Cardiovascular Arousal in Individuals With Autism
advertisement

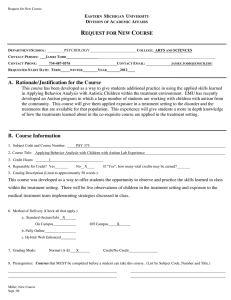
Cardiovascular Arousal in Individuals With Autism Matthew S. Goodwin, June Groden, Wayne F. Velicer, Lewis P. Lipsitt, M. Grace Baron, Stefan G. Hofmann, and Gerald Groden Despite the hypothesized link between arousal and behavior in persons with autism, there is a lack of idiographic research that directly assesses arousal responses to novel stimuli or social situations in this population. The current study used heart rate as a measure of sympathetic activity to compare arousal responses to the presentation of potentially stressful situations in five persons with autism and five age- and sex-matched typically developing individuals. Findings revealed that the group with autism showed significant responses to stressors only 22% of the time compared to the typically developing group, which showed significant responses 60% of the time. Interpretation of these results and methodological considerations for future research on arousal in persons with autism are discussed. A ccording to the Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV; American Psychiatric Association, 1994), autism is characterized by qualitative impairments in socialization, communication, and circumscribed interests, including stereotypical behavior patterns and behavioral rigidity to changes in routines. Although these symptomatic features are well established, it is unclear whether their origin lies simply in the absence of appropriate social skills and behavioral flexibility or arises from a qualitative difference in physiological arousal associated with these abilities. There is currently little research addressing the role of physiological arousal in autism despite earlier suggestions that neurophysiological factors implicated in the disorder can cause or contribute to significant problems in modulating arousal to social and sensory stimuli that are novel or unpredictable (Dawson, 1991; Dawson & Lewy, 1989; Kinsbourne, 1987; Ornitz, 1989; Ornitz & Ritvo, 1968), resulting in behavioral and physiological response patterns of either overarousal (Hutt, Hutt, Lee, & Ounsted, 1964) or underarousal (DesLauriers & Carlson, 1969). According to these arousal modulation theories of autism, both anxious and agitated responses characteristic of overarousal and passivity and lethargy characteris- tic of underarousal can interfere with this population’s ability to attend to, process, and interact with the environment and can result in the failure to learn normative behaviors and skills from other people (Lord & McGee, 2001; Prizant, Wetherby, Rubin, & Laurent, 2003; Siegel, 2003). Despite the hypothesized link between arousal and behavior in persons with autism, there is a lack of idiographic research that directly assesses this population’s arousal responses to novel stimuli or social situations. In an effort to systematically evaluate arousal responses in persons with autism, the present article reviews research on stress, stress-related anxiety, and physiological arousal and experimentally compares arousal responses to identified environmental stressors in five individuals with autism and five age- and sex-matched typically developing children. Stress, Anxiety, and Autism A stressor is any stimulus or circumstance that compromises an individual’s physical or psychological well-being (Lazarus & Folkman, 1984) and that requires an individual to make an adjustment (Selye, 1956). The consequences of stressors within an individual are collectively called the stress response. The stress response typically relates to three periods of interaction between the stressor and the individual’s response: (a) before the stressful event occurs, (b) during the stressor, and (c) after the stressor, when the individual may experience some of the residual effects of the event. Stress and Autism Literature suggests that many of the behaviors associated with autism are related to stress, as stressful events frequently precipitate the maladaptive behavior problems seen in this population, such as aggression, self-injury, tantrums, and destruction of property (Groden, Cautela, Prince, & Berryman, FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES VOLUME 21, NUMBER 2, SUMMER 2006 PAGES 100–123 VOLUME 21, NUMBER 2, SUMMER 2006 101 1994; Prior & Ozonoff, 1998). Stereotypic behaviors including echolalia, twirling, rocking, flicking, and hand flapping are also found to increase when this population is exposed to events commonly defined as stressors in the typical population (Howlin, 1998; Hutt & Hutt, 1968). Characteristics of persons with autism, including communication (e.g., Lord & Paul, 1997) and socialization deficits (e.g., Mundy & Stella, 2000), sensory problems (e.g., Baranek, 2002), and deficits in executive function (e.g., Rogers & Bennetto, 2000), may also make this population exceedingly vulnerable to stressors and limit their ability to cope (Groden, Cautela, Prince, & Berryman, 1994). Ineffective coping to stressors can lead to anxiety, and research suggests that anxiety is more prevalent in persons with autism, Asperger syndrome (AS), and Pervasive Developmental Disorder– Not Otherwise Specified (PDD-NOS) than in individuals who are typically developing, behaviorally disordered, or learning impaired. For example, Muris and colleagues (1998) interviewed parents of 44 children with either autism or PDD-NOS using the Anxiety Disorders section of the Diagnostic and Statistical Manual of Mental Disorders–Third Edition-Revised (DSM-III-R; American Psychiatric Association, 1987) and found that 84.1% met criteria for an anxiety disorder. In a similar study, Kim et al. (2000) conducted standardized interviews with parents of 59 children with either autism or AS and found a greater rate of anxiety in this group compared to a normative sample of 1,751 typical children from the community. Green et al. (2000) compared the psychological comorbidity of 29 individuals with AS to age-matched adolescents with a conduct disorder and found significantly higher levels of anxiety in the AS group. Findings from this study also revealed that 35% of the children with AS met the International Statistical Classification of Diseases and Related Health Problems–Tenth Revision (ICD-10; World Health Organization, 1992) criteria for generalized anxiety disorder and 10% met criteria for a specific phobia. In another study, Gillot et al. (2001) found that 15 children with high-functioning autism scored higher on measures of anxiety than both age-matched children with specific learning impairments and typically developing children. Lastly, Bellini (2004) examined anxiety in 41 adolescents with either high-functioning autism, AS, or PDD-NOS and found that 49% of the sample met criteria for social anxiety. Evidence also suggests