Effects of bradykinin on the fetal cirmlation
advertisement

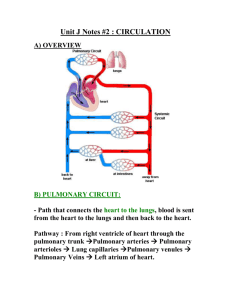
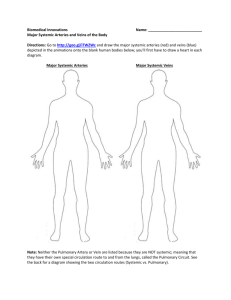
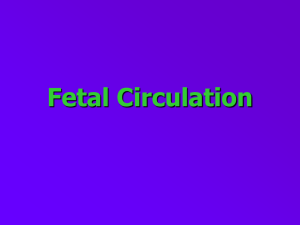
AMERICAN JOURNAL OF PHYSIOLOGY 1971. Printed Vol. 221, No. 5, November in U.S.A. Effects of bradykinin on the fetal cirmlation N. S. ASSALI, G. H. JOHNSON, C. R. BRINKMAN Department of Obstetrics and Gynecology and Physiology, UCLA Los Angeles, California 90024 ASSALI, N. S., G. H. JOHNSON, C. R. BRINKMAN III, AND D. J. HUNTSMAN. Effects of bradykinin on the fetal circulation. Am. J. Physiol. in the adult animal (8, 16, 29), prompted us to investigate its action on the fetal pulmonary, systemic, and umbilical circulation. The intent was to find out if any similarity exists between the hemodynamic action of exogenously administered bradykinin and the circulatory changes that occur at birth. 197 1 .-Effects of bradykinin on pulmonary, 221(5): 1375-1382. systemic, and umbilical hemodynamics were studied in near-term fetal lambs. Bradykinin produced profound pulmonary and sys- temic vasodilatations; it increased pulmonary blood flow by diverting most of the right ventricular output toward the lung. Left ventricular aortic output increased, but effective cardiac output (ascending + ductus flows) decreased slightly. The systemic vasodilatadid not involve the umbilicoplacental circulation whose blood tion flow decreased; a redistribution of resistances and flows occurred with more blood shifted toward the fetal visceral Venous return to the right heart and right ventricular mained unimpaired despite the decrease in umbilical of these circulatory alterations resemble those occurring flows; resistances; pressure; pulmonary; arteriosus; cardiac output circulation. filling reflow. Some at birth. systemic; umbilical; ductus THE MAJOR CIRCULATORY CHANGES that occur at birth are: a) a fall in pulmonary vascular resistance and pressure and a marked increase in pulmonary blood flow; b) a transient fall in the systemic arterial pressure followed by a progressive rise along with a decrease in the effective cardiac output and an increase in the systemic vascular resistance; the systemic changes become more evident after umbilical cord clamping; c) a rise in both atria1 pressure with a greater increment in the left than in the right atrium; d> a constriction and eventual closure of the ductus arteriosus; and, e) if the umbilical cord is not clamped, a diminution and eventual cessation of umbilical blood flow (1, 3, 12). The ductus closure and the pulmonary vasodilatation have been attributed partly to the rise in blood PO:! that follows the onset of breathing (1, 2, 4, 7) ; but the mechanisms by which oxygen produces these effects are not known. The transient fall in the systemic arterial pressure has been related to the changes in the ductus flow direction which becomes left to right (3). The subsequent increase in systemic pressure and resistance and the decrease in the effective cardiac output have been attributed largely to ductus closure and to elimination of the low-resistance system of the umbilicoplacental circulation (1, 3). Recent reports have suggested that bradykinin may play an important role in the transitional circulatory changes that occur at birth (10, 17, 26, 28). It has been further postulated that the oxygen action on the ductus arteriosus and on the pulmonary vessels might be mediated through bradykinin release (17). These hypotheses, together with the interesting hemodynamic properties of bradykinin reported III, AND D. J. HUNTSMAN School of Medicine, Center for Health Sciences, MATERIAL AND METHODS A total of 26 near-term pregnant ewes of mixed breed and their 29 fetal lambs were used in these studies. Each ewe was fasted for 18-24 hr prior to the experiment. The ewe was placed on her left side on the operating table and, under local anesthesia, the right carotid artery and jugular vein were cannulated. The carotid artery catheter served for recording maternal arterial pressure and for collecting arterial blood samples anaerobically. Anesthesia was induced with an initial dose of 6-10 mg/kg of pentobarbital administered through the jugular vein catheter; additional doses were given as needed to maintain an adequate anesthesia. An endotracheal tube was inserted through a tracheostomy and the maternal respiration was supported with compressed air using a positive-negative pressure Bird respirator. The pregnant uterine horn was partially exteriorized by laparotomy and was marsupialized to the abdominal walls to prevent evisceration. The fetus was then delivered by hysterotomy and was marsupialized to the edges of the uterine incision to protect the umbilical circulation. The fetal head was covered with a saline-filled glove to prevent breathing. A polyethylene catheter was inserted into the fetal femoral artery and was advanced into the descending aorta; it served for arterial pressure recording and for anaerobic collections of blood samples. Another catheter was inserted into the femoral vein and served for bradykinin injections. The fetal chest was entered through the fourth leftintercostal space and the main pulmonary artery, the ascending aorta, and the ductus arteriosus *were exposed. The left phrenic and vagus nerves were kept intact in the majority of the animals. The technical steps described above were performed on all animals. Additional surgical procedures were carried out according to the experimental protocol as follows: A) Five