2005 Annual Report North American Pediatric Renal Transplant Cooperative Study (NAPRTCS)
")
North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS)
2005 Annual Report
Renal Transplantation
Dialysis
Chronic Renal Insufficiency
This is a privileged communication not for publication.
This study is sponsored by major grants from:
Novartis Pharmaceutical Corporation
AMGEN Inc.
Genentech, Inc.
NAPRTCS also thanks the following contributors:
Roche Laboratories, Inc.
Wyeth Research
Watson Pharmaceuticals
North American Pediatric Renal Transplant Cooperative Study
Clinical Coordinating Center
William Harmon, M.D.
Data Coordinating Center
NAPRTCS
1 Autumn Street
5th Floor
Boston, Massachusetts 02115
Donald Stablein, Ph.D.
Lynya Talley, Ph.D.
The EMMES Corporation
401 N. Washington Street, Suite 700
Rockville, Maryland 20850
617-355-7707 301-251-1161
Board Members
William Harmon, MD
(President)
Richard Fine, MD
(Vice President/Treasurer)
Steven Alexander, MD
(Secretary)
Bradley Warady, MD
(Member at Large)
Mark Benfield, MD
(Member at Large)
Stuart Goldstein, MD
(Chair, PCC)
Ruth McDonald, MD
(Chair, Special Studies Committee and Vice-Chair, PCC)
This report was developed under the auspices of the Operations Committee and prepared by
Lynya Talley, Ph.D. and Donald M. Stablein, Ph.D.
With assistance from Data Coordinating Center Staff
Stuart Berlin
Angela Norman
Kumar Thotapally
Danielle Weidenhamer-Quarles
TABLE OF CONTENTS
I INTRODUCTION
II TRANSPLANTATION
Section 1: Transplant Patient Characteristics
Section 2: Donor History and Antigen Mismatches
Section 3: Therapy
Section 4: Rejection
Section 5: Graft Function
Section 6: Growth
Section 7: Morbidity, Malignancy, and Mortality
III DIALYSIS
Section 8: Dialysis Patient Characteristics
Section 9: Dialysis Access Data
Section 10: Erythropoietin Use in Dialysis Patients
Section 11: Dialysis Follow-up
Section 12: Growth
IV CHRONIC RENAL INSUFFICIENCY
Section 13: CRI Patient Demographics
Section 14: Termination of Chronic Renal Insufficiency Status
Section 15: CRI Follow-up Data
V APPENDICES
Appendix A: Participating Centers and Contact Physicians
Appendix B: Bibliography C 1988-2004
Appendix C: Special Studies and Analyses i
13-1
14-1
15-1
A-1
B-1
C-1
PAGE
1
1-1
2-1
3-1
4-1
5-1
6-1
7-1
8-1
9-1
10-1
11-1
12-1
LIST OF EXHIBITS
Exhibit 1.7
Section 2
Exhibit 2.1
Exhibit 2.2
Exhibit 2.3
Exhibit 2.4
Section 3
Exhibit 3.1
Section 1
Exhibit 1.1
Exhibit 1.2
Exhibit 1.3
Exhibit 1.4
Exhibit 1.5
Exhibit 1.6
Exhibit 3.2
Exhibit 3.3
Exhibit 3.4
Exhibit 3.5
Exhibit 3.6
Exhibit 3.7
Patient Registrations, Transplants, and Selected Characteristics, by Year of Registration
Recipient and Index Transplant Characteristics
Transplant Characteristics
Age at Transplantation
Age at Index Transplant, by Patient's Sex, Race, and Diagnosis
Sex, Race, and Biopsy Distributions, by Primary Renal Diagnosis
Primary Diagnosis by Age
Donor Information
Use Over Time of Donor-Specific and Random Blood Transfusions
Percent HLA Mismatches
Age at Transplant and Donor Source
Medication Data—First 30 Days, Transplants after 1995
Week 1 Calcineurin Inhibitor Use, by Induction Antibody
3-5
3-6
Induction Antibody Use, by Year
Mean (SE) Daily Drug Dosages, by Drug Combination and Year Post-Transplant
3-6
3-7
Percent of Patients with Functioning Grafts Receiving Immunosuppressive
Medication 30 Days Post Transplant, by Year of Transplant 3-8
Percentage of Patients Receiving Designated Maintenance
Immunosuppression Regimens, by Donor Source and Time of Follow-up 3-9
Percentage of Patients Receiving Concomitant Medications, by Donor
Source and Time Post-Transplantation 3-10
2-3
2-4
2-5
2-6
1-4
1-5
1-6
1-7
1-8
1-9
1-10 ii
Section 4
Exhibit 4.1A Frequency of Acute Rejections 4-4
Exhibit 4.1B Acute Rejection Ratios
Exhibit 4.2
4-4
Time to First Rejection Episode, by Allograft Source and Transplant Year 4-5
Exhibit 4.3A Relative Hazard (RH) of First Rejection Episode,
First Transplant, 1987-1995
Exhibit 4.3B Relative Hazard (RH) of First Rejection Episode,
First Transplant, 1996-2004
Exhibit 4.4 Time to First Rejection Episode, by Selected Characteristics
Exhibit 4.5A Rejection Reversal Outcome by Selected Characteristics
4-6
4-7
4-8
4-10
Exhibit 4.5B Rejection Reversal Outcome by Selected Characteristics for
First Acute Rejection Episode Only
Rejection Reversal Outcome by Transplant Year Exhibit 4.6
Exhibit 4.7 Summary of Late First Rejections, by Selected Characteristics
4-11
4-12
4-13
Section 5
Exhibit 5.1 Causes of Graft Failure 5-7
Exhibit 5.2 Percent Graft Survival by Allograft Source
Exhibit 5.3 Graft Failure Summary, by Allograft Source and Transplant
Characteristics
Exhibit 5.4 Percent Graft Survival for Recipients of Living Donor Source Allografts
5-8
5-9
5-11
Exhibit 5.5 Percent Graft Survival for Recipients of Cadaver Donor Source
Allografts
Exhibit 5.6 Percent Graft Survival for Annual Cohort Group
Exhibit 5.7
Exhibit 5.8
Exhibit 5.9
Graft Survival by Donor Source and HLA-Antigen Disparity
Percent Graft Survival, by Donor Source and Diagnosis
Post Week 1 Graft Survival by Donor Source and Acute Tubular
5-12
5-14
5-15
5-16
5-17
Exhibit 5.10 Serial Serum Creatinine and Calculated Creatinine Clearance
Measures for Functioning Grafts, by Age at Transplant
Exhibit 5.11 Serial Serum Creatinine for Functioning Grafts, by Race and
Induction Antibody Therapy
5-18
5-19 iii
Exhibit 5.12 Graft Function, i.e. Graft Survival and Mean Calculated Clearance at Annual Follow-up, by Donor Source
Exhibit 5.13 Graft Function, i.e. Graft Survival and Mean Calculated Clearance at
Annual Follow-up, by Donor Source and Initial Use of Antibody
Preparations
Exhibit 5.14 Graft Function, i.e. Graft Survival and Mean Calculated Clearance at
Annual Follow-up, by Donor Source and Race
Section 6
Exhibit 6.1
Exhibit 6.2
Exhibit 6.3
Exhibit 6.4
Mean (with SE) Standardized Height and Weight Scores, by Selected
Characteristics and Times Post-Transplantation
Mean Change from Baseline (with SE) in Standardized Height and
Weight Scores in Subjects with Graft Function, by Age at Transplant
Mean (with SE) of Standardized Height at Time of Initial Transplant, by Year of Transplant
Mean (with SE) of Standardized Height at Initial Transplant Over Time, by Year of Transplant and Age at Transplant
Section 7
Exhibit 7.1 Hospitalization Days During the First Post-Transplant Month, by Year of Transplantation and Donor Source
Exhibit 7.2A Transplant Month Hospitalization
Exhibit 7.2B Transplant (1987-1995) Month Hospitalization
Exhibit 7.2C Transplant (1996-2004) Month Hospitalization
Exhibit 7.3A Hospitalization Results for Patients with Functioning Grafts in
Specified Follow-up Periods (Living Donor Transplants)
Exhibit 7.3B Hospitalization Results for Patients with Functioning Grafts in
Specified Follow-up Periods (Cadaver Donor Transplants)
Exhibit 7.4 Selected Characteristics of Transplants with Malignancy
Exhibit 7.5A Percent Patient Survival, by Primary Allograft Source
Exhibit 7.5B Percent Patient Survival, by Era and Primary Allograft Source
Exhibit 7.6A Percent Patient Survival of Primary Transplants, by Age at Transplantation – Living Donor
Exhibit 7.6B Percent Patient Survival of Primary Transplants, by Age at Transplantation – Cadaver Donor
Exhibit 7.7 Causes of Death Following Index Renal Transplantation iv
5-20
5-21
5-22
6-3
6-4
6-5
6-6
7-4
7-5
7-6
7-7
7-8
7-9
7-10
7-11
7-11
7-12
7-12
7-13
Section 8
Exhibit 8.1
Exhibit 8.2
Exhibit 8.3
Exhibit 8.4
Dialysis Patient Demographics
Number and Percent Distributions of Patient Race/Ethnicity, by
Dialysis Modality and Age at Initiation
Post Initiation (1 Month and 12 Months) Concomitant Drug Therapy
Post Initiation (24 Months and 36 Months) Concomitant Drug Therapy
Exhibit 8.5
Exhibit 8.6
Baseline Education Status
Baseline Education Status, by Race
Exhibit 8.7
Exhibit 8.8
Exhibit 8.9
Baseline Education Status, by Age
Percent Full-Time School Attendance
Percent Patient Survival, by Age at Dialysis Initiation
Exhibit 8.10 Causes of Death Following the Index Course of Dialysis
Section 9
Exhibit 9.1A Modality Initiation and Termination
Exhibit 9.1B Termination Reasons for Non-Transplanted Patients by Vintage
Exhibit 9.2A Peritoneal Dialysis Access
Exhibit 9.2B Peritoneal Access Data by Vintage
Exhibit 9.3 Catheter Characteristics for Peritoneal Dialysis Accesses
Exhibit 9.4A Hemodialysis Access
Exhibit 9.4B Hemodialysis Access Data by Vintage
Exhibit 9.5
Exhibit 9.6
Frequency Distribution of Dialysis Access Status, by Selected Characteristics
Reasons for Change of Modality, by Selected Characteristics
Exhibit 9.7 Time to Dialysis Termination for Index Cases
Exhibit 9.8 Time to Dialysis Termination for Index Cases, by Age and
Race/Ethnicity
Exhibit 9.9 Time to Dialysis Termination for Index Cases, by PD Catheter
Characteristics
Exhibit 9.10 Time to Dialysis Termination for Index Cases, by HD Access v
8-4
8-7
8-8
8-9
8-10
8-11
8-12
8-13
8-14
8-15
9-4
9-5
9-6
9-7
9-8
9-9
9-10
9-11
9-12
9-13
9-14
9-15
9-16
Exhibit 9.11 Time to Dialysis Termination for Index Cases, by Reason for
Termination
Exhibit 9.12 Selected CAPD and APD Patient Demographics
Exhibit 9.13 Time to Dialysis Termination for Selected CAPD/APD Cases,
9-17
9-18
9-19
Exhibit 9.14 Time to Transplantation and Change of Modality for Selected
CAPD/APD Cases, by Modality
Exhibit 9.15 Time to First Peritonitis Episode For Selected CAPD/APD Cases,
9-20
9-21
Section 10
Exhibit 10.1 Percent EPO Use, by Months on Dialysis
Exhibit 10.2 Percent EPO Use at Baseline (Day 30)
Exhibit 10.3 Route and Frequency of EPO Administrations
Exhibit 10.4 Mean EPO Dose (Units/Kg/Week)
Exhibit 10.5 EPO Frequency (%) at 6 Months, by Modality and Age at
10-3
10-4
10-5
10-6
10-7
Exhibit 10.6 Distribution of Hematocrit at 6 Months, by EPO Use
Exhibit 10.7 Mean and Median Hematocrit Levels at 6 Months, by EPO Use
10-7
10-7
Section 11
Exhibit 11.1 Peritoneal Dialysis at Follow-up
Exhibit 11.2 Number and Percent of Peritonitis Episodes, by Age
Exhibit 11.3 Peritonitis Infection Rates, by Age and Catheter Characteristics
11-4
11-5
11-6
Exhibit 11.4 Time to First Peritonitis Infection
Exhibit 11.6 Time to First Peritonitis Infection, by Catheter Access Characteristics
11-7
Exhibit 11.5 Time to First Peritonitis Infection, by Age at Peritoneal Dialysis Initiation 11-7
11-8
Exhibit 11.7 Peritoneal Dialysis Access Revision
Exhibit 11.8 Hemodialysis at Follow-up
Exhibit 11.9 Hemodialysis Access Revision
11-10
11-11
11-12 vi
Exhibit 11.10 Time to Cadaver Transplantation, by Era
Exhibit 11.11 Time to Cadaver Transplantation, by Age
Exhibit 11.12 KT/V by Modality, Age, Race, Visit and Baseline BMI
11-13
11-13
11-14
Exhibit 11.13 URR for Hemodialysis Patients by Age, Race, Visit and Baseline BMI 11-15
Section 12
Exhibit 12.1 Mean (SE) Height Z-Scores, by Selected Characteristics and Times
Following Dialysis Initiation
Exhibit 12.2 Mean (SE) Weight Z-Scores, by Selected Characteristics and Times
Following Dialysis Initiation
Exhibit 12.3 Mean Change from Baseline (with SE) in Standardized Height and Weight Scores, by Age, at Times Following Dialysis Initiation
Exhibit 12.4 12-Month Growth Data, for rhGH-Treated and Untreated Short
Control (z < -1.88) and All Control Patients by Age
12-3
12-4
12-5
12-7
Section 13
Exhibit 13.1A CRI Patient Characteristics
Exhibit 13.1B CRI Diagnoses
Exhibit 13.1C CRI Diagnoses by Race and Gender
Exhibit 13.1D CRI Patient Education Status
Exhibit 13.2 Age at CRI Registration
Exhibit 13.3 Primary Diagnosis, by Race and Age
Exhibit 13.4 Percent Distribution of Baseline Tanner Stage, by Age at CRI
Registration
Exhibit 13.5 Mean Baseline Laboratory Measurements
Exhibit 13.6 Mean Baseline Laboratory Measurements, by Year of CRI
Registration
Exhibit 13.7 Baseline Concomitant Drug Therapy, by Year of CRI
Registration
Exhibit 13.8 Baseline Medical Events History, by Year of CRI
13-3
13-4
13-5
13-6
13-7
13-8
13-9
13-10
13-11
13-12
13-13
Exhibit 13.9 Baseline Renal Function, by Age at CRI Registration
Exhibit 13.10 Mean (and SE) Baseline Height, Weight, SDS and BMI
13-14
13-14 vii
Exhibit 13.11A Baseline Height SDS, by Age at CRI Registration
Exhibit 13.11B Baseline Weight SDS, by Age at CRI Registration
Exhibit 13.12 Baseline Renal Function, by Height Z-Score
Exhibit 13.13 Baseline Renal Function, by Height Z-Score and Age at Entry
Exhibit 13.14 Baseline Renal Function, by Height SDS and Age at Entry
13-15
13-15
13-16
13-17
13-18
Section 14
Exhibit 14.1 CRI Termination Summary
Exhibit 14.2 Frequency and Percent CRI Termination, and Reason for
Termination by Selected Patient Characteristics
14-3
14-4
Exhibit 14.3 Risk of Progression to ESRD (Transplant and Dialysis Initiation)
Exhibit 14.4 Progression to ESRD
14-6
14-7
Exhibit 14.5 Progression to ESRD, by Baseline Calculated Creatinine Clearance
) 14-7
Exhibit 14.6 Progression to ESRD, by Race, Gender, Age at Entry, Primary
Diagnosis, and Baseline Laboratory Results
Exhibit 14.7 Progression to ESRD Due to Transplantation and Dialysis Initiation
14-8
14-10
Section 15
Exhibit 15.1 CRI Follow-up Data
Exhibit 15.2 Mean (+SE) Height Z-Score, by CRI Visit and Selected Baseline
Characteristics
Exhibit 15.3 Mean Change from Baseline (+SE) in Height Z-Score, by CRI Visit and
Selected Baseline Characteristics
Exhibit 15.4 Mean (+SE) Weight Z-Score, by CRI Visit and Selected Baseline
Characteristics
Exhibit 15.5 Mean Change from Baseline (+SE) in Weight Z-Score, by CRI Visit and Selected Baseline Characteristics
Exhibit 15.6A Serum Creatinine (mg/dL) and Calculated Creatinine Clearance
): Means and Changes from Baseline (+SE),
15-5
15-6
15-7
15-8
15-9
Exhibit 15.6B by Age at Entry
Schwartz Calculated Clearance by Primary Diagnosis
15-10
15-11
Exhibit 15.6C Delta Schwartz Calculated Creatinine Clearance by Primary Diagnosis 15-12 viii
Exhibit 15.7A 12-Month Growth Data and Renal Function Data, for rhGH Treated and Untreated Short Control (z < -1.88) and Control Patients
Exhibit 15.7B 12-Month Growth Data and Renal Function Data, for rhGH Treated and Untreated Short Control (z < -1.88) and Control Patients Excluding
0 - 1 Year Old Patients
Exhibit 15.8A 18-Month Growth and Renal Function Data, for rhGH Treated and Untreated Short Control (z < -1.88) and Control Patients
Exhibit 15.8B 18-Month Growth and Renal Function Data, for rhGH Treated and Untreated Short Control (z < -1.88) and Control Patients Excluding
0 - 1 Year Old Patients
Exhibit 15.9 Growth Hormone Utilization for All Age-Sex-Appropriate CRI Patients with Height Z-Score of -1.88 or Worse, and Tanner Stage I, II, III at the Baseline, or 6-Month, or 12-Month Visit
15-13
15-14
15-15
15-16
15-17
Exhibit 15.10 Growth Hormone Utilization for All Age-Sex-Appropriate CRI Patients with Height SDS of -1.88 or Worse, and Tanner Stage I, II, III at the Baseline, and 6-Month, and 12-Month Visits 15-18
Exhibit 15.11 Growth Hormone Utilization for Current Age-Sex-Appropriate CRI Patients with Height SDS of -1.88 or Worse, and Tanner Stage I, II, III at the Most Recent Completed Visit in 2003 15-19 ix
I. INTRODUCTION
Introduction
INTRODUCTION
The North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) is a research effort organized in 1987. At the outset of the study, the operational objective of this group was to obtain the voluntary participation of all renal transplant centers in the United States and Canada in which multiple (>4) pediatric patients received renal allografts annually. Scientific objectives included capture of information about current practice and trends in immunosuppressive therapy with an ultimate goal of improving care of pediatric renal allograft recipients in North America. In 1992, the study was expanded to include pediatric patients who receive maintenance hemodialysis or peritoneal dialysis therapy. In 1994, data collection began on patients with chronic renal insufficiency (CRI), defined as a Schwartz calculated creatinine clearance ≤ 75 mL/min/1.73 m 2 .
Now, not only do we hope to register and follow greater than 80% of the children receiving renal allografts in the United States and Canada, but to study the clinical course and natural history of patients with renal dysfunction and to continue following these patients as they move among the end-stage renal disease (ESRD) therapeutic modalities, thus allowing the NAPRTCS to become a complete ESRD patient data system.
The NAPRTCS has three functioning organizational bodies: the Clinical Coordinating Center, the
Data Coordinating Center, and the participating Clinical Centers. Appendix A details the structure and members of the Coordinating Centers and the participating Clinical Centers are listed in
Appendix B.
This report summarizes data received at the Data Coordinating Center through December 15, 2004.
We continue to be particularly pleased and grateful for the enthusiastic response of the volunteer clinical centers, without which this project could not be successful.
At the outset of NAPRTCS, "children" were defined as patients who had not yet attained their 18th birthday at the time of their index transplant. The index transplant is defined as the first transplant reported to NAPRTCS during the study period. When the study expanded in 1992 to include maintenance dialysis patients, the age criterion was expanded to include patients who had not yet attained their 21st birthday at the time of index transplant or at the time of index initiation of dialysis, whichever came first. The expanded age criterion was adopted for CRI patients.
Data submission for the study is organized to enable analysis of both patient and event characteristics. Among transplant patients, for example, we are interested in graft survival,
1
NAPRTCS 2005
Introduction morbidity, and the relationships that these endpoints have to patient characteristics such as race/ethnicity, sex, and primary renal disease, and to transplant (i.e., event) characteristics such as age at transplantation, donor source, immunosuppressive treatment, and HLA antigen mismatches.
Analogous patient and event characteristics are defined in both the CRI and dialysis populations.
As data have matured, it has been our intent to design special studies that focus on issues such as quality of life, rehabilitation, physical and mental development, and other questions of interest for particular patient subgroups. In this manner, the study has served — and continues to serve — as a resource to investigators whose research activities are consistent with the goals and objectives of the program. A list of special studies and analyses is shown in Appendix C.
Transplantation follow-up status forms are submitted 6 months following transplant and every 6 months thereafter. For dialysis, follow-up status forms are submitted 30 days after initiation, 6 months after initiation, and every 6 months thereafter. CRI follow-up status forms are submitted at
6-month intervals following the initial reported clinic visit.
As of database closure for this report, over 14,500 patients had been registered in NAPRTCS, as shown in the table below. Of these patients, data have been reported to all three registries (CRI, dialysis, and transplantation) for 684. Registry-specific sample sizes can be determined by summing the subgroup totals. For example, the number of transplant patients — 8,435 — is given by 4,219 + 744 + 2,788 + 684. These data do not necessarily represent a complete accounting of a patient’s clinical course: a patient may have received care for his CRI at a NAPRTCS center, received maintenance dialysis at a non-NAPRTCS center, and rejoined the study when transplantation was performed at a NAPRTCS center.
NAPRTCS PATIENT REGISTRATIONS
All Patients
CRI only
Dialysis only
Transplant only
CRI and dialysis
CRI and transplant
Dialysis and transplant
CRI, dialysis, and transplant
2
14,575
3,971
1,641
4,219
528
744
2,788
684
100.0
27.2
11.3
28.9
3.6
5.1
19.1
4.7
Introduction
Forms have been submitted for 9,243 renal transplants: 8,435 are for index transplants (i.e., first transplant reported to registry) while 808 represent additional reported transplants in the same patient since the study's start on January 1, 1987. The 8,435 index transplants are comprised of
4,181 cases where transplantation was the initial reported modality and 4,254 cases where transplantation occurred subsequent to an initial report of patient registration in the dialysis
(n=2,833) or CRI (n=1,421) registries.
Modality initiation forms have been submitted for 7,357 independent courses of dialysis. An independent course of dialysis therapy is defined to have occurred when a patient is maintained on a given modality for 30 or more days. Of these, 5,641 represent index initiations and 1,717 are for initiations subsequent to the index course. The 5,641 index dialysis courses are comprised of
3,910 cases where dialysis is reported as the initial therapy and 1,731 cases of dialysis initiation subsequent to failure of the index graft (n=638) or termination of CRI status (n=1,136).
Initial CRI status forms have been submitted for 5,927 patients. In NAPRTCS, patients are eligible for the chronic renal insufficiency component if, at the first reported clinic visit, the Schwartz calculated creatinine clearance is 75 mL/min/1.73 m 2 or lower. In total, we have received a CRI
Termination Form for 2,534 of the 5,927 CRI patients.
This report summarizes both patient-level and therapy-level data. In general, descriptive information will focus on the transplant or dialytic modality as the unit of observation. Variables pertinent to the patient (e.g., sex, race, primary diagnosis) will use the number of patients as the denominator. Formal analysis of failure times — patient and graft survival and rejection-free intervals — include only the first transplant during the study period (the index transplant) for each patient. Occasional missing information on individual characteristics results in the analysis of slightly different subgroups. Continued capture of this information is part of the ongoing data collection process.
In addition to the registry components, NAPRTCS initiated its first randomized prospective clinical trial (Protocol IN01) in 1995, the first ever controlled clinical trial of OKT3 induction therapy in children and adolescents. Nested within the primary random assignment to the OKT3 or No OKT3 groups, patients were randomized to receive either Sandimmune or Neoral maintenance cyclosporine therapy. Randomized prospective trials of growth hormone have been performed: one was designed to evaluate the post transplant use of recombinant human growth hormone (rhGH) therapy and the second was a study of rhGH therapy in pediatric dialysis patients. In the transplant
3
NAPRTCS 2005
Introduction study, patients were randomized to standard dose (.05/mg/kg/day) therapy or a delayed treatment control group. After the initial no treatment period of 12 months, control group patients received rhGH therapy for the duration of the study — which is a total of 42 months. In the dialysis study, all patients receive standard dose rhGH therapy during the first 12 months, after which patients are randomized either to continue on standard dose therapy or to receive a double dose
(.10/mg/kg/day). Patients continued on their "randomized" dose for an additional 12 months.
Through the collaborative Clinical Trials in Pediatric Transplantation effort sponsored by the NIAID,
NAPRTCS sites have completed enrollment into a large double-blind, randomized trial to evaluate potential to withdraw steroid therapy in transplant patients. Increased accrual to such studies is an important current group objective.
4
II. TRANSPLANTATION
SECTION 1: TRANSPLANT PATIENT CHARACTERISTICS
NAPRTCS 2005
Transplant
Patient and transplant characteristics are summarized in Exhibit 1.1 for the 18-year history of the cooperative study. Because of reporting lags, annual accrual totals are still likely to increase, particularly for the later years. The number of transplants for 2004 however has increased by 530 since the previous year’s report. As of database closure for this report, 9,243 renal transplants had been reported for 8,435 pediatric patients. This represents 530 new transplants and 496 patients with their first registry transplant since the last report.
The percentage of males in the registry, about 59%, has been relatively constant over time. White patients comprise 62% of the cohort, black patients 16%, and Hispanic patients 16%. The percentage of white patients in a given year has decreased from a high of 72% in 1987 to under
55% in 2004. There had been a steady increase in the percent of living donors: in 1998, living donation has accounted for about 58% of transplants with living donations peaking at 64% in 2002, compared to 43% in the first four years of the registry. However, the percentage has been under
60% in the last 2 years. Fifty-two percent of all allografts have come from a living donor. Since the study’s initiation, fewer transplants have been reported over time that involve young recipients (<6 years old) or young cadaver donors (<10 years old). While the percentage decrease in recipients
<6 years old has been gradual — in 2000 and 2001 young recipients accounted for 18% and 21% of all transplants, compared to 25% in 1987 — the decline in the use of young donors (<10 years old) has been more precipitous, resulting in a percentage point decrease from 38% in 1988 to 14% in 1999 and 6% in 2004.
Recipient history is further characterized in Exhibit 1.2. The most common primary diagnoses remain as obstructive uropathy and aplastic/hypoplastic/dysplastic kidneys, each present in about
16% of patients. Focal segmental glomerulosclerosis (FSGS) is the third most common (11%) and continues to be the most prevalent acquired renal disease. The five most frequent diagnoses, excluding unknown and “other” diagnoses, total 52% of the cases, while the remaining diagnoses are each present in no more than 3% of patients. A diagnosis was established for 94% of patients, while biopsy or nephrectomy confirmation of diagnosis is known not to have occurred in 44% of patients. The distributions of the five most prevalent diagnoses vary between black and white patients. For blacks, FSGS is most prevalent (23%), followed by obstructive uropathy (15%), aplasia/hypoplasia/dysplasia (14%), chronic glomerulonephritis (GN) (4%), and SLE nephritis (4%).
The prevalences of cystinosis, reflux nephropathy, and hemolytic uremic syndrome were under 2% among black transplant patients. Among whites, however, the order of the five most prevalent
1-1
NAPRTCS 2005
Transplant diagnoses is: obstructive uropathy (17%), aplasia/hypoplasia/dysplasia (17%), FSGS (9%), reflux nephropathy (6%), and medullary cystic disease (4%). The relative order of these prevalent primary diagnoses among Hispanics is similar to that for white patients.
At the time of their index transplant, 10% (827/8,435) of patients were receiving their second (or greater) transplant. Twenty-five percent of primary transplants were preemptive, as these patients had never received maintenance dialysis (Exhibit 1.3). The rate of preemptive transplantation differs significantly (p<0.001) between recipients of living (33%) and cadaver (13%) source organs; between males (28%) and females (20%); among age groups, with rates of 20%, 24%, 28%, 23%, and 21% for recipients 0-1, 2-5, 6-12, 13-17, and 18-20 years old; and across races with whites, blacks, Hispanics, and “other” races having preemptive transplantation rates of 30%, 14%, 16%, and 16%, respectively. Immediately prior to the primary transplant, the percentages of patients maintained exclusively on hemodialysis and peritoneal dialysis were 29.8% and 39.4%. At the time of primary transplant few spleens had been removed (<1%) and all native renal tissue had been removed in 23% of patients; transplanted grafts have been removed in 37.1% of the index nonprimary transplants (Exhibit 1.3).
Exhibit 1.4 details recipient age at transplant. Of the 89 transplants occurring in children younger than 12 months old, there were 5, 21, and 61 transplants, respectively, within the 3-5, 6-8 and 9-11 months age categories, and two were less than 3 months. Only 29 infant transplants have been performed since 1996, six in 1996, three in 1997, three in 1998, five in 1999, one in 2000, four in
2001, six in 2002 and one in 2004 — although these numbers may increase as enrollment reports increase. In Exhibit 1.5, it is observed that the sex distribution is most unbalanced in the youngest age groups where 70% of 0-1 and 66% of 2-5 year old patients are male; the distribution is more even among adolescents. This is due to the fact that males comprise the majority of the aplasia/hypoplasia/dysplasia (62%) and obstructive uropathy (86%) diagnoses (see Exhibit 1.6) and the relative incidence of these diagnoses decreases with age. Forty percent of male patients fall into these two diagnostic categories, compared to 21% of females. The contrast is particularly steep in the obstructive uropathy group, a diagnosis shared by 23% of the males, but only 6% of females.
Exhibit 1.6 provides for each primary diagnosis the percentages of patients who are male, white race, and known not to have had a biopsy or nephrectomy confirmation of diagnosis. Of transplant registrants with FSGS, 51% are white. Systemic lupus erythematosis is predominantly a disease of females (82%) with the female-specific race distribution given by 25% white, 39% black, and 25%
1-2
NAPRTCS 2005
Transplant
Hispanic. The percentages of patients without a histologically confirmed tissue diagnosis are 71%,
69%, and 69% in aplastic/hypoplastic/dysplastic, obstructive uropathy, and reflux nephropathy patients, respectively. The comparable rates for FSGS, hemolytic uremic syndrome, and lupus nephritis are 6%, 47%, and 4%.
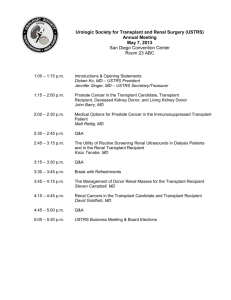
Exhibit 1.7 categorizes primary diagnoses as either FSGS, GN, structural or other and demonstrates how these distributions differ according to age at transplant. GN is comprised of the following primary diagnoses (chronic glomerulonephritis, idiopathic crescentic glomerulonephritis, mebranoproliferative glomerulonephritis – Type I and Type II, SLE nephritis, Henoch-Schonlein nephritis, Berger’s (IgA) nephritis, Wegener’s granulomatosis, and membranous nephropathy.
“Structural” diagnoses (prune belly, reflux nephropathy and aplasia/hypoplasia/displasias) account for the largest proportion of primary diagnoses among children ages 5 and under; whereas, GN diagnoses are more prevalent with increasing age.
1-3
NAPRTCS 2005
Transplant
EXHIBIT 1.1
PATIENT REGISTRATIONS, TRANSPLANTS, AND
SELECTED CHARACTERISTICS, BY YEAR OF REGISTRATION
100
80
%Male
%White
%Living Donor
%Recipient age <6 yrs
%CAD donor age <10 yrs
60
40
20
0
87 89 91 93 95 97 99 01 03
TRANSPLANT YEAR
1987 '88 '89 1990 '91 '92 '93 '94 '95 '96 '97 '98 '99 2000 '01 '02 '03 '04 Total
No. of
Pts 531 501 464 497 498 546 572 545 626 544 547 474 487 399 429 381 259 135 8435
No. of
Tx 542 529 506 549 563 602 620 621 687 622 588 533 536 436 465 412 289 143 9243
1-4
EXHIBIT 1.2
RECIPIENT AND INDEX TRANSPLANT CHARACTERISTICS
NAPRTCS 2005
Transplant
N
(8435)
%
(100.0)
Sex
Race
Primary Diagnosis
Obstructive uropathy
Focal segmental glomerulosclerosis
Reflux nephropathy
Chronic glomerulonephritis
Polycystic disease
Medullary cystic disease
Hemolytic uremic syndrome
Prune Belly
Congenital nephrotic syndrome
Familial nephritis
Idiopathic crescentic glomerulonephritis
Membranoproliferative glomerulonephritis - Type I
Pyelo/interstitial nephritis
SLE nephritis
Renal infarct
Berger's (IgA) nephritis
Henoch-Schonlein nephritis
Membranoproliferative glomerulonephritis - Type II
Wilms tumor
Drash syndrome
Wegener's granulomatosis
Membranous nephropathy
Other systemic immunologic disease
Sickle cell nephropathy
Diabetic glomerulonephritis
1-5
1.9
1.9
1.8
1.7
1.5
1.3
1.2
0.9
0.6
0.5
0.5
0.5
0.4
0.2
0.1
16.1
11.5
5.2
3.5
2.9
2.8
2.7
2.6
2.5
2.2
160
158
156
140
123
110
104
75
47
46
44
40
32
14
9
1355
968
442
292
242
240
231
220
215
188
NAPRTCS 2005
Transplant
EXHIBIT 1.3
TRANSPLANT CHARACTERISTICS
Total Transplants
Index Transplants
Primary Transplants
Repeat Transplant
Maintenance Dialysis Immediately Prior to Transplant
Hemodialysis only
Peritoneal dialysis only
Primary Transplant
9243
8435
7608
1635
2753
3640
7608
100.0
91.3
82.3
17.7
29.8
39.4
100.0
Naive Tissue Removed
Index Non-primary Transplants
Prior Transplants Removed
1744
827
307
23.2
100.0
37.1
1-6
EXHIBIT 1.4
AGE AT TRANSPLANTATION
Age at Transplantation
N
(9243)
%
(100)
NAPRTCS 2005
Transplant
≥ 18
Age Grouping
701 7.6
1-7
NAPRTCS 2005
Transplant
Total
(N=8435)
Gender
Male
Female
Race
White
Black
Hispanic
Other
Diagnosis
Other
EXHIBIT 1.5
AGE AT INDEX TRANSPLANT
BY PATIENT'S SEX, RACE, AND DIAGNOSIS
[Numbers in Table are Percents]
Age at Index Transplantation
0-1
(N=474)
2-5
(N=1276)
6-12
(N=2871)
13-17
(N=3251)
>17
(N=560)
70 66 59 56 55
30 34 41 44 45
76 64 62 59 56
8 14 14 19 24
10 16 17 16 13
6 6 6 6 7
29 24 17 11 9
19 23 16 14 10
51 44 54 62 65
1 9 13 12 15
1-8
NAPRTCS 2005
Transplant
EXHIBIT 1.6
SEX, RACE, AND BIOPSY DISTRIBUTIONS,
BY PRIMARY RENAL DIAGNOSIS
Diagnosis N % Male % White
% Not
Biopsied
Diagnosis
Obstructive uropathy 1355 86 68 69
Focal segmental glomerulosclerosis
Reflux nephropathy
Chronic glomerulonephritis
Polycystic disease
Medullary cystic disease
Hemolytic uremic syndrome
Prune Belly
Congenital nephrotic syndrome
Familial nephritis
968
442
292
242
240
231
220
215
188
57
44
42
51
50
56
98
52
80
51
79
52
78
88
84
64
71
65
6
66
26
48
34
47
62
12
27
Idiopathic crescentic glomerulonephritis
Membranoproliferative glomerulonephritis - Type I
Pyelo/interstitial nephritis
SLE nephritis
Renal infarct
Berger's (IgA) nephritis
Henoch-Schonlein nephritis
Membranoproliferative glomerulonephritis - Type II
Wilms tumor
Drash syndrome
Wegener's granulomatosis
Membranous nephropathy
Other systemic immunologic disease
Sickle cell nephropathy
Diabetic glomerulonephritis
160
158
156
140
123
110
104
75
47
46
44
40
32
14
9
35
45
47
18
48
55
40
51
53
59
41
58
13
57
33
58
62
78
28
82
73
77
79
81
72
83
54
62
0
33
5
3
24
4
63
6
15
4
9
7
7
8
6
29
33
1-9
NAPRTCS 2005
Transplant
100
80
60
40
20
0
0-1
EXHIBIT 1.7
PRIMARY DIAGNOSIS BY AGE
FSGS
GN
Other
Structural
2-5 6-12 >12
1-10
SECTION 2: DONOR HISTORY AND ANTIGEN MISMATCHES
NAPRTCS 2005
Transplant
As described in Exhibit 2.1, 48% of all transplants have involved a cadaver source, 42% came from a parent, with the remaining 10% coming from other living donors. Parents comprise 81% of living donors: a cross-classification of parent and child sexes (n=3,569 pairs with complete data) reveals that mothers comprise the majority of parent-donors (56%), fathers donate to sons 63% of the time, while mothers make 60% of their donation to sons (p=0.044). There have been 335 transplants between siblings, and 163 live-donor grafts have been from donors under the age of 21. Thirteen living donors were under 18 years of age: 12 were transplants between siblings and 1 was a transplant from parent to child. Between siblings, the numbers of 3-, 4-, 5-, and 6-antigen matches were 1, 2, 2, and 7, respectively. The number of unrelated living donors has increased from an average of 3 per year in 1987-1995 to 17 per year since then.