that children with developmental disabilities, including those with autism, are more fearful than typically developing children (Evans, Canavera, Kleinpeter, Maccubbin, & Taga, 2005; Knapp, Barrett, Groden, & Groden, 1992; Matson & Love, 1990). Some of the most common fears identified for children with autism in these studies were associated with noises, presence of other people, and the dark. Individuals with autism have also been shown to exhibit panic-like levels of discomfort in response to environmental changes (Steingard, Zimnitzky, DeMaso, Bauman, & Bucci, 1997). Physiological Arousal and Autism The reviewed research suggests that stressful events are associated with behavioral challenges and anxiety in persons with autism. However, given this population’s difficulties identifying and describing their feelings through self-report (Hill, Berthoz, & Frith, 2004), traditional assessments of stress that utilize verbal communication (e.g., interviews, paper/pencil tests) have limited use in persons with autism. Contemporary researchers have attempted to overcome these unreliable selfreports and measure stress in this population by focusing on physiological reactivity during rest and performance on a task. Physiological Stress Responses Widespread changes in the cardiovascular system, the immune system, the endocrine glands, and brain regions involved in emotion and memory are activated when an organism is aroused by a stressor (Sapolsky, 1998). These physiological actions are controlled primarily by the autonomic nervous system (ANS) and enable an organism to respond adaptively to a stressor by preparing the body to fight or flee. The peripheral part of the nervous system, the ANS controls smooth muscle, cardiac muscle, and glands and includes both sympathetic and parasympathetic branches. The sympathetic branch is dominant in emergency conditions and initiates widespread and profound body changes, including acceleration in heart rate, dilation of the bronchioles, discharge of adrenaline into the bloodstream, inhibition of digestion, and elevation in blood pressure. The parasympathetic branch contains chiefly cholinergic fibers that tend to induce secretion, increase the tone and contractility of smooth muscles, and slow heart rate. In general, the sympathetic division is a catabolic system associated with emergencies; the parasympathetic, an anabolic system associated with vegetative processes. The sympathetic and parasympathetic divisions of the ANS work in antagonistic ways to maintain homeostasis: a dynamic equilibrium in which continuous changes occur, yet relatively uniform conditions prevail (Fox, 1996). Autonomic defensive responding is thought to be an indicator of arousal characterized in part by accelerations in the sympathetic nervous system, including heart rate (HR), respiration, and pupillary dilation, that fail to habituate to environmental stimuli of high intensity (Lacey, 1967). As such, it is thought to be an adaptive strategy that enables an organism to avoid or escape the potential dangers of threatening stimuli (Stern, Ray, & Quigley, 2001). Autonomic defensiveness to environmental stimulation has been observed previously in persons with autism. Cohen and Johnson (1977) measured cardiovascular reactivity during a variety of attention-demanding tasks in 10 individuals with autism and age-matched typical controls. Their tasks were designed to elicit either outward direction of attention (and intake of sensory input) or inward direction of attention (and relative rejection of external sensory FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 102 input). Results indicated that the group with autism had a tendency to reject external sensory input and elicit higher mean blood flow and lower peripheral vascular resistance. In a follow-up study, Kootz and Cohen (1981) measured HR, mean blood flow, and peripheral blood flow in 14 individuals with autism and 16 typical boys while resting, during social interaction, and while engaged in a reaction-time task. Findings revealed that the individuals with autism had elevated HR responses during the entire session and failed to show cardiovascular changes with sensory intake. Finally, Kootz, Marinelli, and Cohen (1982) studied 16 individuals with autism by measuring blood pressure and HR during a reaction-time task, social interaction, and at rest. In this observation, higher functioning individuals with autism displayed a normal pattern of cardiovascular responses to sensory intake, whereas lower functioning individuals showed increased cardiovascular reactivity and rejection of external sensory stimuli. Additional investigations have found that individuals with autism, compared to persons who are typically developing, generally respond with increased sympathetic tone at baseline (Ming, Julu, Brimacombe, Connor, & Daniels, 2005) and when exposed to environmental stimulation (Angus, 1970; Lake, Ziegler, & Murphy, 1977; Palkovitz & Wiesenfeld, 1980; Zahn, Rumsey, & van Kammen, 1987). Other studies, however, have found little to no differences between groups during experimental demands for socialization, attention, or habituation (Althaus, Mulder, Mulder, Aarnoudse, & Minderaa, 1999; Graveling & Brooke, 1978; Hutt, Forrest, & Richer, 1975; MacCulloch & Williams, 1971; Sigman, Dissanayake, Corona, & Espinosa, 2003; Stevens & Gruzelier, 1984; Toichi & Kamio, 2003; van Engeland, 1984). Only one study has found lower than normal arousal levels in persons with autism responding to social demands (DesLauriers & Carlson, 1969). Although these findings suggest some arousal differences in persons with autism, it is difficult to interpret this body of research due to methodological problems. For instance, most of these studies were conducted prior to the publication of the DSM-III-R criteria for autism, calling into question the validity of participant diagnoses. The physiological equipment used in the majority of these investigations was antiquated, likely contributing to participant discomfort, movement artifact, and equipment failures that resulted in a loss of data. Few of these studies incorporated a large sample of novel situations or stimuli to elicit significant arousal responses, and many failed to include a baseline measure from which to compare physiological reactivity. Finally, few studies reported on or controlled for background factors that can affect arousal responses, including comorbid psychological disorders, the participant’s use of pharmaceuticals, and general cardiovascular functioning. To control for some of the methodological problems associated with previous ANS studies of arousal in persons with autism, we conducted two feasibility studies for telemetrically assessing cardiovascular arousal to environmental stressors in individuals with autism. Groden et al. (2005) telemetrically