fetal lambs served for the study of the effects of bradykinin on the pulmonary circulation only. In these animals, the main pulmonary artery and the ductus arteriosus were fitted with electromagnetic flow transducers and their blood flows were recorded simultaneously; net pul1375 1376 monary blood flo*w was estimated from the difference between these two flows (1). Pulmonary artery pressure was recorded through a Rochester-type catheter inserted into the pulmonary artery and secured in situ with a pursestring suture. A similar catheter was inserted into the left atrium and served for atria1 pressure measurement. Right atria1 pressure was monitored through a catheter placed in the right atrium through a jugular vein. B) Five fetuses served for studying the effects of bradykinin on the fetal effective cardiac output only. In these, the ascending aorta and the ductus arteriosus were fitted with flow transducers and their blood flows were measured simultaneously. Fetal effective cardiac output was estimated from the algebraic sum of these two flows (1). C) Six other fetuses served for studying the effects of bradykinin on both pulmonary and systemic circulations concommitantly. In each of these animals, the three great vessels namely, the main pulmonary artery, the ascending aorta, and the ductus arteriosus were fitted with flow transducers and their blood flows -were monitored simultaneously. This procedure allowed estimation of net pulmonary flow, effective cardiac output, and foramen ovale flow in the same animal (1, 3). Pulmonary artery and atria1 pressures were recorded as in the series described under A. D) In seven additional animals, the effects of bradykinin on the umbilica 1 circu la tion and the umbilical fraction of the cardiac output were invest] .gated. In each animal, intraperitoneal segment of the main umbilical vein was exposed prior to its entrance into the liver and was fitted with a flow transducer to measure total umbilical blood flow. Flow transducers were also placed around the ascending aorta and ductus arteriosus to measure simultaneously the effective cardiac output. A catheter was inserted into a cotyledonary branch of the umbilical vein and was advanced into one of the two main umbilical veins where it served to monitor umbilical vein pressure. Systemic pressure was measured through a catheter in the umbilical artery or aorta. In three of the seven animals, the inferior vena cava pressure was measured through a catheter introduced through a femoral vein and placed in the vena cava past the liver as previously described (9). The location of the catheter was checked at the end of the experiment. E) To test whether the changes in ductus blood flow elicited by bradykinin were due to a direct action of this substance on the ductus itself or were secondary to changes in the pulmonary vascular bed (see RESULTS), the following two series of experiments were performed: in three fetuses after exposing the great vessels, the circulation to the lungs was bypassed by introducing a shunt with a polyethylene tube between the left branch of the main pulmonary artery and the left fetal jugular vein. The right branch of the pulmonary artery was ligated. Blood flows in the main pulmonary artery, ductus arteriosus, and ascending aorta, as well as systemic and pulmonary artery pressures, were monitored continuously. This preparation eliminated the variables connected with the pulmonary vascular bed. In another three lambs, the ductus arteriosus was ligated. Main pulmonary a rtery a.nd ascending aortic flows as well vascular pressures were monias svstemic and pulmonary tored. These last experimen ts allowed testing of bradykinin ASSALI, JOHNSON, BRINKMAN, AND HUNTSMAN action on the pulmonary circulation in the absence of the ductus arteriosus. All blood flows were measured using cuff-type, balancedfield electromagnetic flow transducers and amplifiers previously described (3 1). Each transducer was selected to fit each vessel snugly but without undue constriction. The transducers were calibrated in vitro, and a calibration factor obtained for each as described in detail elsewhere (5). Blood flow rate in each vessel was calculated from the product of the calibration factor of that particular transducer and the integrated flow deflection (electronic integrator) elicited on the Dynograph. The error in this method for any given flow in the great fetal vessels is no more than zt 5%. Vascular pressures were measured with matched Statham DB-23 strain gauges calibrated to a common zero base line. Phasic and integrated pressure and flow signals were recorded on an Offner Dynograph and on an Ampex magnetic tape. Net pulmonary blood flo’~, effective cardiac output, and pulmonary, systemic, and umbilical vascular resistances were computed by formula previously described (1, 3). Heart rate was obtained from the phasic pressure or flow records. Maternal and fetal blood pH, POT and Pcoz were analyzed using the Radiometer acid-base analyzer with a microblood-gas (type PHM7 1), in conjunction apparatus. Technical details of the surgical procedures as well as those of measuring flows, pressures, and blood gases have appeared in several publications (2, 3, 4, 9, 19). The experimental protocol comprised the following : A control period of 30 min was observed during which flows and pressures were allowed to stabil .ize and were recorded continuously; blood gases were analyzed at IO-min intervals. A drug-testing period then followed during which