Among cadaver transplants, 67 (1.6%) have come from donors less than 24 months old and 1063
(23.9%) from donors who were between 2 and 12 years of age; the use of cadaver donors <10 years old has declined since the study’s start (see Exhibit 1.1). Prior to 1992, infant donors comprised 2.9% (42/1,466) of cadaver donor sources, compared to 0.9% (25/2,711) in transplants between 1991 and 2004. Thirteen percent of cadaver allografts were preserved by machine perfusion and 69% had cold ischemia times of 24 hours or less, with 17 (0.3%) exceeding 48 hours.
The maximum cold time was 64.5 hours.
Donor-specific transfusions were performed in 7% of living donor grafts but this procedure has been used only occasionally since 1995. The total number of random transfusions given to recipients differed by donor type: 48% of living donor graft recipients and 32% of cadaver graft recipients had zero previous transfusions, while 14% and 29%, respectively, had more than five transfusions. The percent of patients without prior random transfusions has increased from 17% in 1987 (27% living and 10% cadaver donor recipients) to 65% in 2004 (67% living and 62% cadaver). Time trends in the utilization of donor-specific and random transfusions are provided in Exhibit 2.2.
To date, there have been 34 confirmed transplants across ABO blood group compatibility barriers out of 8,564 transplants with complete blood group data; there are 25 O recipient/A donor pairs, 2 O recipient/B donor pair, 4 B recipient/A donor pairs, 1 B recipient/AB donor pair, and 2 A recipient/B donor pair. A special analysis of an early cohort of these patients concluded that pediatric kidney transplantation across ABO compatibility barriers is an uncommon practice, but suggested — based on preliminary experience — that such transplants involving recipients whose anti-A titer history is
2-1
NAPRTCS 2005
Transplant low (1:4) are associated with satisfactory graft outcome and are deserving of further study. Overall,
88% (7,501/8,564) of donor and recipient blood types were identical. Whereas blood group O is present in 56% of donors and 47% of recipients, blood group AB is present in 1.4% of donors and
4.0% of recipients.
Histocompatibility antigen data are shown in Exhibit 2.3. We count an allele as matching only if identical known alleles are reported for both donor and recipient. Among the living donor transplants, 76% had at least one match at each of the A, B, and DR loci, and there were mismatches at all 6 A, B, and DR loci for 13% of cases. No matches in either the B or DR loci occurred in 36% of the transplants from cadaver source donors; a single locus match (of B and DR) occurred in 32%. Known matches of all 6 A, B and DR alleles occurred in 2.5% of cadaver source transplants and in 3.5% of living donor source transplants.
Exhibit 2.4 compares donor sources with varying ages at transplant. Children under 5 years of age are more likely to receive a transplant from a living donor rather than a cadaver donor. For children ages 6-12, the proportion receiving living donor transplants is similar to the proportion receiving cadaver donor transplants. However, children ≥ 13 years of age are more likely to receive a cadaver donor transplant.
2-2
NAPRTCS 2005
Transplant
EXHIBIT 2.1
DONOR INFORMATION
N %
(9243) (100.0)
Donor Source
Live donor/other related
Cadaver
411 4.5
2-5 — 10.0
> 50
Cadaver Source Transplants
Machine Perfusion Used
Cold Ischemia Time
< 24 hours
> 24 hours
170 3.7
2-3
484
2809
1252
260 6.2
12.5
69.2
30.8
NAPRTCS 2005
Transplant
EXHIBIT 2.2
USE OVER TIME OF DONOR-SPECIFIC AND RANDOM BLOOD TRANSFUSIONS
100
80
Living Donor
0 Random transfusions
1-5 Random transfusions
>5 Random transfusions
Donor-specific transfusions
60
40
20
0
87
100
80
89 91 93 95 97
TRANSPLANT YEAR
99
Cadaver Donor
0 Random transfusions
1-5 Random transfusions
>5 Random transfusions
01 03
60
40
20
0
87 89 91 93 95 97
TRANSPLANT YEAR
99
2-4
01 03
HLA-A
EXHIBIT 2.3
PERCENT HLA MISMATCHES
Donor Source
Living
(n=4801)
Cadaver
(n=4427)
NAPRTCS 2005
Transplant
HLA-B
HLA-DR
HLA-B and -DR
HLA-A, -B, and -DR
2-5
NAPRTCS 2005
Transplant
EXHIBIT 2.4
AGE AT TRANSPLANT AND DONOR SOURCE
30
20
10
50
40
0
0-1 2-5 6-12 13-17 > 17
AGE (years)
Living Donor
Cadaver Donor
2-6
NAPRTCS 2005
Transplant
SECTION 3: THERAPY
The NAPRTCS collects information on post-transplant immunosuppressive medications and dosages at Day 30, Month 6, and every six months thereafter. In addition, a record of the date of initiation and dosages of immunosuppressive medication used during the first post-transplant month is collected. Detailed description of pre-operative immunosuppressive therapy is not collected, but it was employed in 50% of living donor transplants. The frequency of use among all recipients had decreased from 48% in 2001 to 40% in 2004.
Because of the changes in therapy in recent years, analyses are restricted to more recent transplant (>1995). Exhibit 3.1 details immunosuppressive medication data for transplants in 1996 and beyond for the first 30 days post-transplant therapy. Note that the frequency of use of various drugs ranges from 9% (of transplants) for sirolimus to 91% for prednisone. Methylprednisolone and azathioprine, when used, were typically initiated on the day of operation. Polyclonal antibody ATG was used in 16% of living donor and 25% of cadaver source transplants, while the respective rates of monoclonal antibody usage are 40% and 45%. Cyclosporine was used for 63% of transplants and, of those, 21% began cyclosporine on Day 0, 24% on Day 1, and 40% during Days 2-6.
Although early graft failures decrease the number of patients still available for immunosuppressive therapy by Day 30, the percentages being treated with prednisone is relatively stable. Over the month, median doses of prednisone decreased to approximately 1/3 of the initial amount and, median doses of cyclosporine increased by 1.0 mg/kg. The median ATG/ALG course was 7 days.
For monoclonal antibody, the median length of course of OKT3 was 9 days; for basiliximab patients, it was 2 days; and for daclizumab recipients, the median course was 5 days.
Exhibit 3.2 shows the percentage of week 1 calcineurin inhibitor use by type of induction antibody while Exhibit 3.3 presents the induction antibody use from 1996 to 2004. The rate of induction antibody use at transplant or one day post transplant, by transplantation year was as follows:
3-1
NAPRTCS 2005
Transplant
PERCENT INDUCTION ANTIBODY, AT TRANSPLANT OR ON 1 DAY POST TRANSPLANT
(n=585) (n=568) (n=510)
1999
(n=513)
2000
(n=419)
2001
(n=451)
2002
(n=397)
2003
(n=284)
2004
(n=142)
None 49.8 51.9 42.5 41.7 48.5 45.3 41.9 39.2 44.8
OKT3 22.0 10.2 5.1 0.5 0.9 1.0 0.7 0
Basiliximab — 0.7 4.7 16.1 23.9 31.7 34.2 31.8 30.8
Daclizumab — 5.0 18.9 26.1 21.5 16.7 16.5 18.0 17.5
ATG/ALG 28.1 27.7 23.8 11.1 5.6 5.4 6.5 10.3 7.0
Exhibit 3.4 presents immunosuppressive therapy dosages for patients with functioning grafts for selected drug combinations after 1995. Median daily prednisone doses decrease over the first 2 years after transplantation, while the percentage of transplanted patients receiving alternate day therapy increases from 6.1% at Month 6 to 13.6%, 25.9%, and 33.0% at Months 12, 24, and 48, respectively. Continued slow increases in alternate day steroid use are observed at 6 years (40%).
At 5 years post transplant, 32.7% of living donor versus 40.2% of cadaver donor transplants are reported to receive alternate day steroids. Note that there is little change in the proportion of patients receiving prednisone, cyclosporine, and azathioprine at each time point. Among those receiving cyclosporine, the mean and standard error of the daily milligram per kilogram doses are
7.7±0.09, 6.9±0.09, 6.0±0.08, and 4.6±0.12 at Months 6, 12, 24, and 60, respectively.
Exhibit 3.5 shows the marked changes in day 30 post transplant dosing strategies that have been observed in the past years. These are substantially caused by the introduction of new drugs such as mycophenolate mofetil and tacrolimus. Although it has substantially effected the later cohort years, the whole experience of the registry has been minimally affected. Use at Day 30 of combination cyclosporine, prednisone, and azathioprine has declined since 1996-1997, from 30% of living donor and 27% of cadaver organ recipients, to 2% and 1% of transplants, respectively, in
2000-2004. The regimen of prednisone, tacrolimus, and mycophenolate mofetil has become more popular. It is used in 39% of living donor and 43% of cadaver organ transplant in 2000-2004, compared to about 9.5% of all transplants in 1996-1997.
3-2
NAPRTCS 2005
Transplant
Approximately 80% of patients receive 3-drug therapy at 6 months post transplant with mycophenolate mofetil replacing azathioprine in recent cohorts. Among transplanted grafts with
≥ 30 days function that have occurred since 1996, the following drug utilization rates were observed:
PERCENT DRUG UTILIZATION - DAY 30 POST TRANSPLANT
(n=568) (n=510) (n=513)
2000
(n=419)
2001
(n=451)
2002
(n=397)
2003
(n=284)
2004
(n=142)
Cyclosporine 80.5 73.9 70.2 58.0 49.5 29.2 15.9 7.0
Tacrolimus 15.0 22.9 24.8 34.8 42.6 58.4 62.0 72.5
Mycophenolate 45.3 68.4 70.0 64.7 54.8 57.4 53.9 60.6
Azathioprine 35.4 20.6 16.2 14.1 13.3 1.8 4.9 2.8
Sirolimus — — 0.2 6.2 16.6 22.2 21.8 11.3
Substantial increases in tacrolimus, mycophenolate mofetil, and sirolimus usage are observed, with a significant decrease in azathioprine usage. Azathioprine usage has decreased sharply from 60% in 1996 to 3% in 2004. The majority of sirolimus therapy (87%) was initiated within the first two days post-transplant. The mean and median dosages were 4.7 and 4.0 mg/m 2 , respectively.
Cyclosporine was used in 82% of the 1996 transplants at Day 30, and it continues to show a decline in utilization. Of cyclosporine recipients since 1996 with known formulation, 84% reported use of Neoral.
Exhibit 3.6 displays the percentage of patients at selected follow-up time points who were receiving the six most common maintenance regiments since 1995, by graft donor source. Through 3 years, about 35% of the patients received combination immunosuppressives with prednisone, cyclosporine, and MMF, compared to approximately 22% of patients with prednisone, cyclosporine and azathioprine. Note that therapy strategies appear similar for cadaver recipients and live donor recipients. For example, dual therapy with prednisone and cyclosporine or prednisone and tacrolimus is received by similar percentages of recipients from living and cadaver graft donors.
Because of the differential graft survival in black and non-black patients, cyclosporine blood levels have been examined. At Day 30 mean median values are within 9 ng/mL for two of the most common measurement methods, HPLC and TDX. For black patients, at 1-year post transplant,
3-3
NAPRTCS 2005
Transplant mean cyclosporine level was 183 ng/mL (versus 168 ng/mL for others); cyclosporine blood levels are shown in the table below.
MEDIAN / MEAN ± SE ONE YEAR BLOOD LEVELS (NG/ML)
BY RACE/ETHNICITY
Cyclosporine
Monoclonal RIA-specific 156/189±9.4 155/169±3.2
TAC
The percentage of patients receiving concomitant anti-hypertensive, prophylactic antibiotic, and anti-convulsant medications, by donor source, are displayed in Exhibit 3.7. A substantial percentage of transplanted children receive anti-hypertensives and antibiotics throughout the followup period. During the first 3 years, an absolute difference in anti-hypertensive medication usage of about 5 percentage points is observed between cadaver and living donor source recipients.
Although the percentage receiving such therapy decreases in the first few years of follow-up, over half of the children are receiving anti-hypertensives throughout the period. Prophylactic antibiotic use decreases for both donor source groups during the first 12 months after transplant. At one year, prophylactic antibiotics are used in 49% of living donor and 44% of cadaver donor source recipients with minimal decreases thereafter. At one year, prophylactic antibiotics are used in 37% of hemolytic uremic syndrome patients and in 37% of those with focal segmental glomerulosclerosis, versus 55% of patients diagnosed with reflux nephropathy and 61% with obstructive uropathy. An anti-convulsant medication was given initially to 7% of the transplant recipients, with a greater frequency observed among recipients of cadaver organs (9.0% vs. 6.0%).
3-4
NAPRTCS 2005
Transplant
EXHIBIT 3.1
MEDICATION DATA - FIRST 30 DAYS
TRANSPLANTS AFTER 1995
Therapy
Percent
Treated
(n=4010)
Median
Day of
Initiation
Median
Initial
Dose
(mg/kg/D)
Percent
Treated
Day 30
(n=3869)
Median
Day 30
Dose
(mg/kg/D)
Prednisone 91 1.7
Methylprednisolone 80 0 8.5 — —
Tacrolimus 32
2.4 2.03
1 0.19 31 0.22
Mycophenolate 1 29.2 52 30.3
ATG/ALG
Monoclonal 34 0 — — —
OKT3
Basiliximab
Daclizumab
Sirolimus**
*Median initial and Day 30 daily dose in mg per body surface area were 897.0 and 949.5 mg/m 2 /Day respectively.
**Median initial dose in mg per body surface area was 3.1 mg/m 2 .
3-5
NAPRTCS 2005
Transplant
EXHIBIT 3.2
WEEK 1 CALCINEURIN INHIBITOR USE, BY INDUCTION ANTIBODY
100
80
Neither
Cyclosporine
Tacrolimus
60
40
20
100
80
None
OKT3
Basiliximab
Daclizumab
ATG/ALG
60
0
None OKT3 Basiliximab Daclizumab ATG/ALG
EXHIBIT 3.3
INDUCTION ANTIBODY USE, BY YEAR
40
20
0
1996 1997 1998 1999 2000 2001 2002 2003 2004
TRANSPLANT YEAR
3-6
0.3
NAPRTCS 2005
Transplant
EXHIBIT 3.4
MEAN (SE) DAILY DRUG DOSAGES
BY DRUG COMBINATION AND YEAR POST-TRANSPLANT
Prednisone Cyclosporine
10
Pred/Cya/Aza
Pred/Cya/MMF
Pred/Tac/MMF
Cya/Pred
Cya/Pred/Aza
Cya/Pred/MMF
8
0.2
6
0.1
0
0.30
1 2
YEAR
Tacrolimus
3
Tac/Pred
Tac/Pred/Aza
Tac/Pred/MMF
4
4
0 1 2
YEAR
3 4
Mycophenolate Mofetil
1400.0
MMF/Pred/Tac
MMF/Pred/Cya
0.25
1200.0
0.20
1000.0
0.15
0.10
0 1 2
YEAR
3 4
3-7
800.0
0 1 2
YEAR
3 4
NAPRTCS 2005
Transplant
EXHIBIT 3.5
PERCENT OF PATIENTS WITH FUNCTIONING GRAFTS RECEIVING
IMMUNOSUPPRESSIVE MEDICATION 30 DAYS POST TRANSPLANT
BY YEAR OF TRANSPLANT
20%
13%
31%
2%
6%
30%
20%
15%
9%
LD
13%
8%
9%
4%
6%
36% 28%
11%
39%
DRUG OTHER
PRED+CYA+MMF
PRED+CYA
PRED+TAC
PRED+CYA+AZA
PRED+TAC+MMF
17%
1%
7%
18%
27%
7%
10%
12%
10%
8%
13%
38%
CAD
36%
10%
5%
26%
11%
43%
DRUG OTHER
PRED+CYA+MMF
PRED+CYA
PRED+TAC
3-8
PRED+CYA+AZA
PRED+TAC+MMF
NAPRTCS 2005
Transplant
EXHIBIT 3.6
PERCENTAGE OF PATIENTS RECEIVING DESIGNATED MAINTENANCE
IMMUNOSUPPRESSION REGIMENS, BY DONOR SOURCE AND TIME OF FOLLOW-UP
Living Donor Cadaver Donor
18% 4%
33%
33%
33%
18%
19%
5%
6%
9%
12%
13%
LD
10%
23%
21%
21%
11%
11%
Living Donor
32%
32%
5%
17%
18%
6%
18% 5%
14%
13%
15%
33%
LD
11%
20%
20%
21%
11%
10%
15% 4%
36%
38%
38%
14%
15%
5%
7%
8%
11%
12%
CAD
23%
9%
24%
22%
8%
9%
Cadaver Donor
33%
34%
14% 5%
13% 5%
14% 5%
13%
14%
14%
35%
CAD
9%
24%
24%
25%
9%
8%
3-9
NAPRTCS 2005
Transplant
EXHIBIT 3.7
PERCENTAGE OF PATIENTS RECEIVING CONCOMITANT MEDICATIONS,
BY DONOR SOURCE AND TIME POST-TRANSPLANTATION
100
80
Anticonvulsant-LD
Anticonvulsant-CAD
Antihypertensive-LD
Antihypertensive-CAD
Proph Antibiotic-LD
Proph Antibiotic-CAD
60
40
20
0
0 1 2
YEARS
3 4
3-10
NAPRTCS 2005
Transplant
SECTION 4: REJECTION
In NAPRTCS, a rejection episode is defined by the physician’s decision to initiate specific antirejection therapy. For time to event analyses, a rejection episode is also considered to have occurred if rejection is the reported cause of graft failure even in the absence of an acute rejection report and 149 episodes were included as such. As a result, a total of 9,350 episodes of rejection, were available for analysis, as described below.
There were 9,201 acute rejection reports submitted for 9,243 transplants. Further, although no acute rejection reports were submitted, 28 grafts were reported to have failed due to hyperacute, accelerated acute, or acute rejection, and 121 grafts were reported to have failed due to chronic rejection. Acute rejection reversal outcome had not been established for 21 of the 9,201 acute rejection reports at the time of database closure.
The frequency of reported acute rejections is presented in Exhibit 4.1A, indicating that of the 9,243 transplants, no acute rejections were reported for 4,633, exactly one rejection was reported for
2,343, two rejections for 1,102, three rejections for 592, and four or more rejections were reported for 573 transplants. Acute rejection ratios (number of rejections/number of transplants) are shown in Exhibit 4.1B. On average, 0.83 acute rejections were reported for each living donor transplant, and 1.19 rejections for each cadaver donor transplant. Age-specific ratios vary from 0.48 to 0.84 for living donor transplants, and from 0.85 to 1.25 for cadaver donor transplants.
Exhibit 4.2 displays the cumulative distribution of times to first rejection by allograft source and entry cohort. Improvements in rejection experience have occurred over the life of the registry. These changes have been substantial throughout the life of the project. The table below presents 12month probabilities of acute rejection by transplant year. While historically over half of cadaver organ recipients experienced a rejection in the first post transplant weeks, the majority of patients now experience an acute rejection free course.
4-1
NAPRTCS 2005
Transplant
12-MONTH PROBABILITY (%) OF FIRST REJECTION, BY TRANSPLANT YEAR
Transplant
Year
Living Donor Cadaver Donor
% SE % SE
1987-1990 54.2 1.7 69.1 1.5
1991-1994 45.0 1.5 60.8 1.6
1995-1998 33.7 1.4 41.0 1.7
1999-2002 23.2 1.4 27.8 1.9
2003-2004 15.8 3.4 20.9 4.8
Donor source-specific analyses were performed to assess the influence of selected patient and transplant characteristics on the occurrence of first rejection episodes. These analyses were restricted to transplants occurring after 1996 and to the first transplant reported for a patient, and only included transplants beyond 1996. Relative hazards (RH) of first rejection episode by cohort era are presented in Exhibits 4.3A and 4.3B. For living donor transplantation, the incidence of first rejection was increased for black patients, for patients with one or two HLA-DR mismatches, and for patients who did not receive antibody prophylaxis on post transplant days 0 or 1. Because of its importance the analysis was adjusted with a linear term for transplant year. No significant effects were observed for transfusion history, donor-specific transfusions or the use of pre-operative immunotherapy. There is an approximate 29% reduction in the hazard of rejection with each successive grouping of transplantation years (p<0.001). The importance of acute tubular necrosis
(ATN) on subsequent acute rejection was evaluated by restricting the analysis to cases with more than 7 days of graft function. Patients with first week dialysis, the operational definition of ATN, were at a significantly increased risk of subsequent acute rejection (RH=1.61, p<0.001).
For cadaver donor transplantation, black patients had 27% higher risk of first acute rejection
(RH=1.27, p<0.001) than non-black patients. Additional risk factors include two HLA-DR mismatches compared to no mismatches (RH=1.29, p=0.002). The effect of transfusion history and cold storage time are not significant when adjusted for the other predictors in the model. The effect of transplant year for the cadaver donor model is similar to that for living donor transplantation.
There is an absolute difference equal to 3% between cadaver donor recipients and living donor recipients.
4-2
NAPRTCS 2005
Transplant
Cumulative rejection distribution estimates are shown in Exhibit 4.4 for selected patient transplant characteristics. Exhibit 4.5A presents the complete (i.e., return to baseline serum creatinine) and partial (i.e., graft function without return to baseline creatinine) reversal rates for each of the treated rejections, by donor source. Among living donor (LD) graft recipients, 53% had a complete reversal of rejection, 43% had a partial reversal, and 4% ended in graft failure or patient death. A poorer prognosis is observed for cadaver donor (CD) graft recipients, where 47% of rejection episodes were completely reversed, 47% partially reversed, and 6% ended with graft failure or patient death.
The percentage of complete recoveries from acute rejection decreases substantially with increasing number of episodes, averaging 61% and 56%, respectively, for LD and CD sources following the first acute rejection, but only about 43% and 35%, respectively, following the third episode. When stratified by age, young transplant recipients are observed to have more severe outcomes from acute rejection, particularly among cadaver donor transplants: 5% of acute rejections among infants with a LD source resulted in graft failure or patient death, compared to rates of 3% to 4% for older children (p=.0120). For infants with a CD source, 11% of acute rejections resulted in graft failure or death, compared to rates of 6% for the older children (p<0.001).
When this analysis was restricted to the first episode of acute rejection (Exhibit 4.5B), the outcome for infants was particularly poor: 10% of LD (p=0.013) and 18% of CD (p=0.009) rejections resulted in graft failure or death. Non-biopsied rejections had slightly higher reversal rates than biopsied rejections, suggesting an association between the severity of the rejection episode and the decision to biopsy. Treatment with antibody at the time of transplant did not by itself appear to negatively influence the probability of completely reversing later rejections. Polyclonal or monoclonal antibodies were used in the treatment of 2,251 (37%) first acute rejection episodes.
Exhibit 4.6 provides information on rejection reversal rates, by transplant year. Despite the decreasing rejection frequency, complete reversal rates appear to be improving (with offsetting decrease in partial reversal rates) for living donor transplant in the latter cohort years.
Rejection history was examined for patients who were rejection-free for a minimum of 365 days post-transplantation and for whom 12-month follow-up data were available. Of the 3,574 patients satisfying these criteria, 768 (22%) subsequently experienced an acute rejection episode (defined here as a late first rejection). Exhibit 4.7 presents rejection rates by selected characteristics for this cohort. There were 314 (41%) complete reversals, 411 (54%) partial reversals, and 36 (5%) graft failures and two patient deaths as a result of the rejection episodes. Interestingly, the mean 1-year daily cyclosporine doses for the respective reversal groups were 6.7, 5.9, and 4.7 mg/kg.
4-3
NAPRTCS 2005
Transplant
EXHIBIT 4.1A
FREQUENCY OF ACUTE REJECTIONS
N % N % N %
All Transplants
Number of Acute Rejections
9243 100.0
4801 100.0
4427 100.0
0 4633 100.0
2688 56.0
1930
1 2343 100.0
1125 23.4
1218
2 1102 100.0
534 11.1
568
3 592 100.0
233 4.9
359
≥ 4 4.6
352 8.0
573 100.0
221
EXHIBIT 4.1B
ACUTE REJECTION RATIOS
Living Cadaver
No. of
Transplants
No. of
Rejections
Rejection
Ratio
No. of
Transplants
No. of
Rejections
Rejection
Ratio
Recipient age
4-4
80
60
0
0
100
40
20
0
0
NAPRTCS 2005
Transplant
EXHIBIT 4.2
TIME TO FIRST REJECTION EPISODE, BY ALLOGRAFT SOURCE
AND TRANSPLANT YEAR
100
LIVING DONOR
80
60
40
20
12 24
MONTHS
CADAVER DONOR
36
1987-1990
1991-1994
1995-1998
1999-2002
2003-2004
48
12 24
MONTHS
4-5
36
1987-1990
1991-1994
1995-1998
1999-2002
2003-2004
48
NAPRTCS 2005
Transplant
Characteristic
EXHIBIT 4.3A
RELATIVE HAZARD (RH) OF FIRST REJECTION EPISODE
FIRST TRANSPLANT, 1987 - 1995
Living Donor Cadaver Donor
RH P-value RH P-value
Recipient Race (Black vs. Non-Black) 1.32 <0.001 1.23 <0.001
Recipient Age (<24 months)
One mismatch vs. zero
Two mismatches vs. zero
No Induction Therapy
Prior Random Transfusions
1-5 vs. none
>5 vs. none
Donor Specific Transfusions
Pre-Op Immunotherapy
Cold Storage Time >24 hrs.
0.73 0.005 1.13 0.427
1.60
1.44
1.27
<0.001
<0.001
<0.001
1.14
1.33
1.24
0.147
0.001
<0.001
0.94
1.09
0.94
0.96
0.271
0.274
0.471
0.455
0.93
1.02
−
−
−
−
0.298
0.828
− − 1.02 0.686
0.82 <0.001 0.77 <0.001
4-6
NAPRTCS 2005
Transplant
Characteristic
EXHIBIT 4.3B
RELATIVE HAZARD (RH) OF FIRST REJECTION EPISODE
FIRST TRANSPLANT, 1996 - 2004
Living Donor Cadaver Donor
RH P-value RH P-value
Recipient Race (Black vs. Non-Black) 0.92 0.536 1.31 0.015
Recipient Age (<24 months)
One mismatch vs. zero
Two mismatches vs. zero
No Induction Therapy
Prior Random Transfusions
1-5 vs. none
>5 vs. none
Donor Specific Transfusions
Pre-Op Immunotherapy
Cold Storage Time >24 hrs.
0.56 0.003 0.63 0.356
1.17
0.95
1.19
0.219
0.7050
0.040
1.22
1.24
0.87
0.292
0.253
0.184
1.03
1.02
0.50
1.09
0.721
0.896
0.172
0.321
0.97
0.96
−
−
−
−
0.754
0.802
1.24 0.122
Transplant Year
−
0.68
−
<0.001 0.74 0.003
4-7
NAPRTCS 2005
Transplant
EXHIBIT 4.4
100
TIME TO FIRST REJECTION EPISODE, BY SELECTED CHARACTERISTICS
LIVING DONOR GRAFTS CADAVER DONOR GRAFTS
Recipient Age
100
Recipient Age
80 80
60 60
40
20
0
0
60
40
40
20
100
0
0 12 24
MONTHS
36
HLA-DR Mismatches
80
0-4
2-5
6-12
>12
48
20
0
0
100
12 24
MONTHS
36
Induction Antibody
Administration
0 Mismatches
1 Mismatch
2 Mismatches
48
80
60
12 24
MONTHS
36
No
Yes
48
4-8
60
40
40
20
0
0
100
12 24
MONTHS
36
HLA-DR Mismatches
80
0-1
2-5
6-12
>12
48
20
0
0
100
12 24
MONTHS
36
Induction Antibody
Administration
0 Mismatches
1 Mismatch
2 Mismatches
48
80
60
40
20
0
0 12 24
MONTHS
36
No
Yes
48
40
20
0
0
100
80
60
40
20
0
0
60
40
20
0
0
100
80
60
NAPRTCS 2005
Transplant
EXHIBIT 4.4 (Continued)
100
TIME TO FIRST REJECTION EPISODE, BY SELECTED CHARACTERISTICS
LIVING DONOR GRAFTS CADAVER DONOR GRAFTS
Recipient Race
100
Recipient Race
80 80
12
12
24
MONTHS
ATN
24
MONTHS
Prior Random
Transfusion
36
36
White
Black
Hispanic
48
No ATN
ATN
48
12 24
MONTHS
36
None
1-5
>5
48
4-9
40
20
0
0
100
80
60
40
20
0
0
60
40
20
0
0
100
80
60
12
12
24
MONTHS
ATN
24
MONTHS
Prior Random
Transfusion
12 24
MONTHS
36
36
White
Black
Hispanic
48
No ATN
ATN
48
36
None
1-5
>5
48
NAPRTCS 2005
Transplant
EXHIBIT 4.5A
REJECTION REVERSAL OUTCOME BY SELECTED CHARACTERISTICS
Living Donors Cadaver Donors
No. of
Rejections
%
Complete
%
Partial
% Graft
Failure
/Death
No. of
Rejections
%
Complete
%
Partial
% Graft
Failure
/Death
Total Rejection
Episodes
Rejection
1
2
3
>4
0-1
2-5
6-12
>12
Biopsy
No
Yes-needle
Yes-tissue
DR Antigen Mismatch
0
1
2
ATG/ALG/OKT3
No
Yes
4-10
NAPRTCS 2005
Transplant
EXHIBIT 4.5B
REJECTION REVERSAL OUTCOME BY SELECTED CHARACTERISTICS
FOR FIRST ACUTE REJECTION EPISODE ONLY
Living Donors
No. of
Rejections
%
Complete
%
Partial
Cadaver Donors
% Graft
Failure
/Death
No. of %
Rejections Complete
%
Partial
% Graft
Failure
/Death
First Rejection Episodes 2107 61 34 5 2486 56 36 8
Recipient Age
0-1
2-5
114
327
67 24
67 28
10 61 61 21
6 327 64 25
18
11
6-12
>12
Biopsy
No
749
917
754
61 34
58 38
70 27
5 889 55 36
4 1209 53 40
3 941 61 33 6
9
7
Yes-needle
Yes-tissue
DR Antigen Mismatch
0
1
2
ATG/ALG/OKT3
No
Yes
639
695
266
1470
371
1281
826
57 40
56 39
59 37
63 33
55 39
62 33
59 37
4 623 51 42
5 880 56 36
4 248 60 33
4 1038 56 37 7
6 1200 54 36 10
5 1061 57 34 9
4 1425 55 37 8
7
7
8
4-11
NAPRTCS 2005
Transplant
EXHIBIT 4.6
REJECTION REVERSAL OUTCOME BY TRANSPLANT YEAR
100 LIVING DONOR
Complete
Partial
Graft failure/Death
80
60
40
20
0
1987
100
1991 1995
TRANSPLANT YEAR
1999
CADAVER DONOR
Complete
Partial
Graft failure/Death
80
60
40
20
0
1987 1991 1995
TRANSPLANT YEAR
1999
4-12
2003
2003
NAPRTCS 2005
Transplant
EXHIBIT 4.7
SUMMARY OF LATE FIRST REJECTIONS, BY SELECTED CHARACTERISTICS
N
No. of
Rejections
Percent
Rejections
Donor
Living Donors
Cadaver Donors
Age
2119
1455
403
365
19.0
25.1
> 12
Sex
1538 328 21.3
Race
4-13
NAPRTCS 2005
Transplant
SECTION 5: GRAFT FUNCTION
A total of 2,414 graft failures among 9,243 (26.1%) transplants have occurred. This includes
291 patients who have lost 2 or more grafts since the study's start, of which 27 subjects had 3 graft failures and 2 had 4 graft failures. Of index transplants, 2,123 of 8,435 (25.2%) transplants have failed, while 291 of 808 (36%) subsequent transplants have failed. Of these 2,414 failures,
1,809 (75%) were returned to dialysis, and 156 (6%) were re-transplanted at the time of failure, and 221 (9%) were deaths with functioning graft. Exhibit 5.1 provides the distribution of graft failure causes. Note that tissue confirmation of cause was obtained in 1,341 (56%) failures. Of the index graft failures occurring since January 1, 2000, chronic rejection accounted for 47.9%
(183/382) while 29 (8%) acute rejection graft failures, 32 (8.4%) cases of medication discontinuation, 36 (9.2%) graft thrombosis, 40 (10.5%) disease recurrences, and 51 (26.4%) deaths with functioning graft were reported as graft failure cause during this period. With increased length of follow-up of the study cohort, chronic rejection continues to be the most common cause of graft failure. Overall, 49% of the graft failures are caused by rejection, with chronic rejection accounting for 34% and acute rejection accounting for 13% of the failures.
Recurrence of original disease as a cause of graft failure has been observed 166 times as follows: focal segmental glomerulosclerosis (74), membranoproliferative glomerulonephritis
Type II (14), oxalosis (10), hemolytic uremic syndrome (16), chronic glomerulonephritis (7), others (45). Vascular thrombosis remains a major cause of failure; 342 graft failures are attributed to primary non-function, vascular thrombosis, or miscellaneous technical causes, suggesting that such problems will occur in 3.7% of pediatric transplants. Renal artery stenosis as a cause of graft failure is observed in 1 living donor versus 14 cadaver source transplants.
Chronic rejection causes graft failure in 6.5% of living donor versus 11% of cadaver source transplants and respective failure rates due to primary non-function are 0.3% versus 0.9% while those for thrombosis are 2.0% versus 3.7%.
Because of the clinical and statistical significance of donor source, graft failure distributions are presented separately for living and cadaver donor transplants. Survival distribution estimates for the index transplants are presented in Exhibit 5.2 by donor source and transplant era.
Overall, the mean and median follow-up for subjects with functioning grafts is 52 and 43 months. Estimated graft survival probabilities and standard errors are 92.9%±0.39%,
87.0%±0.54% and 81.4%±0.69% at Years 1, 3 and 5 post-transplant, respectively, for recipients of living donor organs. Corresponding estimates for recipients of cadaver source organs are
84.9%±0.59%, 74.8%±0.76% and 66.6%±0.90%. Notice from the exhibit, that more recent
5-1
NAPRTCS 2005
Transplant cadaver source transplants have a graft survival experience very similar to that of living donor transplant from the earlier (1987-1994) era. In fact, the graft survival in 1995-2004 is significantly better than in prior years for both cadaver source (p<0.001) and living donor grafts
(p<0.001). Exhibit 5.3 displays graft failure information by transplant source and selected transplant characteristics (the percentage of grafts in the subgroup, the percentage of failures, the product limit estimate of 5-year graft survival probability and associated standard error are provided). Exhibits 5.4-5.8 provide graft survival distributions for selected donor and recipient characteristics.
The table below shows the relative hazard (RH) of individual prognostic factors in the presence of other factors in multivariate proportional hazards models.
Living Donor Cadaver Donor
RH (P-Value) RH (P-Value)
Recipient Age (>2 vs. 0-1) 1.12 (NS) 0.56 (<0.001)
1.46 (0.002) 1.43 (<0.001)
No Induction Antibody Administration 1.19 (0.013) 1.11
>5 Lifetime Transfusions 1.31 (0.003) 1.31
(NS)
(<0.001)
No HLA-DR Matches
1.40 (0.010) 1.18 (0.009)
0.84 (NS) 1.17 (0.009)
1.87 (<0.001) 1.54 (<0.001)
1.12 (NS) 1.23 (0.029) Prior Dialysis*
Cold Storage Time >24 Hours — — 1.17 (0.013)
0.95 (<0.001) 0.94 (<0.001)
Native Nephrectomy (No)
Gender (Male)
0.86 (0.054) 0.98
0.89 (NS)
*Reported as having had dialysis within 2 weeks of transplant.
(NS)
0.86 (0.014)
For recipients of living donor grafts, the most influential prognostic variables (of index transplant graft survival) are race (black vs. non-black; RH=1.9, p<0.001), having had a prior transplant
(RH=1.5, p=0.002), having had greater than 5 lifetime transfusions (RH=1.3, p=0.003), not having had induction antibody (RH=1.2, p=0.002), no HLA-B matches (RH=1.4, p=0.010), and not having a native nephrectomy (RH=0.81, p=0.007). A linear trend in improvement in graft retention with later year of entry is also observed (RH=0.95 per year p<0.001). With increased follow-up, the graft survival disadvantage associated with very young recipients has diminished.
5-2
NAPRTCS 2005
Transplant
For recipients of cadaveric source organs, review of Exhibit 5.3 indicates multiple variables that are important prognostic factors of graft survival. Exhibit 5.5 shows the survival distribution estimates for some of these variables. Proportional hazards models have been fit which suggest that transplant year, race, and recipient age are simultaneous significant contributors to the risk of graft failure. Prior transplant and prior transfusion history also contribute significantly to a patient's prognosis after adjustment for the variables noted.