recorded HR in 10 individuals ranging in age from 13 to 37 years (M = 24 years) who were positively identified with either autism or PDD-NOS. Cardiovascular responses were recorded at baseline and then while the participants engaged in four potentially stressful situations adapted from the Stress Survey Schedule for Persons with Autism and Developmental Disabilities (SSS; Groden et al., 2001). The SSS is a psychometrically sound survey instrument for rating the severity of perceived stress reactions to commonly identified stressors in the lives of persons with autism and developmental disabilities. It contains 49 items/situations that relate to eight dimensions of stress, including changes and threats, anticipation/uncertainty, unpleasant events, pleasant events, sensory/personal contact, food-related activity, social/environment interactions, and ritual-related stress. The potentially stressful situations adapted from the SSS used in the study included losing at a game, eating a preferred food, having a change in staff, and having unstructured time. Using interrupted time series analysis, the data for each participant were examined to see if mean HR responses were significantly different during each stressor phase compared with mean HR during baseline. Results illustrated good compliance with the HR monitor and arousal to all four stressors in some of the participants. In an effort to provide a wider sample of potential stressors that can elicit significant arousal responses in this population, Goodwin et al. (2004) repeated the experimental design and analysis plan from Groden et al. (2005) in five individuals with autism ranging in age from 12 to 20 years (M = 15 years). Cardiovascular reactions were assessed while the participants engaged in three previously untested stressors from the SSS, including exposure to a loud noise, engagement in a difficult task, and attending to a remote control robot (an unpredictable stimulus). This study also used a more sophisticated, wireless HR monitor (LifeShirt, Vivometrics, Inc.) that records concomitant motor movements. Results illustrated that participants tolerated the new ambulatory monitor and showed some significant arousal responses to all three added stressors. The present investigation sought to further replicate the measurement protocol from Groden et al. (2005) and Goodwin et al. (2004) and control for some remaining methodological problems associated with previous ANS assessments of arousal in persons with autism. Controlling for background factors that can affect cardiovascular responses, including comorbid psychological disorders, use of pharmaceuticals, and general cardiovascular functioning, the current study experimentally compared arousal responses to identified environmental stressors in five individuals with autism and five age- and sex-matched typically developing children. A series of 10 single-subject time series designs was used. The singlesubject designs consisted of 14 phases where resting tasks alternated with potentially stressful tasks. Sessions began with a baseline phase. After the baseline phase the participants engaged in six potentially stressful situations. The potentially VOLUME 21, NUMBER 2, SUMMER 2006 103 stressful situations alternated with rest phases. In addition, a physical exertion phase was used to ensure that participants could demonstrate an increase in HR significantly greater than baseline. Given the reviewed literature on stress, stress-related anxiety, and ANS arousal findings in persons with autism, it was hypothesized that the group with autism would have significantly greater cardiovascular reactivity, as compared to baseline, to a greater number of environmental stressors than the group of typically developing peers. Method Participants Two groups of children with parental consent participated in this study. The first group consisted of five males with autism, none of whom were included in the feasibility studies described earlier. They ranged in age from 8 to 18 years (M = 13.8, SD = 4.24) and were recruited from the Groden Center, a day program serving behavioral and academic needs of children with developmental disabilities. Diagnoses were made by a licensed psychologist familiar with autism using DSM-IV guidelines, the Childhood Autism Rating Scale (CARS; Schopler, Reichler, & Renner, 1986), and previous psychiatric reports. Participant cognitive abilities as assessed either by standardized intelligence measures (e.g., Stanford-Binet Intelligence Scale–Fourth Edition [Thorndike, Hagen, & Sattler, 1986]; Leiter International Performance Scale–Revised [Roid & Miller, 1997]) or scales of cognitive development (e.g., Bayley Scales of Infant Development–Second Edition [Bayley, 1993]) ranged from 24 to 38 (M = 31) and 5 months to 24 months, respectively. A familiar staff person also completed a CARS for each participant with autism. Scores on the CARS ranged from 31.5 to 43.5 (M = 39), placing the sample in the moderately to severely autistic range. Four of the five participants with autism used spoken language as their primary method of communication, and one participant used sign language. The second group was composed of five typically developing, chronological age- and sex-matched individuals. Typically developing participants were children of staff members at the Groden Center recruited from advertisements posted at the center. None of the participants in either group were prescribed any psychiatric medications and none had documented comorbid disorders (e.g., attention-deficit/ hyperactivity disorder, obsessive-compulsive disorder, seizure disorder) at the time of the study. Typically developing participants and participants with autism were also assessed for high blood pressure using diastolic and systolic measures and found to be normotensive (< 90 mmHg diastolic blood pressure). Characteristics of the 10 participants are presented in Table 1. Setting Participants were seated in a comfortable chair in a soundattenuated room with low-level incandescent lighting. A oneway mirror provided discrete viewing capabilities from an adjacent observation room. A familiar person accompanied the participants to increase comfort with the setting and experimental phases. Instruments Cardiovascular responses were recorded using the LifeShirt (Vivometrics, Inc.), a noninvasive telemetric recording device that continuously (i.e., beat-to-beat) stores electrocardiograph (ECG) data on a portable battery-powered electronic recorder TABLE 1 Participant Characteristics Age (years) Sex Diagnosis Primary method of communication Diastolic pressure Systolic pressure Cognitive development/IQ CARS Total score Autism M.L. J.L. S.E. M.C. A.F. 8 10 16 17 18 Male Male Male Male Male Autism Autism Autism Autism Autism Verbal Verbal Verbal Verbal Sign language 58 64 84 70 66 