bradykinin was administered intravenously in single-bolus injections in progressively increasing amounts. At the conclusion of each experiment, the fetal weight was obtained and the amounts of the drug used were converted on the basis of body weight; a dosage range of Z-700 rig/kg of fetal body wt was obtained. Each dose was tested at least 12 times and the effects of each injection on flows and pressures were monitored continuously. Adequate time was allowed between subsequent injections for the pressures and flows to return to control values. Blood respiratory gases and pH were analyzed every 5 min during this period. In addition to single intravenous doses, the effects of continuous infusion of bradykinin were tested. In these cases, the drug was administered via the femoral vein at rates of 5-10 rig/kg per min for 3-5 min. Flows and pressures were monitored continuously before, during, and after interruption of the infusion. In a few lambs, the effects of small doses of bradykinin injected into the main pulmonary artery were tested. RESULTS Control data. Average values for blood flows, vascular pressures, and blood respiratory gases and pH recorded after completion of surgery and prior to bradykinin administration are listed in Table 1. These figures are within the range of values obtained by us in previously published experiments (1, 2, 3, 19). BRADYKININ AND FETAL 1377 CIRCULATION TABLE 1. Values for fetal blood jaws, vascular pressures, and blood respiratory gases and PH recorded in control period after completion of surgery and prior to bradykinin injection 65 70 111 96 142 46 181 22 43 7.28 Systemic arterial pressure, mm Hg Pulmonary artery pressure, mm Hg Ascending aorta flow, ml/kg per min Ductus arteriosus flow, ml/kg per min Main pulmonary artery flow, ml/kg per min Net pulmonary flow, ml/kg per min Effective cardiac output, ml/kg per min Aortic blood Paz, mm Hg Aortic blood Pco~, mm Hg Aortic blood pH Values are means parentheses. & 1 Number SD. zt rt zt zt =t= zt rfr zt =t: =t of measurements 4 (70) 6 (35) 16 (35) 22 (56) 18 (35) 22 (35) 24 (35) 6 (70) 8 (70) .08 (70) is given in +60 Pulmonary Arterlul tory changes produced by injection of bradykinin into the main pulmonary artery were not significantly different from those observed after administration by the femoral vein. Ductus arteriosus blood flow decreased invariably following the in.jections of bradykinin (Figs. 2 and 3). The response of this vessel -was also progressive up to 20-30 rig/kg; thereafter increasing the dose produced no further decrease in ductus blood flow (Fig. 7). In order to assess the maximum response of the pulmonary circulation including the ductus arteriosus to bradykinin, the changes in all animals included in series A and C (see MATERIALS AND METHODS) observed after doses of 40-700 rig/kg (the flat portion of the dose-response curve) were pooled together and were plotted as percent of control values (Fig. 4). Maximum decrease in pulmonary artery pressure averaged 40 % while the maximum increase in main pulmonary artery flow averaged about 80%. Mean ROW Exp No. 9 Aug. 19, 1970 Fetus 5.1 kg km 7 /- ---,_ ‘. 504 .---I AORTIC PRESSURE mm Hq -- 4m -.-. 1, .. -- - \ ^ -- ----- O- 20”, ,, 40, 60, 80, 100” , ,, Dose (Nanogram , , , , , 200 300 400 500 600 , 700 1 kg) 100 PULMONARY ARTERY PRESSURE mm Hg 7 5oj . DUCTUS ;;iV;RIOSUS ml / min -30 -4ol- 1. Dose-response pressure and flow. FIG. tery PULMONARY ARTERY FLOW ml / min - P ulmonory relationship Ar fer-ii/ Pressure of bradykinin 4 nangr in pulmonary ar E$ects on pulmonary and ductus arteriosus circulation. The response of the pulmonary vascular bed to progressively increasing doses of bradykinin is illustrated in Fig. 1. The data in this figure ‘were those collected from the experiments listed under A and C (see MATERIALS AND METHODS). Each datum represents the mean I-+ 1 SE of all the tests made for each dose. The response of a given circulatory parameter to each dose was taken as the maximum change observed after the injection. This value ‘was then plotted as percent of the average of several control readings taken prior to the injection. Figure 2 illustrates a typical example of phasic and integrated responses in the systemic and pulmonary artery pressure and in the ductus and main pulmonary artery flows to different doses of bradykinin. Figure 3 illustrates an example in which pulmonary artery, ductus, and ascending aortic flows were recorded simultaneously with the atria1 and vascular pressures. Intravenous administration of single doses of bradykinin consistently produced a prompt and equal fall in systemic and pulmonary artery pressures. Pulmonary artery blood flow increased simultaneously with the fall in pressure #(Figs. l-3). The dose-response relationship of the pulmonary Ocirculation was nearly linear between 2 and cit. 20 rig/kg. Within this dose range, the increase in pulmonary blood flow was greater than the decrease in pulmonary artery pressure (Fig. 1). Dosages from 20 to 700 rig/kg produced no greater response than that of 20 rig/kg (Fig. 1). The circula- chart speed mm /set / kg 8 nangr /kg 16 nangr /kg 40 nangr / kg 5 FIG. 2. Segments of a record depicting effects of various intravenous tdoses of bradykinin on pulmonary artery and aortic pressures and on 1 pulmonary artery and ductus arteriosus flow. PdJd_-rME;~ARY PRESSURE m m Hg AORTIC PRESSURE m m Hg RIGHT ATRIAL PRESSURE m m Hg LEFT ATRIAL PRESSURE m m Hg f”Lff;NARY FLOW ml / min DUCTUS ;FM&RIOSUS ml / min ASCENDING t%iA ml / min ? t 92 nangr / kg chart speed: mm /set I 369 nangr / kg 5 FIG. 3. Segments of a record showing effects of 2 different doses of bradykinin on pulmonary and systemic circulations including left and right atrial pressures. Note reciprocal changes in pulmonary and ductus flows. Note also greater rise in left than right atria1 pressure, 1378 ASSALI, Pulm. t- Pulm. Art. Flow Net Pulm. -120 L. Atrial /SE I -100 I -80 I -60 1 -40 -I Ductus Flow Pulm. Vast. Flow R. Atrial I--- Press. 