The model includes a linear term for year of transplant, whose estimated relative risk increase implies a decreasing hazard (RH=0.94 per year p<0.001). Note that interpretation of the use of antibody is hampered by selection factors that motivate its usage; the size and direction of these biases cannot be quantified and the evaluation of this factor cannot be considered definitive.
Plots of graft survival distributions for annual cohort groups are included in Exhibit 5.6. Marked improvement in cadaver graft survival is observed over time. The following table displays 1year graft survival percentages for the 4-year cohorts. (Standard errors range from 0.7% to
1.0% for living donor, and from 1.0% to 1.3% for cadaver source grafts.) These results may be related to temporal trends in immunosuppressive drugs and dosages, decreased transfusion requirements, and decreased use of young cadaver donors.
PERCENT ONE YEAR GRAFT SURVIVAL
BY DONOR SOURCE AND ANNUAL COHORT GROUPS
1987 – 1990
1991 – 1994
89.4%
91.8%
75.2%
85.0%
1995 – 1998
1999 – 2004
93.9%
95.7%
90.4%
93.2%
Exhibit 5.8 displays graft survival distribution estimates for selected primary diagnosis groupings. Among recipients of living donor kidneys, after adjustment for other risk factors, graft survival of patients diagnosed with focal segmental glomerulosclerosis (FSGS) and other causes (not graphed, but includes, oxalosis, sickle cell anemia, Drash syndrome, and other/unknown) was significantly less than that for patients with congenital/structural diagnoses.
Cadaver donor kidney recipients with FSGS or congenital nephrotic syndrome had decreased graft survival relative to the congenital/structural group.
5-3
NAPRTCS 2005
Transplant
Acute tubular necrosis (ATN) is defined by the cooperative study as the use of dialysis in the transplant week. This delay in graft function is reported for 5.0% of index living donor transplants which is significantly less than the ATN rate reported for cadaver source transplants
(17.1%). Among the living donor transplants, subjects with >5 prior transfusions (11.4%), prior transplants (8.8%), native nephrectomy (7.2%), and black race (7.8%), had significantly higher rates of ATN.
For transplants with cadaver organs, the ATN rate is 17.1%. This rate varies significantly with several factors:
#
#
#
#
# black recipients (23.8%) cold ischemia times >24 hours (25.2%)
>5 transfusions (27.8%) prior transplant (26.2%) native nephrectomy (24.0%)
Note that donor and recipient ages were not consistently predictive of ATN risk among cadavers. The ATN rate differs for Collins iced electrolyte solution (22.8%) versus Wisconsin solution (18.0%).
In a logistic regression analysis, the following variables were significantly predictive of ATN risk in cadaver graft recipients: prior dialysis, race, cold time, number of prior transfusions, native nephrectomy, and induction antibody administration. Moreover, the cohort year linear effect is significant (p=0.016) after adjustment for other prognostic variables.
Subjects who received cyclosporine on transplant day 0 had ATN rates of 3.8% and 17.2% for living and cadaver source transplants, respectively.
Graft survival after the first week is displayed in Exhibit 5.9, and is significantly worse in the presence of acute tubular necrosis in both donor source groups. In the living donor group, black race (RH=2.0), >5 transfusions (RH=1.3), HLA-B disparity (RH=1.4), transplant year, and ATN
(RH=2.4) are associated with simultaneous significant increased risk of post-week graft failure.
Among functioning cadaver grafts at 1 week, 72% of subjects without first week dialysis are estimated to be functioning at 5 years as opposed to 54% of those with ATN. For cadaver
5-4
NAPRTCS 2005
Transplant grafts, after one week, the variates that maintain predictive capability include the following: donor, age, race, prior transplant, prior dialysis, transplant year, and the number of prior transfusions. Cold storage time is not predictive (p=0.5) after adjustment for first week results.
Serum Creatinine and Creatinine Clearance
Exhibits 5.10 and 5.11 display the means and standard errors of serial serum creatinine and creatinine clearance measurements. At each time point only individuals with functioning grafts are included.
Creatinine clearance (mL/min/1.73 m 2 ) values were calculated using the Schwartz formula and available morphologic data, with length replacing height in younger recipients, as follows:
CrCI=
[.45 x height (cm)] serum creatinine
[.55 x height (cm)] serum creatinine
[1.55 x age (years) + .5 x height (cm)] serum creatinine weight < 10 kg
10 kg < weight < 70 kg weight > 70 kg
From Exhibit 5.10, decreases in clearance are observed in living donor recipients over the first 4 years post transplantation. Younger recipients begin with higher calculated clearances that are subject to greater absolute declines, while the oldest subjects behave similarly to adult populations. Likewise, decreases in creatinine clearance appear lower in cadaver organ recipients, while clearance values for both organ source groups approach equivalence in the later years.
In Exhibits 5.12 - 5.14, graft survival percentage and mean calculated clearance values for subjects with functional grafts are plotted at each annual follow-up visit for various groups, including donor source, race and early anti-lymphocyte therapy use. Continued decreases in both graft survival and graft function are seen through the first five post-transplant years.
5-5
NAPRTCS 2005
Transplant
The impact of race on calculated clearance and graft survival is observed in Exhibit 5.14. Note that despite the relatively greater number of graft failures in black recipients, there is no trend towards convergence in serum creatinine values and black recipients have both lower graft survival and clearance values throughout.
5-6
NAPRTCS 2005
Transplant
EXHIBIT 5.1
CAUSES OF GRAFT FAILURE
Index Graft
Failures
Subsequent
Graft Failures
All Graft
Failures
N % N % N %
Total
Death with functioning graft
Primary non-function
Vascular thrombosis
Other technical
Hyper-acute rejection
2123 100 291 100 2414 100
199 9.4 22 7.6 221 9.2
52 2.5 2 0.7 54 2.2
220 10.4 36 12.4 256 10.6
28 1.3 4 1.4 32 1.3
13 0.6 4 1.4 17 0.7
Accelerated acute rejection
Acute rejection
32 1.5 8 2.8 40 1.7
277 13.1 39 13.4 316 13.1
Chronic rejection
Recurrence of original kidney disease 138 6.5 28 9.6 166 6.9
Renal artery stenosis
Bacterial/viral infection
Cyclosporine toxicity
15 0.7
39 1.8
10 0.5
. . 15 0.6
4 1.4 43 1.8
. . 10 0.4
De novo kidney disease
Patient discontinued medication
Malignancy
Other/Unknown
99 4.7
29 1.4
255 12.0
8 2.8 107 4.4
1 0.3 30 1.2
32 11.0 287 11.9
5-7
NAPRTCS 2005
Transplant
EXHIBIT 5.2
PERCENT GRAFT SURVIVAL BY ALLOGRAFT SOURCE
100
90
80
70
60
50
40
Living Donor (1987-1994)
Living Donor (1995-2004)
Cadaver Donor (1987-1994)
Cadaver Donor (1995-2004)
30
0
Living Donor
(87 – 94)
Living Donor
(95 – 04)
Cadaver Donor
(87 – 94)
Cadaver Donor
(95 – 04)
1 2 3 4 5
YEARS
Years Post Transplant
1 3 5 7
90.7% ± 0.65% 83.5% ± 0.85% 77.8% ± 0.98% 71.7% ± 1.1%
94.8% ± 0.46% 90.5% ± 0.68% 85.0% ± 1.08% 75.6% ± 2.0%
80.0% ± 0.87% 69.4% ± 1.0% 61.6% ± 1.1% 55.1% ± 1.2%
91.7% ± 0.70% 82.5% ± 1.1% 74.2% ± 1.5% 64.5% ± 2.4%
5-8
NAPRTCS 2005
Transplant
EXHIBIT 5.3
GRAFT FAILURE SUMMARY, BY ALLOGRAFT SOURCE
AND TRANSPLANT CHARACTERISTICS
% N /
% Failure
Living Donor
(N=4587)
5 Year
Graft
Survival % N /
Cadaver Donor
(N=3834)
5 Year
Graft
Survival
(%) SE
Sex
Male 60.8/18.7 57.8/31.4
Female
Race
39.2/20.5 80.0 1.1 42.2/33.0
64.4 1.4
82.7 51.9/30.5
Black 11.3/29.4 22.6/38.9
Other 3.8/16.9 4.2 2.8
0.7 1.0
Dialysis
90.5 11.0/14.5
Recipient
2.3 5.3
78.1 49.1/29.2
- 2.8
>10 NA 77.1/30.2
<24 hours
>24 hours
NA - - 69.8/30.5
67.6 1.1
NA - - 30.2/41.1
61.1 1.7
5-9
NAPRTCS 2005
Transplant
EXHIBIT 5.3 (Continued)
GRAFT FAILURE SUMMARY, BY ALLOGRAFT SOURCE
AND TRANSPLANT CHARACTERISTICS
% N /
% Failure
Living Donor
(N=4587)
5 Year
Graft
Survival
(%) SE
% N /
% Failure
Cadaver Donor
(N=3834)
5 Year
Graft
Survival
(%) SE
Yes NA 21.2/44.0
Pre-operative
Immunosuppression
Yes
Induction Antibody
Early Administration
82.2 NA
27.6/23.4 79.6
0.8 1.0
1.3 20.2/38.8
62.1 2.0
1.1 1.4
2.1 1.8
1.0 1.4
5-10
70
60
50
100
90
80
40
30
0
0-1
2-5
6-12
>12
NAPRTCS 2005
Transplant
EXHIBIT 5.4
PERCENT GRAFT SURVIVAL FOR RECIPIENTS
OF LIVING DONOR SOURCE ALLOGRAFTS
AGE
100
INDUCTION ANTIBODY THERAPY
90
80
1 2 3
YEARS
RACE
4 5 6
100
90
80
70
60 60
50
40
White
Black
Hispanic
Other
30
0 1 2 3 4 5 6
YEARS
NOTE: Graft survival range plotted from 30% to 100%
50
40
30
0
100
90
80
70
70
60
50
40
30
0 1
TRANSFUSION HISTORY
1
No Induction
Induction
2 3
YEARS
0 Transfusions
<=5 Transfusions
>5 Transfusions
4
2 3
YEARS
4
5
5
5-11
6
6
70
60
50
100
90
80
40
30
0
100
90
80
70
60
50
40
30
0
NAPRTCS 2005
Transplant
EXHIBIT 5.5
PERCENT GRAFT SURVIVAL FOR RECIPIENTS OF
CADAVER DONOR SOURCE ALLOGRAFTS
RECIPIENT AGE
0-1
2-5
6-12
>12
1 2 3
YEARS
DONOR AGE
4
1
0-1
2-5
6-12
>12
2 3
YEARS
4
5
5
6
6
100
90
80
70
60
50
40
30
0
70
60
50
40
30
0
100
INDUCTION ANTIBODY THERAPY
90
80
No Induction
Induction
5 1 2 3
YEARS
4
PRIOR TRANSPLANT
1
Initial Transplant
Prior Transplant
2 3
YEARS
4 5
6
6
5-12
100
90
80
70
60
50
40
30
0
100
90
80
70
60
50
40
30
0
NAPRTCS 2005
Transplant
EXHIBIT 5.5 (continued)
PERCENT GRAFT SURVIVAL FOR RECIPIENTS OF
CADAVER DONOR SOURCE ALLOGRAFTS
COLD ISCHEMIA TIME PRIOR DIALYSIS
100
90
80
70
1
1
<=24 Hours
>24 Hours
2 3
YEARS
CADAVER-RACE
4
White
Black
Hispanic
Other
2 3
YEARS
4
5
5
6
6
90
80
70
60
50
40
30
0
60
50
40 No Prior Dialysis
Prior Dialysis
30
0 1 2 3 4
YEARS
CADAVER-TRANSFUSION
5
100
1
<=5 Transfusions
>5 Transfusions
2 3
YEARS
4 5
5-13
6
6
NAPRTCS 2005
Transplant
EXHIBIT 5.6
PERCENT GRAFT SURVIVAL FOR ANNUAL COHORT GROUP
LIVING DONOR
100
90
80
70
60
50
40
30
0
1987-1990
1991-1994
1995-1998
1999-2004
1 2 3
YEARS
4
CADAVER DONOR
5 6
100
90
80
70
60
50
40
1987-1990
1991-1994
1995-1998
1999-2004
30
0 1 2 3 4 5 6
YEARS
NOTE: Graft survival range plotted from 30% to 100%
5-14
70
60
50
40
30
0
100
90
80
60
50
40
30
0
100
90
80
70
90
80
70
60
50
40
30
0
NAPRTCS 2005
Transplant
EXHIBIT 5.7
100
GRAFT SURVIVAL BY DONOR SOURCE AND HLA-ANTIGEN DISPARITY
LIVING DONOR
HLA A MISMATCH
CADAVER DONOR
HLA A MISMATCH
100
2
1
0
1 2 3
YEARS
4
HLA B MISMATCH
5 6
90
80
70
60
50
40
30
0
2
1
0
1 2 3
YEARS
4
HLA B MISMATCH
5 6
2
1
0
60
50
40
30
0
100
90
80
70
2
1
0
1 2 3 4
YEARS
HLA DR MISMATCH
5 6 1 2 3 4
YEARS
HLA DR MISMATCH
5 6
1
2
1
0
2 3
YEARS
4 5 6
100
90
80
70
60
50
40
30
0 1
2
1
0
2 3
YEARS
4 5 6
5-15
100
90
80
70
60
50
40
30
0
70
60
50
40
30
0
100
NAPRTCS 2005
Transplant
EXHIBIT 5.8
PERCENT GRAFT SURVIVAL BY DONOR SOURCE AND DIAGNOSIS
LIVING DONOR CADAVER DONOR
100
90
80
90
80
Congenital/Structural
Glomerulonephritis
FSGS
CNS
1 2 3
YEARS
LIVING DONOR
4 5 6
70
60
50
40
30
0
Congenital/Structural
Glomerulonephritis
FSGS
CNS
1 2 3
YEARS
4
CADAVER DONOR
1
HUS
Renal Infarct
Cystinosis
Familial Nephritis
2 3
YEARS
4 5 6
100
90
80
70
60
50
40
30
0 1
HUS
Renal Infarct
Cystinosis
Familial Nephritis
2 3
YEARS
4
5
5
6
6
5-16
100
90
80
70
60
50
40
30
0
EXHIBIT 5.9
POST WEEK 1 GRAFT SURVIVAL BY DONOR SOURCE AND
ACUTE TUBULAR NECROSIS STATUS
LIVING DONOR
NAPRTCS 2005
Transplant
100
90
80
70
60
50
40
30
0
No ATN
ATN
5 6 1 2 3
YEARS
CADAVER DONOR
4
1
No ATN
ATN
5 6 2 3
YEARS
5-17
4
2.0
NAPRTCS 2005
Transplant
EXHIBIT 5.10
SERIAL SERUM CREATININE AND CALCULATED CREATININE CLEARANCE MEASURES
(MEAN ± SE) FOR FUNCTIONING GRAFTS, BY AGE AT TRANSPLANT
SERUM CREATININE
LIVING DONOR
Living Donor
CALCULATED CLEARANCE
LIVING DONOR
Living Donor
110
1.5
1.0
0.5
0.0
0 1 2 3
YEARS
CADAVER DONOR
Cadaver Donor
4 5
0-1
2-5
6-12
>12
6
100
90
80
70
60
50
0 1 2 3
YEARS
CADAVER DONOR
Cadaver Donor
4 5
0-1
2-5
6-12
>12
6
2.0
1.5
110
100
90
0-1
2-5
6-12
>12
1.0
0.5
0.0
0 1 2 3
YEARS
4 5
0-1
2-5
6-12
>12
6
80
70
60
50
0 1 2 3
YEARS
4 5 6
5-18
2.0
NAPRTCS 2005
Transplant
EXHIBIT 5.11
SERIAL SERUM CREATININE (MEAN ± SE) FOR FUNCTIONING GRAFTS,
BY RACE AND INDUCTION ANTIBODY THERAPY
RACE
LIVING DONOR
Living Donor
INDUCTION ANTIBODY THERAPY
LIVING DONOR
Living Donor
2.0
1.5
1.5
1.0
0.5
0 1 2 3
YEARS
CADAVER DONOR
Cadaver Donor
4
Black
Non-Black
5 6
2.0
1.0
0.5
0 1 2 3
YEARS
CADAVER DONOR
Cadaver Donor
4
No Induction
Induction
5 6
2.0
1.5
1.5
1.0
0.5
0 1 2 3
YEARS
4
Black
Non-Black
5 6
5-19
1.0
0.5
0 1 2 3
YEARS
4
No Induction
Induction
5 6
NAPRTCS 2005
Transplant
EXHIBIT 5.12
GRAFT FUNCTION, I.E. GRAFT SURVIVAL AND MEAN CALCULATED CLEARANCE
AT ANNUAL FOLLOW-UP, BY DONOR SOURCE
90
85
Living Donor 1996-2004
Living Donor 1987-1995
Cadaver Donor 1996-2004
Cadaver Donor 1987-1995
80
75
70
65
60
55
50
50 60 70 80 90 100
% GRAFT SURVIVAL
NOTE: Symbols refer to post-transplant follow-up years, with Year 1 represented by the upper right position of the line, Year 5 by the bottom left point.
5-20
NAPRTCS 2005
Transplant
80
75
70
65
EXHIBIT 5.13
GRAFT FUNCTION, I.E. GRAFT SURVIVAL AND MEAN CALCULATED CLEARANCE
AT ANNUAL FOLLOW-UP, BY DONOR SOURCE AND
INITIAL USE OF ANTIBODY PREPARATIONS
Living Donor Cadaver Donor
90 90
No Antibody Therapy
Antibody Therapy
No Antibody Therapy
Antibody Therapy
85 85
80
75
70
65
60 60
55 55
50
50 60 70 80 90 100
50
50 60 70 80 90 100
% GRAFT SURVIVAL % GRAFT SURVIVAL
NOTE: Symbols refer to post-transplant follow-up years, with Year 1 represented by the upper right position of the line, Year 6 by the bottom left point.
5-21
NAPRTCS 2005
Transplant
80
75
70
65
EXHIBIT 5.14
GRAFT FUNCTION, I.E. GRAFT SURVIVAL AND MEAN CALCULATED CLEARANCE
AT ANNUAL FOLLOW-UP, BY DONOR SOURCE AND RACE
Living Donor Cadaver Donor
90 90
Black
Non-black
Black
Non-black
85 85
80
75
70
65
60 60
55 55
50
50 60 70 80 90 100
50
50 60 70 80 90 100
% GRAFT SURVIVAL % GRAFT SURVIVAL
NOTE: Symbols refer to post-transplant follow-up years, with Year 1 represented by the upper right position of the line, Year 6 by the bottom left point.
5-22
NAPRTCS 2005
Transplant
SECTION 6: GROWTH
At each six-month follow-up, the cooperative study requests the submission of height and weight information on all transplanted patients. Standardized Z-scores are computed following an age- and sex-specific formula based on the NHANES III 2000 growth chart data set. NHANES III is a study sponsored by the National Center for Health Statistics/CDC which provides values at monthly intervals for each sex until the age of 21 years. This is a change in the standardized height and weight calculation from early reports, thus direct comparisons to reports prior to the 2004 annual report should not be made.
Exhibit 6.1 presents standardized height and weight Z-scores for index graft recipients at entry and at follow-up visits for selected characteristics; subjects are excluded from further calculation at the time of graft failure. At transplantation, the mean height deficits for all patients is –1.85; that is, the average patient is nearly 2 standard deviations below the appropriate age- and sex-adjusted height level or is shorter than the third percentile of their peers. This deficit is greater for males (-1.90) than females (-1.77). Younger subjects and those with prior transplants have substantially greater height deficits at the time of transplantation. Overall, mean height scores remain relatively constant over the available follow-up period. However, growth patterns differ by age at transplant, with younger subjects (less than 6 years of age) experiencing improvement in mean growth deficit. This is further characterized in Exhibit 6.2, where, rather than mean scores, mean changes from baseline Z-scores are presented graphically. For the youngest age group, an immediate increase in height of .21 standard deviations is observed in the first six months post-transplant, which increases to approximately half of a standard deviation (.49) by 12 months post transplant.
Subjects with functioning grafts who were age 2-5 at transplant appear to achieve similar acceleration in linear growth for a couple of years and have a mean increase in Z-score of .56 at 2 years. For subjects aged 6-12, linear growth appears to be stable and consistent with that of the normal population, and the older subjects have no mean increase in Z-scores.
Note that as the study has matured, some transplant patients have reached their adult height. The mean Z-score of these subjects, at least 19 years of age (N=1,405), is -1.5. Twenty-five percent of these patients have a Z-score of -2.4 or worse, and 10% are over 3.3 standard deviations below the population average. Significant improvement in terminal height has been observed with the 1987 cohort having an average terminal height of -2.1 versus –1.4 for the 1995 cohort.
6-1
NAPRTCS 2005
Transplant
Exhibit 6.3 demonstrates the improvement in height deficit at the time of initial transplant that has occurred over time. In 1987, patients receiving their initial transplant were an average of 2.4 standard deviations below average. This has improved in later annual cohorts to –1.4 in the 2000 and 2003 cohorts.
Besides age, several variables such as donor source and concomitant therapy are predictive of 2year standardized height changes, but each observed mean difference is less than 0.3 Z-score.
Subjects not receiving anti-hypertensive therapy during the first post-transplant month have better growth in the first two post-transplant years (difference in mean standardized height scores=0.18,
(p<0.001) ∆ z=0.18 after adjustment for age), a difference which is maintained at 3 years
(difference=0.21).
With respect to weight scores, a rapid increase in standardized weight scores is observed for all age groups. In the youngest age group, mean standardized weight is still significantly less than national norms 3 years after transplantation, but continued relative weight gain is observed into the fifth post transplant year. Half of patients over the age of 6 years, gain over 0.9 Z-score within 6 months following transplantation, with relative stability in average standardized weight scores over the next 4 years.
6-2
NAPRTCS 2005
Transplant
EXHIBIT 6.1
MEAN (WITH SE) STANDARDIZED HEIGHT AND WEIGHT SCORES,
BY SELECTED CHARACTERISTICS AND TIMES POST-TRANSPLANTATION
Baseline Month 24 Month 72
(N=8141) (N=4777) (N=1673)
Standardized Height Mean SE Mean SE Mean SE
Total -1.85 0.02 -1.73 0.02 -1.97 0.03
Sex
Male
Female
Age
-1.90 0.03 -1.75 0.02 -2.01 0.04
-1.77 0.04 -1.70 0.03 -1.91 0.06
0-1
2-5
6-12
13-17
-1.98 0.17 -1.65 0.08 -1.76 0.11
-2.34 0.05 -1.79 0.05 -1.91 0.07
-2.07 0.03 -1.93 0.03 -2.12 0.05
-1.49 0.03 -1.51 0.03 -1.75 0.08
No
Yes
-1.76 0.02 -1.66 0.02 -1.92 0.03
-2.62 0.07 -2.44 0.08 -2.61 0.13
Baseline Month 24 Month 72
(N=8255) (N=4856) (N=1537)
Standardized Weight Mean SE Mean SE Mean SE
Total -1.23 0.03 -0.34 0.02 -0.40 0.04
Sex
Male -1.21 0.04 -0.38 0.03 -0.45 0.05
Female
Age
0-1
2-5
6-12
13-17
-1.26 0.03 -0.27 0.04 -0.32 0.07
-1.23 0.33 -0.64 0.08 -0.51 0.11
-1.33 0.05 -0.37 0.05 -0.10 0.08
-1.34 0.03 -0.21 0.04 -0.49 0.06
-1.11 0.03 -0.41 0.04 -0.65 0.17
No
Yes
-1.18 0.03 -0.31 0.02 -0.36 0.04
-1.68 0.07 -0.67 0.09 -0.92 0.16
6-3
NAPRTCS 2005
Transplant
EXHIBIT 6.2
MEAN CHANGE FROM BASELINE (WITH SE) IN STANDARDIZED HEIGHT AND
WEIGHT SCORES IN SUBJECTS WITH GRAFT FUNCTION BY AGE AT TRANSPLANT
1.25
1.00
0.75
0-1
2-5
6-12
>12
0.50
0.25
0.00
-0.25
0 1 2
YEARS
3 4 5
2.00
1.75
1.50
1.25
1.00
0.75
0-1
2-5
6-12
>12
0.50
0.25
0.00
0 1 2 3 4 5
YEARS
Sample sizes for Height Delta Z at Follow-up Months:
6-4
-1.5
-2.0
-1.0
EXHIBIT 6.3
MEAN (WITH SE) OF STANDARDIZED HEIGHT AT TIME OF
NAPRTCS 2005
Transplant
INITIAL TRANSPLANT, BY YEAR OF TRANSPLANT
-2.5
1987 1991 1995
YEAR
1999 2003
6-5
NAPRTCS 2005
Transplant
EXHIBIT 6.4
MEAN (WITH SE) OF STANDARDIZED HEIGHT AT INITIAL TRANSPLANT OVER TIME,
BY YEAR OF TRANSPLANT AND AGE AT TRANSPLANT
-1.0
-1.5
0-1
2-5
6-12
>12
-2.0
-2.5
-3.0
-3.5
1987 1991 1995
YEAR
1999 2003
6-6
SECTION 7: MORBIDITY, MALIGNANCY, AND MORTALITY
NAPRTCS 2005
Transplant
Morbidity
In this report, we measure morbidity by the number of hospitalization days. The median duration (to initial discharge) of hospitalization at the time of transplant is 12 days, with lower and upper quartiles of 8 and 19 days. Due to re-hospitalization, patients were hospitalized for a median duration of 14 days during the transplant month with lower and upper quantities of 9 and 21 days.
Transplant month hospitalization times are negatively correlated with patient age such that the mean hospital stays are 20, 18, 16, and 14 days for patients aged 0-1, 2-5, 6-12, and >12 years, respectively. The median number of hospitalization days in the transplant month for recipients of cadaver source allografts (17 days) is three days longer than for those who received grafts from a living donor. Donor-specific hospitalization data for the first post transplant month are presented in
Exhibit 7.1. In 1987, living donor (LD) transplant recipients, on average, were hospitalized for 18 days during the first post transplant month, compared to nearly 22 days for cadaver donor (CD) transplant recipients. Between 1997 and 2004, mean hospital stay during this initial post transplant period has ranged between 9.9 to 13.0 days for LD and 10.8 to 14.6 days CD transplant recipients.
Exhibit 7.2A, 7.2B, and 7.2C present transplant month hospitalization data for selected patient and transplant characteristics (of all, LD, and CD transplants). In regression analyses that took into account transplant era (1987-1995 vs. 1996-2004) and the characteristics shown in Exhibit 7.2A and 7.2B, we observed that, with the exception of prior transplant, each characteristic was statistically significant at less than the .001 level of significance — overall and for living donor recipients. However, among cadaver donor recipients, all characteristics were statistically significant at less than .001 level with the exception of prior transplant AND prior dialysis. Overall, the transplant month hospitalization stays have been significantly shorter in the recent era (1996-
2004) compared to the earlier era (1987-1995) by 5 days.
Exhibits 7.3A and 7.3B detail length of hospital stays and reasons for hospitalization for those patients surviving the interval with a functioning graft. Results are provided separately for living
(Exhibit 7.3A) and cadaver (Exhibit 7.3B) donor sources. During months 1-5, 48.3% of living donor graft recipients were re-hospitalized compared to 56.7% of cadaver donor graft recipients. The most common reason for hospitalization in this interval was treatment of rejection, which occurred in
28.5% and 19.6% of CD and LD patients, respectively. Viral (15.7% vs. 13%) and bacterial (13.4% vs. 12.1%) infections and treatment of hypertension (5.9% vs. 3.6%) were other major causes of hospitalization. Hospital stays decrease in both frequency and length by month 6 and beyond,
7-1
NAPRTCS 2005
Transplant while the treatment of rejection remains the primary reason for hospitalization. Since 1996, it appears that the hospitalization lengths have plateaued and that the difference between LD and CD graft recipients diminished.
Malignancy
To date, 232 malignancies have been reported of which 222 have confirmed diagnoses 179 lymphoproliferative (LPD) and 43 non-lymphoproliferative (non-LPD). Exhibit 7.4 shows selected transplant characteristics for the cohort with malignancy. Using the 9,228 transplants, 2.5% of transplants are associated with development of malignancy during the follow-up period. The median time from transplant to malignancy for those with a confirmed diagnosis was 18 months
(range 1-163). One- and three-year product limit estimates of the malignancy rates by era of entry are as follows:
Post Transplant Malignancy Rate Percentages (Mean ± SE)
1987-1991
1992-1995
1 Year
0.62 ± 0.16
1.30 ± 0.24
3 Year
0.96 ± 0.21
2.0 ± 0.30
≥ 1996 2.0 ± 0.25 3.14 ± 0.34
While substantial temporal improvements have been observed in graft failure, rejection and other endpoints, reported malignancy rates appear to be increasing.
Mortality
To assess post transplant patient survival, we considered 8,420 index transplants (4,587 LD and
3,833 CD). We have not adjusted the analysis for patient deaths that occurred subsequent to graft failure while the patient was receiving maintenance dialysis. Percent patient survival estimates
(with standard errors) for all patients at 12, 24, and 60 months post transplant are 97.6±0.17,
96.6±0.21, and 95.0±0.28, respectively. Exhibit 7.5A depicts patient survival by allograft source.
Percent patient survival estimates for recipients of index living donor kidneys are 98.2±0.21,
97.3±0.26, and 95.6±0.36 percent, at 12, 24, and 60 months post transplant, respectively.
Comparable values for recipients of primary cadaver donor allografts are 96.9±0.29, 95.8±0.35, and
92.2±0.54 percent (donor source p<0.001). Exhibit 7.5B compares patient survival of transplants in
1987-1995 (early era) and in 1996-2004 (recent era), by primary allograft source. Patient survival
7-2
NAPRTCS 2005
Transplant has significantly improved for CD patients in the recent era (p<0.001). Their 5-year post transplant survival in the early era was 90.8
± 0.67, compared to 95.4
± 0.94 for the recent era. LD patients 5year survival rate was 95.1
± 0.48 in the early era and 96.1
± 0.63 in the recent era (p=0.099).
Patient survival, by recipient age at transplant, is shown below and in Exhibits 7.6A and 7.6B for living and cadaver donor source transplants. Post transplant survival is markedly lower for infants
(<24 months old at transplant), for recipients of cadaver donor grafts. The table below shows percent survival at 36 months post transplant, by age at transplantation. Although infants’ post transplant survival is lower compared to the other age groups, the situation has been significantly improved recently. The 3-year patient survival of infants receiving cadaver donor source grafts has increased from 78.0% (SE=4.7%) between 1987 and 1995 to 94.4% (SE=5.4%) in 1996 and later.
For infants receiving living donor grafts, their 3-year survival also improved from 90.2% (SE=2.2%) in 1987-1995 to 94.3% (SE=2.1%) in 1996 and beyond.
36-Month Post Transplant Patient Survival
Living Donor
% Surv. SE
Cadaver Donor
% Surv. SE
All
0-1
2-5
96.8 0.26 94.9 0.39
91.9 1.54 81.3 4.00
96.9 0.70 91.7 1.27
6-12 97.6 0.42 96.1 0.56
>12 97.1 0.43 95.7 0.55
In total, death reports have been received for 495 of the 8,420 patients (5.9%). Crude donor source-specific mortality rates are 4.7% (217/4,587) for recipients of living donor primary transplants and 7.3% (278/3,833) for recipient of cadaver donor primary transplants. Reasons for patient death are shown in Exhibit 7.7. Infection was the cause of death in 145 patients (29.3% of deaths). Other reported causes include cancer/malignancy (n=55, 11.1%), cardiopulmonary (n=76,
15.4%), and dialysis-related complications (n=14, 2.8%). Of the expired patients, 227 (45.9%) died with a functioning graft.
7-3
NAPRTCS 2005
Transplant
EXHIBIT 7.1
HOSPITALIZATION DAYS DURING THE FIRST POST-TRANSPLANT MONTH,
BY YEAR OF TRANSPLANTATION AND DONOR SOURCE (MEAN ± SE)
25
20
15
10
5
1987 1989 1991 1993 1995 1997 1999 2001 2003
TRANSPLANT YEAR
7-4
NAPRTCS 2005
Transplant
EXHIBIT 7.2A
TRANSPLANT MONTH HOSPITALIZATION
All Patients
(N=9067)
Living Donor
(N=4709)
Cadaver Donor
(N=4358)
Mean SE Mean SE Mean SE
0-1
2-5
6-12
>12
19.8 0.37 19.0 0.41 22.2 0.81
18.0 0.22 17.0 0.29 19.2 0.34
15.7 0.14 14.3 0.18 17.3 0.20
13.8 0.11 12.1 0.15 15.4 0.16
One or more transplants 16.9 0.20 15.0 0.37 17.7 0.24
ATN
No
Yes
Rejection during
14.8 0.08 13.9 0.11 16.0 0.13
20.1 0.25 20.1 0.52 20.1 0.29
No
Yes
Native renal tissue removed
13.6 0.09 12.7 0.11 14.7 0.13
20.9 0.15 19.8 0.24 21.7 0.20
No, Not all removed
Prior dialysis
17.1 0.16 16.1 0.21 18.4 0.25
7-5
NAPRTCS 2005
Transplant
EXHIBIT 7.2B
TRANSPLANT (1987-1995) MONTH HOSPITALIZATION
Total
(N=4508)
Living Donor
(N=2093)
Cadaver Donor
(N=2415)
Mean SE Mean SE Mean SE
0-1
2-5
6-12
>12
22.4 0.44 21.3 0.50 24.8 0.79
20.3 0.27 19.5 0.36 21.0 0.40
18.0 0.17 16.5 0.24 19.3 0.23
16.0 0.15 14.1 0.21 17.4 0.20
One or more transplants 19.4 0.24 18.4 0.49 19.7 0.28
ATN
No
Yes
Rejection during
17.2 0.11 16.2 0.15 18.3 0.16
21.1 0.31 21.1 0.70 21.1 0.34
No
Yes
Native renal tissue removed
15.6 0.12 14.6 0.16 16.7 0.17
21.6 0.16 20.6 0.26 22.2 0.21
No, Not all removed
Prior dialysis
19.0 0.20 18.0 0.27 20.3 0.29
7-6
NAPRTCS 2005
Transplant
EXHIBIT 7.2C
TRANSPLANT (1996-2004) MONTH HOSPITALIZATION
Total
(N=4559)
Living Donor
(N=2616)
Cadaver Donor
(N=1943)
Mean SE Mean SE Mean SE
0-1
2-5
6-12
>12
16.3 0.57 16.5 0.61 15.1 1.51
14.7 0.34 14.1 0.41 15.8 0.58
12.4 0.20 11.6 0.24 13.5 0.32
11.2 0.15 10.2 0.19 12.5 0.24
One or more transplants 12.9 0.30 11.8 0.47 13.7 0.39
ATN
No
Yes
Rejection during
11.7 0.11 11.4 0.14 12.3 0.19
18.4 0.41 18.9 0.76 18.2 0.49
No
Yes
Native renal tissue removed
11.7 0.12 11.2 0.15 12.4 0.19
18.0 0.37 17.0 0.52 19.1 0.53
No, Not all removed
Prior dialysis
14.3 0.24 13.8 0.30 15.2 0.40
7-7
NAPRTCS 2005
Transplant
EXHIBIT 7.3A
HOSPITALIZATION RESULTS FOR PATIENTS WITH FUNCTIONING
GRAFTS IN SPECIFIED FOLLOW-UP PERIODS
LIVING DONOR TRANSPLANTS
Months
1-5
Months
6-11
Months
12-17
Months
18-23
Months
30-35
Months
42-47
Months
54-59
Total
Days Hospitalized
3989 3636 3280 2987 2443 1940 1471
Median 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Mean 6.0 2.7 2.0 1.4 1.3 1.0 1.0
[Hospitalized only]
Median
Mean
% Hospitalized for:
8.0 5.0 5.0 5.0 4.0 4.0 4.0
12.5 9.5 8.8 7.0 7.0 5.9 6.5
48.3 28.9 22.9 20.5 18.3 16.5 16.1
Rejection
Hypertension
12.1 7.7 6.8 5.9 4.5 4.3 5.0
0.7 0.2 0.3 0.2 0.2 0.3 0.2
13.0 7.7 5.5 5.3 4.4 3.8 4.2
19.6 8.6 6.2 5.4 4.3 2.9 3.3
3.6 1.7 1.4 1.1 0.7 0.8 0.6
7-8
NAPRTCS 2005
Transplant
EXHIBIT 7.3B
HOSPITALIZATION RESULTS FOR PATIENTS WITH FUNCTIONING
GRAFTS IN SPECIFIED FOLLOW-UP PERIODS
CADAVER DONOR TRANSPLANTS
Months
1-5
Months
6-11
Months
12-17
Months
18-23
Months
30-35
Months
42-47
Months
54-59
Total
Days Hospitalized
3453 3125 2820 2503 1966 1521 1164
Median 3.0 0.0 0.0 0.0 0.0 0.0 0.0
Mean 8.6 3.5 2.6 2.0 1.6 1.3 1.2
[Hospitalized only]
Median
Mean
% Hospitalized for:
10.0 7.0 6.0 5.0 4.0 4.0 4.0
15.2 11.1 9.8 8.1 7.3 7.6 7.0
56.7 31.5 26.8 24.6 22.1 17.8 17.8
Rejection
Hypertension
13.4 9.1 6.4 5.2 5.0 4.9 4.1
1.1 0.6 0.3 0.1 0.2 0.1 0.2
15.7 7.5 6.0 6.0 4.9 3.7 4.0
28.5 11.3 8.8 7.7 6.2 4.5 3.9
5.9 2.9 2.1 2.1 2.0 1.7 1.1
7-9
NAPRTCS 2005
Transplant
EXHIBIT 7.4
SELECTED CHARACTERISTICS OF TRANSPLANTS WITH MALIGNANCY*
All patients
Donor source
Malignancies
Yes
N %
232 2.51
Age
Sex
Race
Transplant year
*Denominator is the number of transplants with functioning graft of 30 days or longer.