102 110 136 128 124 32b 5 mo.a 38b 18–24 mo.a 24c 36 43.5 31.5 39 42.5 Typically developing B.A. C.N. D.P. D.V. S.M. 8 10 16 17 18 Male Male Male Male Male —————- —————- 68 62 74 66 72 96 106 106 98 118 Participant Note. CARS = Childhood Autism Rating Scale (Schopler, Reichler, & Renner, 1986). a Bayley Scales of Infant Development-Second Edition (Bayley, 1993). bStanford-Binet Intelligence Scale-Fourth Edition (Thorndike, Hagen, & Sattler, 1986). c Leiter International Performance Scale-Revised (Roid & Miller, 1997). FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 104 worn on the body (for description see Wilhelm, Roth, & Sackner, 2003). The LifeShirt also collected motor movements and changes in posture positions using a dual-axis accelerometer positioned on the anterior surface of the rib cage. Movement data were obtained for the present study to control for HR responses attributable to physical demands. All of the information stored in the electronic recorder was downloaded to a PC computer as an ASCII file and exported to Excel in preparation for statistical analyses. Procedure Preobservation Procedure. To increase comfort and compliance with the stress assessment, each participant was introduced to the laboratory setting and heart monitor prior to the experimental session. For the participants with autism, laboratory visits occurred once a day for a week prior to being observed. For the typically developing participants, a minimum of 30 minutes prior to the assessment period was provided to try on the HR monitor, ask questions about the device, and sit in the laboratory. Both groups of participants were given a rationale for measuring HR appropriate to their developmental level (e.g., “We are interested in seeing how fast your heart beats when you are doing activities”). To accommodate for difficulties with changes in daily routines, par- ticipants with autism had visits to the laboratory included on their weekly classroom schedules. Finally, all participants chose from a reward menu (food, game, or activity) at the end of their preobservation visits to increase future participation. Design. The observational design for each participant consisted of 14 phases (see Table 2). Each session began with a 5-minute baseline phase (sitting quietly with a familiar person). After the baseline phase the participants engaged in six potentially stressful situations (see Stress Phases). These potentially stressful situations alternated with 2-minute rest phases (sitting quietly with a familiar person). A physical exertion task (riding a stationary bicycle for 2 minutes) was included to ensure that participants could demonstrate an increase in HR significantly greater than baseline. The order of presentation of the stress phases was intentionally not counterbalanced to permit direct comparisons both between and within the typically developing and autism groups. Stress Phases. A wide sample of potential stressors was selected to enable adequate opportunities for the participants to elicit a cardiovascular stress response. The following stress phases and accompanying stress dimensions identified in the SSS (Groden et al., 2001) were included in the study because they (a) included events that naturally occur in the environ- TABLE 2 Observational Design and Stress Task Descriptions Phase Task Task length Task description 1 Baseline 5 min With a familiar person, seated in a comfortable chair 2 Loud noise 2 min With a familiar person, seated in a comfortable chair while a vacuum cleaner runs outside the room 3 Rest 2 min With a familiar person, seated in a comfortable chair 4 Remote robot 2 min With a familiar person, seated in a comfortable chair while a remote control robot navigates around the room 5 Rest 2 min With a familiar person, seated in a comfortable chair 6 Unstructured time 2 min Sitting in the room alone, given no other instructions than “We will be back in 2 minutes” 7 Rest 2 min With a familiar person, seated in a comfortable chair 8 Eating preferred food 2 min With a familiar person, given preferred food to eat 9 Rest 2 min With a familiar person, seated in a comfortable chair 10 Difficult task 2 min With a familiar person, seated in a comfortable chair and asked to mimic how the familiar person folds a towel 11 Rest 2 min With a familiar person, seated in a comfortable chair 12 Change in staff 2 min Familiar person leaves and person unfamiliar to the participant sits in the room 13 Rest 2 min With a familiar person, seated in a comfortable chair 14 Physical exertion 2 min With a familiar person, riding a stationary bicycle Transition Time between tasks Stress survey domain Sensory/personal contact Anticipation/uncertainty Anticipation/uncertainty Pleasant event Changes/threats Unpleasant event VOLUME 21, NUMBER 2, SUMMER 2006 105 ment; (b) could be replicated in an experimental setting; (c) consist of physical, social, and cognitive stimuli that overlap considerably with the problems of socialization, communication, and behavioral rigidity characteristic of persons with autism; and (d) were shown to elicit increased heart activity in the two feasibility studies (Goodwin et al., 2004; Groden et al., 2005). The stress phases included were as follows: 1. Loud noise (sensory/personal contact): with a familiar person, seated in a comfortable chair while a vacuum cleaner runs outside the room. 2. Remote robot (anticipation/uncertainty): with a familiar person, seated in a comfortable chair while a remotecontrol robot navigates around the room. 3. Unstructured time (anticipation /uncertainty): sitting in the room alone, given no other instructions than “We will be back in 2 minutes.” 4. Eating a preferred food (pleasant event): with a familiar person, seated in a comfortable chair and given preferred food to eat. 5. Difficult task (changes/threats): with a familiar person, seated in a comfortable chair and asked to fold a towel the same way the familiar person folds it. The familiar person is instructed prior to the session to fold the towel at a pace difficult for the participant to imitate. When the participant folds the towel incorrectly, the familiar person says, “Try it this way.” 6. Change in staff (unpleasant event): seated in a comfortable chair, familiar person leaves the room and a person unfamiliar to the participant sits in the room. 7. Transition: an artifact of the study design consisting of time between stressors and rest phases when the participant waited for the investigator to set up and begin the subsequent phase. Analysis The data analyses consisted of 10 separate univariate time series analyses (Crosbie, 1993; Glass, Willson, & Gottman, 1975; Velicer & Colby, 1997; Velicer & Fava, 2003) performed on each participant for the dependent variable HR. Time series analysis (TSA) requires repeated measurement at equally spaced