1-b 4-1 I Art. Press. - Press. --- Res. I I I -20 0 I +20 I +40 I +60 +80 l//l +lOO +200 I +300 I +400 % CHANGES FIG. 4. Maximum changes in pulmonary hemodynamics and atria1 pressures in response to 40-700 r&kg of bradykinin. Note marked increase in net pulmonary blood flow and decrease in pulmonary vascular resistance. Note also difference between left and right atria1 pressure increments. TABLE 2. Changes in pulmonary and systemic circulations response to 15-20 rig/kg of bradykinin when ductus was occluded or when pulmonary vascular bed was bypassed JOHNSON, BRINKMAN, AND HUNTSMAN the dose-response relationship of the systemic circulation including the response of the ductus arteriosus. The systemic arterial pressure responded in a manner similar to that of the pulmonary artery pressure. A progressive decrease occurred between doses of 2-20 rig/kg. Thereafter, increasing the dose produced no further systemic arterial pressure decrement (Fig. 7). Ascending aortic flow increased progressively up to 20 rig/kg; but thereafter the dose-response curve became flat (Fig. 7). For any given dose, the increment in ascending aortic flow was significantly less than that of the pulmonary flow (Figs. 1 and 7). Ductus arteriosus blood flow decreased in a manner similar to that observed in the series of pulmonary studies (Fig 7). Figure 8 presents the maximum systemic hemodynamic changes produced by doses of 40 rig/kg and above in all animals in which ascending aortic and ductus blood flows in Bradykinin Systemic Pressure mmHg Arterial I.V. & 6o 0.3 pg Fetal weight 4.1 kg Experiment 1A LUNGS BYPASSiD 0 Ductus Occluded Systemic arterial pressure Pulmonary artery pressure Main pulmonary artery flow Ascending aorta flow Ductus arteriosus flow Heart rate -25 -30 +27 +18 =f= It rt rt 2 2 8 6 (18) (15) (15) (15) Lungs Bypassed -28 -26 3-18 +16 +20 0 (1% Values are net percent changes from Number of tests is given in parentheses. control values =f= 3 (15) =t 5 (12) zt: 9 (12) =t 8 (12) xt 10 (12) 0 =t 1 Pulmonary Pressure mmHg Arterial 60 0 SE. decrease in ductus blood flow also was about 80 %. Net pulmonary blood flow (main pulmonary artery-ductus flow) rose, and pulmonary vascular resistance decreased strikingly (Fig. 4). Both right and left atria1 pressures increased, but the increment was greater in the left than in the right atrium (Figs. 3 and 4). In view of the fact that the decrease in ductus flow was of the same magnitude as the increase found in the pulmonary blood flow, we designed the experimental protocol described under E (see MATERIALS AND METHODS) to investigate whether the ductus changes produced by bradykinin were primary or secondary to the blood shift caused by the pulmonary vasodilatation. When the pulmonary vascular bed was bypassed, bradykinin produced the usual equivalent fall in systemic and pulmonary artery pressures (Table 2 and Fig. 5). Ductus blood flow, however, instead of decreasing as previously described, increased consistently; the increment was of the same magnitude as that of the main pulmonary artery blood flow (Table 2 and Fig. 5). It is of interest that, in the absence of the pulmonary circulation, the action of bradykinin lasted longer (Fig. 5). In the experiments in which the ductus arteriosus was occluded, bradykinin produced the typical decrease in systemic and pulmonary pressures and the increase in main pulmonary artery and ascending aortic blood flow as observed in the other animals (Table 2 and Fig. 6). Effects on systemic circulation. Figure 7 presents the data on 820 Main Pulmonary Arterial Flow mlimin 410 p 0 : FIG. 5. A representative example of effects of bradykinin in a fetus with lung vasculature bypassed. Note that ductus arteriosus flow increased instead of decreasing. Increase was largely in diastolic flow. Note also more prolonged action of bradykinin (see text). 120 Bradykinin r Pulmonary Arterial Pressure mmHg I.V. 0.5 ug G Fetal weight 4. 7 kg Experiment 4A DUCTUS OCCLUDED OL Systemic Arterial Pressure mmHg ASC. Aortic Flow mllmin. 360 0 6. A typical example of effects of bradykinin ductus arteriosus occluded. Note that pulmonary fell and main pulmonary artery flow increased despite tus circulation (see text). FIG. in a fetus with artery pressure absence of duc- BRADYKININ AND +4ok FETAL CIRCULATION 1379 Ascending ;lSE. Dose (Nanogram/kg Ductus Aorflc ) Flow FIG. 7. Dose-response relationship of bradykinin circulation including ductus arteriosus. l-1 1 -i30 -80 Flow in fetal systemic monary artery flow exceeded the sum of OAA and QD. Foramen ovale flow decreased by about 50% and became negative, i.e., from left to right. Effects on umbilical circulation and on inferior vena cava pressure. Figure 9 illustrates a representative example of the effects of bradykinin on systemic arterial (equivalent to umbilical arterial) and venous pressures and on the blood flows in the umbilical vein, ascending aorta, and ductus arteriosus. Figure 10 presents the average changes in these circulatory parameters including