DSM-V: The context of personality structure. Journal of Abnormal Psychology, 117, 812–825. Tackett, J. L., Silberschmidt, A. L., Krueger, R. F., & Sponheim, S. R. (2008). A dimensional model of personality disorder: Incorporating DSM Cluster A characteristics. Journal of Abnormal Psychology, 117, 454–459. 516 Trull, T. J., & Durrett, C. A. (2005). Categorial and dimensional models of personality disorder. Annual Review of Clinical Psychology, 1, 355–380. Wang, W., Du, W., Wang, Y., Livesley, W. J., & Jang, K. L. (2004). The relationship between the Zuckerman-Kuhlman Personality Questionnaire and traits delineating personality pathology. Personality and Individual Differences, 36, 155–162. Widiger, T. A., & Simonsen, E. (2005). Al­ ternative dimensional models of per­ sonality disorder: Finding a common ground. Journal of Personality Disorders, 19, 110–130. KUSHNER ET AL. Widiger, T. A., Simonsen, E., Krueger, R. F., Livesley, W. J., & Verheul, R. (2005). Personality disorder research agenda for DSM-V. Journal of Personality Disorders, 19, 315–338. Widiger, T. A., & Trull, T. J. (2007). Plate tectonics in the classification of personality disorder: Shifting to a dimensional model. American Psychologist, 62, 71– 83. Zanarini, M. C., Frankenburg, F. R., Sickel, A. E., & Yong, L. (1996). The Diagnostic Interview for DSM-IV Personality Disorders (DIPD-IV). Belmont, MA: McLean Hospital.