A NICE perspective on the treatment of childhood mental disorders
advertisement

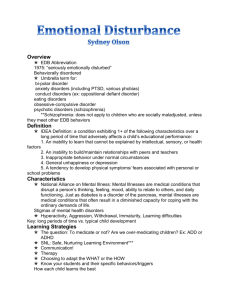
A NICE perspective on the treatment of childhood mental disorders Professor Stephen Pilling PhD Director, National Collaborating Centre for Mental Health University College London The Issues • The obvious – origin of adult disorders • The comparison – broad range of effective adult interventions • The evidence - narrow range of CYP interventions • The curious – limits on the development of the CYP evidence base • Two case studies – conduct disorder and social anxiety disorder • The solutions – questions to consider Origin of adult disorders • 50%+ of adult disorders have their origins in childhood • Course of disorder can be more chronic with early onset (depression, conduct disorder) • Impact on mental health can be wide ranging (e.g. SAD 15% at 25 but 60% have sig. symptoms – Beedas et al, 2012) • Impairments in functioning (e.g. education, employment) can have lasting effects (conduct disorder, social anxiety disorder) – 28% reduction in earnings at 50yrs (Goodman et al 2011) • Problems not recognised – Depression simply missed (DD% missed) – Depression mis-diagnosed (BPD – 20% of 1st presentations) – CD – mis-labelled as ‘naughty behaviour Stepped-care for common adult mental health disorders Step 3: Persistent subthreshold depressive symptoms or mild to moderate depression that has not responded to a low-intensity intervention; initial presentation of moderate or severe depression; GAD with marked functional impairment or that has not responded to a low-intensity intervention; moderate to severe PD; OCD with moderate or severe functional impairment; PTSD. SAD, Eating disorders, Depression: CBT, IPT, behavioural activation, behavioural couples therapy, counselling*, short-term psychodynamic psychotherapy*, GAD: CBT, applied relaxation, drug treatment, combined interventions, self-help groups. Panic disorder: CBT, antidepressants, self-help groups. OCD: CBT (including ERP), self-help groups. PTSD: Trauma-focused CBT, EMDR, Social Anxiety Disorder: CBT, STPP, CCBT Eating Disorders: CBT, IPT, Family Interventions, All disorders: Support groups, befriending, rehabilitation programmes, educational and employment support services; referral for further assessment and interventions. Step 2: Persistent subthreshold depressive symptoms or mild to moderate depression; GAD; mild to moderate panic disorder; mild to moderate OCD; PTSD (including people with mild to moderate PTSD)., Eating Disorders Depression: Individual facilitated self-help, computerised CBT, structured physical activity, groupbased peer support (self-help) programmes**, non-directive counselling †,, self-help groups. GAD and panic disorder: Individual non-facilitated and facilitated self-help, psychoeducational groups, self-help groups. OCD: Individual or group CBT (including ERP), self-help groups. PTSD: Trauma-focused CBT or EMDR. Eating Disorders:, CCBT* All disorders: Support groups, educational and employment support services; referral for further assessment and interventions. Step 1: All disorders – known and suspected presentations of common mental health disorders. All disorders: Identification, assessment, psychoeducation, active monitoring; referral for further assessment and interventions * Discuss with the person the uncertainty of the effectiveness of counselling and psychodynamic psychotherapy in treating depression. ** For people with depression and a chronic physical health problem. † For women during pregnancy or the postnatal period. CBT, cognitive behavioural therapy; ERP, exposure and response prevention; EMDR, eye movement desensitisation and reprocessing; GAD, generalised anxiety disorder; OCD, obsessive compulsive disorder; IPT, interpersonal therapy; PTSD, post-traumatic stress disorder. Care for CYP mental health disorders Step 3: Persistent subthreshold depressive symptoms or mild to moderate depressionor anxiety disorders that has not responded to a low-intensity intervention; GAD PD; OCD; PTSD. SAD, CD Depression: CBT, STPP. Conduct Disorder: Parent training, MST, CBT GAD: CBT*, Panic disorder: CBT*,. OCD: CBT (including ERP)*. PTSD: Trauma-focused CBT, EMDR, Social Anxiety Disorder: CBT Step 2: Mild to moderate depression and anxiety disorders and eating disorders . Depression: CCBT Anxiety Disorders: CCBT Eating Disorders : CCBT ODD/CD: Parent training Step 1: All disorders – known and suspected presentations of common mental health disorders. All disorders: Identification, assessment; referral for further assessment and interventions * Discuss with the person the uncertainty of the effectiveness of counselling and psychodynamic psychotherapy in treating depression. ** For people with depression and a chronic physical health problem. † For women during pregnancy or the postnatal period. CBT, cognitive behavioural therapy; ERP, exposure and response prevention; EMDR, eye movement desensitisation and reprocessing; GAD, generalised anxiety