those in the inferior cava pressure. Intravenous administration of bradykinin decreased the pressure in the umbilical artery and vein in a similar manner and by an equivalent amount (about 40 %) (Figs. 9 and 10). Total umbilical blood flow also decreased by an average of 40%, umbilical vascular resistance did not change significantly (Fig. 10). Effective cardiac output fell only slightly but the fraction of the cardiac output destined for the placenta decreased markedly (Fig. 10). Heart Rate S.E. / I -60 I -40 , -20 I 0 +20 I +40 ! +60 1 +80 I +I00 % CHANGES FIG. 8. Maximum changes in aortic pressure, ductus and aortic flows, effective cardiac output, systemic vascular resistance, and heart rate in response to doses of bradykinin, 40-700 rig/kg. Note marked decrease in systemic vascular resistance. Effective cardiac output changed very little because decrease in ductus flow was offset by increase in ascending aortic flow. were measured simultaneously (series B and C). Systemic arterial pressure decreased by an average of about 40%, and ductus flow decreased by an average of 80 %. Maximum increase in ascending aortic flow averaged about 70 % (Fig. 8). Because of the opposite changes in ductus and ascending aortic flows, the effective cardiac output of the fetus (ascending aortic + ductus flows) decreased only slightly but the changes were not significant; fetal systemic vascular resistance fell markedly (Fig. 8). Foramen ovale flow. Blood flow through the foramen ovale (OFO) was estimated in the animals included in ..series C (see MATERIALS AND METHODS) using the formula: QFO = (OAA .+ GDA) - QPA; where Q&A = ascending aortic flow, QD = ductus arteriosus flow, and QPA = main control values for this pulmonary artery flow. Average series of experiments was 5? f 15 ml/kg per min. In the control period, the sum of QAA and QD was greater than QPA, and foramen flow was from right to left. After bradykinin injections, left atria1 pressure increased much more than right atria1 pressure and the decrement in ductus flow was greater than the increment in ascending aortic flow. Consequently, in the majority of instances, the main pul- FIG. 9. Segments of a record illustrating simultaneous effects of bradykinin on systemic and umbilical circulations. Note parallel fall in systemic and umbilical vein pressures and umbilical blood flow. Inf. vena cava press. - Umb V Press i Unk b--lS.E I -80 I -60 -40 ’ Vast. Res. -217 hk~orzkz& % CHAhGES FIG. 10. Maximum changes in umbilical circulation and in umbilical fraction of cardiac output in response to bradykinin. Note unchanged umbilical vascular resistance and marked fall in umbilical fraction. Note also divergent effects on umbilical vein and inferior vena cava pressures. 1380 While bradykinin decreased umbilical vein pressure, it increased consistently the pressure in the inferior vena cava, between the ductus venosus and right atrium, by an average of over 75 % (Fig. 10). of instances, E$ects on heart rate. In the great majority intravenous administrations of single doses of bradykinin up to 700 rig/kg did not alter the heart rate appreciably. However, in occasional animals, a bradycardia occurred after large doses. Such a bradycardia was unpredictable and not reproducible. When it did occur, however, all pressures and flows in the pulmonary and systemic circulations decreased. E#ects of continuous infusion. The pattern of the circulatory changes produced by continuous intravenous infusion of bradykinin was similar to that of a single rapid injection. However, pressures and flows tended to return toward control values after 2-3 min despite continuation of the infusion. These findings are in agreement with other reports (8, 16, 29). E$ects on blood respiratory gases andpH. Neither single intravenous injections nor continuous infusion of bradykinin had any effect on fetal blood POT, Pco~, or PH. DISCUSSION The available information indicates that the circulatory effects of bradykinin vary according to: a) animal species, b) the vascular bed under observation, c) the dose, d) the interaction of bradykinin with other vasoactive substances, and e) the integrity of the autonomic nervous system (8, 16, 28, 29). Despite the variation, it is generally agreed that, in the adult animal, bradykinin produces a fall in the systemic vascular pressure and resistance and an increase in the cardiac output (8, 16, 28, 29). Bradykinin also produces coronary, cerebral, and splanchnic vasodilatation (20, 30). The action of bradykinin on the pulmonary circulation of the adult animal is somewhat more complex than that on the systemic circulation. Pulmonary vascular resistance may not change or may decrease somewhat, but pulmonary artery pressure may rise slightly depending on the animal species (8, 16, 18, 2 1). The decrease in pulmonary vascular resistance has been attributed to the increase in cardiac output and pulmonary blood volume (8, 16, 18, 2 1). The reports on the response of the venous system to bradykinin are not consistent. Some authors (6, 14, 18) have observed venous constriction following bradykinin; others believe the primary action is venous dilatation (28). In the neonatal period, endogenously generated bradykinin is believed to promote the pulmonary vasodilatation and the ductus arteriosus constriction that occur with initiation of breathing ( 10, 17, 26, 28). Blood concentrations of bradykinin have been found to be higher in the neonatal than in the fetal lamb ( 17, 26) ; higher concentrations