intervals over a large number of observations and as such is a powerful longitudinal method for modeling change over time. In TSA, sample size reflects the number of observations over time rather than the number of subjects. The telemetric HR monitor provided beat-to-beat HR values generating approximately 3,500 data points per participant. TSA was used to analyze these data given that repeated measurements over time on a single subject creates serial dependency that violates the statistical assumption that errors in the data are independent across observations. TSA can calculate an autocorrelation between adjacent observations and thus transform serially dependent data to be independent. Once the data has been transformed to be independent, TSA can em- ploy traditional tests of statistical significance using the general linear model. Three waves of analyses were conducted for each participant using SAS Proc ARIMA (SAS Institute, 1988). The first wave involved a graphical display of the data. The second wave involved a model identification procedure to determine the best-fitting ARIMA (p, d, q) model. For all 10 participants, the general transformation approach of Velicer and McDonald (1991) was used. This approach is the equivalent to assuming a higher order (5+) autoregressive model and has been shown to perform accurately in previous simulation studies (Harrop & Velicer, 1985, 1990; Velicer & Colby, 2005). The third analysis wave employed a within-subject, interrupted TSA to determine whether mean HR during each potential stressor phase was significantly different from mean HR during baseline. The data points used to calculate baseline were the last 3 minutes of the first 5 minutes of observation for each participant. The first 2 minutes of the baseline phase were excluded a priori from the analysis for each participant to allow habituation to the telemetric apparatus and laboratory setting. Results Movement Data Table 3 lists the mean motor movement results for the participants with autism and the typically developing group. The motion component ranges from 0 for no movement to 50 for running very fast. With the exception of the physical exertion task, where motor movements were expected to increase, there was very little movement detected across phases for either group. In addition, for each participant motor movement was included in the time series analysis as a time-varying covariate to account for any explained variance in the HR data. The findings suggest that the subsequent reported HR results are virtually free from detected movement artifacts. Heart Rate Data Within Individual Differences: Autism Group. M.L. (see Appendix A) showed statistically significant HR increases from baseline (M = 106, SD = 7) to eating a preferred food (M = 112, SD = 8), t(629) = 2.65, p < .01; difficult task (M = 110, SD = 10), t(629) = 2.14 p < .05; and physical exertion (M = 122, SD = 11), t(629) = 6.58, p < .0001. J.L. (see Appendix B) showed statistically significant HR increases from baseline (M = 84, SD = 7) to remote robot (M = 92, SD = 19), t(540) = 2.40, p < .05; unstructured time (M = 95, SD = 1), t(540) = 2.11, p < .05; and physical exertion (M = 93, SD = 15), t(540) = 2.32, p < .05. S.E. (see Appendix C) only showed statistically significant HR changes from baseline (M = 113, SD = 3) to physical exertion (M = 125, SD = 10), t(700) = 2.22, p < .05. M.C. (see Appendix D) only showed statistically significant HR changes from baseline (M = 87, FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 106 TABLE 3 Mean Movement Results for Autism and Typically Developing Participants Baseline Loud noise Remote robot Unstructured time Eating food Difficult task Change in staff Transition Physical exertion 0.41 0.19 0.12 0.29 0.41 0.33 0.13 0.19 0.61 0.25 0.30 0.34 0.41 0.14 1.48 0.33 0.54 0.38 0.28 0.21 2.14 0.40 0.68 0.34 0.42 0.27 0.50 0.38 0.38 0.77 0.86 0.72 0.59 0.56 0.70 0.90 0.55 0.25 0.65 0.35 0.54 0.72 0.53 0.35 0.64 0.74 0.60 1.45 1.44 1.09 1.49 1.13 1.32 1.09 0.14 0.09 0.10 0.12 0.27 0.34 0.23 0.05 0.19 0.22 0.12 0.48 0.22 0.03 0.14 0.20 0.46 0.39 0.21 0.18 0.21 0.29 0.27 0.38 0.18 0.23 0.27 0.27 1.24 0.71 0.89 0.84 0.72 0.88 0.22 0.41 0.22 0.04 0.25 0.23 0.63 0.80 0.20 0.23 0.35 0.44 2.22 2.60 0.94 1.17 1.09 1.60 M SD Autism M.L. J.L. S.E. M.C. A.F. Group 0.41 0.19 0.31 0.23 0.46 0.32 Typically developing B.A. C.N. D.P. D.V. S.M. Group 0.55 0.21 0.26 0.28 0.31 0.32 Participant Note. Motion component ranges from 0 for no movement to 50 for running very fast. SD = 5) to physical exertion (M = 110, SD = 10), t(563) = 10.37, p < .0001. A.F. (see Appendix E) showed statistically significant HR changes from baseline (M = 90, SD = 8) to eating a preferred food (M = 103, SD = 11), t(601) = 5.63, p < .0001; difficult task (M = 106, SD = 13), t(601) = 6.17, p < .0001; change in staff (M = 97, SD = 13), t(601) = 3.22, p < .001; transition (M = 101, SD = 12), t(601) = 5.18, p < .0001; and physical exertion (M = 108, SD = 12), t(601) = 7.35, p < .0001. Within Individual Differences: Typically Developing Group. B.A. (see Appendix F) showed statistically significant HR changes from baseline (M = 98, SD = 10) to remote robot (M = 110, SD = 9), t(673) = 2.81, p < .01; unstructured time (M = 119, SD = 7), t(673) = 4.13, p < .0001; eating a preferred food (M = 116, SD = 3), t(673) = 4.44, p < .0001; difficult task (M = 114, SD = 5), t(673) = 3.18, p < .01; change in staff (M = 105, SD = 5), t(673) = 4.62, p < .0001; transition (M = 112, SD = 13), t(673) = 4.88, p < .0001; and physical exertion (M = 141, SD = 9), t(673) = 5.28, p < .0001. C.N. (see Appendix G) showed statistically significant HR changes from baseline (M = 89, SD = 6) to transition (M = 93, SD = 9), t(571) = 2.18, p < .05, and physical exertion (M = 105, SD = 18), t(571) = 5.37, p < .0001. D.P. (see Appendix H) showed statistically significant HR changes from baseline (M = 57, SD = 5) to unstructured time (M = 60, SD = 6), t(478) = 1.99, p < .05; eating a preferred food (M = 68, SD = 5), t(478) = 4.57, p < .0001; difficult task (M = 70, SD = 7), t(478) = 5.42, p < .0001; change in staff (M = 62, SD = 7), t(478) = 2.64, p < .001; transition (M = 65, SD = 8), t(478) = 4.44, p < .0001; and physical exertion (M = 73, SD = 9), t(478) = 5.52, p < .0001. D.V. (see Appendix I) showed statistically significant HR changes from baseline (M = 74, SD = 6) to eating a preferred food (M = 90, SD = 5), t(484) = 5.32, p < .0001; difficult task (M = 89, SD = 5), t(484) = 3.62, p < .0001; transition (M = 81, SD = 8), t(484) = 3.66, p < .0001; and physical exertion (M = 94, SD = 7), t(484) = 6.87, p < .0001. S.M. (see Appendix J) showed statistically significant HR changes from baseline (M = 50, SD = 5) to unstructured time (M = 58, SD = 8), t(497) = 3.12, p < .01; eating a preferred food (M = 67, SD = 7), t(497) = 3.68, p < .001; difficult task (M = 64, SD = 8), t(497) = 3.20, p < .01; change in staff (M = 56, SD = 7), t(497) = 2.06, p < .05; transition (M = 62, SD = 13), t(497) = 3.63, p < .001; and physical exertion (M = 78, SD = 11), t(497) = 6.25, p < .0001. Within-Group Differences: Autism Group. Two of the participants (S.E., M.C.) showed no significant HR changes to any of the potentially stressful situations. Two other participants (M.L., J.L.) showed significant HR changes to only two of the stressors. The remaining participant (A.F.) showed significant HR changes to four of the stressors. In all participants, the physical exertion phase elicited significant mean HR responses greater than baseline. Within-Group Differences: Typically Developing Group. One participant (C.N.) showed significant HR changes to only one stressor. One participant (D.V.) showed significant HR changes to three stressors. One participant (S.M.) showed significant HR changes to five of the stressors. Two participants (B.A., D.P.) showed significant HR changes to six of the stressors. Again, in all participants, the physical exertion phase elicited significant mean HR responses greater than baseline. VOLUME 21, NUMBER 2, SUMMER 2006 107 Between-Group Differences. Figures 1 and 2 illustrate for each phase the mean HR results for each participant with autism and each typically developing participant, respectively. The mean HR for baseline in the autism group ranged from 84 bpm to 113 bpm with an overall group mean of 96 bpm (SD = 12). The mean HR for baseline in the typically developing group ranged from 50 bpm to 98 bpm with an overall group mean of 74 bpm (SD = 20). The mean HR for loud noise in the autism group ranged from 87 bpm to 113 bpm with an overall group mean of 97 bpm (SD = 11). The mean HR for loud noise in the typically developing group ranged from 52 bpm to 94 bpm with an overall group mean of 75 bpm (SD = 18). The mean HR for remote robot in the autism group ranged from 86 bpm to 112 bpm with an overall group mean of 96 bpm (SD = 11). The mean HR for remote robot in the typically developing group ranged from 49 bpm to 110 bpm with an overall group mean of 75 bpm (SD = 26). The mean HR for unstructured time in the autism group ranged from 90 bpm to 113 bpm with an overall group mean of 100 bpm (SD = 10). The mean HR for unstructured time in the typically developing group ranged from 58 bpm to 119 bpm with an overall group mean of 80 bpm (SD = 25). The mean HR for eating a preferred food in the autism group ranged from 85 bpm to 113 bpm with an overall group mean of 100 bpm (SD = 13). The mean HR for eating a preferred food in the typically developing group ranged from 67 bpm to 116 bpm with an overall group mean of 87 bpm (SD = 20). The mean HR for difficult task in the autism group ranged from 87 bpm to 115 bpm with an overall group mean of 101 bpm (SD = 13). The mean HR for difficult task in the typically developing group ranged from 64 bpm to 114 bpm with an overall group mean of 85 bpm (SD = 19). The mean HR for change in staff in the autism group ranged from 85 bpm to 102 bpm with an overall group mean of 97 bpm (SD = 11). The mean HR for change in staff in the typically developing group ranged from 56 bpm to 105 bpm with an overall group mean of 78 bpm (SD = 20). The mean HR for transition in the autism group ranged from 87 bpm to 115 bpm with an overall group mean of 100 bpm (SD = 12). The mean HR for transition in the typically developing group ranged from 62 bpm to 112 bpm with an overall group mean of 83 bpm (SD = 21). The mean HR for physical exertion in the autism group ranged from 92 bpm to 125 bpm with an overall group mean of 112 bpm (SD = 14). The mean HR for physical exertion in the typically developing group ranged from 73 bpm to 141 bpm with an overall group mean of 98 bpm (SD = 27). Discussion The present study compared the cardiac responses of five relatively low-functioning persons with autism to five age- and sex-matched typically developing individuals under repeated conditions of environmental stressors. Based on arousal mod- M.L. J.L. S.E. M.C. A.F. Baseline Loud noise Remote Unstructured Eating Difficult task Change in Transition preferred staff time robot foods PHASE FIGURE 1. Mean heart rate level by phase for autism group. Physical exertion FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 108 B.A. C.N. D.P. D.V. S.M. Baseline Loud noise Remote Unstructured Eating Difficult task Change in Transition preferred staff time robot foods Physical exertion FIGURE 2. Mean heart rate level by phase for typical group. ulation theories of autism (Dawson, 1991; Dawson & Lewy, 1989; Kinsbourne, 1987; Ornitz, 1989; Ornitz & Ritvo, 1968), reports of stressful events being associated with behavioral challenges (Groden et al., 1994; Howlin, 1998; Hutt & Hutt, 1968; Prior & Ozonoff, 1998), and documented comorbid anxiety disorders in persons with autism (Bellini, 2004; Gillot et al., 2001; Green et al., 2000; Kim et al., 2000; Muris et al., 1998), it was hypothesized that the group with autism would show significant cardiovascular responses to a greater number of stressors than the typically developing control group. However, the findings revealed just the opposite: Out of the 35 opportunities for each group to show a significant mean HR response to a stressor (i.e., seven potentially stressful phases × five participants), the group with autism showed significant responses only 22% of the time (8 out of 35), compared to the typically developing group, which showed significant responses 60% of the time (21 out of 35). At first glance, these results suggest that the group of individuals with autism is less aroused by environmental stressors than the typically developing control group. However, the diminished cardiovascular reactivity to potential stressors in the group with autism may be related to their high basal HR and reduced variance in responsivity (see Figure 3). On average, the participants with autism showed mean HR responses approximately 20 bpm higher during baseline and nearly every potentially stressful situation. The group with autism also showed approximately half the amount of variance in HR responsivity compared to the typically developing group. These data appear to replicate the previous findings of Cohen and colleagues (Cohen & Johnson, 1977; Kootz & Cohen, 1981; Kootz, Marinelli, & Cohen, 1982) and suggest that persons with autism who have high basal HR are unable to elicit significantly greater increases in cardiovascular reactivity to environmental stimulation. The diminished cardiovascular reactivity to environmental stressors suggests that the group with autism was either overly aroused by the testing situation on the whole (which included the same characteristics and staff that may be stressful on a daily basis) or in a general state