7-10
NAPRTCS 2005
Transplant
EXHIBIT 7.5A
PERCENT PATIENT SURVIVAL BY PRIMARY ALLOGRAFT SOURCE
100
90
80
Living Donor
Cadaver Donor
70
0 12 24 36 48 60 72 84
MONTHS
EXHIBIT 7.5B
PERCENT PATIENT SURVIVAL BY ERA AND PRIMARY ALLOGRAFT SOURCE
100
90
80
70
0
LD 1987-1994
LD 1995-2004
CD 1987-1994
CD 1995-2004
12 24 36
MONTHS
7-11
48 60
NAPRTCS 2005
Transplant
EXHIBIT 7.6A
PERCENT PATIENT SURVIVAL OF PRIMARY TRANSPLANTS,
BY AGE AT TRANSPLANTATION - LIVING DONOR
100
90
80
0-1
2-5
6-12
>12
70
0 12 24 36 48 60 72 84
MONTHS
EXHIBIT 7.6B
PERCENT PATIENT SURVIVAL OF PRIMARY TRANSPLANTS,
BY AGE AT TRANSPLANTATION - CADAVER DONOR
100
90
80
0-1
2-5
6-12
>12
70
0 12 24 36 48
MONTHS
60 72 84
7-12
NAPRTCS 2005
Transplant
EXHIBIT 7.7
CAUSES OF DEATH
FOLLOWING INDEX RENAL TRANSPLANTATION
Living Donor Cadaver Donor
Func.
graft 1 N %
Func.
graft 1
Func.
N % graft 1
All deceased patients 495 100.0
227 217 100.0
106 278 100.0
121
Cause of death
Bacterial
42 8.5
64 12.9
21
30
22
31
10.1
14.3
11
13
20 7.2
33 11.9
10
17
Other infection
Total
39 7.9
20 7.2
Cardiopulmonary
Hemorrhage
76 15.4
33 6.7
11
39
36
12
1
19 8.8
30 13.8
26 12.0
9 4.1
3 1.4
5
23
14
2
1
50 18.0
24 8.6
5 1.8
6
16
22
10
--
Dialysis-related complication
Other
14 2.8
121 24.4
--
57
7
56
14
3.2
25.8
6.5
--
31
6
7 2.5
65 23.4
--
26
1 Number of functioning grafts at time of death
7-13
III. DIALYSIS
NAPRTCS 2005
Dialysis
SECTION 8: DIALYSIS PATIENT CHARACTERISTICS
Maintenance dialysis initiation data have been submitted for 5,639 patients; selected characteristics of these patients are presented in Exhibit 8.1. The percentages of white, black, and Hispanic patients reported to the dialysis registry are 50%, 24%, and 20%, respectively, compared to 62%,
16%, and 16% reported to the transplant registry. Thirteen percent of patients were less than 2 years old at initiation of the first registered (i.e., index) course of dialysis, compared to 5.5% who were less than 2 years old at index transplantation. (The index dialysis initiation or index transplant is defined as the first of each event reported since the start of the respective study component,
1992 for dialysis and 1987 for transplantation.) Patients 2-5, 6-12, 13-17, and >17 years of age at index initiation comprise 10.3%, 31.0%, 38.3%, and 7.6%, respectively, of the cohort. Whereas patients with focal segmental glomerulosclerosis (FSGS) comprise 11.5% of the transplant cohort
(4 percentage points less than the two most common primary renal diseases for that group), they comprise 14.2% of dialysis patients, almost equaling the prevalence of renal dysplasia. FSGS cases comprise 23.6% of all black dialysis patients and 30.4% of black patients >12 years old. The second most prevalent diagnosis among all blacks is renal dysplasia (12.0%), and among black patients >12 years old it is SLE nephritis (10.5%). FSGS accounts for 11.2% of all white dialysis patients, as well as 11.1% of white adolescents. Renal dysplasia (16.0%) remains most common for all whites, but obstructive uropathy (15.0%) is most prevalent among white patients ≥ 12 years old.
Also shown are distributions of selected characteristics, by cohort year. A total of 739 patients
(13.1%) were already receiving maintenance dialysis as of the January 1, 1992 (start date for data collection); an additional 476 (8.4%) patients initiated dialysis that year. The distributions of age, race, gender, and dialysis modality have remained stable over the years of data collection.
Race and age distributions, by dialysis modality, are shown in Exhibit 8.2 for all index courses of PD and HD. Among white patients, 41.8% are older than 12 years of age (34.4% of PD >12 years old,
59.1% of HD >12 years old), compared to 57.0% of blacks (46.9% PD, 68.5% HD). This phenomenon may, in part, be explained by the prevalence of FSGS among black adolescents already described.
Concomitant drug therapy is described in Exhibits 8.3 and 8.4 for the 1-, 12-, 24- and 36-month follow-up visits of dialysis courses. Notable trends include the decreased use over time of antihypertensives among both PD and HD patients. Among HD, the use of intravenous iron peaks at
8-1
NAPRTCS 2005
Dialysis
24 months (39% vs. 22% at baseline). The use of oral iron among PD patients increases from 78% at baseline to 83% at 36 months.
At baseline (30 days following index initiation), 3.7% of patients had completed their high school education and 21.0% were not of school age. Available education data for the remaining dialysis patients are presented in Exhibits 8.5 through 8.8. Among school-age patients maintained on peritoneal dialysis, 77% were attending school full-time and 10% part-time, compared to 52% and
28% of children on hemodialysis (Exhibit 8.5). Eight percent of HD patients were not attending school even though they were medically capable, compared to 5% of PD patients.
Education status is also shown according to race (Exhibit 8.6) and age (Exhibit 8.7). Patterns of school attendance are similar between black and white PD patients. Hispanic children have less full-time school attendance than black or white patients. The percentage of children and adolescents not receiving any schooling, by age, is 9% (PD) and 9% (HD) for patients aged 6-12;
7% (PD) and 13% (HD) for patients older than 12. Full-time school attendance — through three years of maintenance dialysis therapy — is depicted in Exhibit 8.8, by dialysis modality, race, and age. Exhibit 8.8 shows that the percentage of Hispanic patients on HD who attend school full-time is much less than half that of black, white, or other patients. There are 249 Mexican and Costa
Rican subjects. Full-time school attendance at entry is 46% in North American Hispanics versus
14% in "South of the Border" Hispanics.
To assess dialysis patient survival, we considered 2,696 patients on dialysis whose first reported course of dialysis appears to be the first ever with no history of prior renal transplantation (310 under 1 year-olds, 103 1 year-olds, 292 2-5 year-olds, 825 6-12 year-olds, and 1166 >12 year-olds).
The descending age groups have significantly worse survival experience relative to the >12 year old group (6-12 RH= 1.0 (95% CI= 0.74-1.48); 2-5 RH= 1.6 (95% CI= 1.1-2.5); 0-1 RH= 3.9 (95%
CI= 2.8-5.3)). Exhibit 8.9 shows patient survival by age at dialysis initiation. Patient survival is measured from the time of dialysis initiation to death, with censoring for transplantation or lost to follow-up visit.
8-2
NAPRTCS 2005
Dialysis
Patient survival estimates at 12, 24, and 36 months following dialysis initiation are provided in the table below.
N
12 Months
%
Survival
Patient Survival
SE
24 Months 36 Months
%
Survival SE
%
Survival SE
Age
0 310 83.0 2.3 74.3 3.0 66.0 3.7
1 103 92.8 2.9 75.7 6.5 68.5 7.7
2-5 292 92.6 1.8 88.4 2.5 84.6 3.3
6-12 825 96.2 0.79 93.1 1.2 90.1 1.6
>12 1166 97.3 0.56 93.2 1.1 88.7 1.6
Exhibit 8.10 lists the causes of death according to age at time of first dialysis. Of the causes of death specified, cardiopulmonary was the reason cited most (21.6%), both overall and for each of the individual age groups. For those deaths from malignancy with a reported diagnosis, 73.6% were lymphoproliferative disorders.
Survival rates estimated by the product limit method by year of entry are shown below. It appears that year of entry has not had a major impact on patient mortality (p=0.246).
Years
92 – 94
95 – 97
98 – 00
01 – 04
Patient Survival by Era
N
1 Year 2 Years
% %
Survival SE Survival SE
1404 95.4 0.6 90.7 1.0
1438
1160
653
95.0
95.5
97.5
0.7
0.7
0.7
91.0
92.7
92.6
1.0
1.0
1.5
8-3
NAPRTCS 2005
Dialysis
EXHIBIT 8.1 - DIALYSIS PATIENT DEMOGRAPHICS
Gender
Race and Ethnicity
Diagnosis
Aplasia / hypoplasia / dysplasia 815 14.5
Focal segmental glomerulosclerosis
Obstructive uropathy
800
748
14.2
13.3
Reflux nephropathy
SLE nephritis
Chronic glomerulonephritis
Hemolytic uremic syndrome
196
193
181
176
3.5
3.4
3.2
3.1
Polycystic disease
Congenital nephrotic syndrome
Medullary cystic disease
Prune Belly
Idiopathic crescentic glomerulonephritis
Membranoproliferative glomerulonephritis Type I
Familial nephritis
Pyelonephritis / interstitial nephritis
163
144
120
116
116
106
104
89
2.9
2.6
2.1
2.1
2.1
1.9
1.8
1.6
Renal infarct
Berger's (IgA) nephritis
Henoch-Schonlein nephritis
Membranoproliferative glomerulonephritis Type II
Wilms tumor
Other systemic immunologic disease
81
71
65
57
41
37
1.4
1.3
1.2
1.0
0.7
0.7
Wegener's granulomatosis
Drash syndrome
34
34
0.6
0.6
Oxalosis 28
Membranous nephropathy 24 0.4
Sickle cell nephropathy
Diabetic GN
19
6
0.3
0.1
8-4
NAPRTCS 2005
Dialysis
EXHIBIT 8.1 - DIALYSIS PATIENT DEMOGRAPHICS - (Continued)
Age at Index Initiation
5 160
12 346
Age Groupings
Number of Dialysis Initiations by Year
'91 '92 '93 '94 '95 '96 '97 '98 '99 '00 '01 '02 '03 '04
Total
(N) 739 476 462 466 508 468 462 397 409 360 331 266 192 103
8-5
NAPRTCS 2005
Dialysis
8-6
NAPRTCS 2005
Dialysis
White
Black
Hispanic
Other
EXHIBIT 8.2
NUMBER AND PERCENT DISTRIBUTIONS OF PATIENT RACE/ETHNICITY,
BY DIALYSIS MODALITY AND AGE AT INITIATION
Peritoneal Dialysis
0-1 2-5 6-12 >12
3647 678 18.6 449 12.3 1155 31.7 1365 37.4
1960 438 22.3 254 13.0 594 30.3 674 34.4
751 104 13.8 95 12.6 287 38.2 265 35.3
215 32 14.9 35 16.3 60 27.9 88 40.9
Hemodialysis
0-1 2-5 6-12 >12
1987 47 2.4 134 6.7 587 29.5 1219 61.3
Other
11 6.2
8-7
Concomitant Drug Therapy
Sevelamer HCl
Anticonvulsant
Antihypertensives
Calcium Acetate
Calcium Carbonate
Other Calcium
Immumosuppressives
Oral Vitamin D
Intravenous Vitamin D
Enteral Nutrition
Parenteral Nutrition
Oral Iron
Intravenous Iron
Prophylactic Antibiotics
Lipid Lowering Agents
Epo
HGH
0
NAPRTCS 2005
Dialysis
EXHIBIT 8.3
POST INITIATION (1 MONTH AND 12 MONTHS)
CONCOMITANT DRUG THERAPY
25 50
PERCENT
Hemodialysis
Peritoneal dialysis
75 100
34
1
16
21
3
2
61
74
22
3
16
15
15
14
94
88
10
10
23
15
46
78
74
74
7
5
Percent
21
12
64
58
12
11
8
6
0 25 50
PERCENT
75
Hemodialysis
Peritoneal dialysis
100
Percent
12
17
10
15
96
95
13
20
46
2
14
23
3
2
59
83
36
5
71
73
10
7
36
80
5
5
62
49
17
12
28
17
12
7
8-8
Concomitant Drug Therapy
Sevelamer HCl
Anticonvulsant
Antihypertensives
Calcium Acetate
Calcium Carbonate
Other Calcium
Immumosuppressives
Oral Vitamin D
Intravenous Vitamin D
Enteral Nutrition
Parenteral Nutrition
Oral Iron
Intravenous Iron
Prophylactic Antibiotics
Lipid Lowering Agents
Epo
HGH
0
NAPRTCS 2005
Dialysis
EXHIBIT 8.4
POST INITIATION (24 MONTHS AND 36 MONTHS)
CONCOMITANT DRUG THERAPY
25 50
PERCENT
Hemodialysis
Peritoneal dialysis
75 100
Percent
9
16
8
15
95
95
16
27
14
24
2
1
59
83
39
5
10
4
31
78
51
2
26
19
12
8
55
48
16
14
71
68
7
6
0 25 50
PERCENT
Hemodialysis
Peritoneal dialysis
75 100
Percent
9
13
95
96
59
85
39
7
11
13
16
24
12
23
2
1
10
5
32
83
49
2
52
45
17
9
25
31
14
8
73
72
9
8
8-9
NAPRTCS 2005
Dialysis
100
EXHIBIT 8.5
BASELINE EDUCATION STATUS
75
77
PD
HD
50
52
28
25
10
5
8
5
8
3 4
0
Full-time Part-time Home
Schooling
None
(Capable)
None
(Incapable)
8-10
100
75
82
EXHIBIT 8.6
BASELINE EDUCATION STATUS BY RACE
PD
HD
100
75
83
50
56
PD
HD
NAPRTCS 2005
Dialysis
50
50
28
25
0
Full-time
6
10
6
2
7
3
5
Part-time Home
Schooling
None
(Capable)
None
(Incapable)
100
25
5
8
0
Full-time
6
3
5
3 3
Part-time Home
Schooling
None
(Capable)
None
(Incapable)
100
75
80
66
50
28
PD
HD 75
PD
HD
58
50
43
32
25
20
15 14
4
8
0
Full-time
3 3
Part-time Home
Schooling
None
(Capable)
None
(Incapable)
25
0
Full-time
20
11
Part-time
3
1
Home
Schooling
4
10
None
(Capable)
1
3
None
(Incapable)
8-11
NAPRTCS 2005
Dialysis
EXHIBIT 8.7
BASELINE EDUCATION STATUS BY AGE
100 100
75
50
63
55
PD
HD
34
25
0
Full-time
17
Part-time
3
0
Home
Schooling
14
10
3
0
None
(Capable)
None
(Incapable)
75
76
PD
HD
50
53
31
25
11
5
7
5 4
4 5
0
Full-time Part-time Home
Schooling
None
(Capable)
None
(Incapable)
100
75
79
PD
HD
50
51
27
25
0
Full-time
8
6
9
5
10
2 3
Part-time Home
Schooling
None
(Capable)
None
(Incapable)
8-12
50
25
EXHIBIT 8.8
PERCENT FULL-TIME SCHOOL ATTENDANCE
PERITONEAL DIALYSIS HEMODIALYSIS
NAPRTCS 2005
Dialysis
100 White
Hispanic
Black
Other
75
83
85
72
83
86
81
77
78
85
85
84
80
83
90
73
100 100 White
Hispanic
Black
Other
75
50
47
56
44
62
49
55
38
67
48
54
39
65
41
50
32
77
25
0
6 Months 12 Months 24 Months 36 Months
100
6-12
82
81
75
> 12
85
80
85
84
89
74
50
25
0
6 Months 12 Months 24 Months 36 Months
100
6-12 > 12
75
50 50
51
56
48
57
45
52
42
25
0
6 Months 12 Months 24 Months 36 Months
0
6 Months 12 Months 24 Months 36 Months
8-13
NAPRTCS 2005
Dialysis
EXHIBIT 8.9
PERCENT PATIENT SURVIVAL BY AGE AT DIALYSIS INITIATION
100
90
80
70
60
50
0
0-1
2-5
6-12
>12
12 48 24
MONTHS
36 60
8-14
NAPRTCS 2005
Dialysis
EXHIBIT 8.10
CAUSES OF DEATH FOLLOWING THE INDEX COURSE OF DIALYSIS
Age at Dialysis Initiation
Total 0-1 2-5 6-12 >12
N % N % N % N % N %
Viral infection
Bacterial infection
Disease recurrence
Dialysis-related
13
49 11.8 23 16.5
Other infection 31
Cancer / Malignancy 29
4
3.1
7.5
7.0
2
11
5
1.0 1
1.4
7.9
3.6
1 2.0
5 10.2
3 6.1
7 14.3
9 18.4
1 2.0
--0.7
2 4.1
35 36.7
3 6.1
8
10
7
7
1
6.3
6.3
7.1
8.9
3
14
9
7
2.6
12.1
7.8
6.0
18.8 24.1
0.9 2
4.3
1.7
4.3
32 24.1
12 12.9
8-15
NAPRTCS 2005
Dialysis
SECTION 9: DIALYSIS ACCESS DATA
Exhibit 9.1A presents information on modality initiations and terminations of patients whose index courses (i.e., first reported to NAPRTCS) were initiated after January 1, 1992. Data are shown for
6,318 courses of dialysis therapy. Index courses comprise about 77.6% of available data; 59.6% of courses are PD. Seventy-three percent (4,618/6,318) of index cases have been terminated. The majority of dialysis courses terminations are due to patient transplantation (64.4%), or due to a change of modality (22.3%). When change of modality is the reason for termination, excessive infection and patient or family choice are the primary reasons. Access failure is the reason for change in about 10.3% of such cases. Exhibit 9.1B shows termination reasons by vintage.
A summary of peritoneal dialysis access information is shown in Exhibits 9.2A. Peritoneal dialysis access by vintage is shown in Exhibit 9.2B. Most catheters were of the Tenckhoff curled (63.3%) or
Tenckhoff straight (28.6%) configuration; among all dialysis initiations, Tenckhoff curled catheters were used about twice as often as Tenckhoff straight. About 56.1% of catheters had single cuffs,
72.2% had a straight tunnel, and 43.5% of the exit sites had a lateral orientation. The most prevalent combinations of PD access characteristics are shown in Exhibit 9.3 for index cases. In fact, the most frequently occurring combination (15.8%) consisted of a curled catheter with a single cuff, straight tunnel with a lateral exit site.
Data on 2,507 hemodialysis (HD) access locations and devices are shown in Exhibit 9.4A. HD access devices include external percutaneous catheters (1,978 or 78.9%), external arteriovenous shunts (8 or 0.3%), internal arteriovenous fistulae (309 or 12.3%), and internal arteriovenous grafts
(212 or 8.5%). Most of 1,978 percutaneous catheter accesses were in the subclavian vein (60.8%), followed by the jugular (33.4%) and femoral (4.1%) veins. HD access devices by vintage are shown in Exhibit 9.4B.
Exhibit 9.5 provides details of the current status of the 6,318 accesses, as of database closure
(December 15, 2004) for this report. Overall, there are 1,700 cases (26.9%) of ongoing dialysis therapy and 4,618 terminations. As a percent of all accesses, the terminations are due to patient transplant (2,976 or 47.1%), change of modality (1,030 or 16.3%), and other reasons (612 or 9.7%).
The percent of patients terminated for transplant, by age, ranges from 40.7% for infants to 55.2% for children between the ages of 2 and 5 years. Reasons for the 1,030 changes of modality include
(Exhibit 9.6) excessive infection (28%), patient/family choice (22%), access failure (10%), other medical (23%), and other non-medical (16%). Whereas changes of modality due to excessive
9-1
NAPRTCS 2005
Dialysis infection occur primarily with PD accesses, changes due to patient or family choice occur primarily with HD accesses. Within modality type, modality change caused by access failure is significantly more common in black patients and female patients.
Patients are maintained on their index course of dialysis as follows: 10.2% ± 0.4% terminate by 3 months, 21.3% ± 0.5% by 6 months, 38.9% ± 0.6% by 12 months, 62.2% ± 0.6% by 24 months, and
75.8% ± 0.6% by 36 months. Exhibit 9.7 depicts time to index dialysis termination for all reasons, by modality. Although time to termination is shorter for HD (relative to PD) courses initially
(27.5% ± 0.9% vs. 17.1% ± 0.6% at 6 months), by 36 months of follow-up PD courses have a higher percent of terminations than HD (77.1% ± 0.7% PD vs. 73.5% ± 1.0% HD). Time to dialysis termination, by age and race, are shown for each modality in Exhibit 9.8. Adolescents (age >12) tend to remain on dialysis longer than the younger children, and white patients tend to terminate dialysis sooner, particularly among HD.
Exhibit 9.9 shows time to dialysis termination for PD catheter characteristics; similar data for HD catheter access are shown in Exhibit 9.10. Dialysis courses for HD patients with an external percutaneous catheter terminate much sooner than for arteriovenous fistulae or grafts. By 3 months, 14.7% ± 1.0% of percutaneous catheter accesses have terminated, compared to
6.4% ± 1.7% for AV fistulae and 1.4% ± 1.0% for AV grafts. By 24 months, comparable percents are
65.4% ± 1.5%, 44.9
± 0.4%, and 50.0
± 4.5%.
Exhibit 9.11 shows time to termination, according to reason. If the reason for termination was that the patient was transplanted, then the relationship between PD and HD terminations is similar.
However for patients who terminate their index dialysis to change modalities, HD patients experience most of their terminations in the first 6 months while PD patients appear to have a slow and steady increase in terminations over time.
To compare experience of PD patients with different procedure type, 2,598 index dialysis courses initiated between 1992 and 2004 were selected. To capture the PD procedure information, we only include patients who had submitted their Day 30 post dialysis forms where modality information was collected. There were a total of 639 (54% males, 38% white and 25% under 6 years of age) patients with CAPD and 1959 (56% male, 58% white and 33% under 6 years of age) patients with
APD at Day 30 post-dialysis. Compared to patients who used APD, those who used CAPD were significantly older when they initiated dialysis (p<0.001) and were significantly more likely to have a
9-2
NAPRTCS 2005
Dialysis minority ethnic background (p<0.001) (see Exhibit 9.12). Moreover, the majority of patients stayed in the initial procedure through their PD dialysis course: 79.8% and 92.7% of Day 30 modality stayed in CAPD and APD, respectively, throughout their whole index dialysis course or till the latest visit. Patient survival of these 2 groups did not differ.
A higher percentage of patients terminated dialysis due to transplantation in CAPD group (74.7%) than in APD group (66.2%) (p=0.002) while terminations were more likely due to change of modality in APD group (20.4%) than in CAPD group (13.6%). In general, time to termination for all reasons in CAPD vs. APD patients was significantly different (p=0.019, Exhibit 9.13). Time to termination due to transplantation differed (p<0.001, Exhibit 9.14) while time to termination due to change of modality was also significantly different (p=0.022).
Peritonitis exposure in patients in the APD group was significantly better than those of the CAPD group (p=0.025), as shown in Exhibit 9.15. Median time to first peritonitis episode in CAPD patients was 457 days compared to 583 days for APD patients. At 1 year post initiation, 45.8% of CAPD patients had experienced peritonitis compared to 40.9% of APD patients.
9-3
NAPRTCS 2005
Dialysis
EXHIBIT 9.1A
MODALITY INITIATION AND TERMINATION*
N
(6318)
Dialysis Course
%
(100)
Fifth or more
Modality
TERMINATIONS
Patient transplanted
Change of modality
Native kidney function returned
Administrative closure
Excessive infection
Patient/family choice
Access failure
Inadequate ultra-filtration
Inadequate solute clearance
Excessive hospitalization (dialysis-related)
Other (medical)
Other (non-medical)
*Dialysis initiated after January 1, 1992
9-4
37 0.6
64.5
22.3
2.6
0.0
28.4
21.9
10.3
4.9
2.1
2.0
14.1
16.2
2976
1030
122
1
293
226
106
50
22
21
145
167
9-5
NAPRTCS 2005
Dialysis
NAPRTCS 2005
Dialysis
EXHIBIT 9.2A
PERITONEAL DIALYSIS ACCESS
N
(4182)
%
(100)
Catheter
Tenckhoff straight
Tenckhoff curled
Toronto western
1194
2647
33
28.6
63.3
0.8
Cuffs
Tunnel
Swan neck/curved
Exit Site Orientation
1161 27.8
9-6
NAPRTCS 2005
Dialysis
EXHIBIT 9.2B
PERITONEAL ACCESS DATA BY VINTAGE
% % % % %
1998
2000
2002 16.0 74.6 1.4 4.2 3.8
9-7
NAPRTCS 2005
Dialysis
EXHIBIT 9.3
CATHETER CHARACTERISTICS FOR PERITONEAL DIALYSIS ACCESSES
Catheter Cuffs
N
2005
(7796)
%
(100)
Curled One Straight Lateral 657 15.8
Curled One Straight Lateral 553 15.3
Swan Down 303 8.4
Curled Two Straight Lateral 302 8.3
Curled Two Straight Lateral 337 8.1
Straight One Straight Lateral 315 7.6
Swan Down 311 7.5
Straight One Straight Lateral 260 7.2
Curled Two Straight Down 294 7.0
Curled Two Straight Down 252 7.0
Curled One Straight Down 277 6.6
Curled One Straight Down 238 6.6
Curled One Straight Up 188 5.2
Curled One Straight
Straight One Straight
Up 206 4.9
Up 159 3.8
Straight One Straight Up 126 3.5
Swan Down 122 3.4
Straight Two Straight Lateral 126 3.0
Swan Down 126 3.0
Straight One Straight Unknown
Straight One Straight Unknown
107 3.0
121 2.9
Straight Two Straight Lateral 98 2.7
Swan Lateral 95 2.6
Straight One Straight Down 103 2.5
Straight One Straight Down 91 2.5
Other
Combinations*
*Includes all combinations <2.5%
9-8
EXHIBIT 9.4A
HEMODIALYSIS ACCESS
N
(2507)
%
(100)
Subclavian vein
Jugular vein
Femoral vein
Single lumen
Double lumen
Autologous vein
Bovine graft
PTFE graft
Other graft
Locations of Shunts, Fistulae, and Grafts
Upper arm
Lower arm
1203
661
81
64
1881
7
1
194
6
152
36
97
100.0
6.8
18.3
NAPRTCS 2005
Dialysis
9-9
NAPRTCS 2005
Dialysis
1999
2000
2001
2002
2003
2004
All
1992
1993
1994
1995
1996
1997
1998
EXHIBIT 9.4B
HEMODIALYSIS ACCESS DATA BY VINTAGE
External PQ
Catheter
External AV
Shunt
Internal AV
Fistula
Internal AV
Graft
%
85.0
83.1
86.3
74.8
75.6
69.3
78.9
59.7
76.0
72.6
76.4
80.5
78.0
84.6
%
0
2.3
0.32
0
0
0
0
0.6
0.9
0.4
0.7
0
0
0.4
%
11.7
9.3
9.0
21.5
18.9
19.3
12.3
21.1
12.2
14.2
11.1
10.9
12.8
8.9
%
3.4
7.6
4.7
3.7
5.6
9.1
8.5
18.6
10.9
12.8
11.8
8.6
9.2
6.1
N
219
208
189
119
89
43
2507
181
205
213
275
273
266
227
9-10
EXHIBIT 9.5
FREQUENCY DISTRIBUTION OF DIALYSIS ACCESS STATUS,
BY SELECTED CHARACTERISTICS
NAPRTCS 2005
Dialysis
Working
Access
Access Terminated
Patient
Transplanted
Change of
Modality Other
Modality
Hemodialysis
Year
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
Age
0-1
2-5
6-12
>12
Gender
Male
Female
Race
White
Black
Hispanic
Other
2549 819 32.1 1097 43.0 424 16.6 209 8.2
518 82 15.8 275 53.1 98 18.9 63 12.2
565 59 10.4 312 55.2 122 21.6 72 12.7
590 97 16.4 304 51.5 111 18.8 78 13.2
670 101 15.1 348 51.9 144 21.5 77 11.5
680 130 19.1 325 47.8 145 21.3 80 11.8
645 176 27.3 313 48.5 94 14.6 62 9.6
524 146 27.9 254 48.5 81 15.5 43 8.2
525 162 30.9 247 47.0 70 13.3 46 8.8
476 164 34.5 219 46.0 60 12.6 33 6.9
431 153 35.5 198 45.9 52 12.1 28 6.5
339 170 50.1 118 34.8 36 10.6 15 4.4
114 97 85.1 11 9.6 3 2.6 3 2.6
760 146 19.2 309 40.7 133 17.5 172 22.6
701 121 17.3 387 55.2 119 17.0 74 10.6
1913 404 21.1 1034 54.1 316 16.5 159 8.3
2944 1029 35.0 1246 42.3 462 15.7 207 7.0
3454 905 26.2 1699 49.2 517 15.0 333 9.6
2864 795 27.8 1277 44.6 513 17.9 279 9.7
3068 686 22.4 1606 52.3 482 15.7 294 9.6
1538 522 33.9 596 38.8 260 16.9 160 10.4
1310 383 29.2 589 45.0 221 16.9 117 8.9
402 109 27.1 185 46.0 67 16.7 41 10.2
9-11
NAPRTCS 2005
Dialysis
EXHIBIT 9.6
REASONS FOR CHANGE OF MODALITY, BY SELECTED CHARACTERISTICS
Reasons (%) for Changes of Modality
Excessive
Infection
Patient/
Family
Choice
Access
Failure
Other
Medical
Other
Non-
Medical/
None
Total Changes of
Modality
Modality
PD
HD
Initiation Age
0-1
2-5
6-12
>12
Gender
Male
Female
Race
White
Black
Hispanic
Other
9-12
NAPRTCS 2005
Dialysis
40
20
0
0
100
80
60
EXHIBIT 9.7
TIME TO DIALYSIS TERMINATION FOR INDEX CASES
12
MONTHS
24
9-13
PD
HD
36
NAPRTCS 2005
Dialysis
EXHIBIT 9.8
TIME TO DIALYSIS TERMINATION FOR INDEX CASES,
BY AGE AND RACE/ETHNICITY
PERITONEAL DIALYSIS HEMODIALYSIS
100 100
80
80
60
60
40 40
20
0-1
2-5
6-12
>12
20
0
0 12
MONTHS
24 36
0
0 12
MONTHS
24
100 100
0-1
2-5
6-12
>12
36
80 80
60 60
40 40
20
White
Black
Hispanic
Other
20
White
Black
Hispanic
Other
0
0 12
MONTHS
24 36
0
0 12
MONTHS
24 36
9-14
100
80
60
40
20
0
0
60
40
20
0
0
100
80
NAPRTCS 2005
Dialysis
EXHIBIT 9.9
TIME TO DIALYSIS TERMINATION FOR INDEX CASES,
BY PD CATHETER CHARACTERISTICS
CATHETER TYPE NUMBER OF CUFFS
100
80
60
40
20
12
MONTHS
TUNNEL
24
Tenckhoff Straight
Tenckhoff Curled
Other
36
100
0
0 12 24
MONTHS
EXIT SITE ORIENTATION
One
Two
36
20
12
MONTHS
24
Swan Neck
Straight
36
0
0
80
60
40
12
MONTHS
24
Up
Down
Lateral
Unknown
36
9-15
60
40
20
0
0
NAPRTCS 2005
Dialysis
100
EXHIBIT 9.10
TIME TO DIALYSIS TERMINATION FOR INDEX CASES, BY HD ACCESS
Percutaneous cathether
Arteriovenous fistula
Arteriovenous graft
80
12
MONTHS
24
9-16
36
EXHIBIT 9.11
TIME TO DIALYSIS TERMINATION FOR INDEX CASES,
BY REASON FOR TERMINATION
PATIENT TRANSPLANTED
100
PD
HD
80
NAPRTCS 2005
Dialysis
60
40
20
100
0
0
PD
HD
12 24
MONTHS
CHANGE OF MODALITY
80
36
60
40
20
0
0 12
MONTHS
9-17
24 36
NAPRTCS 2005
Dialysis
EXHIBIT 9.12
SELECTED CAPD AND APD PATIENTS DEMOGRAPHICS
CAPD APD
N % N %
Race
38 58
6 6
Gender
Initiation Age
Dialysis Initiation Year
9-18
40
20
0
0
NAPRTCS 2005
Dialysis
EXHIBIT 9.13
TIME TO DIALYSIS TERMINATION FOR SELECTED CAPD/APD CASES, BY MODALITY
100
CAPD
APD
80
60
12
MONTHS
24
9-19
36
NAPRTCS 2005
Dialysis
EXHIBIT 9.14
TIME TO TRANSPLANTATION AND CHANGE OF MODALITY FOR
SELECTED CAPD/APD CASES, BY MODALITY
PATIENT TRANSPLANTED
100
80
CAPD
APD
60
40
20
0
0
20
0
0 12 24
MONTHS
CHANGE OF MODALITY
100
80
CAPD
APD
60
40
12
MONTHS
9-20
24
36
36
40
20
0
0
NAPRTCS 2005
Dialysis
EXHIBIT 9.15
TIME TO FIRST PERITONITIS EPISODE FOR SELECTED CAPD/APD CASES,
BY MODALITY
100
CAPD
APD
80
60
6 24 12
MONTHS
18 30
9-21
NAPRTCS 2005
Dialysis
SECTION 10: ERYTHROPOIETIN USE IN DIALYSIS PATIENTS
Data on the use of erythropoietin (EPO) are presented in this section. The cohort of interest is the
6,318 cases of maintenance dialysis, as described in the preceding section, for which the index course of dialysis was initiated after January 1, 1992. [Recall that these cases are composed of
4,902 index courses of dialysis, 1,007 persons who had exactly two courses, and 409 individuals who had at least three courses (see Exhibit 9.1)]. In particular, we evaluate herein the use of EPO following the reported index initiation of dialysis for these 4,902 patients.
The percent use of EPO across time (during the first course of dialysis) is described in Exhibit 10.1 for patients with complete follow-up and non-missing data at the post dialysis initiation times shown.
The use of EPO increases from 88% at baseline (Day 30) to 94.7% after two years of dialysis.
While EPO use is a bit lower initially for peritoneal dialysis (PD) patients (86.7%) compared to hemodialysis (HD) patients (92.4%), by two years of dialysis therapy, EPO use in similar (94.6% for
PD and 94.7% for HD). EPO use at baseline, by patient age, gender, and race/ethnicity is depicted in Exhibit 10.2. Overall, EPO is used similarly among the age groups, with 88.8%, 89.8%, 88.5%, and 88.4% of patients, respectively, in age groups 0-1, 2-5, 6-12, and >12 receiving EPO therapy initially. Since about 90% of infants and toddlers (<6 years old) are treated with peritoneal dialysis, data are sparse regarding EPO usage patterns among HD patients in this age group. Among older children and adolescents, initial use of EPO is 6 to 8 percentage points higher for HD relative to PD patients (Exhibit 10.2). EPO usage patterns, by gender, are similar within dialysis modality group.
Hispanic PD patients receive EPO therapy less frequently than their HD counterparts (79.9% vs.
93%).
Of those treated with EPO therapy, data pertaining to route and frequency of use are described in
Exhibit 10.3. As shown, most PD patients (95.8%) receive subcutaneous administration, whereas most HD patients are treated intravenously (85.3%). Although less than 2% of PD receive intraperitoneal administration of EPO, frequency of EPO administration is more varied among PD than HD. About 72% of PD patients are treated once or twice weekly, and about 22% are treated three times per week. The percentage of PD patients who are treated less frequently than once per week increased from 3.0% initially to 6% at 12 months, and remains stable afterwards. HD patients, however, are mostly treated three times per week, presumably at the time of their dialysis therapy.
Over time, 87.3% or more of EPO-treated patients receive Epogen.
10-1
NAPRTCS 2005
Dialysis
EPO dosing was examined in units per kilogram per week (Exhibit 10.4). As Exhibit 10.4 suggests, mean doses for the younger patients (<24 months, 2-5 years) tend to fluctuate. However, mean doses for the older patients (6-12, >12) remain more stable over time. Moreover, mean doses of different gender, race, and dialysis modality groups are similar and remain stable overtime.
To assess more clearly the usage and potential effect of EPO therapy on hematocrit, we considered
3,009 patients still maintained on their index course of dialysis at 6 months. By year of dialysis initiation, the percent use of EPO is increasing from 85.1% in 1992, 93.9% in 1997, to 95.5% in
2004. Frequency of EPO administration, by dialysis modality and patient age at initiation, is shown in Exhibit 10.5. Frequency of administration is slightly greater for infants receiving PD therapy, relative to older PD patients. Of these 3009 patients, we have complete reporting on EPO use and hematocrit at the baseline and 6-month post dialysis initiation visits for 2,644. The percent distribution of hematocrit at 6 months, by EPO use, is shown in Exhibit 10.6. Of the 2,644 patients,
2,355 (93.2%) began EPO therapy by Day 30, 172 (7.3%) began EPO therapy after Day 30, and
117 (5%) had not received EPO through 6 months of dialysis therapy. Of patients who began EPO therapy by Day 30, 50% had a hematocrit level of 33% or above at 6 months. Thirty-seven percent of patients not treated by EPO during the first 6 months of dialysis had hematocrit levels of 33% or above at 6 months. Mean and median hematocrit levels at 6 months are shown in Exhibit 10.7 by
EPO use.