were also observed in fetal lambs whose blood Paz was raised with hyperbaric oxygenation ( 17). Isolated observations on exogenous administration of bradykinin (4-10 ng) to fetal lambs showed a rise in pulmonary blood flow ( 10, 17). The present studies carried out on fetal lambs with intact umbilical circulation and unexpanded lung show that bradykinin action is somewhat different from that observed , in adult animals. Pulmonary circulation. Unlike in the adult animal bradv- ASSALI, JOHNSON, BRINKMAN, AND HUNTSMAN kinin in the fetus invariably produced a marked fall in pulmonary vascular pressure and resistance and a striking increase in net blood flow. This pulmonary vasodilatation occurred irrespective of the dose and site of injection. It could be argued that : I) the fall in the fetal pulmonary . artery pressure produced by bradykinin is secondary to, the systemic hypotension since the two vascular beds are connected by the ductus arteriosus; and 2) the increase in. net pulmonary blood flow is secondary to a shift of blood from the ductus arteriosus which was primarily constricted by bradykinin. Since ductus occlusion did not eliminate the pressure fall or the flow increase, it 1s obvious th .at the changes in pulmona ry hemodynamic s are caused by an, active dilatation of the pulmonary vascular bed by bradykinin. The reasons for the difference between the adult and fetal pulmonary vascular responses to bradykinin are not clear. Campbell- and his co-workers ( 10) observed a considerably smaller pulmonary response to bradykinin in 5- to 14-weekold (newborn) than in fetal lambs; the response of the neonatal lamb became greater when the lungs were collapsed and pulmonary vascular resistance increased. These authors suggested that the magnitude of changes depends a great deal on the initial status of the pulmonary vessels. Since in the neonate and in the adult animal the pulmonary vessels are already widely dilated and the pressure is low, the response to bradykinin is less. This plausible hypothesis may explain a smaller response; it may not be sufficient, however, to explain a reversal of pressure effect, namely, a rise in the pulmonary artery pressure as often observed in the adult animal as opposed to the profound pulmonary hypotension of the fetus. Ductus arteriosus circulation. Bradykinin decreased ductus blood flow consistently by an amount equivalent to the increase in the main pulmonary artery blood flow. The decrease was not related to changes in such factors as the pressure gradient across the ductus, the blood POT or the right ventricular output since the first two factors were not altered and the latter increased. The decrease in ductus flow produced by bradykinin could then be due to either an active ductus constriction or passive contraction secondary to the pulmonary vasodilatation. The data obtained from the experiments in which the pulmonary vascular bed was bypassed show a reversal of ductus response to bradykinin. In every instance, an increase instead of a decrease in ductus blood flow occurred and the increment was similar to that which occurred in the main pulmonary artery blood flow. These observations seem to indicate that the fall in ductus flow produced by bradykinin is most likely to be secondary to a shift of blood to the dilated pulmonary vessels. True, in vitro observations have shown that the ductus arteriosus contracts under the action of bradykinin (22). But similar ductus contractions have been observed in vitro in response to a variety of stimuli (23, 25). When some of these stimuli are tested in vivo, however, the hemodynamic effects on the systemic and pulmonary circulation render the ductus response so complex that it may not correspond to the simple in vitro system (4, 27). Systemic circulation. The present data show that the systemic vasodilatation produced by bradykinin in the fetus is BRADYKININ AND FETAL CIRCULATION closely similar to that observed in the adult animal (8, 16, 29). However, comparison of the effects of bradykinin on the cardiac output of the fetus and the adult animal cannot be made for reasons of anatomic and physiologic differences. In the fetus, because of the ductus arteriosus, we define effective cardiac output as the algebraic sum of ascending aortic flow (roughly left ventricular output) and ductus flow ( 1, 3). Since, in the present experiments, ductus blood flow decreased by an amount greater than the increase in ascending aortic flow, the effective cardiac output decreased slightly. The increase in left ventricular output produced by bradykinin was obviously caused by the marked increase in blood returning from the lungs to the left side of the heart. But the increment in ascending aortic flow was always less than that of the net pulmonary blood flow. The discrepancy could be due to one or a combination of the three following factors: a) Bradykinin increased fetal pulmonary blood volume through a rise in vascular compliance. b) Bradykinin dilated the fetal coronary circulation and increased the coronary fraction of the cardiac output. Such an increase would have been missed since our method of measuring left ventricular output does not include coronary flow. c) Some of the blood returning from the lungs passed through the foramen ovale to the right side of the heart. This latter possibility will be discussed further below. At any rate, as in the adult, bradykinin must have acted on the peripheral vascular resistance to produce the systemic vasodilatation