of autonomic defensiveness. If the hypothesis is tenable that some individuals with autism are in a general state of high autonomic arousal, then it is of interest to identify the underlying mechanisms contributing to such responsivity. Although no one theory has gained overwhelming support, several putative mechanisms have been suggested. Ornitz (1989) speculated that dysfunctions in the neuronal networks in the brainstem, including the diencephalon, can cause disordered sensory processing that result in problems of arousal modulation. Hutt and Hutt (1970) hypothesized dysfunctions in sympathetic inhibitory control mediated by the limbic system. Others have postulated dysfunctions in the central control of HR modulation (Graveling & Brooke, 1978; Hutt, Forrest, & Richer, 1975; MacCulloch VOLUME 21, NUMBER 2, SUMMER 2006 109 Autism Typical Baseline Loud noise Remote Unstructured Eating Difficult task Change in Transition Physical preferred staff time exertion robot foods FIGURE 3. Average mean heart rate level by phase for autism and typical groups. & Williams, 1971), including the vagus nerve (Althaus, Mulder, Mulder, Aarnoudse, & Minderaa, 1999). More recently, the amygdala, which plays a central role in moderating fear and anxiety (Davis & Whalen, 2001), is thought to be abnormal in autism (Baron-Cohen et al., 2000; Schultz, Romanski, & Tsatsanis, 2000; Sweeten, Posey, Shekhar, & McDougle, 2002), contributing to improper arousal regulation in this population (Amaral, Bauman, & Mills Schumann, 2003). Although biological preconditions leading to and behavioral observations indicative of overarousal are implicated in autism, one must still reconcile the fact that physiological overarousal does not always replicate in this population. Some tentative reasons for this discrepancy have been offered by Zahn (1986) in an early review of ANS arousal findings in autism: (a) that most individuals with autism have chronically high levels of autonomic activity, but that a subgroup within the disorder may respond at normal levels; (b) that persons with autism may exhibit heightened ANS activity only some of the time; and (c) that physiological studies requiring interaction with people or that create confusion about what the participant is being asked to do can cause study participants to exhibit high arousal. Clearly, all of these potential conditions can vary depending on the experimental research design used, the procedure for gaining compliance, and the sample studied. Dawson and Lewy (1989) have also suggested that levels of stimulation can vary across individuals with autism as a function of developmental level, degree of familiarity with the test- ing situation, and biologically based individual differences, including severity of the disorder. In light of these cautions, there are methodological strengths and weaknesses associated with the present study’s findings. First, several steps were taken to control for arousal induced by the testing environment: (a) The preobservation protocol enabled the participants with autism to sample the laboratory setting and heart monitor repeatedly prior to the observation; (b) a relatively noninvasive, wireless HR monitor that can be worn underneath a garment was used; (c) observations were undertaken in a minimally stimulating (e.g., incandescent lighting, pattern-free walls and carpet), soundproof laboratory; and (d) a familiar person accompanied the participants throughout the observational sessions. Second, several steps were taken to control for arousal artifacts unrelated to the independent variables: (a) With the exception of riding the stationary bicycle, participants were seated in a comfortable chair for the duration of the observation to minimize HR increases associated with physical activity; (b) the HR monitor recorded postural changes and motor movements and inclusion of this data as a covariate in the statistical analyses controlled for HR increases due to recorded physical activity; and (c) participants in this study had normal blood pressure measurements and were free of medications, ruling out the possibility that their arousal responses were affected by abnormal cardiovascular systems or pharmacological agents. Finally, a wide sample of potential stressors was used to provide mul- FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 110 tiple opportunities for participants to elicit a stress response. Sampling just one potentially stressful situation may or may not have elicited significant physiological reactions across all participants, enabling potentially erroneous conclusions about arousal responses in this sample. While these experimental controls attempt to minimize extraneous variables that can affect measurement of arousal responses in persons with autism, there are a few potential confounds and limitations associated with the current study that merit future research. For example, there were instances across both the autism and control groups where significant cardiovascular reactivity occurred during rest phases. A review of the data suggests that these responses might be related to (a) a carry-over effect from a previous stress condition, (b) cumulative arousal mediated by a participant’s relevant cognitions or emotions, or (c) participant reactivity to being observed in an artificial setting. In the present study, a carry-over effect seems evident in the autism group for M.L., who showed significant HR responses during rest only after a significant response to a preceding stressor. While representing a potential threat to the internal validity of the experimental stressors, this carry-over effect suggests that arousal associated with a stressor can extend over time even when the stressful stimuli or situation is removed. This phenomenon, if replicated in future studies, may be of clinical interest as it demonstrates that some individuals with autism cannot self-regulate their arousal response to a stressor in a timely manner. Cumulative stress responses evidenced by increased cardiovascular reactivity in every previous and subsequent condition, typically toward the end of the observation, occurred for A.F. in the autism group and B.A., D.P., D.V., and S.M. in the control group. This pattern of responding may be related to unobservable thoughts or feelings (e.g., memory of a previous stimulating occasion, boredom, anticipation) that are themselves arousal producing. Although only speculative, this hypothesis has some face validity given that this pattern of responding occurred primarily in the more cognitively able, typically developing group. It is also possible that these arousal responses are not related to the environmental stressors per se, but to the simple act of being monitored in a laboratory setting. For instance, three participants with autism (M.L., S.E., A.F.) and one typically