10-2
EXHIBIT 10.1
PERCENT EPO USE, BY MONTHS ON DIALYSIS
[NUMBER AT TOP OF BAR IS SUBGROUP SAMPLE SIZE]
ALL PATIENTS
NAPRTCS 2005
Dialysis
100
4050
3013
1966 1290 842 556 374
80
60
40
20
60
40
0
1 6 12 18 24 30 36
DIALYSIS MODALITY
100
2691
2119
1379 897 558 365 240
1355
890 585 391 283 191 134
80
20
0
1 6 12 18 24 30 36
PD
1 6 12 18 24 30 36
HD
10-3
NAPRTCS 2005
Dialysis
EXHIBIT 10.2
PERCENT EPO USE AT BASELINE (DAY 30)
[NUMBER AT TOP OF BAR IS SUBGROUP SAMPLE SIZE]
AGE GENDER
100 0-1
6-12
2-5
>12
518 333
852 988 33
97
424
801
100
1488 1201
80
80
751
604
60
60
40
40
20
20
0
PD HD
RACE/ETHNICITY
100
80
1430
532
563
166
554 441 257
103
0
M F
PD
M F
HD
60
40
20
0
W B H O
PD
W B H O
HD
10-4
100
EXHIBIT 10.3
ROUTE AND FREQUENCY OF EPO ADMINISTRATIONS
PERITONEAL DIALYSIS HEMODIALYSIS
NAPRTCS 2005
Dialysis
SubQ IP IV 100
SubQ IP IV
80 80
60 60
40 40
20 20
0
100
QD
1-Mo 6-Mo 12-Mo
EPO FREQUENCY
TIW BIW QW
24-Mo
>QW
0
100
QD
1-Mo 6-Mo 12-Mo
EPO FREQUENCY
TIW BIW QW
24-Mo
>QW
80 80
60 60
40 40
20 20
0
1-Mo 6-Mo 12-Mo 24-Mo
0
1-Mo
10-5
6-Mo 12-Mo 24-Mo
500
400
300
200
100
0
1
NAPRTCS 2005
Dialysis
EXHIBIT 10.4
MEAN EPO DOSE (UNITS/KG/WEEK)
DIALYSIS MODALITY AGE
500 500
400
PD
HD
400
0-1
2-5
6-12
>12
300 300
200 200
100
0
1 6 12 18
FOLLOW-UP MONTH
24
RACE
White
Black
Hispanic
Other
100
30
0
1
500
400
300
200
100
6 12 18
FOLLOW-UP MONTH
24
GENDER
Male
Female
6 12 18
FOLLOW-UP MONTH
24 30
10-6
0
1 6 12 18
FOLLOW-UP MONTH
24
30
30
NAPRTCS 2005
Dialysis
EXHIBIT 10.5
EPO FREQUENCY (%) AT 6 MONTHS, BY MODALITY AND AGE AT DIALYSIS INITIATION
0-1
Peritoneal dialysis
2-5 6-12 >12 0-1
Hemodialysis
2-5 6-12 >12
EPO
Daily
Three times/week
2
24
0
18
0
16
0
16
4
81
0
74
0
73
0
75
Two times/week
Weekly
<Weekly
37
33
36
40
35
42
32
45
11
4
19
6
22
5
5 5 6
EXHIBIT 10.6
7 0 1
DISTRIBUTION OF HEMATOCRIT AT 6 MONTHS, BY EPO USE
0
18
6
1
EPO Use
Hematocrit (%)
N 1 < ≥ 35
Began EPO by Day 30
Began EPO after Day 30
2355
172
16
20
21
27
14
9
15
12
35
31
117 25 20 19 9 28
1 EPO status reported at both day 30 and 6 months
EXHIBIT 10.7
MEAN AND MEDIAN HEMATOCRIT LEVELS AT 6 MONTHS, BY EPO USE
EPO Use
Began EPO by Day 30
Began EPO after Day 30
No EPO
N
2355
172
117
Mean
32.3
31.3
30.9
Median
32.7
31.0
31.0
SE
0.1
0.5
0.6
10-7
NAPRTCS 2005
Dialysis
SECTION 11: DIALYSIS FOLLOW-UP
Follow-up data on peritoneal dialysis and hemodialysis initiations are presented in this section. We consider only those courses of dialysis for which we have the actual start date (i.e., initiation date after January 1, 1992).
Exhibit 11.1 presents follow-up data at 1 month and at 6, 12, 24, and 36 months following PD initiation. Most patients used automated peritoneal dialysis (APD) [67.8% at 1 month, 72.7% at 36 months] rather than continuous ambulatory peritoneal dialysis (CAPD) or intermittent peritoneal dialysis (IPD). At one month post-initiation, 86.3% of patients were receiving erythropoietin (EPO) and 9.7% were receiving human growth hormone (rhGH); at 6 months, 90.8% were receiving EPO and 14.2% rhGH; at 36 months, 90.8% EPO and 22.4% rhGH. Exit site infections occurred in about
22% of cases between 6-month follow-up visits. Transplant status is also characterized: at 6 months post initiation, 24.8% of patients were on the cadaver waiting list and 31.6% had a CD or
LD work-up in progress. Of the 42.1% of patients who were not transplant candidates at 6 months
72% had a medical reason for remaining on dialysis and 28% were due to family or patient preference. By 12 months, 32.1% of patients were on the cadaver list and 27.3% had a work-up in progress.
Also shown is the number of reported peritonitis episodes. During the first 30 days of PD, 463 patients had a peritonitis episode, and 50 of these patients had two episodes. Of the 513 reported infections that occurred within the first month, 15 (2.9%) were fungal, 228 (44.4%) were Grampositive, and 101 (19.7%) were Gram-negative. Exhibit 11.2 presents number and percent of peritonitis episodes, by age at dialysis initiation. Over the course of the study, 3,744 peritonitis infections have been reported in this cohort of PD patients: 747 patients have had only 1 infection,
372 patients have had two infections, 434 patients have had 3 to 7 infections, and 46 patients have had at least 8.
Peritonitis infection rates, by age and catheter characteristics, are presented in Exhibit 11.3. A total of 3,744 episodes of peritonitis have occurred in 5,117 years of follow-up (3,875 PD patients), yielding an annualized rate of 0.73, or 1 episode every 16 months. The annualized rate decreases with age, and is better for double cuffs, swan neck tunnels, and downward pointed exit sites. The percentage of patients using the double cuffs/swan neck/downward pointed exit site configuration increased from 5% in 1992-1995 to 17.4% since then.
11-1
NAPRTCS 2005
Dialysis
Time to first peritonitis infection is depicted in Exhibits 11.4, 11.5, and 11.6. Shown are time to first infection for all new index PD courses (Exhibit 11.4), by age at initiation (Exhibit 11.5), and by catheter access characteristics (Exhibit 11.6). Overall, 42% of patients have had at least one infection by 12 months; 56% have had an infection by 24 months. Tenckhoff straight and Tenckhoff curled catheters have similar times to first peritonitis infection. Overall, the time to first peritonitis infection is longer for two cuffs compared to one, for swan neck tunnels compared to straight tunnels, and for down exit sites compared to up, lateral, or unknown exit sites.
Data on PD catheter access revisions are shown in Exhibit 11.7. The revision access ratio (number of revisions / number of accesses) is 0.21. In those cases where a reason was specified, accesses were revised due to catheter malfunction (44%), peritonitis (18%), exit site tunnel infections (20%), and dialysate leaks (4%). Percent distributions of reasons for access revisions are also shown according to catheter access characteristics. Recall that the most common access configuration is a Tenckhoff curled catheter with one cuff, a straight tunnel, and a lateral exit site orientation.
Follow-up data on HD patients and accesses are shown in Exhibit 11.8 and Exhibit 11.9. The use of EPO in HD patients exceeds that of PD patients for the first year of dialysis, but is about 87% at
24 months for both groups. On the other hand, the use of rhGH is less in HD than in PD. The transplant status of HD patients is similar to that observed for the PD cohort. The revision access ratio for HD is 2.57. In those cases where a reason was specified, accesses were revised because of infection (15%), clotting (26%), malfunction (25%), and to create a more permanent access
(25%).
For patients who were placed on the cadaver waiting list at dialysis initiation, Exhibits 11.10 and
11.11 show the time to cadaver transplantation by year listed and by age when listed, respectively.
In 2003, NAPRTCS initiated collection of dialysis dose measurements with capture, at each reporting time point of most recent single pool Kt/V and Urea Reduction Ratio (URR) for hemodialysis patients and most recent weekly Kt/V for peritoneal dialysis patients. Exhibit 11.12 displays initial reported Kt/V by age grouping, race, visit timing since initiation and baseline BMI standardized score for 258 peritoneal dialysis and 173 hemodialysis patients. Within modality, dialysis dose is similar in all subgroups except for a trend (p=0.014) towards higher peritoneal dialysis dose in non-black patients. Thus dose appears to be delivered similarly across multiple subgroups. For peritoneal dialysis the median Kt/V was 2.2, the lower quartile was 1.7 and the lowest decile was 1.3. Peritoneal dialysis strategies (CAPD vs. APD vs. IPD) did not differ
11-2
NAPRTCS 2005 significantly in Kt/V values but the 7 IPD patients had a mean of 1.7. Kt/V percentiles( 50 th
Dialysis
, 25 th and
10 th ) for hemodialysis patients are 1.7, 1.3 and 1.1.
Mean URR values for selected hemodialysis patient subgroups are presented in Exhibit 11.13. As with Kt/V statistically significant differences between the subgroups are not detected. For the 153 hemodialysis cases with both measures, a strong rank correlation was observed (r=0.85, p<0.001) between Kt/V and URR values.
In addition, for patients with more than one Kt/V measurement, the mean of the first reported Kt/V was compared with the mean of their second Kt/V. This was performed separately for both hemodialysis and peritoneal dialysis patients. Results indicated no significant difference in mean values for either HD or the PD groups (p=0.612 HD, p=0.946 PD).
Among HD patients with more than one URR measurement, the mean of the first reported URR was compared with the mean of the second reported URR measurement. The average difference in values was –2.56 and was of borderline statistical significance (p=0.070).
11-3
NAPRTCS 2005
Dialysis
EXHIBIT 11.1
PERITONEAL DIALYSIS AT FOLLOW-UP
1 Month 6 Months 12 Months 24 Months 36 Months
N % N % N % N % N %
Total 3313 100.0 2633 100.0 1770 100.0
741
Current Modality
CAPD 677 20.4
484 18.4
300 16.9
113
APD 2247 67.8 1850 70.3 1244 70.3
531
IPD 230 6.9
171 6.5
97 5.5
27
Missing/Unknown 159 4.8
128 4.9
129 7.3
70
Yes 2860 86.3 2392 90.8 1609 90.9
659
No 399 12.0
193 7.3
86 4.9
37
Missing/Unknown 54 1.6
48 1.8
75 4.2
45
Yes 322 9.7
373 14.2
338 19.1
190
No 2933 88.5 2207 83.8 1352 76.4
507
Missing/Unknown 58 1.8
53 2.0
80 4.5
44
Seizures
Yes 121 3.7
127 4.8
62 3.5
8 2.5
No 3105 93.7 2436 92.5 1615 91.2
661
Missing/Unknown 87 2.6
70 2.7
93 5.3
53
Yes 321 9.7
577 21.9
380 21.5
144
No 2886 87.1 1972 74.9 1288 72.8
544
Missing/Unknown 106 3.2
84 3.2
102 5.8
53
On Cadaver List 457 13.8
653 24.8
569 32.1
293 39.5
127 39.0
Workup in progress 1250 37.7
832 31.6
483 27.3
132 17.8
42 12.9
Medical reasons 1 1210 36.5
768 29.2
391 22.1
17.1
65 19.9
Family/patient preference 1 311 9.4
299 11.4
237 13.4
18.4
72 22.1
Missing/Unknown 85 2.6
81 3.1
90 5.1
53
0 2850 86.0 1863 70.8 1266 71.5
553
1 413 12.5
515 19.6
331 18.7
126
2 50 1.5
165 6.3
104 5.9
42
>2 --90 3.4
69 3.9
20
1 Demoninator is the number of patients who are not transplant candidates
11-4
NAPRTCS 2005
Dialysis
7
8
9
10
11
12
13
0
1
2
3
4
5
6
EXHIBIT 11.2
NUMBER AND PERCENT OF PERITONITIS EPISODES, BY AGE
[N = Number of episodes per sequence]
Total
Age at PD Initiation
0-1 2-5 6-12 >12
N % N % N % N % N %
2276 58.7
358 53.8
283 58.5
727 59.4 908 60.4
747 19.3
132 19.8
100 20.7
232 19.0 283 18.8
372 9.6
168 4.3
73
36
11.0
5.4
47
16
9.7
3.3
105 8.6 147
56 4.6 60
9.8
4.0
125 3.2
66 1.7
51 1.3
20
13
12
3.0
2.0
1.8
18
8
4
3.7
1.7
0.8
37 3.0 50
22 1.8 23
18 1.5 17
3.3
1.5
1.1
24 0.6
19 0.5
8 0.2
8 0.2
4 0.1
2 0.1
2 0.1
6
5
2
4
1
1
--
0.9
0.8
0.3
0.6
0.2
0.2
--
3
--
2
1
1
--
--
1
--
0.6
--
0.4
0.2
0.2
--
--
0.2
--
11-5
NAPRTCS 2005
Dialysis
EXHIBIT 11.3
PERITONITIS INFECTION RATES, BY AGE AND CATHETER CHARACTERISTICS
Number of Episodes
Years of Follow-up
Annualized
Rate*
Expected Months
Between Infections*
Total
Age
0-1
2-5
6-12
>12
Catheter
Tenckhoff straight
Tenckhoff curled
Toronto western
Cuffs
One
Two
3744
799
452
1200
1293
1060
2373
224
2341
1352
5117
864
624
1659
1970
1374
3182
412
2841
2164
0.73 (0.71, 0.76) 16.4 (15.8, 16.9)
0.92 (0.86, 0.99) 13.0 (12.1, 13.9)
0.72 (0.66, 0.79) 16.7 (15.2, 18.2)
0.72 (0.68, 0.77) 16.7 (15.6, 17.5)
0.66 (0.62, 0.69) 18.2 (17.4, 19.2)
0.77 (0.73, 0.82) 15.6 (14.7, 16.4)
0.75 (0.72, 0.78) 16.0 (15.4, 16.7)
0.54 (0.47, 0.62) 22.2 (19.2, 25.6)
0.82 (0.79, 0.86) 14.7 (13.9, 15.2)
0.62 (0.59, 0.66) 19.3 (18.2, 20.4)
Tunnel
Swan neck or curved
Straight
Exit site orientation
Up
Down
Lateral
Unknown
857
2817
666
1031
1664
383
1447
3511
744
1670
2058
644
0.59 (0.55, 0.63)
0.80 (0.77, 0.83)
0.90 (0.83, 0.97)
0.62 (0.58, 0.66)
0.81 (0.77, 0.85)
0.59 (0.53, 0.66)
20.3 (19.0, 21.8)
15.0 (14.5, 15.6)
13.3 (12.3, 14.5)
19.4 (18.2, 20.8)
14.8 (14.1, 15.6)
20.4 (18.2, 22.7)
Transplant year
1997 – 2004 1995 2798 0.71 (0.68, 0.74) 16.9 (16.1, 17.5)
<1997 1749 2319 0.75 (0.71, 0.79) 16.0 (15.2, 16.9)
*Lower and upper limits of the 95% confidence interval are provided in the parentheses.
11-6
EXHIBIT 11.4
TIME TO FIRST PERITONITIS INFECTION
100
80
60
40
20
0
0 6 12 18 24 30
MONTHS
EXHIBIT 11.5
TIME TO FIRST PERITONITIS INFECTION,
BY AGE AT PERITONEAL DIALYSIS INITIATION
100
80
0-1
2-5
6-12
13-17
60
40
20
0
0 6 24 12 18
MONTHS
11-7
30
NAPRTCS 2005
Dialysis
40
20
0
0
NAPRTCS 2005
Dialysis
100
80
EXHIBIT 11.6
TIME TO FIRST PERITONITIS INFECTION,
BY CATHETER ACCESS CHARACTERISTICS
CATHETER TYPE NUMBER OF CUFFS
100
One
Two
Tenckhoff straight
Tenckhoff curled
Other
80
60 60
40 40
20
100
0
0 6 12
MONTHS
18
TUNNEL TYPE
Swan neck
Straight
80
24
60
6 12
MONTHS
18 24
20
30
0
0
100
6 12
MONTHS
18
EXIT SITE ORIENTATION
24
Up
Down
Lateral
Unknown
80
60
30
0
0
11-8
40
20
6 12
MONTHS
18 24
30
30
NAPRTCS 2005
Dialysis
40
20
0
0
EXHIBIT 11.6 (Continued)
TIME TO FIRST PERITONITIS INFECTION,
BY CATHETER ACCESS CHARACTERISTICS
100
Other strategies
2 Cuffs, Swan Neck, Downward
80
60
6 12
MONTHS
18 24 30
11-9
NAPRTCS 2005
Dialysis
11-10
EXHIBIT 11.8
HEMODIALYSIS AT FOLLOW-UP
1 Month 6 Months 12 Months 24 Months 36 Months
N % N % N % N % N %
Total 2094 100.0 1447 100.0 1000 100.0
509 100.0
EPO Therapy
Yes 1899 90.7 1315 90.9
905 90.5
444 87.2
No 124 5.9
58 4.0
39 3.9
23 4.5
Missing 71 3.4
74 5.1
56 5.6
42 8.3
Human Growth Hormone Therapy
Yes 200 9.6
158 10.9
122 12.2
74 14.5
No 1819 86.9 1214 83.9
820 82.0
392 77.0
Missing 75 3.6
75 5.2
58 5.8
43 8.4
Seizures
Yes 101 4.8
113 7.8
56 5.6
28 5.5
No 1895 90.5 1233 85.2
856 85.6
430 84.5
Unknown 24 1.1
20 1.4
20 2.0
5 1.0
Missing 74 3.5
81 5.6
68 6.8
46 9.0
Exit Site Infections
Yes 201 9.6
244 16.9
137 13.7
50 9.8
No 1766 84.3 1082 74.8
770 77.0
402 79.0
Missing 127 6.1
121 8.4
93 9.3
57 11.2
Transplant status
CD waiting list 310 14.8
419 29.0
374 37.4
229 45.0 111 43.7
CD or LD work-up in progress 773 36.9
379 26.2
188 18.8
62 12.2 25 9.8
Medical reason 1 729 34.8
389 26.9
249 24.9
102 20.0
Family/patient preference 1 194 9.3
162 11.2
118 11.8
33 13.0
Missing 88 4.2
98 6.8
71 7.1
52 10.2
1 Demoninator is the number of patients who are not transplant candidates
11-11
NAPRTCS 2005
Dialysis
NAPRTCS 2005
Dialysis
11-12
EXHIBIT 11.10
TIME TO CADAVER TRANSPLANTATION, BY ERA
100
90
80
70
60
50
50
40
30
20
10
0
0
90
80
70
60
40
30
20
10
<1999
1999-2004
0
0 1 2 3 4 5
Years
EXHIBIT 11.11
TIME TO CADAVER TRANSPLANTATION, BY AGE
100
1
0-1
2-5
6-12
>12
4 2
Years
11-13
3 5
NAPRTCS 2005
Dialysis
NAPRTCS 2005
Dialysis
EXHIBIT 11.12
KT/V BY MODALITY, AGE, RACE, VISIT AND BASELINE BMI
MODALITY
Peritoneal dialysis
KT/V
N Mean
Age
Race
Non-Black 200 2.5
Visit Month
Hemodialysis
BMI Z-score
Age
Race
Non-Black 93 1.7
Visit Month
BMI Z-score
11-14
NAPRTCS 2005
Dialysis
EXHIBIT 11.13
URR FOR HEMODIALYSIS PATIENTS BY AGE, RACE, VISIT AND BASELINE BMI
URR
N Mean SE
Age
Race
Visit Month
BMI Z-score
≤ 0 54 72.0 2.0
11-15
NAPRTCS 2005
Dialysis
SECTION 12: GROWTH
Data on growth following dialysis initiation are presented in this section. The first course of dialysis starting after January 1, 1992 is used for the baseline measurement and provides the reference value from which changes in height are calculated. Patients are censored from the analysis at the time of dialysis termination and do not re-enter, even if a subsequent course of dialysis is initiated.
As with transplant patients, height and weight measurements are reported at each 6-month followup visit, and baseline measurements are obtained 30 days following initiation. Z-scores are calculated by using the appropriate gender-age specific mean, standard deviation and adjustment parameters for the national population derived from NHANES III study (2000) of the National Center of Health Statistics. This is a change in standardization approaches for the registry, and direct comparison with prior reports is not possible because of the use of these new standards.
Exhibit 12.1 presents mean height scores, by selected characteristics and times after dialysis initiation. At baseline, patients are about 1.7 standard deviations below the appropriate age- and sex-adjusted height levels. Height deficits are worse for males and for younger patients. Patients were also stratified according to baseline Z-score (<–1.88 vs. ≥ –1.88 Z-score). Note that the third percentile of the population corresponds to –1.88 in Z-score. Post-dialysis height deficits for children with worse deficit score at baseline remain relatively constant, ranging from –3.22
± 0.03 at
1 month to –3.11
± 0.06 at 24 months. Children who had less deficit at baseline, –0.56
± 0.02, experience worse deficit by 24 months (–0.76
± 0.04). Changes from baseline in height deficit (i.e., delta Z-score) are 0.05
± 0.02 (n=943) and 0.07
± 0.05 (n=384) at 12 and 24 months, respectively, for patients whose baseline Z-score is ≥ –1.88. Comparatively, –0.11
± 0.03 (n=762) and –0.15
± 0.05
(n=344) are the delta Z-scores for patients with baseline Z-score <–1.88. Although the weight deficits of dialysis patients are not as severe as for height, patients are, on average, more than one standard deviation below normal in weight (Exhibit 12.2). Changes from baseline in height and weight Z-score are depicted graphically in Exhibit 12.3 (Panels A and B respectively). Note that the sample sizes at follow-up times are still relatively small, particularly for young dialysis patients.
Young patients (less than 6 years) gain weight Z-score relative to older children. In Exhibit 12.3
Panels C and D, height changes for peritoneal dialysis and hemodialysis patients are shown, respectively.
Growth for rhGH-treated and untreated dialysis patients by age is shown in Exhibit 12.4. Treated patients are patients who had consistently reported rhGH use at baseline, 6 months, and one year.
12-1
NAPRTCS 2005
Dialysis
Similarly, untreated patients are patients who had consistently reported no rhGH use at baseline, 6 months, and one year. There are 2 control groups, all untreated patients (all control) and those untreated patients whose baseline height Z-score was worse than –1.88 (short control). Treated patients in all age groups have improved height at one year. Non-infant patients have worse height deficits at one year than at baseline. However, height deficit of short control patients is more stable at one year compared to baseline, which may be due to regression to the mean. Infants in both untreated control groups exhibited some catch up growth in the first 6 months (0.55
± 0.13 in short control and 0.21
± 0.11 in all control groups).
12-2
NAPRTCS 2005
Dialysis
EXHIBIT 12.1
MEAN (SE) HEIGHT Z-SCORES, BY SELECTED CHARACTERISTICS
AND TIMES FOLLOWING DIALYSIS INITIATION
Month 1
(N=3910)
Month 6
(N=2647)
Month 12
(N=1705)
Month 24
(N=728)
N Mean SE N Mean SE N Mean SE N Mean SE
Modality
Peritoneal
-1.52 772 -1.61 0.06
504 -1.71 0.08
Gender
Male 2166 939 -1.88 0.05
Female 1744 766 -1.60 0.06
Age
0-1 503 243 -2.34 0.10
2-5 421 164 -2.11 0.11
6-12 1249 832 -1.76 0.05
524 -1.79 0.06
>12 1737 774 -1.48 0.06
Baseline Height
Deficit
<5% 1620 762 -3.16 0.04
≥ 5% 2290 -0.76 0.04
12-3
NAPRTCS 2005
Dialysis
EXHIBIT 12.2
MEAN (SE) WEIGHT Z-SCORES, BY SELECTED CHARACTERISTICS
AND TIMES FOLLOWING DIALYSIS INITIATION
Month 1
(N=4043)
Month 6
(N=2744)
Month 12
(N=1770)
Month 24
(N=737)
N Mean SE N Mean SE N Mean SE N Mean SE
Modality
Peritoneal
-1.05 827 -1.17 0.07
538 -1.29 0.08
Gender
Male 2253 982 -1.21 0.06
Female 1790 788 -1.04 0.06
Age
0-1 542 266 -1.72 0.11
2-5 445 172 -1.11 0.12
6-12 1293 872 -1.15 0.05
553 -1.10 0.07
>12 1763 779 -0.97 0.07
Baseline Weight
Deficit
<5% 1351 871 -3.19 0.04
532 -3.19 0.05
≥ 0.02 1873 -0.23 0.03 1238 -0.25 0.03
12-4
NAPRTCS 2005
Dialysis
EXHIBIT 12.3
MEAN CHANGE FROM BASELINE (WITH SE) IN STANDARDIZED HEIGHT
AND WEIGHT SCORES, BY AGE, AT TIMES FOLLOWING DIALYSIS INITIATION
Panel A
1.0
0-1
2-5
6-12
13-17
0.5
0.0
-0.5
0.0
-0.5
-1.0
6
-1.0
6
2.0
1.5
0-1
2-5
6-12
13-17
1.0
12 18
MONTHS
24
Panel B
0.5
12 18
MONTHS
24
12-5
30 36
30 36
NAPRTCS 2005
Dialysis
EXHIBIT 12.3 (Continued)
MEAN CHANGE FROM BASELINE (WITH SE) IN STANDARDIZED DELTA HEIGHT SCORES
BY MODALITY, AT TIMES FOLLOWING DIALYSIS INITIATION
Peritoneal Dialysis
1.0
0-1
2-5
6-12
13-17
0.5
0.0
-0.5
0.0
-0.5
-1.0
6
1.0
2-5
6-12
13-17
4
12 18
MONTHS
24
Hemodialysis
0.5
30 36
-1.0
6 12 18
MONTHS
24 30 36
12-6
12-7
NAPRTCS 2005
Dialysis
IV. CHRONIC RENAL INSUFFICIENCY
NAPRTCS 2005
Chr o nic Renal Insufficiency
SECTION 13: CRI PATIENT DEMOGRAPHICS
As of database closure for this report, 5,927 patients with chronic renal insufficiency (CRI) had been registered. Exhibits 13.1A, 13.1B, and 13.1C present the distributions of gender, race/ethnicity, and primary renal diagnosis for these patients, as well as the percent of patients in each subgroup for which the primary renal diagnosis had been confirmed by biopsy. Of these patients, 64% were male and 61% white. The most common primary diseases were obstructive uropathy (22.4%); renal aplasia, hypoplasia, and dysplasia (17.9%), reflux nephropathy (8.4%), and focal segmental glomerulosclerosis (8.6%); patients with polycystic kidney disease comprised 4.1% of the cohort.
Other renal diseases were each present in less than 3% of patients. Data on biopsy confirmation of primary diagnosis pertain to the 5,680 (of 5,927) patients for whom we know whether a biopsy was performed. Of these cases, 29% of diagnoses were reported to be biopsy-proven. Data on education status is available for 5,766 patients and is shown in Exhibit 13.1D.
About one-third of patients (32.3%) were between 6 and 12 years of age at entry into the study;
20.1% were less than 24 months and 3.5% were between 18 and 20 years old (Exhibit 13.2). Note that we do not collect information on age at time of CRI diagnosis. Exhibit 13.3 presents age- and race-specific percentages of selected diagnoses. About 59% of all patients have a structural anomaly. The prevalence of FSGS among blacks is three times that of whites (18% vs. 6%), and is particularly high among black adolescents, comprising 34% of this subgroup.
Information on baseline pubertal status, as measured by Tanner stage, is presented in Exhibit 13.4.
Among males, reporting of baseline Tanner stage data is 86.1% complete. Missing data, however, are most prevalent among the 6 - 12 (15.6%) and 13 - 17 (19.8%) age groups. Among females, reporting of baseline Tanner stage data is 85.5% complete. Again, missing data are most prevalent among the 6 – 12 (12.7%) and 13 – 17 (23%) age groups. Among patients between 13 and 17 years of age at CRI registration, females are reported to be more physically mature: 65.8% of girls in this age group were Tanner stage IV or V, compared to 52.9% of boys.
Baseline laboratory measurements are presented in Exhibit 13.5. Mean serum creatinine is 2.3 mg/dL, ranging from 1.5 to 3.0 mg/dL, concordant with age. The mean Schwartz calculated creatinine clearance is 37.8 mL/min/1.73 m 2 . Mean blood urea nitrogen (BUN), albumin, and carbon dioxide (CO
2
) levels are 36.7 mg/dL, 3.8 g/dL, and 22.4 mEq/L, respectively. Similar data, by year of CRI registration, are shown in Exhibit 13.6, and reveal no apparent cohort trends for these baseline laboratory assessments.
13-1
NAPRTCS 2005
Chronic Renal Insufficiency
The baseline parathyroid hormone level (PTH) for patients with known height was unknown or not reported for half of patients (2,887/5,827), less than twice the upper normal limit for 30.9% (1,798), and greater than twice the upper normal limit for 19.6% (1,142). Of the 2,940 patients with known
PTH, the percentage with levels greater than twice the upper normal limit varied slightly with age at
32.6% (138), 32.8% (174), 40.1% (426), and 43.7% (404), for patients 0-1, 2-5, 6-12, and >12 years old respectively.
Concomitant drug therapy is depicted in Exhibit 13.7. At baseline, 38.9% were being treated with anti-hypertensive medications. The percentages of patients receiving alkali therapy, oral 1,25dihydroxy vitamin D, and calcium carbonate, were 35.6%, 33.1%, and 32%. Few patients (1% or less) were treated with aluminum hydroxide or intravenous iron supplements. No cohort trends are apparent (data not shown) in a review of these data, by registration year. Patient medical events history is shown in Exhibit 13.8. At study entry, 41.9% of patients had been diagnosed with fluid and electrolyte abnormalities, urologic surgery had been performed in 33.4%, and 32.5% had had a urinary tract infection; 3.2% of patients had already undergone orthopedic surgery.
Baseline renal function, by age at entry, is presented in Exhibit 13.9. Approximately, sixty-nine percent of all patients had a baseline Schwartz calculated creatinine clearance of 25 mL/min/1.73 m 2 or higher. Relatively fewer infants (49%) had this level of renal function compared to older children (74%). Mean height, weight and BMI standardized Z-score at entry are shown in
Exhibit 13.10. On average, patients were about 1.47 Z-score below age- and sex-specific norms for height, and .93 Z-score below weight norms. Patients who entered the study at 13 years of age or older had less severe height and weight deficits, particularly for weight — where the average Zscore is -0.22.
Grouped Z-score data are shown in Exhibits 13.11A (height) and 13.11B (weight), by age. For both height and weight, more than 41% of patients’ standardized scores fall between the third and fiftieth percentiles (Z-score values of 0 and -1.88 correspond to the fiftieth and third percentiles of the standard normal distribution.) More than one-third of the patients are less than the third percentile for height. Baseline renal function, by height Z-score, is depicted in Exhibit 13.12, showing that there are patients with severe height deficits even though they have relatively good function (>25 mL/min/1.73 m 2 ). Of patients with calculated clearance between 50 and 75 mL/min/1.73 m 2 , 22%
(379/1720) had height Z-score worse than -1.88. Among the patients with relatively good renal function (creatinine clearance ≥ 50 mL/min/1.73 m 2 ), the percentages of height deficit has been dichotomized according to whether the height Z-score exceeds the third percentile (> -1.88 Zscore).
13-2
NAPRTCS 2005
Chr o nic Renal Insufficiency
Gender
Race/Ethnicity
EXHIBIT 13.1A
CRI PATIENT CHARACTERISTICS
All Patients
Renal Biopsy
Confirmed
Diagnosis*
N % N %
*Based on patients with complete biopsy information.
13-3
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.1B
CRI DIAGNOSES
All Patients
Renal Biopsy
Confirmed Diagnosis 2
N 1 % N %
Primary Diagnosis
Obstructive uropathy 1330 22.4 1295 8
Aplasia/hypoplasia/dysplasia 1063 8
Focal segmental glomerulosclerosis 507 8.6 500 93
Reflux nephropathy
Polycystic kidney disease
496
244
8.4
4.1
478
237
8
21
Prune Belly
Renal infarct
Hemolytic uremic syndrome
SLE nephritis
179
154
129
88
3.0
2.6
2.2
1.5
171
149
121
87
11
5
27
89
Familial nephritis
Pyelo/interstitial nephritis
Medullary cystic disease
Chronic glomerulonephritis
Membranoproliferative glomerulonephritis -
Type I
Berger's (IgA) nephritis
Congenital nephrotic syndrome
Idiopathic crescentic glomerulonephritis
Henoch-Schonlein nephritis
Membranoproliferative glomerulonephritis -
Type II
Membranous nephropathy
Other systemic immunologic disease
Wilms tumor
Wegener's granulomatosis
Sickle cell nephropathy
Diabetic glomerulonephritis
Drash syndrome
84
82
74
74
66
59
51
43
39
28
27
25
25
16
12
11
5
1.4
1.4
1.2
1.2
1.1
1.0
0.9
0.7
0.7
0.5
0.5
0.4
0.4
0.3
0.2
0.2
0.1
82
79
69
73
65
59
49
43
38
28
27
25
25
16
12
11
5
66
52
59
74
97
100
80
86
87
100
100
92
72
88
75
45
100
1
2
All patients in the registry
Patients with complete renal biopsy information
13-4
NAPRTCS 2005
Chr o nic Renal Insufficiency
Total
EXHIBIT 13.1C
CRI DIAGNOSES BY RACE AND GENDER
Aplasia/hypoplasia/dysplasia
Focal segmental glomerulosclerosis
Reflux nephropathy
Polycystic kidney disease
Hemolytic uremic syndrome
N 1 % Male % White % Black % Other
5927 64 61 19 20
1330 86 61 22 18
1063 62 63 17 20
507
496
244
57
52
55
40
74
73
40
6
12
20
20
16
179 97 61 24 15
154 53 66 13 21
129 58 81 8 12
88 26 28 43 28
Medullary cystic disease
Membranoproliferative glomerulonephritis - Type I
Berger's (IgA) nephritis
Congenital nephrotic syndrome
Idiopathic crescentic glomerulonephritis
Henoch-Schonlein nephritis
Membranoproliferative glomerulonephritis - Type II
Other systemic immunologic disease
Wegener's granulomatosis
Sickle cell nephropathy
Drash syndrome
Other
Unknown
1 All patients in the registry
66
59
51
43
39
84 88 63 11 26
82 40 66 20 15
74 51 85 9 5
74 50 43 28 28
61
61
43
51
67
48
64
51
53
77
20
17
10
26
3
32
19
39
21
21
28 71 79 4 18
27 52 33 37 30
25 32 40 32 28
25 56 56 24 20
16
12
75
67
94
0
0
92
6
8
11 50 36 45 18
5 100 80 0 20
773 58 62 16 22
150 51 48 21 31
13-5
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.1D
CRI PATIENT EDUCATION STATUS
All Patients
N 1 %
Education Status (Grades 1-12)
Attends school full-time
Not of school age
Attends school part-time
Receives home schooling only
Not attending school, capable
Not attending school, incapable
1 Does not include missing
3443
1922
157
67
50
47
59.7
33.3
2.7
1.2
0.9
0.8
13-6
NAPRTCS 2005
Chr o nic Renal Insufficiency
EXHIBIT 13.2
AGE AT CRI REGISTRATION*
N %
Age at CRI Registration
0 (Less than 12 months)
1 (12-23 months)
878
314
14.8
5.3
Age Grouping
*Percent missing not shown.