seen in the fetal lamb. But the regional site of the peripheral vasodilatation is considerably more complex than that of the adult circulation. Umbilical circulation and venous return. The complexity is related to the interesting effects of bradykinin on the umbilicoplacental circulation. The equivalent fall in the arterial and umbilical vein pressures and in the total umbilical blood flow indicates an unaltered umbilical vascular resistance following bradykinin administration. This puzzling action is not in keeping with the marked fall in the total fetal systemic resistance to which the umbilicoplacental vascular bed contributes a great deal. The fall in the umbilical artery pressure reflects the overall systemic arteriolar dilatation; it is not, however, consistent with the in vitro observations which show that bradykinin constricts the human umbilical artery (11, 15). Th is d iscrepancy could be due either to the difference in sensitivity to bradykinin between the human and the sheep umbilical artery (24) or to the inherent differences in the in vivo and in vitro experimental results. The fall in the umbilical vein pressure indicates either dilatation of these vessels by bradykinin or relaxation of the ductus venosus or both. At any rate, in the presence of such a massive umbilical arterial and venous relaxation, one would expect an increase in flow. Yet, umbilical blood flow decreased instead of increasing. This decrease can be explained on the basis of either pooling of blood in the placenta, or redistribution of blood flows and resistances between the placenta and other fetal organs. In view of the marked decrease in the fraction of cardiac output destined to the placenta, we are inclined to believe that bradykinin produces a marked vasodilatation in other parts of the fetal organism (most likely the visceral circulation) ; hence, blood flow is redistributed and is shifted from the placenta toward these other dilated regions. This hypothesis receives 1381 further support from the fact that, despite the decrease in the umbilicoplacental blood flow, the inferior vena cava and the right atria1 pressures increased along with the right ventricular output. These changes indicate an unimpaired venous return to the right heart. Of course, it is possible that bradykinin, while dilating the umbilical veins, constricted the other parts of the venous system, including the vena cava, maintaining, thereby, a normal venous return. Or, that the rise in the inferior vena cava and right atria1 pressures was caused by a passage of blood from the left to the right atrium through the foramen ovale. This passage would be facilitated by the marked rise in the left atria1 pressure secondary to the increased pulmonarv blood flow. We realize that our estimates of foramen ovale flow involve a large error due to multiple flow measurements. Nevertheless, they do suggest a reversed flow, i.e., from left to right. Similar changes in left and right atria1 pressures have been observed after fetal lung expansion with air or oxygen despite a marked decrease in umbilical flow (3, 13). There is no obvious reason to believe that the foramen ovale flow would be always unidirectional, that is from right to left, and that this shunt should close promptly and totally upon raising the left atria1 pressure. The increase in right ventricular output (main pulmonary artery blood flow) observed when the lungs were bypassed seems to suggest a positive inotropic effect on the fetal heart. Such an action has been observed in the adult animal (8, 16, 29). The increase could also be secondary to the systemic vasodilatation since the two vascular beds are connected by the ductus arteriosus. In attempting to integrate all these hemodynamic alterations produced ‘by bradykinin in the fetus, we can state that this substance produces a profound pulmonary vasodilatation, diverting, thereby, most of the right ventricular output toward the lungs. This leads to an increase in the left venOn the systemic side, bradykinin also tricular output. produces a marked vasodilatation which is directed more toward the visceral than the umbilical circulation. A redistribution of flows and resistances occurs through which blood is shifted from the placenta toward the rest of the fetal circulation. This seems to insure an adequate venous return to the right side of the heart and a higher than normal right ventricular output. In comparing the circulatory changes produced by bradykinin to those occurring during the transitional period of neonatal life, similarities definitely exist. The changes in the pulmonary and umbilical circulations and in the cardiac functions produced by bradykinin are not greatly different from those observed after lung expansion with air or oxygen (1,3, 12). The only obvious difference is the decrease in the systemic vascular resistance and pressure produced by bradykinin -which usually does not occur after birth. But here the situation is complicated by the presence of an intact umbilicoplacental circulation. In the fetal lamb, expansion of the lungs without clamping the umbilical cord produces a transient fall in the aortic pressure (1 y 3). Although this fall has been attributed to the change in the direction of ductus flow, there is no reason to believe that it cannot be due to other factors. The arterial pressure rises after clampelimination ing the cord; but under these circumstances, of the low resistance of the placenta plays a major role. If the cord is not clamped for several minutes after lung ven- 1382 tilation, the blood flow through the umbilicoplacental vascular bed decreases progressively and is shifted to the visceral vasculature which undergoes a dilatation (1, 3). These changes are again similar to those produced by bradykinin. ASSALI, JOHNSON, BRINKMAN, AND HUNTSMAN The authors are indebted to Sandoz Pharmaceuticals for the supply of bradykinin and to Mr. R. Cutait for his technical assistance. This study was supported by National Heart and Lung Institute Grant HE O1755* Received for publication ‘23 April 1971. REFERENCES 1. ASSALI, N. S., G. A. BEKEY, AND L. W. MORRISON. Fetal and neonatal circulation. In: Biology of Gestation, edited by N. S. Assali. New York: Academic, 1968, vol. II, p. 51-141. 