disorder; OCD, obsessive compulsive disorder; IPT, interpersonal therapy; PTSD, post-traumatic stress disorder. Reasons for limitations of CYP evidence base • Resources – Limited funding of treatment research childhood disorders • Capacity – Limited number of individuals with treatment development/evaluation skills • Focus in research settings – Developmental psychopathology/neurodevelopmental • Focus in clinical settings – Psychodynamic/systemic approaches • Models of disorder – Comorbidity and complexity – Social and family setting NICE mental health guidelines - criticism of methods (1) • Results from RCTs will not generalise – but they can – Effects similar in clinically representative populations (Shadish et al, 2000 Psych. Bull.) – Replicated in routine, unselected populations Panic Disorder (PCT) Wade et al 1998 (JCCP) (CT) Grey et al 2009 (Beh. Cog. Psych.) PTSD (CT) Gillespie et al 2002 (Behav. Res.Ther.) (CBT) Brewin et al. 2008 (J. Traum. Stress) Social Phobia (CBT) Lincoln et al 2003 (Behav. Res.Ther.) Depression & Anxiety (CBT) Persons 2006 (Behav. Res.Ther.) – Replicated in populations rejected from RCTs OCD (CBT) Franklin et al 2000 (JCCP) • But only if if you use the same treatment programme and appropriately trained therapists NICE mental health guidelines - criticism of methods (2) • Comorbidities are excluded from RCTs and so limit generalisation but in fact – are common in trials (for example, see NICE Guidelines on: Eating Disorder, 2003; PTSD, 2005; Drug Misuse, 2008; ADHD, 2008; ASPD (conduct disorder), 2009) and participation in trials – results in significant reductions in depression in PTSD and eating disorders – results in positive outcomes on primary outcomes in drug misuse, ADHD and conduct disorder • Presence of comorbidities may require – careful selection of the intervention – extension of duration of the (same) evidence based treatment Contingency Management in Substance Misuse Review: Comparison: Outcome: Study or sub-category DMP TG3 - 07: CM by number of urinalyses 02 MMT + CM (1, 2 or 3 urines a week) 01 Achieved a minimum period of abstinence CM + MMT n/N 01 1 urine sample weekly 9/16 CHUTUAPE2001: Weekly 17/29 MCCLELLAN1993 45 Subtotal (95% CI) Total events: 26 (CM + MMT), 9 (MMT + Control) Test for heterogeneity: Chi² = 0.77, df = 1 (P = 0.38), I² = 0% Test for overall effect: Z = 3.61 (P = 0.0003) 02 2 urine samples weekly 11/19 PETRY2002 12/40 PETRY2005c 33/198 PIERCE2006 257 Subtotal (95% CI) Total events: 56 (CM + MMT), 13 (MMT + Control) Test for heterogeneity: Chi² = 3.31, df = 2 (P = 0.19), I² = 39.6% Test for overall effect: Z = 5.11 (P < 0.00001) 05 3 urine samples weekly 12/40 SCHOTTENFELD2005 11/26 SILVERMAN2004 8/25 STITZER1992 10/20 SILVERMAN1998 19/30 RAWSON2002 141 Subtotal (95% CI) Total events: 60 (CM + MMT), 16 (MMT + Control) Test for heterogeneity: Chi² = 6.41, df = 4 (P = 0.17), I² = 37.6% Test for overall effect: Z = 5.19 (P < 0.00001) 443 Total (95% CI) Total events: 142 (CM + MMT), 38 (MMT + Control) Test for heterogeneity: Chi² = 11.06, df = 9 (P = 0.27), I² = 18.6% Test for overall effect: Z = 8.14 (P < 0.00001) MMT + Control n/N RR (fixed) 95% CI Weight % RR (fixed) 95% CI 2/19 7/32 51 4.78 17.40 22.18 5.34 [1.34, 21.25] 2.68 [1.30, 5.52] 3.25 [1.72, 6.17] 5/23 4/37 4/190 250 11.82 10.86 10.67 33.36 2.66 2.78 7.92 4.38 [1.12, [0.98, [2.86, [2.48, 6.33] 7.85] 21.92] 7.72] 6/40 0/26 2/25 0/19 8/30 140 15.68 1.31 5.23 1.34 20.91 44.47 2.00 23.00 4.00 20.00 2.38 3.57 [0.83, [1.43, [0.94, [1.25, [1.24, [2.21, 4.81] 371.00] 17.00] 319.22] 4.56] 5.77] 441 100.00 0.1 0.2 0.5 Favours MMT +Control 1 2 5 10 Favours MMT + CM 3.77 [2.74, 5.19] Conduct Disorder (NICE, 2013) • School-based interventions – classroom based social and emotional learning programmes for at risk children • Parent training (PPP, IYs) – group based – group based fostering – individually based • Multi-modal interventions – Multi-systemic therapy • CBT - group based social and cognitive problem solving Social Anxiety Disorder (NICE, 2013) • Non-disorder specific anxiety disorder – Individual CBT (smd = 0.15) • CBT – Group or individual CBT (with possible parental involvement for younger children) (smd = 0.56) • Adult CBT – Adult CBT for children over 15 (smd = 1.2 (in adults)) Prevention • SEAL (Durlak et al, 2011) – Classroom based interventions – Improvements in • social and emotional skills • behavioural problems • academic achievement • Depression (Garber et al 2009) – Group based CBT for CYP with at risk of depression parents (HR= 0.68) The Future • Prevention – School – Internet • Case identification and recognition – Effective tools (?SDQ) – Effective referral pathways – Location of services • Models/theories of childhood disorders – disorder based models – which theories The Future (2) • Disorder/problem specific approaches – Disorder specific interventions – Pan-diagnostic interventions – Competence based approaches • Parent led interventions – Anxiety disorders • Adaptation of adult interventions – long term or short term solution