13-7
NAPRTCS 2005
Chronic Renal Insufficiency
0-1
2-5
6-12
>12
0-1
2-5
6-12
>12
0-1
2-5
6-12
>12
0-1
2-5
6-12
>12
EXHIBIT 13.3
PRIMARY DIAGNOSIS, BY RACE AND AGE
% %
GN
%
FSGS
%
Other
5917 59 8 9 25
1193 77 0 1 22
961 67 2 6 25
1918 61 6 8 25
1845 40 18 16 26
3621 62 7 6 26
717 77 0 0 22
586 66 1 6 26
1231 63 5 6 26
1087 48 15 9 28
1125 52 10 18 20
220 83 0 1 15
166 76 2 3 19
304 57 7 15 22
435 25 20 34 20
820 54 9 10 27
172 69 1 1 29
146 60 4 10 27
278 55 9 10 27
224 38 20 16 26
351 54 11 7 28
84 73 1 0 26
63 65 2 5 29
105 57 10 6 27
99 28 27 14 30
0-1
2-5
6-12
>12
13-8
EXHIBIT 13.4
PERCENT DISTRIBUTION OF BASELINE TANNER STAGE,
BY AGE AT CRI REGISTRATION
[Tables exclude patients without reported gender or age]
Males ( Testicular size )
Tanner Percent Distribution 1
0-1
2-5
6-12
13-17
3812 66.3 8.4 6.1 7.8 9.1
836
639
1183
1026
>17 128
1 Percent of non-missing values
98.1 -- -- -- --
99.2 -- -- -- --
80.7 13.5 2.6 0.7 0.3
6.4 16.5 20.5 28.1 24.8
-- 2.6 2.6 12.1 77.6
Females ( Breast development )
Tanner Percent Distribution 1
8.8 13.9 All Females
Age at Entry
2106
0-1 354
2-5 322
6-12 739
13-17 614
>17 77
1 Percent of non-missing values
59.5
97.2
99.3
71.1
3.0
1.5
8.6
6.8
15.7
10.9
--
--
1.5
6.1
16.6
--
--
4.4
13-9
NAPRTCS 2005
Chr o nic Renal Insufficiency
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.5
MEAN BASELINE LABORATORY MEASUREMENTS
Age
All
Systolic blood pressure (mm Hg) 5641 114.0 98.8 105.7 114.0 126.4
Diastolic blood pressure (mm Hg) 5641 68.2 58.1 63.6 69.3 74.7
Creatinine clearance 1
Blood urea nitrogen (mg/dL)
5906 2.3 1.5 1.6 2.4 3.0
5873 38.0 28.1 40.9 40.6 40.1
5706 36.7 29.6 36.0 39.4 38.9
4977 3.8 3.9 4.0 3.9 3.7
5290 33.6 32.9 33.6 33.4 34.3
5523 22.4 22.2 21.9 22.4 22.7
5530 9.5 10.1 9.7 9.3 9.1
Alkaline phosphatase (IU/mL) 4603 262.8 353.6 257.6 270.2 205.5
1 Schwartz calculated creatinine clearance (mL/min/1.73 m 2 )
13-10
13-11
NAPRTCS 2005
Chronic Renal Insufficiency
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.7
BASELINE CONCOMITANT DRUG THERAPY, BY YEAR OF CRI REGISTRATION
[PERCENTS SHOWN IN TABLE]
Concomitant Drug Therapy
All
Patients CRI Registration Year
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Anticonvulsant
Antihypertensives
Prophylactic Antibiotics
Aluminum Hydroxide
Alkali Therapy
Immumosuppressives
Lipid Lowering Agents
Oral Vitamin D
3.8 3.3 4.4 3.7 4.1 3.3 4.6 3.4 2.5 5.3 3.0 2.9
38.9 32.0 35.3 38.5 40.1 39.3 46.6 44.9 44.4 45.4 46.0 42.9
28.0 30.3 26.2 27.5 25.7 28.8 27.7 28.1 28.6 28.6 28.0 30.4
-- -------- -- -- ---
35.6 41.6 38.9 34.6 34.1 28.8 34.4 33.6 33.0 32.6 26.1 31.2
9.8 6.3 8.5 10.7 9.4 10.9 13.0 12.1 10.6 13.6 12.6 11.8
3.4 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 5.3 2.7 4.7
33.1 37.1 35.3 30.2 28.5 29.0 35.3 32.8 33.9 29.9 28.1 37.4
Other Vitamin D Compounds
Oral Iron
Intravenous Iron
Parenteral Nutrition
6.5
27.6 21.2 27.5 22.8 27.4 28.9 30.5 33.3 30.3 34.9 33.2 40.6
0.4
0.9
8.1 7.7 8.2 7.3 5.5 4.6 6.1 2.7 3.7 4.0 2.3
0.1 0.5 0.1 0.5 1.3 0.3 0.3 0.0 1.3 1.0 1.2
0.7 1.3 0.7 0.8 0.7 0.3 1.3 1.1 1.0 1.0 0.6
Supplemental Enteral Nutrition 10.9 10.9 11.0 8.5 11.4 10.1 12.7 11.9 10.4 10.7 12.6 12.9
Calcium Carbonate 32.0 33.0 34.9 32.3 32.6 27.5 33.8 34.0 28.2 31.8 23.5 25.1
Calcium Acetate
Other Calcium Supplements
Epo
HGH
2.4
2.8
2.5 2.8 3.3 2.3 3.5 1.3 1.3 1.9 1.0 2.5 2.3
3.4 3.0 2.0 3.0 1.3 2.0 2.9 2.5 2.7 4.0 3.5
18.2 11.3 14.3 15.4 19.7 19.1 22.1 26.0 25.3 28.6 23.5 28.1
6.5 7.8 7.7 6.3 3.7 3.1 5.8 6.9 6.3 8.9 7.0 5.8
13-12
Chr o nic Renal Insufficiency
EXHIBIT 13.8
BASELINE MEDICAL EVENTS HISTORY,
BY YEAR OF CRI REGISTRATION (PERCENT)
Medical Event
All
CRI Registration Year
Patients1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Urologic Surgery
Orthopedic Surgery
Urinary Tract Infection
Hip X-ray
33.4 38.4 35.7 35.4 28.4 30.9 33.6 27.9 31.0 28.3 28.1 32.4
3.2 3.5 3.4 2.1 3.5 2.6 4.8 3.9 4.1 1.0 4.1 0.6
32.5 35.4 35.6 34.0 31.6 32.2 32.1 29.7 26.9 25.0 26.7 28.4
7.1 9.3 9.2 6.1 6.0 4.1 8.2 8.9 5.0 5.4 3.1 2.4
Seizures
Renal Biopsy
7.4 7.6 9.0 7.4 8.5 4.8 8.9 7.9 3.6 7.4 4.1 4.7
22.0 17.3 22.9 22.3 25.3 23.6 27.0 21.9 21.2 24.7 20.4 18.8
Fluid/Electrolyte Abnormalities 41.9 42.0 45.4 47.7 45.7 41.6 48.2 33.0 34.1 34.8 28.6 28.8
Blood Transfusions 9.8 9.2 10.0 11.2 10.4 9.4 12.0 12.1 8.2 11.0 4.6 3.6
13-13
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.9
BASELINE RENAL FUNCTION, BY AGE AT CRI REGISTRATION*
Age at Entry
All Patients 0-1 2-5 6-12 >12
N % N % N % N % N %
Total 5927 963 100.0 1922 100.0
Calculated GFR
<10 238 10 1.0
42 2.2
10-24 1555 438 36.7
226 23.5
442 23.0
25-49 2355 427 35.8
403 41.8
771 40.1
50-75 1725 155 13.0
313 32.5
658 34.2
*Percent missing not shown.
EXHIBIT 13.10
MEAN (AND SE) BASELINE HEIGHT SDS, WEIGHT SDS AND BMI SDS
Height SDS Weight SDS BMI SDS
N Mean SE N Mean SE N Mean SE
All 5827 -1.47 0.02 5834 -0.93 0.02 4684 0.17 0.02
0-1
2-5
6-12
13-17
18-20
1138 -2.32 0.06 1172 -2.25 0.05 13 -0.36 0.26
949 -1.69 0.05 957 -1.15 0.05 954 0.18 0.05
1909 -1.36 0.03 1910 -0.70 0.04 1916 0.15 0.03
1631 -0.95 0.04 1623 -0.20 0.04 1627 0.22 0.04
200 -0.92 0.12 172 -0.24 0.14 174 0.05 0.13
Gender
Male 3747 -1.47 0.03 3758 -0.95 0.03 2945 0.19 0.03
Female 2080 -1.47 0.04 2076 -0.91 0.04 1739 0.14 0.04
*Percent missing not shown.
13-14
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.11A
BASELINE HEIGHT SDS, BY AGE AT CRI REGISTRATION
All Patients
Age at Entry
0-1 2-5 6-12 >12
N % N % N % N % N %
Total 5827 1831 100.0
Height SDS
-1.88 or worse 2115 36.3
665 58.4
405 42.7
633 33.2 412 22.5
-1.88 to 0 2712 46.5
380 33.4
452 47.6
948 49.7 932 50.9
Better than 0 1000 17.2
93 8.2
92 9.7
328 17.2
EXHIBIT 13.11B
BASELINE WEIGHT SDS, BY AGE AT CRI REGISTRATION
487 26.6
All Patients
Age at Entry
0-1 2-5 6-12 >12
N % N % N % N % N %
Total 5834 1795 100.0
Weight SDS
-1.88 or worse 1630 27.9
686 58.5
275 28.7
410 21.5 259 14.4
-1.88 to 0
Better than 0
2443 41.9
404 34.5
489 51.1
866 45.3 684 38.1
1761 30.2
82 7.0
193 20.2
634 33.2 852 47.5
13-15
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.12
BASELINE RENAL FUNCTION, BY HEIGHT Z-SCORE
40
20
0
100
<10
25-49
80
60
10-24
>=50
<=-1.88
>-1.88 to 0 >0
13-16
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.13
BASELINE RENAL FUNCTION, BY HEIGHT Z-SCORE AND AGE AT ENTRY
AGE 0-1 AGE 2-5
40
20
0
100
<10
25-49
80
60
10-24
>=50
<=-1.88
>-1.88 to 0
AGE 6-12
>0
100
<10
25-49
80
60
40
20
0
10-24
>=50
<=-1.88
>-1.88 to 0 >0
40
20
0
100
<10
25-49
80
60
10-24
>=50
<=-1.88
>-1.88 to 0
AGE 13+
100
<10
25-49
80
60
40
20
0
10-24
>=50
<=-1.88
>-1.88 to 0
>0
>0
13-17
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 13.14
BASELINE RENAL FUNCTION, BY HEIGHT SDS AND AGE AT ENTRY
Height SDS > -1.88 Height SDS ≤ -1.88
N % N %
Age at Entry
CO
2
≤ 20 1261
PTH
<2X upper normal limit
>2X upper normal limit
1159 31.2 639 30.2
701 18.9 441 20.9
13-18
NAPRTCS 2005
Chronic Renal Insufficiency
SECTION 14: TERMINATION OF CHRONIC RENAL INSUFFICIENCY STATUS
As of database closure, there had been 2,523 reports of chronic renal insufficiency (CRI) status termination, representing 42.6% of 5,927 registered cases, as summarized in Exhibit 14.1. In the absence of a CRI Termination Form, the date of termination was established by the independent report of maintenance dialysis initiation or renal transplantation. Note that this occurred only two times in the data file. There are a total of 2,200 CRI cases with progression to ESRD, which is defined as either receiving a transplant or initiating dialysis. The majority of ESRD cases (54.1%) were due to dialysis initiation. Apparent preemptive transplant patients accounted for about onethird of terminations. Patient death is uncommon (3.8%) with cardiopulmonary and infection complications being the leading causes.
CRI termination is further characterized in Exhibit 14.2. Shown for each patient characteristic are the numbers of patients and terminations, the percent terminated, and the percentage distribution of reasons for termination, including transplantation and dialysis initiation. There is a noticeable difference in the percentage of white versus black patients who terminated CRI by receiving a transplant, while transplant as the reason of termination is also common in patients with higher albumin. Age at entry, primary diagnosis, baseline renal function and laboratory readings are statistically important, independent predictors of progression to ESRD. Multivariate Cox regression analyses in which death, native kidney regaining function, and “other” causes of CRI termination were classified as censored observations are summarized in Exhibit 14.3. Since a significant portion (2,949/5,927 or 49.8%) of CRI patients had no baseline parathyroid hormone level (PTH) information (unknown or not reported), analyses including and excluding baseline PTH as a factor are both presented in Exhibit 14.3. The estimates of relative risk of progression to ESRD were similar in both columns of the table. The results revealed that primary diagnosis was a significant factor: compared to Focal Segmental Glomerulosclerosis (FSGS) patients, patients with other primary diagnosis were less likely (RH ~ 0.6) to progress to ESRD. The risk of progression to
ESRD was also inversely proportional to baseline calculated creatinine clearance (mL/min/1.73m
2 ), but concordant with age. Moreover, patient whose baseline albumin was below 4 g/dL, inorganic phosphorous above 5.5 mg/dL, calcium below 9.5 mg/dL, BUN above 20 mq/dL or hematocrit below
33% had significantly higher risk of reaching ESRD (p<0.001).
By 12, 24, and 36 months following the initial CRI report, 16.7%, 29.4%, and 37.8% of cases, respectively, had reached ESRD (Exhibit 14.4). As indicated previously, rate of progression to
ESRD is inversely proportional to baseline renal function, as displayed in the table below and in
14-1
NAPRTCS 2005
Chronic Renal Insufficiency
Exhibit 14.5. Estimates of progression rate to ESRD according to patient race, sex, age at entry, primary diagnosis, and baseline laboratory results are presented in Exhibit 14.6. Race-specific rates are shown in Exhibit 14.7 for termination due solely to transplantation (first panel) or dialysis initiation (second panel).
CRI PROGRESSION TO ESRD PERCENTAGES (+STANDARD ERRORS)
Baseline Creatinine Clearance (mL/min/1.73m
2 )
CRI Follow-up
(months) <10 10 - 25 25 - 50 50 - 75 ALL
12
24
36
50.7
± 3.5 35.7
± 1.3 9.3
± 0.6 4.9
± 0.6 16.7
± 0.5
65.9
± 3.4 54.8
± 1.4 21.6
± 1.0 11.4
± 0.9 29.4
± 0.7
74.8
± 3.2 64.7
± 1.4 30.9
± 1.1 16.6
± 1.1 37.8
± 0.7
14-2
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 14.1
CRI TERMINATION SUMMARY*
All CRI Terminations 1
Reason for Termination:
Kidney transplant
Dialysis initiation
Native renal function regained
Patient death
*Table does not include missing.
1 2,523 (or 42.6%) of 5,927 CRI patients terminated
834
1366
91
95
33.1
54.1
3.6
3.8
14-3
NAPRTCS 2005
Chronic Renal Insufficiency
14-4
14-5
NAPRTCS 2005
Chronic Renal Insufficiency
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 14.3
RISK OF PROGRESSION TO ESRD (TRANSPLANT AND DIALYSIS INITIATION)
Factor
Model I: PTH Excluded
R.R. (P-value)
Model II: PTH Included
R.R. (P-value)
Gender
Male vs. Female 0.9 (NS) 1.0 (NS)
Race
Black vs. Non-Black 1.0 (NS) 1.0 (NS)
Age
6-12 vs. 0-5 1.7 (<0.001) 1.4 (<0.001)
> 12 vs. 0-5 2.1 (<0.001)
Glomerular Filtration Rate (mL/min/1.73m
2 )
2.0 (<0.001)
0-10 vs. ≥ 50
10-24 vs. ≥ 50
25-49 vs. ≥ 50
Primary Diagnosis
Obstructive Uropathy vs. FSGS
8.0 (<0.001)
4.2 (<0.001)
1.9 (<0.001)
0.5 (<0.001)
11.1 (<0.001)
5.3 (<0.001)
2.2 (<0.001)
0.4 (<0.001)
Renal Aplasia/Hypoplasia/Dysplasia vs. FSGS
Reflux Nephropathy vs. FSGS
Other vs. FSGS
Albumin (g/dL)
0-4 vs. > 4
Inorganic Phosphorus (mg/dL)
> 5.5 vs. 0-5.5
BUN (mg/dL)
>45 vs. <20
31-45 vs. <20
20-30 vs. <20
Calcium (mg/dL)
0-9.5 vs. > 9.5
Hematocrit (%)
< 33 vs. ≥ 33
Parathyroid hormone
< 2x UNL vs. > 2x UNL
0.5 (<0.001)
0.4 (<0.001)
0.6 (<0.001)
1.5 (<0.001)
1.4 (<0.001)
2.7 (<0.001)
1.8 (<0.001)
1.3 (<0.001)
1.4 (<0.001)
1.3 (<0.001)
-
0.4 (<0.001)
0.4 (<0.001)
0.6 (<0.001)
1.6 (<0.001)
1.4 (<0.001)
2.9 (<0.001)
2.0 (<0.001)
1.4 (0.012)
1.2 (0.004)
1.2 (0.002)
1.4 (<0.001)
14-6
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 14.4
PROGRESSION TO ESRD
100
80
60
40
20
0
0 12 24 36 48
MONTHS
EXHIBIT 14.5
PROGRESSION TO ESRD
BY BASELINE CALCULATED CREATININE CLEARANCE (mL/min/1.73 m 2 )
100
80
<10
10-24
25-49
50-75
60
40
20
0
0 12 24
MONTHS
36 48
14-7
NAPRTCS 2005
Chronic Renal Insufficiency
100
80
60
40
20
0
0
EXHIBIT 14.6
PROGRESSION TO ESRD, BY RACE, GENDER, AGE AT ENTRY, PRIMARY DIAGNOSIS,
AND BASELINE LABORATORY RESULTS
100 100
80
White
Black
Hispanic
Other
80
Male
Female
60 60
40
20
0
0
0-1
2-5
6-12
12-17
18-20
12 24
MONTHS
36
12 24
MONTHS
36
48
48
100
80
60
40
20
0
0
40
20
0
0 12 24
MONTHS
36
Obstructive Uropathy
A/Hypo/Dysplasia
Reflux Nephropathy
FSGS
Other
12 24
MONTHS
36
48
48
14-8
100
80
60
40
20
0
0
60
40
20
0
0
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 14.6 (Continued)
PROGRESSION TO ESRD, BY RACE, GENDER, AGE AT ENTRY, PRIMARY DIAGNOSIS,
AND BASELINE LABORATORY RESULTS
100 100
ALB <= 4 g/dl
ALB > 4 g/dl
P <= 5.5 mg/dl
P > 5.5 mg/dl
80 80
12 24
MONTHS
Ca <= 9.5 md/dl
Ca > 9.5 md/dl
36 48
60
40
20
0
0 12 24
MONTHS
Hematocrit < 33%
Hematocrit => 33%
36 48
12 24
MONTHS
36 48
14-9
100
80
60
40
20
0
0 12 24
MONTHS
36 48
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 14.7
PROGRESSION TO ESRD DUE TO TRANSPLANTATION
50
40
White
Black
Hispanic
30
20
10
0
0 12 24 36 48
MONTHS
PROGRESSION TO ESRD DUE TO DIALYSIS INITIATION
50
40
White
Black
Hispanic
30
20
10
0
0 12 24
MONTHS
36 48
14-10
SECTION 15: CRI FOLLOW-UP DATA
NAPRTCS 2005
Chronic Renal Insufficiency
We have received CRI follow-up forms representing completed study visits for 4,505 patients at 6 months following registration, 3,782 patients at 12 months, and 2,656 at 24 months. In addition, at the time of database closure, forms had been received for 1,873 36-month visits and 1,329 48month visits.
Point-prevalence data are presented in Exhibit 15.1 describing the use of erythropoietin and growth hormone, parathyroid hormone (PTH) levels, medical events data, and hospitalization event data.
(The PTH data exclude cases where the level was reported as “unknown” – about half of submitted forms.) At baseline, 18.2% of all patients were receiving rhEPO therapy and 6.5% were treated with rhGH. By the 24-month visit, percentage use had increased to 18.4% (rhEPO) and 15.8% (rhGH) of patients still being followed. Throughout 36 follow-up months, between 61% and 69% of patients had a PTH less than twice the upper normal limit. The medical events data, at baseline, describe any history of the event. For the semi-annual follow-up visits, these data describe whether the event has occurred in the last 6-month report period. Whereas about 34.5% of patients entered the study with a history of urologic surgery, 3% to 6.9% of patients had urologic surgery during each of the 6-month intervals through four years of follow-up. The duration and reason for hospitalizations in the 6-month report periods were collected at the semi-annual follow-up visits. Should hospitalization occur, the median duration was typically 5 days in the 6-month intervals. The main reason for hospitalization was infection, which caused 37.4% and 43.2% of all hospitalizations at the 6-month and 24-month visits.
Standardized height and weight data are presented in Exhibits 15.2 - 15.5. Recently, pediatric growth data of NHANES III were made available by CDC and have been adopted as the new standardization reference in this annual report. For height and weight, the mean standardized scores and mean changes from baseline in standardized Z-scores with standard errors, are shown.
At baseline, patients were 1.47 Z-score below age- and sex-adjusted norms for height or at about the seventh percentile of their peers. Mean standardized height remained unchanged over time at
–1.40
± 0.03, -1.40
± 0.03 and –1.35
± 0.03, respectively, at the 6-, 12-, and 24-month CRI visits.
Standardized height data are shown in Exhibit 15.2, according to age at study entry, sex, and median baseline calculated creatinine clearance (i.e., GFR). Adolescents (>12 years old) had less severe height deficits (-0.95
± 0.04) at baseline, relative to infants (-2.23
± 0.11; age <24 months) and toddlers (-1.66
± 0.06; age 2-5 years). The height deficit for males was marginally worse than for females, and patients with worse baseline GFR had more severe growth retardation than the
15-1
NAPRTCS 2005
Chronic Renal Insufficiency patients with better baseline GFR. Anemic patients (baseline Hct<33%) had worse height deficit than non-anemic patients. Mean change from baseline in height Z-score is shown in Exhibit 15.3.
At 6, 12, and 24 months following study entry, the overall mean changes in height Z-score were
0.11
± 0.02, 0.11
± 0.02, and 0.18
± 0.02. Of patients followed at four years, mean change in height Zscore was 0.27
± 0.04. Infants appear to experience a period of catch-up growth beginning around the 6-month visit by 0.52 delta height Z-score. Age-specific mean ( ± SE) and median delta height Zscore at the 24-month CRI visit are listed in the table below. A comparison of the mean and median scores suggests that the means are not overly affected by extreme values. The 0 – 1 age group is most affected. Exhibits 15.4 and 15.5 present standardized data for weight and weight changes, in a format similar to that for height and height changes.
24-MONTH DELTA HEIGHT Z-SCORE
Age at entry N Mean SE Median
0-1
2-5
530 0.77 0.09 0.62
421 0.05 0.05 0.01
6-12 799 0.0 0.02 0.00
12-20
Renal Function
538 -0.02 0.03 -0.03
Renal function data are presented in Exhibit 15.6A for serum creatinine and calculated GFR.
Overall kidney function for patients who remain in the registry (i.e., do not develop ESRD) is relatively stable over time. Mean serum creatinine values, with standard errors, at baseline, 6 months, 12 months, and 24 months are 2.3
± 0.03, 2.3
± 0.03, 2.3
± 0.03, and 2.3
± 0.03. Comparable values for calculated GFR are 38.0
± 0.25, 40.2
± 0.36, 41.8
± 0.42, and 43.1
± 0.51. As indicated in
Exhibit 15.6A, an increase in calculated creatinine clearance over time occurs among the youngest enrolled patients. An analysis of patients with at least 24 months follow-up shows a similar pattern over time for patients who have been followed the two years.
Data presented in Exhibit 15.6B include Schwartz Calculated Creatinine Clearance over time by primary diagnosis. Data presented in Exhibit 15.6C include the mean change in Schwartz calculated creatinine clearance over time by primary diagnosis. The most dramatic changes are seen for patients with a primary diagnosis of FSGS.
15-2
NAPRTCS 2005
Chronic Renal Insufficiency
To evaluate renal function, growth, and the use of growth hormone therapy, we defined 12- and 18month cohorts as follows. Patients receiving rhGH therapy at baseline, 6 months, and 12 months were defined as the "12-month" rhGH group. Similarly an "18-month" rhGH group was defined.
The control (i.e., untreated comparison) groups were defined by those patients who were not receiving growth hormone at any of the corresponding visits. To enhance comparison between the control cohort and the rhGH group in which patients typically had shorter baseline height Z-score, contrasts with 2 untreated control groups, untreated “short” control and untreated “all” control groups were made. Untreated “all” control groups include all untreated patients, while patients in
“short” control group had baseline height Z-score shorter than or equal to -1.88 or the third percentile of their age and gender-specific peers. Exhibit 15.7A presents the 12-month data for the rhGH patients and the two control group patients. For each outcome (i.e., height Z-score, serum creatinine, and calculated creatinine clearance), we present the mean baseline value, the mean 12month value, and the mean and median changes from baseline. Similar data for 18 months of follow-up are presented in Exhibit 15.8A. Exhibits 15.7B and 15.8B exclude 0 – 1 year olds at time of entry.
Growth Hormone Utilization
In order to investigate the utilization of recombinant human growth hormone therapy (rhGH), we identified two cohorts of patients. The first cohort was selected to assess time trends and the second to assess "current" usage; each is described below. Patients in both groups were selected based on their likelihood to be candidates for rhGH therapy, as follows: age-sex-appropriate (i.e., males <16 years old and females <15 years old), height Z-score of -1.88 or worse, and Tanner stage I, II, or III. Tanner stage is defined by testicular size for boys and breast development for girls.
The data presented in Exhibit 15.9 describe patients who, at the baseline (n=1,727), 6-month
(n=1,146), or 12-month (n=888) CRI visit, satisfied the aforementioned selection criteria for age, sex, height deficit, and pubertal development. Overall, rhGH use increased from 11.1% at baseline to 22.1% by the 12-month visit. In addition to the demographic factors shown in the table, rhGH use is shown for patients according to levels of CO
2
and PTH, since clinically optimal levels of these two parameters are desirable in order to maximize the effectiveness of growth hormone. A crosstabulation of CO
2
and PTH levels revealed that rhGH utilization was highest among patients with
CO
2
>20 mEq/L and PTH greater than twice the upper normal limit. Growth hormone use was greater for patients enrolled in the earlier years (1994 and 1995) of the registry compared to the late
90s. However, these patients at baseline were more likely to have been followed by study
15-3
NAPRTCS 2005
Chronic Renal Insufficiency physicians before the CRI registry was initiated, compared to patients enrolled in 1996 or later whose baseline visit is more likely to have coincided with their first physician visit. Growth hormone utilization for the subset of 617 patients who satisfied the selection criteria at all three visits
(baseline, 6-month, 12-month) is described in Exhibit 15.10.
The second cohort (Exhibit 15.11) consisted of 209 patients who, in addition to the age, sex, height, and Tanner stage criteria, were defined as “current” CRI patients. The basis for this definition was
(a) the most recent reported CRI visit must have occurred in 2004 and (b) there was no evidence of
CRI termination, initiation of maintenance dialysis, or preemptive transplantation. At that time, about 19.1% of patients were receiving rhGH therapy and was more commonly used with children
(Exhibit 15.11) between 6-12 years of age at the time of dialysis initiation.
15-4
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.1
CRI FOLLOW-UP DATA
6 12 24
Months
36
Months
48
Months
Number of visits
% rhEPO Use
% rhGH Use
PTH < 2X UNL 1
Events Data (%)
5927
18.2
6.5
4505
22.2
10.8
3782
21.2
12.7
2656
18.4
15.8
1873
19.2
16.2
1329
18.1
15.7
61.2 66.7 67.9 68.1 69.0 66.6
34.5 6.9 4.8 3.8 3.0 2.6
3.4 0.7 0.8 0.7 0.8 0.9
UTI
Seizure
8.0 3.2 2.3 2.2 1.8 0.9
8.0 1.9 1.3 1.4 1.7 1.7
22.7 3.0 0.8 0.6 0.5 0.6
Fluid/Electrolyte 45.6 19.7 17.0 14.4 13.2 10.1
12.1 1.8 0.9 0.5 0.5 0.4
Hospitalized Patients (%)
Total Number of Days (Mean)
Total Number of Days (Median)
[Hospitalized Patients Only]
Total Number of Days (Mean)
Total Number of Days (Median)
Hospitalization Reason (%)
Infection
Hypertension
--
--
--
-- 18.6 14.6 10.2 8.2 8.1
-- 1.8 1.2 0.7 0.5 0.4
0.0
9.9
5.0
0.0
8.7
5.0
0.0
7.1
5.0
0.0
5.5
4.0
0.0
4.8
3.0
-- 37.4 41.9 43.2 34.6 38.2
-- 9.7 4.6 6.0 7.2 2.0
-- 8.2 4.4 7.1 4.6 3.0
1 Excludes “Unknown” PTH data
15-5
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.2
MEAN ( ± SE) HEIGHT Z-SCORE
BY CRI VISIT AND SELECTED BASELINE CHARACTERISTICS
0.0
0.0
-0.5
Age 0-1
Age 2-5
Age 6-12
Age >12
-0.5
Male
Female
-1.0
-1.0
-1.5
-1.5
-2.0
-2.5
Baseline
0.0
-0.5
12 24
CRI VISIT MONTH
36
GFR 0-24
GFR 25-49
GFR 50-75
-1.0
-1.5
-2.0
-2.5
Baseline 12 24
CRI VISIT MONTH
36
-2.0
48
-2.5
Baseline
0.0
12 24
CRI VISIT MONTH
36
Hematocrit < 33%
Hematocrit => 33%
-0.5
-1.0
-1.5
-2.0
48
-2.5
Baseline 12 24
CRI VISIT MONTH
36
15-6
48
48
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.3
MEAN CHANGE FROM BASELINE ( ± SE) IN HEIGHT Z-SCORE,
BY CRI VISIT AND SELECTED BASELINE CHARACTERISTICS
1.25
1.00
0.75
0.50
Age 0-1
Age 2-5
Age 6-12
Age >12
1.25
1.00
0.75
0.50
Male
Female
0.25
0.00
0.25
0.00
-0.25
6
1.25
1.00
12 18 24 30
CRI VISIT MONTH
36 42 48
GFR 0-24
GFR 25-49
GFR 50-75
0.75
0.50
0.25
0.00
-0.25
6 12 18 24 30 36 42 48
CRI VISIT MONTH
15-7
-0.25
6
1.25
1.00
0.75
0.50
0.25
0.00
-0.25
6
12 18 24 30
CRI VISIT MONTH
36
Hematocrit < 33%
Hematocrit => 33%
42 48
12 18 24 30
CRI VISIT MONTH
36 42 48
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.4
MEAN ( ± SE) WEIGHT Z-SCORE,
BY CRI VISIT AND SELECTED BASELINE CHARACTERISTICS
0.0
0.0
-0.5
-1.0
-0.5
-1.0
-1.5
-1.5
0.0
-0.5
-1.0
-1.5
-2.0
-2.5
Baseline 12 24
CRI VISIT MONTH
36
Age 0-1
Age 2-5
Age 6-12
Age >12
48
-2.0
-2.5
Baseline
0.0
-0.5
-1.0
-1.5
-2.0
GFR 0-24
GFR 25-49
GFR 50-75
-2.5
Baseline 12 24
CRI VISIT MONTH
36 48
-2.0
-2.5
Baseline
15-8
12 24
CRI VISIT MONTH
36
Male
Female
48
Hematocrit < 33%
Hematocrit => 33%
12 24
CRI VISIT MONTH
36 48
2.0
1.5
1.0
Age 0-1
Age 2-5
Age 6-12
Age >12
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.5
MEAN CHANGE FROM BASELINE ( ± SE) IN WEIGHT Z-SCORE,
BY CRI VISIT AND SELECTED BASELINE CHARACTERISTICS
1.0
Male
Female
0.5
0.5
0.0
0.0
-0.5
6
1.0
12 18 24 30
CRI VISIT MONTH
36 42 48
GFR 0-24
GFR 25-49
GFR 50-75
-0.5
6 12 18 24 30
CRI VISIT MONTH
36 42 48
1.0
Hematocrit < 33%
Hematocrit => 33%
0.5
0.5
0.0
0.0
-0.5
6 12 18 24 30 36 42 48
CRI VISIT MONTH
-0.5
6 12 18 24 30
CRI VISIT MONTH
36 42 48
15-9
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.6A
SERUM CREATININE (mg/dL) AND CALCULATED CREATININE CLEARANCE (mL/min/1.73m
2 ):
MEANS AND CHANGES FROM BASELINE ( ± SE), BY AGE AT ENTRY
Serum Creatinine (SCr) Calculated Clearance (GFR)
4.5
55
4.0
Age 0-1
Age 2-5
Age 6-12
Age >12
50
Age 0-1
Age 2-5
Age 6-12
Age >12
3.5
45
3.0
40
2.5
35
2.0
1.5
30
1.0
Baseline 12 24
CRI VISIT MONTH
36
Change from Baseline in SCr
2.0
1.5
Age 0-1
Age 2-5
Age 6-12
Age >12
48
25
Baseline 12 24
CRI VISIT MONTH
36
Changes from Baseline in GFR
30
15
Age 0-1
Age 2-5
Age 6-12
Age >12
48
1.0
0.5
0.0
0
-0.5
6 12 18 24 30
CRI VISIT MONTH
36 42 48
15-10
-15
6 12 18 24 30
CRI VISIT MONTH
36 42 48
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.6B
SCHWARTZ CALCULATED CREATININE CLEARANCE (mL/min/1.73m
2 )
BY PRIMARY DIAGNOSIS
75
70
65
60
55
50
45
40
35
30
25
20
15
Baseline
Obstructive Uropathy
A/Hypo/Dysplasia
Reflux Nephropathy
FSGS
Other
12 24
CRI VISIT MONTH
36 48
15-11
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.6C
DELTA SCHWARTZ CALCULATED CREATININE CLEARANCE (mL/min/1.73m
2 )
BY PRIMARY DIAGNOSIS
20
15
10
5
0
-5
-10
-15
-20
Baseline
Obstructive Uropathy
A/Hypo/Dysplasia
Reflux Nephropathy
FSGS
Other
12 24
CRI VISIT MONTH
36 48
15-12
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.7A
12-MONTH GROWTH DATA AND RENAL FUNCTION DATA, FOR rhGH
TREATED AND UNTREATED SHORT CONTROL (Z < -1.88) AND CONTROL PATIENTS rhGH
Short Control
(Z<-1.88)
Control
(All Untreated Patients)
Mean SE Median Mean SE Median Mean SE Median
Baseline
12-Month
Delta
-2.19 0.08 -2.11 -3.34 0.06 -2.77 -1.41 0.04 -1.21
-1.80 0.08 -1.76 -2.77 0.05 -2.51 -1.32 0.03 -1.20
0.39 0.05 0.30 0.57 0.06 0.17 0.09 0.02 -0.02
Serum
Baseline
12-Month
Delta
2.23 0.09 1.80 1.80 0.04 1.50 1.90 0.02 1.60
2.76 0.12 2.30 2.04 0.06 1.55 2.26 0.03 1.70
0.54 0.08 0.30 0.24 0.03 0.10 0.36 0.02 0.10
Baseline
12-Month
Delta -2.33 0.81 -2.21 5.36 0.71 1.46 2.32 0.39 -0.63
15-13
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.7B
12-MONTH GROWTH DATA AND RENAL FUNCTION DATA, FOR rhGH
TREATED AND UNTREATED SHORT CONTROL (Z < -1.88) AND CONTROL PATIENTS
EXCLUDING 0 – 1 YEAR OLD PATIENTS rhGH
Short Control
(Z<-1.88)
Control
(All Untreated Patients)
Mean SE Median Mean SE Median Mean SE Median
Baseline
12-Month
Delta
-2.12 0.08 -2.06 -3.04 0.06 -2.63 -1.12 0.03 -0.98
-1.79 0.08 -1.71 -3.01 0.06 -2.60 -1.18 0.04 -1.03
0.33 0.03 0.29 0.04 0.03 0.01 -0.06 0.02 -0.04
Serum
Baseline
12-Month
Delta
2.28 0.10 1.90 2.06 0.05 1.70 2.07 0.03 1.70
2.82 0.13 2.30 2.52 0.08 1.90 2.56 0.04 2.00
0.53 0.08 0.30 0.45 0.04 0.20 0.49 0.03 0.20
Baseline
12-Month
Delta -2.86 0.84 -2.37 -0.94 0.62 -1.66 -1.54 0.38 -2.67
15-14
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.8A
18-MONTH GROWTH AND RENAL FUNCTION DATA, FOR rhGH
TREATED AND UNTREATED SHORT CONTROL (Z < -1.88) AND CONTROL PATIENTS rhGH
Short Control
(Z<-1.88)
Control
(All Untreated Patients)
Mean SE Median Mean SE Median Mean SE Median
Baseline
18-Month
Delta
-2.16 0.10 -2.13 -3.25 0.04 -2.73 -0.46 0.04 -0.62
-1.65 0.09 -1.63 -2.57 0.04 -2.41 -0.64 0.04 -0.71
0.51 0.06 0.42 0.68 0.05 0.27 -0.18 0.03 -0.08
Serum
Baseline
18-Month
Delta
2.14 0.09 1.90 1.73 0.03 1.40 1.88 0.03 1.60
3.10 0.17 2.80 2.05 0.05 1.50 2.39 0.05 1.80
0.96 0.12 0.50 0.32 0.03 0.10 0.51 0.04 0.20
Baseline
18-Month
Delta -4.56 1.04 -2.82 6.52 0.57 2.73 0.34 0.65 -2.25
15-15
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.8B
18-MONTH GROWTH AND RENAL FUNCTION DATA, FOR rhGH
TREATED AND UNTREATED SHORT CONTROL (Z < -1.88) AND CONTROL PATIENTS
EXCLUDING 0 – 1 YEAR OLD PATIENTS rhGH
Short Control
(Z<-1.88)
Control
(All Untreated Patients)
Mean SE Median Mean SE Median Mean SE Median
Baseline
18-Month
Delta
-2.09 0.10 -2.10 -2.91 0.04 -2.55 -0.47 0.03 -0.59
-1.63 0.10 -1.52 -2.86 0.05 -2.60 -0.61 0.04 -0.67
0.46 0.05 0.40 0.05 0.03 0.10 -0.14 0.03 -0.07
Serum
Baseline
18-Month
Delta
2.20 0.10 1.90 2.01 0.05 1.60 1.99 0.03 1.70
3.19 0.19 2.80 2.54 0.07 1.90 2.60 0.06 2.00
0.99 0.14 0.50 0.53 0.04 0.20 0.61 0.04 0.30
Baseline
18-Month
Delta -5.41 1.10 -3.25 -1.38 0.54 -1.94 -2.79 0.54 -4.14
15-16
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.9
GROWTH HORMONE UTILIZATION FOR ALL AGE- SEX-APPROPRIATE CRI PATIENTS
WITH HEIGHT Z-SCORE OF -1.88 OR WORSE, AND TANNER STAGE I, II, III
AT THE BASELINE, OR 6-MONTH, OR 12-MONTH VISIT
Gender
Male
Female
Race
White
Baseline
No. of
Patients
No. on rhGH
% on rhGH
6 Months
No. of
Patients
No. on rhGH
% on rhGH
12 Months
No. of
Patients
No. on rhGH
% on rhGH
1727 192 11.1 1146 223 19.5 888 196 22.1
1121 124 11.1 724 147 20.3 552 116 21.0
606 68 11.2 422 76 18.0 336 80 23.8
1046 132 12.6 713 160 22.4 548 131 23.9
9.8 18.1
Age
0-1
2-5
6-12
>12
1994-95
7.9 16.2
639 23 3.6 356 28 7.9 227 31 13.7
381 48 12.6 287 68 23.7 238 49 20.6
561 93 16.6 393 92 23.4 327 79 24.2
146 28 19.2 110 35 31.8 96 37 38.5
714 92 12.9 524 122 23.3 424 96 22.6
2000-02
2003
CO 2 (mEq/L)
≤ 20
>20
PTH
CO 2 ≤ 20 (mEq/L) and
PTH <2X UNL
PTH >2X UNL
PTH Unknown
CO 2 >20 (mEq/L) and
PTH <2X UNL
PTH >2X UNL
PTH Unknown
280 38 13.6 149 26 17.4 100 30 30.0
38 6 15.8 26 5 19.2 15 2 13.3
0.0 0.0
594 65 10.9 358 69 19.3 278 66 23.7
1042 118 11.3 716 143 20.0 552 124 22.5
521 76 14.6 474 105 22.2 374 93 24.9
336 49 14.6 234 55 23.5 181 52 28.7
152 24 15.8
133 15 11.3
309 26 8.4
352 49 13.9
188 32 17.0
502 37 7.4
114
93
151
332
133
251
25 21.9 107
22 23.7 70
22 14.6 101
75 22.6 254
31 23.3 99
37 14.7 199
27 25.2
25 35.7
14 13.9
63 24.8
27 27.3
34 17.1
15-17
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.10
GROWTH HORMONE UTILIZATION FOR ALL AGE-SEX-APPROPRIATE CRI PATIENTS
WITH HEIGHT SDS OF -1.88 OR WORSE, AND TANNER STAGE I, II, III
AT THE BASELINE, AND 6-MONTH, AND 12-MONTH VISITS
No. of
Patients
Baseline
No. on rhGH
% on rhGH
6 Months
No. on rhGH
% on rhGH
12 Months
No. on rhGH
% on rhGH
617 62 10.0 126 20.4 161 26.1
Gender
Male
Female
Race
White
Black
Hispanic
Other
Age
0-1
2-5
6-12
>12
240 32 13.3 52 21.7 71 29.7
379 41 10.8 86 22.7 108 28.6
37 4 10.8 9 24.3 11 29.7
207 6 2.9 16 8.7 22 13.9
218 31 14.2 56 24.7 71 30.3
38 11 28.9 20 39.2 28 44.4
311 38 12.2 71 22.8 84 27.0 1994-95
1996-97
1998-99
2000-02
2003
CO 2 (mEq/L)
<20
76 9 11.8 19 25.0 22 29.3
64 7 10.9 14 21.9 23 35.9
8 1 12.5 1 12.5 2 25.0
209 26 12.4 46 21.9 55 28.4
PTH
200 28 14.0 58 22.7 79 29.5
103 13 12.6 34 27.4 38 32.8
Unknown
CO 2 ≤ 20 (mEq/L) and
PTH <2X UNL
PTH >2X UNL
CO 2 >20 (mEq/L) and
PTH <2X UNL
PTH >2X UNL
60 11 18.3 19 25.7 22 30.6
42 4 9.5 17 29.8 20 47.6
107 11 10.3 10 12.7 13 16.3
134
60
16
9
11.9
15.0
36
17
21.6
26.2
PTH 192 10 5.2 22
54
18
29.2
26.9
15-18
NAPRTCS 2005
Chronic Renal Insufficiency
EXHIBIT 15.11
GROWTH HORMONE UTILIZATION FOR CURRENT AGE-SEX-APPROPRIATE CRI
PATIENTS WITH HEIGHT SDS OF -1.88 OR WORSE, AND TANNER STAGE I, II, III
AT THE MOST RECENT COMPLETED VISIT IN 2003
All Patients
Gender
Number of Patients Number on rhGH Percent on rhGH
209 40 19.1
Race
Age
Time Since Enrollment
6 Months
12 Months
18 Months
24 Months
30 Months
36 Months
42 Months
34
22
18
20
21
11
8
6
1
6
9
7
3
2
17.6
4.5
33.3
45.0
33.3
27.3
25.0
0.0
16.7
48 Months
54 Months
5
12
0
2
CO
2
(mEq/L)
≤ 20
>20 150
PTH
<2X UNL
>2X UNL
114
53
22
15
19.3
28.3
CO
2
≤ 20 mEq/L and
PTH <2X UNL
PTH >2X UNL
PTH Unknown
CO
2
>20 mEq/L and
PTH <2X UNL
PTH >2X UNL
PTH Unknown
25
14
12
86
38
26
6
3
0
15
11
3
24.0
21.4
0.0
17.4
28.9
11.5
15-19
V. APPENDICES
APPENDIX A
PARTICIPATING CENTERS AND CONTACT PHYSICIANS
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PARTICIPATING CENTERS AND CONTACT PHYSICIANS
CENTER CITY, STATE PRINCIPAL INVESTIGATOR
A
Alberta Children's Hospital
Alfred I. duPont Institute
All Children's Hospital
Arkansas Children's Hospital
B
Babies and Children's Hospital of NY
Calgary, Alberta, CN Julian Midgley, M.D.