2. A~SALI, N. S., T. H. KIRSCHBAUM, AND P. V. DILTS, JR. Effects of hyperbaric oxygen on uteroplacental and fetal circulation. Circulation Res. 22 : 573-588, 1968. 3. ASSALI, N. S., J. A. MORRIS, AND R. BECK. Cardiovascular hemodynamics in the fetal lamb before and after lung expansion. Am. J. Physiol. 208 : 122-129, 1965. 4. ASSALI, N. S., J. A. MORRIS, R. W. SMITH, AND W. A. MANSON. Studies on ductus arteriosus circulation. Circulation Res. 13: 478489, 1963. 5. BECK, R., J. A. MORRIS, AND N. S. A~SALI. Calibration characteristics of the pulsed field electromagnetic flowmeter. Am. J. Med. Electron. 4 : 87-91, 1965. 6. BOBBIN, R. P., AND P. S. GUTH. Venoconstrictive action of bradykinin. J. Pharmacol. Exftl. Therap. 160 : 1 l-2 1, 1968. 7. BORN, G. V. R., G. S. DAWES, J. C. MOTT, AND B. R. RENNICK. The constriction of the ductus arteriosus caused by oxygen and by asphyxia in newborn lambs. J. Physiol., London 132 : 304-342, 1956. 8. BRECHER, G. A., AND G. F. BROBMANN. Effects of kallikrein on the cardiovascular system. In : Bradykinin, Kallidin, and Kallikrein, edited by E. G. Erdos. Berlin: Springer, 1970, p. 351-361. 9. BRINKMAN, C. R. III, T. H. KIRSCHBAUM, AND N. S. ASSALI. The role of the umbilical sinus in the regulation of placental vascular resistance. Gynecol. Invest. 1 : 115-127, 1970. 10. CAMPBELL, A. G. M., G. S. DAWES, A. P. FISHMAN, A. I. HYMAN, AND A. M. PERKS. Release of a bradykinin-like pulmonary vasodilator substance in faetal and newborn lambs. J. Physiol., London 195 : 83-96, 1968. 11. DAVIGNON, J., R. R. LORENZ, AND J. T. SHEPHERD. Response of human umbilical artery to changes in transmural pressure. Am. J. Physiol. 209 : 5 l-59, 1965. 12. DAWES, G. S. Foetal and Neonatal Physiology. Chicago: Year Book, 1968. 13. DAWES, G. S., J. C. MOTT, AND J. G. WIDDICOMBE. Closure of the foramen ovale in newborn lambs. J. Physiol., London 128 : 384395, 1955. 14. DEPASQUALE, N. P., AND G. E. BURCH. Influence of bradykinin on isolated canine venous strip. Am. Heart J. 75 : 630-633, 1968. 15. ELTHERINGTON, L. G., J. STOFF, T. HUGHES, AND K. L. MELMON. Constriction of human umbilical arteries : Interaction between oxygen and bradykinin. Circulation Res. 22 : 747-754, 1998. 16. HADDY, F. J., T. E. EMMERSON, JR., J. B. SCOTT, AND R. DAUGH- ERTY, JR. The effects of the kinins on the cardio-vascular system. Kallidin, and Kallikrein, edited by E. G. Erdos. In: Bradykinin, Berlin : Springer, 1970, p. 362-384. 17. HEYMAN, M. A., A. M. RUDOLPH, A. S. NIES, AND K. L. MELMON. Bradykinin production associated with oxygenation of the fetal lamb. Circulation Res. 25 : 52 l-534, 1969. 18. HYMAN, A. L. The effects of bradykinin on the pulmonary veins. J. Pharmacol. Exptl. Therap. 161 : 78-87, 1968. 19. JOHNSON, G. H., C. R. BRINKMAN III, AND N. S. ASSALI. Effects of acid, base, and hypertonicity on fetal and neonatal cardiovascular hemodynamics. Am. J. Physiol. 220: 1798-1807, 197 1. 20. KELLERMEYER, R. W., AND R. C. GRAHAM, JR. Kinins: possible physiologic and pathologic roles in man. New Engl. J. Med. 279: 802-807, 1968. 21. KONZETT, H., AND G. BAUER. The action of hypotensive polypeptides on the pulmonary artery pressure. Proc. Intern. Symp. Hypotensiue Peptides. 1966, p. 375-383. 22. KOVAL~IK, V. The response of the isolated ductus arteriosus to oxygen and anoxia. J. Physiol., London 169: 185-197, 1963. 23. KOVAL~IK, V., M. KRISKA, J. SLAMOVA, AND S. DALEZEL. Concerning the mechanisms of constriction of ductus arteriosus. Proc. Intern. Congr. Physiol. Sci., 26th, Washington, D. C., 1948. p. 246. 24. LEWIS, B. V. The response of isolated sheep and human umbilical arteries to oxygen and drugs. J. Obstet. Gynaecol. Brit. Commonwealth 75 : 87-91, 1968. 25. MCINTYRE, T. W. Active and Passive Mechanical Properties of Vascular Smooth it4uscZe (PhD Dissertation). UCLA School of Medicine, 1965. 26. MELMOX, K. L., M. J. CLINE, T. HUGHES, AND A. S. NIES. Kinins: possible mediators of neonatal circulatory changes in man. J. Clin. Invest. 47 : 1295-1302, 1968. 27. MORRIS, J. A., G. A. BEKEY, N. S. ASSALI, AND R. BECK. Dynamics of blood flow in the ductus arteriosus. Am. J. Physiol. 208 : 47 l-476, 1965. 28. REICHGOTT, M. J., AND K. L. MELMON. Bradykinin and the cardiovascular system. Circulation 42 : 563-566, 1970. 29. ROSAS, R., D. MONTAGUE, M. GROSS, AND D. F. BOHR. Cardiac action of vasoactive polypeptides in the rat. Circulation Res. 26: 150-161, 1965. 30. ROWE, G. G., S. AFONSO, C. A. CASTILLO, F. LIOY, J. E. LUGO, AND C. W. CRUMPTON. The systemic and coronary hemodynamic effect of synthetic bradykinin. Am. Heart J. 65 : 656-663, 1963. 31. WESTERSTEN, A., E. RICE, C. R. BRINKMAN III, AND N. S. ASSALI. A balanced field-type electromagnetic flowmeter. J. Ap,cll. Physiol. 26 : 497-500, 1969.