Lorraine Hamiwka, M.D.
Wilmington, DE Laszlo Hopp, M.D.
St. Petersburg, FL
Little Rock, AR
New York, NY
New York, NY
Sharon Perlman, M.D.
Eileen Ellis, M.D.
Martin A. Nash, M.D.
Robert L. Seigle, M.D.
BC Children's Hospital
C
Cardinal Glennon Hospital
Carolina's Medical Center
Vancouver, BC, CN
St. Louis, MO
Charlotte, NC
Cedars-Sinai Medical Center Los Angeles, CA
Children's Healthcare of Atlanta Atlanta, GA
Children's Healthcare of Atlanta @ Scottish Rite Atlanta, GA
Children's Hospital & Medical Center-Seattle
Children's Hospital- Boston
Children's Hospital Central California
Children's Hospital Medical Center-Cincinnati
Children's Hospital Medical Center-Akron
Children's Hospital National Medical Center
Children's Hospital Oakland
Children's Hospital of Alabama
Children's Hospital of Eastern Ontario
Children's Hospital of Los Angeles
Children's Hospital of Michigan
Children's Hospital of Oklahoma
Children's Hospital of Philadelphia
Children's Hospital of Pittsburgh
Seattle, WA
Boston, MA
Madera, CA
Cincinnati, OH
Akron, OH
Washington, DC
Oakland, CA
Birmingham, AL
Ottawa, ON, CN
Los Angeles, CA
Los Angeles, CA
Los Angeles, CA
Detroit, MI
Oklahoma City, OK
Philadelphia, PA
Pittsburgh, PA
R.Morrison Hurley, MD
Ellen Wood, M.D.
Susan Massengill, M.D.
Elaine Kamil, M.D.
Dechu Puliyanda, M.D.
Barry L. Warshaw, M.D.
Julius Sherwinter, M.D.
Sandra L. Watkins, M.D.
John Herrin, M.B.B.S, F.R.A.C.P.
Jerome Murphy, M.D.
C. Frederic Strife, M.D.
Ian Dresner, M.D.
Asha Moudgil, M.D.
Rose Ellen Morrell, M.D.
Mark Benfield, M.D.
Guido Filler, M.D., Ph.D., F.R.C.P.C.
Carl Grushkin, M.D.
Gary Lerner, M.D.
Mark Mentser, M.D.
Tej Mattoo, M.D.
Martin Turman, M.D., Ph.D.
Mary B. Leonard, M.D.
Demetrius Ellis, M.D.
A-1
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PARTICIPATING CENTERS AND CONTACT PHYSICIANS
CENTER
Children's Hospital of the King's Daughters
Children's Hospital of Winnipeg
Children's Hospital-Columbus
Children's Hospital-New Orleans
Children's Medical Center-Dallas
Children's Memorial Hospital-Chicago
Children's Mercy Hospital
Children's Renal Center-Galveston
Cleveland Clinic Foundation
Columbia Presbyterian Medical Center
Connecticut Children's Medical Center
Cook Children's Medical Center
E
East Carolina University
ETSU Physicians & Associates Pediatrics
H
Hackensack University Medical Center
Hospital for Sick Children-Toronto
Hospital Infantil de Mexico
Hospital National de Ni ň os
Hospital St. Justine
I
Inova Hospital for Children
J
Johns Hopkins University
JW Riley Hospital for Children
K
CITY, STATE PRINCIPAL INVESTIGATOR
Norfolk, VA
Winnipeg, MB
Columbus, OH
New Orleans, LA
Dallas, TX
Chicago, IL
Kansas City, MO
Galveston, TX
Cleveland, OH
New York City, NY
Hartford, CT
Fort Worth, TX
Irene Restaino, M.D.
Tom Blydt-Hansen, M.D., F.R.C.P.C.
Donald L. Batisky, M.D.
Matti Vehaskari, M.D.
Mouin Seikaly, M.D.
Richard A. Cohn, M.D.
Bradley A. Warady, M.D.
Amita Sharma, M.D.
Deepa Chand, MD
Valerie Johnson M.D.
Majid Rasoulpour, M.D.
Watson C. Arnold, M.D.
Greenville, NC
Johnson City, TN
Hackensack, NJ
Toronto, ON, CN
Jen-Jar Lin, M.D.
Ahmad Wattad, M.D.
Kenneth Lieberman, M.D.
Denis Geary, M.D.
Mexico 7, D.F. Ricardo Munoz, M.D.
San Jose, Costa Rica Gilbert Madrigal, M.D.
Montreal, Quebec, CN Marie-Jose Clermont, M.D.
Fairfax, VA Glenn Bock, M.D.
Baltimore, MD
Indianapolis, IN
Barbara Fivush, M.D.
Alicia Neu, M.D.
Sharon Andreoli, M.D.
A-2
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PARTICIPATING CENTERS AND CONTACT PHYSICIANS
CENTER CITY, STATE PRINCIPAL INVESTIGATOR
Kids Kidney Center @ Phoenix Children's Hospital Phoenix, AZ
Kosair Charities Pediatric Center
L
Louisville, KY
LAC+USC Medical Center
Lebonheur Children's Medical Center
Loma Linda University Medical Center
Lutheran General Children's Medical Center
M
Los Angeles, CA
Memphis, TN
Loma Linda, CA
Park Ridge, IL
Maine Pediatric Specialty Group
Mary Bridge Children's Hospital
Massachusetts General Hospital
Mayo Clinic
Medical College of VA Hospitals & Phy
Medical College of Georgia
Medical College of Wisconsin
Mercy Children's Hospital
Michigan State University - Kalamazoo
Michigan State University
Milton S. Hershey Medical Center
Montefiore Medical Center
Montreal Children's Hospital
Mount Sinai Hospital
N
Nemours Children's Clinic
New York Hospital
North Shore University Hospital
Northwest Ped. Kidney Specialists
O
Oregon Health Sciences University
Mark Joseph, M.D.
Larry Shoemaker, M.D.
Donna Elliott, M.D.
Robert J. Wyatt, M.D.
Shobha Sahney, M.D.
Ronald Kallen, M.D.
Portland, ME
Tacoma, WA
Boston, MA
Rochester, MN
Richmond, VA
Augusta, GA
Milwaukee, WI
Toledo, OH
Kalamazoo, MI
Lansing, MI
Matt Hand, M.D.
Robert Holleman, M.D.
Julie Ingelfinger, M.D.
Dawn S. Milliner, M.D.
Vimal Chadha, M.D.
Coral D. Hanevold, M.D.
Cynthia Pan, M.D.
Martin DeBeukelaer, M.D.
Alfonso Torres, M.D.
Pinhas Geva, M.D.
Hershey, PA
Bronx, NY
Steven J. Wassner, M.D.
Joseph Flynn, M.D.
Montreal, Quebec, CN Lorraine Bell, M.D.
New York, NY Lisa Satlin, M.D.
Orlando, FL
New York, NY
Manhasset, NY
Jorge Ramirez, M.D.
Valerie Johnson, M.D., Ph.D.
Manju Chandra, M.D.
Portland, OR
Portland, OR
Randy Jenkins, M.D.
Amira Al-Uzri, M.D.
A-3
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PARTICIPATING CENTERS AND CONTACT PHYSICIANS
CENTER CITY, STATE PRINCIPAL INVESTIGATOR
P
Pediatric Specialty Center
R
Rainbow Babies & Children's Hospital
S
Schneider Children's Hospital
St. Barnabas Medical Center
Hollywood, FL Michael Freundlich, M.D.
Cleveland, OH Ira D. Davis, M.D.
New Hyde Park, NY Marcele Vergara, M.D.
Livingston, NJ Isabel Roberti, M.D.
St. Christopher's Hospital for Children
St. Francis Renal Institute-Honolulu
St. Louis Children's Hospital
Stanford University Medical Center
State University of New York-Stony Brook
T
Texas Children's Hospital
Philadelphia, PA
Honolulu, HI
St Louis, MO
Stanford, CA
Stony Brook, NY
Houston, TX
Susan B. Conley, M.D.
James E. Musgrave, M.D.
S. Paul Hmiel, M.D.
Steven R. Alexander, M.D.
Dilys Whyte, M.D.
Eileen D. Brewer, M.D.
Stuart L. Goldstein, M.D.
Texas Tech University Amarillo, TX
The Children's Hospital @ Albany Medical Center Albany, NY
The Children's Hospital - Denver Denver, CO
The Children's Hospital of Austin
The Children's Hospital of Buffalo
Tulane University Medical Center
Austin, TX
Buffalo, NY
New Orleans, LA
U
UCLA School of Medicine Los Angeles, CA
UCSF Children's Renal Center
UMDNJ Robert Wood Johnson Medical School
University of Alberta Hospital
University of California at San Diego
University of Florida
San Francisco, CA
New Brunswick, NJ
Deogracias R. Pena, M.D.
Rod E. Urizar, M.D.
Douglas Ford, M.D.
Phillip Berry, M.D.
James Springate, M.D.
Frank G. Boineau, M.D.
Robert Ettenger, M.D.
Edmonton, Alberta, CN Manjula Gowrishankar, M.D.
La Jolla, CA
Gainesville, FL
Robert Mathias, M.D.
Lewis Reisman, M.D.
Verna Yiu, M.D.
Nadine Benador, MD
Robert S. Fennell, M.D.
A-4
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PARTICIPATING CENTERS AND CONTACT PHYSICIANS
CENTER
University of Illinois
University of Iowa Hospitals
University of Maryland Medical Center
University of Michigan
University of Mississippi Medical Center
University of Missouri
University of Nebraska Medical Center
University of New Mexico
University of North Carolina, Chapel Hill
University of Rochester Medical Center
University of South Florida
University of Tennessee Medical Center
University of Texas HSC @ San Antonio
University of Vermont
University of Virginia Medical Center
University of Wisconsin Hospital and Clinics
V
Vanderbilt University Medical
W
Westchester County Medical Center
CITY, STATE
Chicago, IL
Iowa City, IA
Baltimore, MD
Ann Arbor, MI
Jackson, MS
Columbia, MO
Omaha, NE
Albuquerque, NM
Chapel Hill, NC
Rochester, NY
Miami, FL
Knoxville, TN
San Antonio, TX
Burlington, VT
Charlottesville, VA
Madison, WI
Nashville, TN
Valhalla, NY
PRINCIPAL INVESTIGATOR
Vikas Dharnidharka, M.D.
Eunice G. John, M.D.
Craig Porter, M.D.
Susan Mendley, M.D.
Susan Thomas, M.D.
Radharkrishna Baliga, M.D.
Ted D. Groshong, M.D.
Helen Lovell, M.D.
John Brandt, M.D.
Debbie Gipson, M.D.
William Primack, M.D.
Marc Lande, M.D.
Alfonso Campos, M.D.
Maricarment Malagon-Rogers, M.D.
Mazen Y. Arar, M.D.
Ann P. Guillot, M.D.
John Barcia, M.D.
Sharon M. Bartosh, M.D.
Kathy Jabs, M.D.
Robert A. Weiss, M.D.
A-5
APPENDIX B
BIBLIOGRAPHY - 1988-2004
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
1. Alexander SR, Arbus GS, Butt KMH, et al. The 1989 Report of the North American
Pediatric Renal Transplant Cooperative Study. Pediatr Nephrol 4:542-553, 1990.
2. Tejani A, Stablein D, Alexander S. Growth in North American children one year after renal transplantation: A report of the North American Pediatric Renal Cooperative Study.
Kidney Int 37:614, 1990.
3. Alexander S, Tejani A, Stablein D, Fine R and Harmon W. Poor graft outcome of black live related donor (LRD) kidneys compared to Hispanic and Caucasian children: A report of the North American Renal Transplant Cooperative Study (NAPRTCS). J Am
Soc Nephrol 2:790, 1991.
4. Harmon W, Alexander SR, Stablein DM, Tejani A. Graft thrombosis as a cause of graft failure in pediatric renal transplant recipients: A report of the North American Pediatric
Renal Transplant Cooperative Study. Transplantation 51:406-412, 1991.
5. Tejani A, Stablein D, Alexander S, Fine R. Renal allograft outcome in North American children: A report of the North American Renal Transplant Cooperative Study. J Am
Soc Nephrol 1:772, 1991.
6. Harmon WE, Alexander SR, Tejani A, Stablein D. The effect of donor age on graft survival in pediatric cadaver renal transplant recipients. A report of the North American
Pediatric Renal Transplant Cooperative Study. Transplantation 54:232-237, 1992.
7. McEnery PT, Stablein DM. Does HLA matching improve the outcome in pediatric renal transplants? J Am Soc Nephrol 2:S234-S237, 1992.
8. McEnery PT, Stablein DM, Arbus G, Tejani A. Renal transplantation in children: A report of the North American Pediatric Renal Transplant Cooperative Study. N Eng J Med
326:1727-1732, 1992.
9. Tejani A and Stablein DM. Recurrence of focal segmental glomerulosclerosis posttransplantation: A special report of the North American Pediatric Renal Transplant
Cooperative Study. J Am Soc Nephrol 2:S258-S263, 1992.
10. Alexander SR, Sullivan EK, Harmon WE, Stablein DM, Tejani A, for the North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS). Maintenance dialysis in
North American children and adolescents: a preliminary report. Kidney Int 44:S104-
S109, 1993.
11. Arbus GS, Sullivan EK, Tejani A. Hospitalization in children during the first year after kidney transplantation. Kidney Int 44:S83-S86, 1993.
12. Harmon WE and Sullivan EK. Cyclosporine dosing and its relationship to outcome in pediatric renal transplantation. Kidney Int 44:S50-S55, 1993.
B-1
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
13. McEnery PT, Alexander SR, Sullivan K, Tejani A. Renal transplantation in children and adolescents: the 1992 Annual Report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Pediatr Nephrol 7:711-720, 1993.
14. Stablein DM and Tejani A. Five-year patient and graft survival in North American children:
A report of the North American Pediatric Renal Transplant Cooperative Study. Kidney
Int 44:S16-S21, 1993.
15. Tejani A and Sullivan K. Long-term follow-up of growth in children post-transplantation.
Kidney Int 44:S56-S58.
16. Tejani A, Fine R, Alexander S, Harmon W, Stablein D. Factors predictive of sustained growth in children after renal transplantation. A report of the North American Pediatric
Renal Transplant Cooperative Study. J Pediatr 122:397-402, 1993.
17. Tejani A, Stablein D, Fine R, Alexander S. Maintenance immunosuppression therapy and outcome of renal transplantation in North American children - A report of the North
American Pediatric Renal Transplant Cooperative Study. Pediatr Nephrol 7:132-137,
1993.
18. Baluarte HJ, Gruskin AB, Ingelfinger JR, Stablein D, Tejani A. Analysis of hypertension in children post renal transplantation - A report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Pediatr Nephrol 8:570-573, 1994.
19. Fine R, Tejani A, Sullivan EK. Pre-emptive renal transplantation in children: report of the
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Clin
Transplant 8:474-478, 1994.
20. Stablein DM, Sullivan EK, Lilienfeld DE. Renal transplantation in children: The North
American Pediatric Renal Transplant Cooperative Study (NAPRTCS) experience. In:
Pediatric Renal Transplantation (A Tejani and R Fine, eds). New York: John Wiley and Sons, 1994.
21. Tejani A, Sullivan EK, Alexander S, Fine R, Harmon W, Lilienfeld D. Posttransplant deaths and factors that influence the mortality rate in North American children.
Transplantation 57:547-553, 1994.
22. Avner E, Chavers B, Sullivan EK, Tejani A. Renal transplantation and chronic dialysis in children and adolescents: The 1993 Annual Report of the North American Pediatric
Renal Transplant Cooperative Study. Pediatr Nephrol 9:61-73, 1995.
23. Fine RN, Stablein DM, Tejani A. Do children exhibit catch-up growth post transplant:
North American Pediatric Renal Transplant Cooperative Study special study. Pediatr
Nephrol 1995;9 Suppl:S66-8.
24. Scheinman JI, Alexander M, Campbell ED, Chan JC, Latta K, Cochat P. Transplantation for primary hyperoxaluria in the USA. Nephrol Dial Transplant 1995;10 Suppl 8:42-6.
B-2
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
25. Singh A, Cortes L, Tejani A. Pediatric renal transplantation. Curr Opin Nephrol Hypertens.
1995 Nov;4(6):478-81. Review.
26. Kashtan CE, McEnery PT, Tejani A, Stablein DM. Renal allograft survival according to primary diagnosis: A report of NAPRTCS. Pediatr Nephrol 9(6):679-684, Dec 1995.
27. Kerman RH, Sullivan EK. Impact of HLA matching, type of crossmatch and immunosuppressive therapy on primary pediatric cadaver renal allograft survival.
Transplant Proc 27:656-657, 1995.
28. Sullivan EK, Lilienfeld DE, Stablein DM. Analysis of the NAPRTCS dialysis data. In:
Clinical Dialysis (A Nissensen, R Fine, and DE Gentile, eds). Connecticut: Appleton and Lange, 1995.
29. Tejani A, Stablein D, Alexander S, Fine R, Harmon W. Analysis of rejection outcomes and implications. A report of the North American Pediatric Renal Transplant Cooperative
Study. Transplantation 59:500-504, 1995.
30. Tejani A, Sullivan EK, Fine RN, Harmon W, Alexander S. Steady improvement in renal allograft survival among North American children. A five year appraisal by the North
American Pediatric Renal Transplant Cooperative Study. Kidney Int 48:551-553,
1995.
31. Jabs K, Sullivan EK, Avner ED, Harmon WE. Alternate day steroid dosing improves growth without adversely affecting graft survival or long-term graft function: A report of the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS).
Transplantation 61(1):31-36, Jan 1996.
32. Tejani A, Cortes L, Sullivan EK. A longitudinal study of the natural history of growth posttransplantation. Kidney Int Suppl 53:103-108, Jan 1996.
33. Warady BA, Sullivan EK, Alexander SR. Lessons from the peritoneal dialysis patient database: A report of the North American Pediatric Renal Transplant Cooperative
Study. Kidney Int Suppl 53:S68-S71, Jan 1996.
34. Tejani A, Cortes L, Stablein DM. Clinical correlates of chronic rejection in pediatric renal transplantation: A report of the North American Pediatric Renal Transplant Cooperative
Study. Transplantation 61(7):1054-1058, Apr 15, 1996.
35. Tejani A, Sullivan EK. Higher maintenance cyclosporine dose decreases the risk of graft failure in North American children: A report of the North American Pediatric Renal
Transplant Cooperative Study. J Am Soc Nephrol 7(4):550-555, Apr 1996.
36. Kohaut EC, Tejani A. The 1994 Annual Report of the North American Pediatric Renal
Transplant Cooperative Study. Pediatr Nephrol 10(4):422-434, Aug 1996.
B-3
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
37. Neu A, Furth SL, Zachary A, Stablein DM, Fivush BA. Beneficial effect on non-inherited maternal antigens on graft survival in pediatric renal transplantation. J Am Soc
Nephrol 7(9):1917, Sep 1996.
38. Tejani A, Sullivan EK. Factors that impact on the outcome of second renal transplants in children. Transplantation 62 (5):606-611, Sep 15, 1996.
39. Salvatierra O, Alfrey E, Tanney DC, Mak R, Hammer GB, Krane EJ, So SK, Lemley K,
Orlandi PD, Conley SB. Superior outcomes in pediatric renal transplantation. Arch
Surg. 1997 Aug;132(8):842-7; discussion 847-9.
40. Bock GH, Sullivan EK, Miller D, Gimon D, Alexander SR, Ellis E, Elshihabi I.
Cytomegalovirus infections following renal transplantation-effects of antiviral prophylaxis: A report of the North American Pediatric Renal Transplant Cooperative
Study (NAPRTCS). Pediatr Nephrol 11:665-671, 1997.
41. Chavers BM, Sullivan EK, Tejani A, Harmon WE. Pre-transplant blood transfusion and renal allograft outcome: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Pediatr Transplant 1(1):22-28, 1997.
42. Feld LG, Stablein DM, Fivush BA, Harmon WE, Tejani A. Renal transplantation in children from 1987-1996: The Annual Report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Pediatr Transplant 1(1):146-162, 1997.
43. Fine RN. Growth post renal transplantation in children: A report of the North American
Pediatric Cooperative Study (NAPRTCS). Pediatr Transplant 1(1): 85-89, 1997.
44. Furth SL, Sullivan EK, Neu AM, Tejani A, Fivush BA. Varicella in the first year after renal transplantation: A report of the North American Pediatric Renal Transplant Cooperative
Study. Pediatr Transplant 1(1):37-42, 1997.
45. Jabs K, Sullivan EK, Fivush B. Prevalence of anemia in children with chronic renal insufficiency (CRI): A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). J Am Soc Nephrol 8:70, 1997.
46. Warady BA, Hebert D, Sullivan EK, Alexander SR, Tejani A. Renal transplantation, chronic dialysis, and chronic renal insufficiency in children and adolescents. The 1995
Annual Report of the North American Pediatric Renal Transplant Cooperative Study.
Pediatr Nephrol 11:49-64, Feb 1997.
47. Singh A, Stablein DM, Tejani A. Risk factors for vascular thrombosis in pediatric renal transplantation: a special report of the North American Pediatric Renal Transplant
Cooperative Study. Transplantation 1997;63:1263-1267, May 1997.
B-4
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
48. Mentser M, Breen TJ, Sullivan EK, Fine RN. Growth-hormone treatment of renal transplant recipients: the National Cooperative Growth Study--A report of the National
Cooperative Growth Study and the North American Pediatric Renal Transplant
Cooperative Study. J Pediatr 131 (1 Pt 2):S20-S24, Jul 1997.
49. Furth SL, Neu AM, Sullivan EK, Gensler G, Tejani A, Fivush BA. Immunization practices in children with renal disease: A report of the North American Pediatric Renal
Transplant Cooperative Study. Pediatr Nephrol 11(4) 443-446, Aug 1997.
50. Al-Uzri A, Sullivan EK, Fine RN, Harmon WE. Living-unrelated renal transplantation in children: a report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS) Pediatr Transplant 1998 May;2(2):139-44.
51. Baqi N, Tejani A, Sullivan EK. Renal transplantation in Down Syndrome: A report of the
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Pediatr
Transplant 2:139-144, 1998.
52. Fivush BA, Jabs K, Neu AM, Sullivan EK, Feld LG, Kohaut E, Fine RN. Chronic renal insufficiency in children and adolescents: The 1996 Annual Report of the North
American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Pediatr Nephrol
12:328-337, 1998.
53. Kim MS, Stablein D, Harmon WE. Renal transplantation in children with congenital nephrotic syndrome: A report of the North American Pediatric Cooperative Study
(NAPRTCS). Pediatr Transplant 2:305-308, 1998.
54. Neu AM, Stablein DM, Zachary A, Furth SL, Fivush BA. Effect of parental donor sex on rejection in pediatric renal transplantation: A report of the North American Pediatric
Cooperative Study (NAPRTCS). Pediatr Transplant 2:309-312, 1998.
55. Osorio AV, Sullivan EK, Alexander SR, Bryan CF, Shield CF, Warady BA. ABOmismatched renal transplantation in children: A report of the North American Pediatric
Renal Transplant Cooperative Study (NAPRTCS) and the Midwest Organ Bank
(MOB). Pediatr Transplant 2:26-29, 1998.
56. Tejani A, Emmett L, Harmon WE. Travails of organizing an International Congress.
Pediatr Transplant 2:245-248, 1998.
57. Tejani AH, Stablein DM, Sullivan EK, Alexander SR, Fine RN, Harmon WE, and Kohaut
EC. The impact of donor source, recipient age, preoperative immunotherapy and induction therapy on early and late acute rejections in children: A report of the North
American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Pediatr
Transplant 2:318-324, 1998.
B-5
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
58. Tejani AH, Sullivan EK, Harmon WE, Fine RN, Kohaut E, Emmett L, Alexander SR.
Pediatric Renal Transplantation - The NAPRTCS Experience. In JM Cecka, PI
Terasaki (eds). Clinical Transplants 1997. Los Angeles: UCLA Tissue Typing
Laboratory. 87-100, 1998.
59. Warady BA, Sullivan EK. Renal transplantation in children with sickle cell disease: A report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). Pediatr Transplant 2:130-133, 1998.
60. Kim MS, Stablein D, Harmon WE. Renal transplantation in children with congenital nephritic syndrome: a report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Pediatr Transplant 1998 Nov;2(4):305-8. PMID:
10084734
61. Tejani A, Stablein DM, Donaldson L, Harmon WE, Alexander SR, Kohaut E, Emmett L,
Fine RN. Steady improvement in short-term graft survival of pediatric renal transplants: the NAPRTCS experience. Clin Transpl 1999:95-110.
62. Fine RN, Sullivan EK, Tejani A. The impact of recombinant human growth hormone treatment on final adult height. Pediatr Nephrol 2000 Jul;14(7):679-81. Review.
63. Saborio P, Scheinman JI. Transplantation for primary hyperoxaluria in the United States.
Kidney Int 1999 Sep;56(3):1094-100.
64. Benfield MR, McDonald R, Sullivan EK, Stablein DM, Tejani A. The 1997 Annual Renal
Transplantation in Children: Report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Pediatr Transplant 1999;2:152-167.
65. Benfield D, Stablein D, Tejani A. Trends in immunosuppressive therapy: A report of the
North American Pediatric Cooperative Study (NAPRTCS). Pediatr Transplant 1999;3:
27-32.
66. Benfield MR, Herrin J, Feld L, Rose SR, Stablein DM, Tejani A: Safety of kidney biopsy in pediatric transplantation: A report of the Controlled Clinical Trials in Pediatric
Transplantation (CCTPT) trial of induction therapy study group. Transplantation
1999;67:544-547.
67. Lerner GR, Warady BA, Sullivan EK, Alexander SR. Chronic dialysis in children and adolescents. The 1996 annual report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Pediatr Nephrol 1999;5:404-17.
68. Schurman S, Stablein DM, Perlman SA, Warady BA. Center volume effects in pediatric renal transplantation. A report of the North American Pediatric Renal Transplant
Cooperative Study. Pediatr Nephrol 1999;5:373-8.
B-6
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
69. Sorof JM, Sullivan EK, Tejani A, Portman RJ. Antihypertensive medication and renal allograft failure: a North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). J Am Soc Nephrol 1999;6:1324-30.
70. Tejani A, Sullivan EK, Alexander SR, Fine RN, Harmon WE, Kohaut EC. Predictive factors for delayed graft function (DGF) and its impact on renal graft survival in children: A report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). Pediatr Transplant 1999;3:293-300,1999.
71. Tejani A, Sullivan EK: The impact of acute rejection on chronic rejection: A report of the
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Pediatr
Transplant 1999;4:107-111.
72. Tejani A, Stablein DM, Donaldson L, Harmon WE, Alexander SR, Kohaut E, Emmett L,
Fine RN. Steady improvements in short-term graft survival of pediatric renal transplants: The North American Pediatric Transplant Cooperative Study (NAPRTCS) experience, in Terasaki PI, Cecka JM (eds), Clinical Transplants 1999. Los Angeles,
UCLA Tissue Typing Laboratory, 2000.
73. Alexander SR, Donaldson LA, Sullivan EK. CAPD/CCPD for children in North America:
The NAPRTCS Experience. In RN Fine, BA Warady, SR Alexander (eds). CAPD and
CCPD in Children, 2 nd Edition. 2000, Norwell, MA: Kluwer Academic Publishers. In press.
74. Brouhard BH, Donaldson LA, Lawry KW, McGowan KRB, Drotar D, Davis I, Rose S, Cohn
RA, Tejani A. Cognitive functioning in children on dialysis and post-transplantation.
PediatrTransplant 2000;4:261-267
75. Elshihabi I, Chavers B, Donaldson L, Emmett L, Tejani A: Continuing improvement in cadaver donor graft survival in North American children: The 1998 Annual Report of the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS).
Pediatr Transplant 2000;4:235-246.
76. Fine RN, Sullivan EK, Kuntze J, Blethen S, Kohaut E. The impact of recombinant human growth hormone treatment during chronic renal insufficiency on renal transplant recipients. J Pediatr 2000;3:376-382.
77. Furth SL, Donaldson LA, Sullivan EK, Watkins SL. Peritoneal dialysis catheter infections and peritonitis in children: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Pediatr Nephrol 2000;15(3-4);179-182.
78. McDonald R, Donaldson L, Emmett L, Tejani A. A decade of living donor transplantation in North American children: The 1998 annual report of the North American Pediatric
Renal Transplant Cooperative Study (NAPRTCS). Pediatr Transplant 2000;4:221-234.
79. Tejani A. Chronic rejection in pediatric renal transplantation: Where are we? Editorial,
Pediatr Transplant 2000;4:83-85.
B-7
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
80. Tejani A, Sullivan EK. Do six-antigen matched cadaver donor kidneys provide better graft survival to children compared to one-haploidentical living-related donor transplants?: A report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). Pediatr Transplant 2000;4:140-143.
81. Vats AN, Donaldson L, Fine RN, Chavers BM. Pretransplant dialysis status and outcome of renal transplantation in North American children: a NAPRTCS Study. North
American Pediatric Renal Transplant Cooperative Study. Transplantation
2000;69(7):1414-9.
82. Warady BA, Bashir M, Donaldson LA. Fungal peritonitis in children receiving peritoneal dialysis: A report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). Kidney Int 2000;58(1):384-9.
83. McDonald R, Ho PL, Stablein DM, Tejani A; North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Rejection profile of recent pediatric renal transplant recipients compared with historical controls: a report of the North American Pediatric
Renal Transplant Cooperative Study (NAPRTCS). Am J Transplant 2001 May;1(1):55-
60.
84. Warady BA. Should the DOQI adequacy guidelines be used to standardize peritoneal dialysis in children? Perit Dial Int 2001;21 Suppl 3:S174-8.
85. Ellis EN, Yiu V, Harley F, Donaldson LA, Hand M, Warady BA, Wood EG; North American
Pediatric Renal Transplant Cooperative Study. The impact of supplemental feeding in young children on dialysis: a report of the North American Pediatric Renal Transplant
Cooperative Study. Pediatr Nephrol 2001 May;16(5):404-8.
86. Langlois V, Geary D, Murray L, Champoux S, Hebert D, Goodyer P. Polyuria and proteinuria in cystinosis have no impact on renal transplantation. A report of the North
American Pediatric Renal Transplant Cooperative Study. Pediatr Nephrol 2000
Nov;15(1-2):7-10. Erratum in: Pediatr Nephrol 2001 Feb;16(2):201.
87. Al-Uzri A, Stablein DM, A Cohn R. Post-transplant diabetes mellitus in pediatric renal transplant recipients: a report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Transplantation 2001;27;72(6):1020-4.
88. Bartosh SM, Fine RN, Sullivan EK. Outcome after transplantation of young patients with systemic lupus erythematosus: A report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Transplantation 2001;72(5):973-8.
89. Baum MA, Stablein DM, Panzarina VM, Tejani A, Harmon WE, Alexander SR. Loss of living donor renal allograft survival advantage in children with focal segmental glomerulosclerosis: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Kidney Int 2001;59:328-333.
B-8
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
90. Dharnidharka VR, Sullivan EK, Tejani A, Harmon WE. Risk factors for post-transplant lymphoproliferative disorder (PTLD) in pediatric kidney transplantation: A report of the
North American Pediatric Cooperative Study (NAPRTCS). Transplantation
2001;71(8):1065-8.
91. Fine RN, Ho PL, Tejani A. The contribution of renal transplantation to final adult height: a report of the North American Pediatric Cooperative Study (NAPRTCS). Pediatr
Nephrol 2001;16(12):951-6.
92. McDonald RA, Ho PL, Stablein DM, Tejani A. Rejection profiles of recent pediatric renal transplant recipients compared to historical controls: A report of the North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS). Transplantation
2001;(1):55-60.
93. Quan A, Sullivan EK, Alexander SR. Recurrence of hemolytic uremic syndrome after renal transplantation in children a report of the North American Pediatric Renal
Transplant Cooperative Study. Transplantation 2001;72:742-745.
94. Seikaly M, Ho PL, Emmett L, Tejani A. The 12th Annual Report of the North American
Pediatric Renal Transplant Cooperative Study: renal transplantation from 1987 through
1998. Pediatr Transplant 2001;5(3):215-31.
95. Neu AM, Ho PL, McDonald RA, Warady BA. Chronic dialysis in children and adolescents.
The 2001 NAPRTCS Annual Report, Pediatr Nephrol 2002 Aug;17(8):656-63.
96. Baum M, Ho M, Stablein D, Alexander S. Outcome of Renal Transplantation in
Adolescents with Focal Segmental Glomerulosclerosis. Pediatr Transplant 2002
Dec;6(6):488-92.
97. Dharnidharka VR, Ho PL, Stablein DM, Harmon WE, Tejani AH. Mycophenolate, tacrolimus and post-transplant lymphoproliferative disorder: a report of the North
American Pediatric Renal Transplant Cooperative Study. Pediatr Transplant 2002
Oct;6(5):396-9.
98. Dharnidharka V, Tejani A, Ho P, Harmon W. Post-Transplant Lymphoproliferative
Disorder in the United States: Young Caucasian Males are at Highest Risk. Am J
Transplant 2002;2(10):993-8.
99. Fine RN, Stablein D, Cohen AH, Tejani A, Kohaut E. Recombinant human growth hormone post-renal transplantation in children: A randomized controlled study of
NAPRTCS. Kidney Int 2002;62(2):688-696.
100. Furth SL, Stablein D, Fine RN, Powe NR, Fivush BA. Adverse clinical outcomes associated with short stature at dialysis initiation. A report of the North American
Pediatric Renal Transplant Cooperative Study. Pediatrics 2002;109(5):909-13.
B-9
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
101. Smith J, Ho M, McDonald R, Renal Transplant Outcomes in Adolescents: A Report of the
North American Renal Transplant Cooperative Study (NAPRTCS). Pediatr Transplant
2002;6(6):493-9.
102. Tejani A, Ho PL, Emmett L, Stablein DM. Reduction in acute rejections decreases chronic rejection graft failure in children: A report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Am J Transplant 2002;2(2):142-7.
103. Fine RN, Ho M. The role of APD in the management of pediatric patients: a report of the
North American Pediatric Renal Transplant Cooperative Study. Semin Dial 2002 Nov-
Dec;15(6):427-9.
104. Baum MA, Ho PL, Stablein DM, Alexander SR. Outcome of renal transplantation in adolescents with focal segmental glomerulosclerosis: A report of the North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS). Pediatr Transplant 2002
Dec;6(6):488-492.
105. Leonard MB, Donaldson LA, Ho M, Geary DF. A prospective cohort study of incident maintenance dialysis in children: An NAPRTC study. Kidney Int 2003 Feb;63(2):744-
755.
106. McDonald RA, Smith JM, Stablein D, Harmon WE. Pretransplant peritoneal dialysis and graft thrombosis following pediatric kidney transplantation: a NAPRTCS report.
Pediatr Transplant 2003 Jun;7(3):204-8.
107. Neu AM, Ho PL, Fine RN, Furth SL, Fivush BA. Tacrolimus vs. cyclosporine A as primary immunosuppression in pediatric renal transplantation: a NAPRTCS study. Pediatr
Transplant 2003 Jun;7(3):217-22.
108. Seikaly MG, Ho PL, Emmett L, Fine RN, Tejani A. Chronic renal insufficiency in children: the 2001 Annual Report of the NAPRTCS. Pediatr Nephrol 2003 Aug;18(8):796-804.
109. Davis ID, Ho M, Hupertz V, Avner ED. Survival of childhood polycystic kidney disease following renal transplantation: the impact of advanced hepatobiliary disease. Pediatr
Transplant 2003 Oct;7(5):364-9.
110. Mitsnefes M, Ho PL, McEnery PT. Hypertension and progression of chronic renal insufficiency in children: a report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). J Am Soc Nephrol 2003 Oct;14(10):2618-22.
111. Warady BA, Ho M. Morbidity and mortality in children with anemia at initiation of dialysis.
Pediatr Nephrol 2003 Oct;18(10):1055-62.
112. Smith JM, Nemeth TL, McDonald RA. Current immunosuppressive agents: efficacy, side effects, and utilization. Pediatr Clin North Am 2003 Dec;50(6):1283-300.
B-10
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
PUBLICATIONS
113. Ferrara E, Lemire J, Grimm PC, Reznik VM, Mendoza SA, Leake JA, Benador NM.
Mycobacterial peritonitis in pediatric peritoneal dialysis patients. Pediatr Nephrol 2004
Jan;19(1):114-7.
114. Dharnidharka VR, Stablein DM, Harmon WE. Post-transplant infections now exceed acute rejection as cause for hospitalization: a report of the NAPRTCS. Am J Transplant 2004
Mar;4(3):384-9.
115. Hinds AC. Obstructive uropathy: considerations for the nephrology nurse. Nephrol Nurs J
2004 Mar-Apr;31(2):166-74, 179; quiz 180-1.
116. Leonard MB, Stablein DM, Ho M, Jabs K, Feldman HI; North American Pediatric Renal
Transplant Cooperative Study. Racial and center differences in hemodialysis adequacy in children treated at pediatric centers: a North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS) report. J Am Soc Nephrol 2004
Nov;15(11):2923-32.
117. Dharnidharka VR, Stablein, DM. IL-2 receptor antibodies and malignancy: an analysis of early pediatric renal transplant registry data. Am J Transplant 2004;8(Suppl):1060A.
B-11
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
1. North American Pediatric Renal Transplant Cooperative Study. Demographics, immunotherapy and outcome of pediatric renal transplants in North America: A report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). Presented, ASN, San Antonio, 1988.
2. North American Pediatric Renal Transplant Cooperative Study. Patient and graft survival of renal transplants in North American children. A report of the North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS). Presented, APS,
Washington, DC, 1989.
3. North American Pediatric Renal Transplant Cooperative Study. Growth in North American children one year after renal transplantation. A report of the North American
Pediatric Renal Transplant Cooperative Study. Presented, ASN, Washington, DC,
1989.
4. North American Pediatric Renal Transplant Cooperative Study. Mortality and morbidity of renal transplantation in North American children. A report of the North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS). Presented, VII
Congress Int Ped Nephrol Assoc, Toronto, 1989.
5. North American Pediatric Renal Transplant Cooperative Study. Comparative rejection and graft survival rates of live related donor transplant recipients and cadaver kidney recipients in North American children. Presented, IV Congress Europ Soc Organ
Transplant, Barcelona, 1989.
6. North American Pediatric Renal Transplant Cooperative Study. Incidence, diagnosis, treatment and outcome of acute rejection in North American children receiving a renal transplant. A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1989.
7. Harmon W, Alexander SR, Stablein DM. Graft thrombosis as a cause of graft failure in pediatric renal transplant recipients: A report of the North American Pediatric Renal
Transplant Cooperative Study. Presented, ASTP, Chicago, 1990.
8. North American Pediatric Renal Transplant Cooperative Study. Renal transplant outcome in
North American children. A report of the NAPRTCS. Presented, XIth Int Congress
Nephrol, Tokyo, 1990.
9. North American Pediatric Renal Transplant Cooperative Study. Evaluation of graft survival relative to the initiation of cyclosporine and ATG/ALG or OKT-3 in pediatric cadaver renal transplants. A report of the NAPRTCS. Presented, XIIIth Int Congress
Transplant Soc, San Francisco, 1990.
10. North American Pediatric Renal Transplant Cooperative Study. Renal allograft outcome in
North American children - A report of the NAPRTCS. Presented, ASN, Washington,
DC, 1990.
B-12
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
11. North American Pediatric Renal Transplant Cooperative Study. Maintenance immunosuppression therapy (MIT) and renal outcome in North American children. A report of the NAPRTCS. Presented, ASTP, Chicago, 1991.
12. North American Pediatric Renal Transplant Cooperative Study. The effect of donor age on graft survival in pediatric cadaver renal transplant recipients: A report of the
NAPRTCS. Presented, ASTP, Chicago, 1991.
13. Tejani A, Stablein D, Fine R. Predictive factors of sustained growth post-transplant in renal transplant recipients: A report of the North American Renal Transplant Cooperative
Study. Presented, APS, New Orleans, 1991.
14. Tejani A and Stablein D. Recurrence (rec) of focal segmental glomerulosclerosis (FSGS) post transplantation (PTr): A report of the North American Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASN, Boston, 1991.
15. Harmon W, Alexander S, Tejani A, Stablein D. Pretransplant blood transfusions (PBTx) provide no benefit to children who receive renal transplants (Rtx): A report of the
North American Renal Transplant Cooperative Study (NAPRTCS). Presented,
ASTP, Chicago, 1992.
16. Tejani A, Stablein D, Fine R, Alexander S, Harmon W. Risk factors (RF) for cadaver transplant (CT) graft failure in North American children. A report of the North
American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Presented,
APS, Washington, DC, 1992.
17. Baluarte HJ, Gruskin A, Ingelfinger J, Stablein D, Tejani A. Analysis of hypertension in the
North American Pediatric Renal Transplant Cooperative Study. Presented, ASTP,
Houston, 1993.
18. Friedman A, Stablein D, Tejani A. Four-year follow-up of renal function after renal transplantation: Report of NAPRTCS. Presented, 1st Int Congress Tx, Minneapolis,
1993.
19. Tejani A, Sullivan EK, Harmon W, Alexander S, Fine R, Lilienfeld D. Post transplant deaths and factors that influence mortality rate (MR) in North American children. Presented,
ASTP, Houston, 1993.
20. Harmon W and Stablein D. Causes of diminished graft survival in infants receiving renal transplants (RTx): A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1994.
21. Fine RN, Avner E, Sullivan EK, Tejani A. Pre-emptive transplantation (PED) in children: improved graft survival rates. (Report of the North American Pediatric Renal
Transplant Cooperative Study - NAPRTCS). Presented, ASN, Orlando, 1994.
B-13
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
22. Jabs K, Sullivan EK, Avner E, Harmon W. Alternate day steroid dosing improves growth without adversely affecting graft survival or long-term graft function: A report of the
North American Pediatric Transplant Cooperative Study (NAPRTCS). Presented,
ASTP, Chicago, 1994.
23. McEnery PT, Kashtan CE, Stablein DM, Tejani A. Renal Allograft survival according to primary diagnosis in North American children. A report of NAPRTCS. Presented,
APS/SPR, Seattle, 1994.
24. Sullivan EK, Tejani A. Steady Improvement in cadaver (C) graft survival (GS) among North
American children. A 5 year appraisal by North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASN, Orlando, 1994.
25. Tejani A, Kashtan C, McEnery PT, Stablein DM. Renal allograft survival according to primary diagnosis in North American children. A report of NAPRTCS. Presented,
ASTP, Chicago, 1994 and SPR, Seattle, 1994.
26. Tejani A, Stablein D, Harmon W, Alexander S, Fine R. The impact of first rejection on graft survival in North American children. A report of the North American Pediatric Renal
Transplant Cooperative Study. Presented, APS/SPR, Seattle, 1994.
27. Tejani A, Stablein D, Sullivan EK, Fine R, Harmon W, Alexander S. The impact of the first rejection on graft survival in children. Presented, ASTP, Chicago, 1994.
28. Tejani A, Sullivan EK. Higher Maintenance Cyclosporine Doses in MG/KG (MCD) Prevent
Graft Failure in Children. A Special Study of North American Pediatric Renal
Transplant Cooperative Study. Presented, ASN, Orlando, 1994.
29. Bock G, Elshihabi I, Ellis E, Sullivan EK, Miller D, Gimon D. Serious cytomegalovirus (CMV) infections following pediatric renal transplantation (RTx): II. Short and long-term effects of viral prophylaxis (PX). Presented, ASN, November 1995.
30. Bock G, Ellis E, Elshihabi I, Sullivan EK, Miller D, Gimon D. Serious cytomegalovirus (CMV) infections following pediatric renal transplantation (RTx): I. Changing patterns and risk factors. Presented, ASN, November 1995.
31. Fine R, Sullivan EK, Alexander S, Tejani A. Demography of chronic renal insufficiency (CRI) in North American children. Presented, ASN, November 1995.
32. Tejani A, Fine RN, Alexander S, Harmon W, Sullivan EK. Growth post transplantation (Tx) -
A long term analysis of North American children receiving a renal allograft.
Presented, ASTP, Chicago, 1995.
33. Tejani A, Sullivan EK. Growth post transplantation (Tx) - Long term analysis by the North
American Pediatric Renal Transplant Cooperative Study. Presented, APS/SPR, San
Diego, 1995.
B-14
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
34. Tejani A, Sullivan EK, Fine RN, Harmon W, Alexander S. Steady improvement in cadaver graft survival (GS) among North American children. A 5 year appraisal by North
American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Presented,
APS/SPR, San Diego, 1995.
35. Tejani A, Sullivan EK, Stablein D, for the North American Pediatric Renal Transplant
Cooperative Study. Clinical co-relates of graft failure due to chronic rejection in
North American children. Presented, ASTP, Chicago, 1995.
36. Jabs K, Sullivan EK, Harmon W. Excess graft losses in adolescent recipients of living donor
(LD) renal transplants (TX): A report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Presented, ASTP, Dallas, 1996.
37. Singh A, Stablein DM, Tejani A. Risk factors for vascular thrombosis (VT) in pediatric renal transplantation. Presented, ASTP, Dallas, 1996.
38. Tejani A, Stablein DM, Fine RN, Harmon WE, Alexander SR. Steady improvement in post 1 year half-life of pediatric renal transplants. Presented, ASTP, Dallas, 1996.
39. Al-Uzri A, Sullivan EK, Harmon W, Fine, RN. Living unrelated renal transplantation in children: report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). Presented, ASTP, Chicago, 1997.
40. Benfield MR, Herrin J, Tejani A, Feld L, Rose S, Stablein DM. Safety of kidney biopsy in pediatric transplantation: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1997.
41. Ellis EN, Hand M, Briscoe DM, Harley F, Yiu V, Donaldson LA, Warady BA, Wood EG.
Nutrition and outcome of young children on dialysis: A report of the North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS). Presented, ASN, San
Antonio, 1997.
42. Furth S, Donaldson LA, Neu AM, Fine R, Fivush B. Effect of renal diagnosis on height SDS in children with CRI: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASN, San Antonio, 1997.
43. Furth S, Sullivan EK, Neu AM, Tejani A, Fivush BA. Varicella requiring hospitalization in the first year after renal transplantation: A report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1997.
44. Osorio A, Sullivan EK, Bryan C, Alexander S, Warady BA. ABO - mismatched renal transplantation (RT) in children: A report of the North American Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1997.
45. Schurman SJ, Stablein DM, Perlman SA. Center volume effects in pediatric renal transplantation: A report of the North American Pediatric Renal Transplantation
Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1997.
B-15
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
46. Warady BA, Bashir M, Donaldson LA. Fungal peritonitis in children receiving long-term peritoneal dialysis: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASN, San Antonio, 1997.
47. Warady BA, Sullivan EK, Kohaut E. Renal transplantation in children with sickle cell disease: A report of the North American Pediatric Renal Transplant Cooperative
Study (NAPRTCS). Presented, ASTP, Chicago, 1997.
48. Wood E, Hand M, Donaldson LA, Sullivan EK, Briscoe D, Harley F, Yiu V, Warady BA, Ellis
E. Risk factors for mortality in infants and young children on dialysis: A report of the
North American Renal Transplant Cooperative Study (NAPRTCS). Presented, ASN,
San Antonio, 1997.
49. Al-Uzri A, Cohn RA, Sullivan EK. Post transplant diabetes mellitus in pediatric renal transplant recipients: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1998.
50. Al-Uzri A, Cohn RA, Sullivan EK. Post transplant diabetes mellitus in pediatric renal transplant recipients: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, 3 rd International Congress for Pediatric
Transplantation, Boston, 1998.
51. Benfield MR, Tejani A, Stablein DM. Trend in immunosuppressive therapy: A report of the
North American Pediatric Cooperative Study (NAPRTCS). Presented, 3 rd
International Congress for Pediatric Transplantation, Boston, 1998.
52. Brouhard BH, Lawry KW, Drotar D, Davis I. Cognitive functioning in children with renal failure and post transplantation: A report of the North American Pediatric
Cooperative Study (NAPRTCS). Presented, ASTP, Chicago, 1998.
53. Brouhard BH, Lawry KW, Drotar D, Davis I. Cognitive functioning in children with renal failure and post transplantation: A report of the North American Pediatric
Cooperative Study (NAPRTCS). Presented, 3 rd International Congress of
Transplantation, Boston, 1998.
54. Cohn RA, Sullivan EK. Acute rejection probability and severity are declining after pediatric renal transplantation: A report of the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, 3 rd International Congress for Pediatric
Transplantation, Boston, 1998.
55. Ding R, Schachter AD, Sharma VK, Strehlau J, Li D, Vasconcellos L, Zheng XX, Stablein
DM, Harmon WE, Tejani A, Strom TB, Suthanthiran M. For the NAPRTCS/CCTPT study group: Intrarenal expression of cytotoxic attack molecules during acute rejection of renal allografts in pediatric recipients. Presented, ASTP, Chicago, 1998.
B-16
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
56. Fine RN, Tejani A. Growth post-renal transplantation in children: 11 year North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS) report. Presented, 3 rd
International Congress for Pediatric Transplantation, Boston, 1998.
57. Hebert D, Sullivan EK. Malignancy and post-transplant lymphoproliferative disorder (PTLD) in pediatric renal transplant recipients: A report of the North American Pediatric
Renal Transplant Cooperative Study (NAPRTCS), Presented, 3 rd International
Congress for Pediatric Transplantation, Boston, 1998.
58. Jabs K, Sullivan EK. Morbidity following renal transplantation: A report of the North
American Pediatric Renal Transplant Cooperative Study (NAPRTCS), Presented, 3 rd
International Congress on Pediatric Transplantation, Boston, 1998.
59. Kohaut EC, Tejani A, Fine R, Stablein DM. Adequacy of care for children with chronic renal insufficiency: A report of the North American Pediatric Renal Transplant Cooperative
Study (NAPRTCS). Presented, APS/SPR, New Orleans, 1998.
60. Schachter AD, Strehlau J, Kim YS, Vasconcellos L, Zheng XX, Harmon WE, Herrin JT,
Tejani A, Strom TB. Increased intragraft angiotensinogen gene expression in posttransplant recurrent FSGS. Presented, 3 rd International Congress on Pediatric
Transplantation, Boston, 1998.
61. Sorof JM, Sullivan EK, Portman RJ, Tejani A. The need for anti-hypertensive medication
(anti-HTN) independently predicts graft failure in pediatric renal transplant recipients:
A report of the North American Pediatric Renal Transplant Cooperative Study
(NAPRTCS). Submitted, ASN, 1998.
62. Tejani A, Donaldson L, Lawry K, McGowan K, Dotar D, Emmett L, Brouhard B, Harmon WE,
Alexander SR, Kohaut E, Davis I, Ettenger R, Weiss N, Baqi N, Cohn R. For the
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS): Quality of life of children post-transplantation compared to children on dialysis. Presented,
ASTP, Chicago, 1998.
63. Tejani A, Sullivan EK, Alexander SR, Harmon WE, Kohaut E, Fine RN. For the North
American Pediatric Renal Transplant Cooperative Study (NAPRTCS): The impact of donor source, pre-operative immunotherapy and prophylactic antibody therapy on first rejection episodes in children. Presented, ASTP, Chicago, 1998.
64. Tejani A, Stablein DM, Harmon WE, Fine RN, Alexander ST, Kohaut EC. Dramatic improvement in cadaver donor graft survival of North American children. Presented,
ASN, 1998.
65. Bartosh SM, Fine RN, Sullivan EK. Outcome after transplantation of young patients with systemic lupus erythematosus (SLE): A North American Pediatric Transplant
Cooperative Study (NAPRTCS) Report. Presented at, Am Soc Transplantation,
Chicago, 1999.
B-17
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
66. Baum MA, Stablein D, Panzarino V, Tejani A, Harmon WE. Graft loss due to recurrence eliminates the graft survival advantage of living donor (LD) over Cadaveric (CD) renal transplants (Tx) in children with focal segmental glomerulosclerosis (FSGS): A report of the North American Pediatric Transplant Cooperative Study (NAPRTCS).
Presented, Am Soc Transplantation, Chicago, 1999.
67. Dharnidharka VR, Sullivan EK, Tejani AH, Harmon WE. Risk factors for post transplant lymphoproliferative disorder (PTLD): An analysis of the cases in the North American
Pediatric Renal Transplant Cooperative Study (NAPRTCS). Presented, Am Soc
Transplantation, Chicago, 1999.
68. Fine RN, Sullivan EK, Blethen S, Kohaut E. Prior rhGH and renal transplant function.
Presented, Am Soc Transplantation, Chicago, 1999.
69. Leonard MB, Sullivan EK, Jabs K, Feldman HI. Comparison of mortality risks of dialysis and renal transplantation in children: A report of the North American Pediatric
Cooperative Study (NAPRTCS). Presented, Am Soc Transplantation, Chicago,
1999.
70. Tejani A, Sullivan EK. Do six-antigen matched cadaver donor (CAD) kidneys provide better graft survival to children compared to one-haploidentical living-related (LRD) transplants? A report of the North American Pediatric Cooperative Study
(NAPRTCS). Presented, Am Soc Transplantation, Chicago, 1999.
71. Vats A, Donaldson LA, Fine RN, Chavers B. Outcome of renal transplantation in North
American children on peritoneal dialysis: A report of the North American Pediatric
Renal Transplant Cooperative Study (NAPRCTS). Presented, Am Soc
Transplantation, Chicago, 1999.
72. Bartosh SM, Stablein DM. Tacrolimus as primary immunosuppression for children receiving non-primary renal transplants: A report of the North American Pediatric Cooperative
Study (NAPRTCS). Presented, International Pediatric Transplant Association .
Venice, Italy, 2000.
73. Elshihabi I, Stablein DM, Tejani A: Emerging immunosuppressive profile of pediatric renal transplant recipients and its impact on graft survival. Presented, Transplant 2000
AST/ASTS Joint Meeting. Chicago, 2000.
74. McDonald R, Ho PL, Stablein DM, Tejani A. Acute rejection rate, time to first rejection and rejection reversals comparing the 1987-1989 pediatric renal transplant recipient cohort to the 1997-1999 cohort. A report of the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Presented, Transplant 2000 AST/ASTS
Joint Meeting. Chicago, 2000
B-18
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
75. Schurman S, Stablein DM, Garin EH, Tejani A. For the North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS): Impact of puberty on renal function in children with chronic renal insufficiency (CRI). Presented, PAS/AAP Joint Meeting,
2000.
76. Stablein DM, Emmett L, Tejani A. After six thousand transplants where are we? The state of pediatric renal transplantation in North America. Presented, First IPTA Congress.
Venice, Italy, 2000.
77. Tejani A, Harmon WE, Benfield M, Elshihabi I, McDonald R, Stablein D, Rose S, Strom T,
Suthanthiran M, for the CCTPT study group: A randomized prospective multicenter trial of T-cell antibody induction therapy in pediatric renal transplantation. Presented,
Transplant 2000 AST/ASTS Joint Meeting. Chicago, 2000.
78. Tejani A, Sullivan EK: Should living-related renal transplant be performed for primary oxalosis? Presented, Transplant 2000 AST/ASTS Joint Meeting. Chicago, 2000.
79. Dharnidharka VR, Ho PL, Stablein DM, Harmon WE, Tejani A. Initial immunosuppression with Mycophenolate or Tacrolimus is not associated with increased risk for posttransplant lymphoproliferative disorder: a North American Pediatric Renal
Cooperative Study (NAPRTCS) Report. Presented, AST. Chicago, 2001.
80. Harmon WE, Stablein DM, Tejani A. A rejection-free milieu provides accelerated growth, better graft function and superior graft survival in children. Presented, Transplant
2001 Joint Meeting.
81. Neu AM, Ho PL, Furth SL, Fine RN, Fivush BA. Hospitalization for CMV in pediatric renal transplant patients treated with MMF vs. Azathioprine: a North American Pediatric
Renal Cooperative Study (NAPRTCS) Report. Submitted, IPNA. Seattle, 2001.
82. Neu AM, Ho PL, Furth SL, Fine RN, Fivush BA. Tacrolimus vs. Cyclosporine as primary immunosuppression in pediatric renal transplant patients: a North American
Pediatric Renal Cooperative Study (NAPRTCS) Report. Presented, IPNA. Seattle,
2001.
83. Wong CS, Ho PL, Stablein DM, Alexander S, Warady B, Tejani A, Watkins SL. Risk Factors for anemia during erythropoietin therapy among pediatric dialysis patients: a North
American Pediatric Renal Cooperative Study (NAPRTCS) Report. Presented, ASN.
Toronto, 2001.
84. Bartosh S, Ho PL, Tejani A. Racial differences in donor source, matching, rejection and outcome in Pediatric renal transplantation (PRT). Presented, ATC. Washington,
DC, 2002.
85. Benfield M, Tejani A, Ho PL. Comparative study of the safety, efficacy, and practice patterns of Monoclonal antibodies (MAbs) in pediatric renal transplantation (PRT).
Presented, ATC. Washington, DC, 2002.
B-19
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
86. McDonald RA, Ho PL, Tejani A. The impact of the maintenance dose of cyclosporine (cys) at day-30: Efficacy comparison of an earlier (e) (1990-1994) vs. a recent (r)
(1995-2001) era. Submitted, ATC. Washington, DC, 2002.
87. Tejani A, Stablein DM, Ho PL. Calculated creatinine clearance (CCC) as the most promising candidate surrogate end point for clinical trials. Presented, ATC.
Washington, DC, 2002.
88. Neu AM, Ho M, Furth SL, Fine RN, Fivush BA. Tacrolimus vs. cyclosporine as primary immunosuppression in pediatric renal transplant patients: a NAPRTCS study.
Presented, ATC. Washington, DC, 2002. (Published: Pediatr Transplantation 2003:
7:217-222. © 2003 Blackwell Munksgaard)
89. Kist-van Holthe JE, Ho PL, Harmon WE, Bau MA. Outcome of children after renal transplantation for Wilms tumor and Drash syndrome: a report of the North American
Pediatric Renal Transplant Cooperative Study. Presented, ATC. Washington, DC,
2003.
90. Bartosh SM, Ho PL, Stablein DM, Harmon WE. Improving adult height for pediatric renal transplant recipients: a report from the North American Pediatric Renal Transplant
Cooperative Study (NAPRTCS). Presented, ATC. Washington, DC, 2003.
91. Sarwal M, Vidhun J, Ho M, Salvatierra O. Single center and NAPRTCS analyses confirm unprecedented growth patterns in steroid-free immunosuppression. Presented, ATC.
Washington, DC, 2003.
92. Smith JM, McDonald RA, Stablein DM, Singh A, Harmon WE. The impact of interleukin-2 receptor antibodies on renal allograft thrombosis: an analysis of the North American
Pediatric Renal Cooperative Study (NAPRTCS). Presented, ATC. Washington, DC,
2003.
93. Harmon WE, Stablein DM, Sayegh MH. Trends in immunosuppressive strategies in pediatric kidney transplantation. Presented, ATC. Washington, DC, 2003.
94. Dharnidharka V, Stablein DM, Harmon WE. Risk of hospitalization due to infection now exceeds risk due to acute rejection at early and late time points in pediatric renal transplant recipients. Presented, ATC. Washington, DC, 2003.
95. Bartosh, Sharon. Improving outcomes in the very young renal transplant recipient: a report from the North American Pediatric Renal Transplant Co-Operative Study
(NAPRTCS). Presented, IPTA. Rio de Janeiro, Brazil, 2003.
96. Bartosh S, Ho PL, Harmon W. Successful steroid withdrawal in pediatric renal transplant recipients: a NAPRTCS report. Presented, IPTA. Rio de Janeiro, Brazil, 2003.
B-20
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
ABSTRACTS AND PRESENTATIONS
97. Mitsnefes MM, Hanevold CD, and Ho PL. Obesity and long-term outcome in children and adolescents after renal transplantation: a report of North American Pediatric Renal
Transplant Cooperative Study (NAPRTCS). Presented, APS/SPR. Seattle, 2003.
98. Kist-van Holthe J. Outcome of children after renal transplantation for Wilms tumor and Drash syndrome: a report of the North American Pediatric Renal Transplant Cooperative
Study. Presented, World Congress of Nephrology. Berlin, Germany, 2003.
99. Harmon W, Meyers K, McDonald R, Ingelfinger J, McIntosh M, Tinckam K, Najafian N,
Sayegh M. Calcineurin inhibitor (CNI) avoidance in pediatric renal transplantation
(RTx). Presented, ASN. St. Louis, 2004.
100. Mitsnefes M, Stablein D. Hypertension in Children on Chronic Dialysis: A Report of the
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS).
Presented, ASN. St. Louis, 2004.
101. Warady BA, Zobrist H, Zu Z. Sodium Ferric Gluconate Complex (SFGC) Therapy in children receiving hemodialysis: a randomized trial. Presented, ASN. St. Louis, 2004.
102. Furth SL, Cole SR, Mims MM, Munoz A, Warady BA. Design and methods of a prospective cohort study of chronic kidney disease in children (CKiD). Presented,
ASN. St. Louis, 2004.
103. Muir J, Greenberg J, Medeiros M, Sharma VK, Ding R, Muthukumar T, Fine R,
Suthanthiran M, August P. Increased TGF- beta2 Gene Expression in Black Children with Renal Disease. Presented, ASN. St. Louis, 2004.
104. Greenberg J, Muir J, Medeiros M, Muthukumar T, Fine R, August P, Suthanthiran M,
Sharma VK. TGF-beta2 protein levels in peripheral blood are higher in black children with kidney disease compared to their white counterparts. Presented, ASN. St. Louis,
2004.
105. Mitsnefes MM, Stablein D. Blood pressure control in children on long-term maintenance dialysis: the NAPRTCS Report. Presented, ASN. St. Louis, 2004.
106. Dharnidharka VR, Stablein, DM. IL-2 receptor antibodies and malignancy: an analysis of early pediatric renal transplant registry data. Presented, ATC. Boston, 2004. (Am J
Transplant 2004;8(Suppl):1060A).
107. Bartosh S, Stablein D , Fine RN. Recurrence of FSGS following pediatric kidney transplantation in the modern immunosuppression era: a NAPRTCS report.
Presented, ATC. Boston, 2004.
108. Braun MC, Stablein DM, Hamiwka LA, Bell L, Bartosh SM, Strife CF. Recurrence of
MPGN II in Renal Allografts: The NAPRTCS Experience. Presented, IPNA World
Congress, Adelaide, Australia, 2004.
B-21
APPENDIX C
SPECIAL STUDIES AND ANALYSES
Lead Investigator
2004
Eileen Ellis, M.D.
William Carey, M.D.
Vikas Dharnidharka, M.D.
Jodi Smith, M.D.
2003
Alicia Neu, M.D.
Vikas Dharnidharka, M.D.
Paul Hmiel, M.D. Ph.D.
Mark Mitsnefes, M.D.
Minnie Sarwal, M.D.
2002
Coral Hanevold, M.D.
Paul McEnery, M.D.
Michelle Baum, M.D.
2001
Alicia Neu, M.D.
Mark Mitsnefes, M.D.
Peter Yorgin, M.D.
Michael Braun, M.D.
Lorraine Bell, M.D.
Lorraine Hamiwka, M.D.
2000
Sharon Bartosh, M.D.
Susan Furth, M.D.
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
SPECIAL STUDIES AND ANALYSES
Topic Status
Factors related to long-term renal transplant function in children
Outcomes of renal replacement therapy initiated during the neonatal period (birth to three months)
BK virus nephropathy (BKVN) in pediatric renal transplantation
Tacrolimus vs. cyclosporine A as primary immunosuppression in pediatric renal transplantation: A
NAPRTCS study
Profile of infections post-transplantation in NAPRTCS
Graft survival after preemptive kidney transplantation
Completed
Completed
Completed
Published
Analysis of hypertension in children on chronic dialysis
Complete steroid free immunosuppression achieves unprecedented advantages in growth and graft function in pediatric renal transplantation: a single center and
NAPRTCS analysis
The impact of obesity on pediatric renal transplant outcome
Outcome of children with Wilms’ tumor as a primary diagnosis following renal transplant
Tacrolimus vs. Cyclosporine as primary immunosuppression in pediatric renal transplant patients
Blood pressure changes in renal function in children with chronic renal insufficiency
Comparison of effects of recombinant human growth hormone in children with chronic renal insufficiency and on dialysis
Transplantation in Children with Membranoproliferative
Glomerulonephritis*
Published
Presented; under review
Published
Presented
Published
Published
Published
Published
In Press; Published
Presented Outcomes of pediatric renal transplantation in children receiving non-primary transplants using tacrolimus as primary immunosuppression
Does poor growth predict morbidity and mortality in children with ESRD?
C-1
Published
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
SPECIAL STUDIES AND ANALYSES
Lead Investigator Topic Status
Ira Davis, M.D.
Peter Yorgin, M.D.
The impact of advanced hepatobility disease on the survival of patients with autosomal recessive polycystic kidney diseases following renal transplantation
The effect of recombinant human growth hormone in children with chronic renal insufficiency
Presented
Presented
1999
Richard Cohn, M.D.
Mary Leonard, M.D.
Alicia Neu, M.D.
Scott Schurman, M.D.
1998
Sharon Bartosh, M.D.
Outcome after renal transplantation for Drash Syndrome Presented
The dose of hemodialysis and outcomes in children Published
Presented Comparison of CMV disease in pediatric renal transplant patients receiving azathioprine vs. mycophenolate mofetil
Changes in renal function through puberty in children with chronic renal insufficiency
Presented
Outcomes in children with ESRD secondary to systemic lupus erythematosus
Published
Published Mary Leonard, M.D.
Valerie Panzarino, M.D.
Blanche Chavers, M.D.
Comparison of mortality risks of maintenance dialysis and renal transplantation
The effect of donor sex on renal allograft survival in pediatric renal transplantation
Outcome of renal transplantation in pediatric peritoneal dialysis patients
Post transplant diabetes mellitus
1997
Amira Al-Uzri, M.D.
1996
Scott Schurman, M.D.
Anup Singh, M.D.
Impact of transplant center volume on pediatric allograft outcome
Risk factors that impact on renal graft thrombosis in the
NAPRTCS registry
Bradley A. Warady, M.D.
Alicia Neu, M.D.
Fungal peritonitis in children receiving long-term peritoneal dialysis
Beneficial effect of maternal vs. paternal kidney donation in pediatric renal transplant patients
Risk factors in young children on dialysis Ellen Wood, M.D.
Amira Al-Uzri, M.D. Living-unrelated transplantation
1995
The NAPRTCS Investigators Controlled clinical trial in pediatric transplantation
Albert Quan, M.D. Graft outcome of patients with hemolytic uremic syndrome
Published
Published
Published
Published
Published
Published
Published
Published
Published
Presented
Published
C-2
Lead Investigator
Kathy Jabs, M.D.
Susan Furth, M.D.
Noosha Baqi, M.D.
1994
Glenn Bock, M.D.
Benjamin Brouhard, M.D.
Diane Hebert, M.D.
Bradley Warady, M.D.
1993
Aaron Friedman, M.D.
Kathy Jabs, M.D.
Ronald Kerman, M.D.
Melanie Kim, M.D.
Paul McEnery, M.D.
NORTH AMERICAN PEDIATRIC RENAL
TRANSPLANT COOPERATIVE STUDY
SPECIAL STUDIES AND ANALYSES
Topic Status
Graft loss and decreased function in adolescent recipients of LRD grafts
Vaccine-preventable illness in pediatric renal patients
Graft outcome of patients with Down Syndrome
Post-transplant CMV infection
Education status of children with ESRD
Post-transplant malignancies
Socioeconomic status and mortality of children with
ESRD
Presented
Published
Published
Published
Published
Presented
Completed
Serial serum creatinine assessments and graft outcome Completed
Daily versus alternate day steroids and graft outcome
MLR hyporesponsiveness
Graft outcome of patients with congenital nephrotic syndrome
Primary diagnosis and graft outcome
Published
Published
Published
Published
C-3