developing individual (B.A.) had basal HR, prior to any presentation of an experimental stressor, equal to or greater than 90 bpm. A nurse on staff at the Groden Center reviewed the medical records of all the participants to verify that no one had documented problems with cardiovascular functioning before entry into the study. Therefore, it is unclear whether these basal rates are accurate estimates of resting HR or whether they are artificially high in response to being observed in an artificial setting. Future studies that deploy wireless HR monitors in the natural environment might gather data from individuals with autism and indicate whether the high basal HR and stress response patterns observed in the current study are attributable to characteristics of the partici- pants or environmental stressors, or simply to the act of being observed in a simulated environment. The individual differences found within the autism and typically developing groups also demonstrate the advantages and complexity inherent in interpreting single-subject data. Nomothetic approaches that classify large, random groups of people based on an average response statistic to find interindividual variation prevail in psychology. However, this approach often yields superficial understanding of any one person because limited data are typically collected. In contrast, idiographic methods (see Molenaar, 2004) that gather singlesubject data, such as those used in the present study, investigate a small sample of individuals in detail and focus on a person’s uniqueness. Quantitative analysis of idiographic data highlights intraindividual variation over time to gain a thorough and more subtle understanding of a few people to lead to more general understanding of others. In this framework, systematic replication (Barlow & Hersen, 1984) becomes the basis for generalizability. Because the current study only included five individuals with autism, it is questionable whether the observed HR results and accompanying interpretation of the data would generalize to a large sample. Therefore, larger sample sizes are needed in future studies to assure more accurate representation of response types in a notoriously heterogeneous population. Continuing research might also recruit participants who have a greater range of functioning abilities and might employ standardized, adaptive behavioral measures that better identify individual differences by differentiating between high- and low-functioning individuals with autism, a variable that Kootz and colleagues (1982) and Dawson and Lewy (1989) suggest can mediate arousal responses. Future studies might also make attempts to record and correlate overt behavioral responding with underlying physiological functioning to determine if there is synchrony or dysynchrony across levels of measurement. Despite the general finding of high HR in the participants with autism, anecdotal observation of overt behavior in this study indicated only minor signs of arousal. This is a potentially interesting happening that deserves more systematic study given that communication deficits characteristic of this population require educators to make inferences about internal states from overt behavioral responses. It may well be that some individuals with autism look relatively calm overtly, but are experiencing significant physiological arousal covertly. Finally, while HR is a robust measure of general physiological arousal, it is influenced by both sympathetic and parasympathetic nervous system activities. Heart rate variability, on the other hand, allows more fine-grained analyses of stress on cardiovascular arousal, including the assessment of vasovagal tone. Physiological research supports the notion that HR patterns are predominantly mediated via the vagus nerve (Levy, 1984). Measures of vagal reactivity to sensory, visceral, or cognitive challenges indicate the adaptive functioning of the nervous system. Therefore, measures of cardiac vagal tone can provide an important window into the central control of au- VOLUME 21, NUMBER 2, SUMMER 2006 111 tonomic processes and by inference the central processes necessary for organized behavior. Future studies that employ such data may determine if restricted autonomic flexibility (Porges, 1985) contributes to the cardiovascular overarousal found in this study. In sum, this study further explores the role that stress, stress-related anxiety, and physiological arousal play in the behavior of individuals with autism. Continuing research that focuses on these constructs and addresses the methodological considerations raised when using HR as a direct measure of stress will be required to determine if qualitative differences in arousal prevent this population from attending to, processing, and interacting with their environment and learning normative behaviors and skills from other people. However, if replicated, the findings from this study have important assessment and treatment implications for psychologists, educators, family members, and individuals with autism. For instance, heightened arousal might constrain the ability of persons with autism to benefit from behavioral and social interventions that fail to address this physiologic reactivity. If an individual with autism is identified as being overaroused, stress reduction techniques such as relaxation training (Cautela & Groden, 1978) and cognitive picture rehearsal (Groden, LeVasseur, Diller, & Cautela, 2002) might be used as preparatory steps to any further behavioral or academic instruction. This study also highlights the promise of developing noninvasive, wireless technologies that persons with autism can wear to monitor physiological stress in real time, thus facilitating more effective ways for these individuals to communicate their arousal states and for educators and family members to respond appropriately. ABOUT THE AUTHORS Matthew S. Goodwin, MA, is the research coordinator at the Groden Center, a day and residential treatment and education program serving children and youth who have developmental and behavioral difficulties. He is also a PhD candidate in behavioral science at the University of Rhode Island. His research and clinical experience with children with autism spectrum disorders focuses primarily on the assessment of behavioral and physiological responses using telemetric monitors and digital video/editing systems. June Groden, PhD, is the director of the Groden Center and is on appointment at Brown University and the University of Rhode Island. Wayne F. Velicer is the co-director of the Cancer Prevention Research Center and professor of psychology at the University of Rhode Island. In behavioral statistics, his work has focused on factor analysis and component analysis, the application of time series analysis to the behavioral sciences, and methods for measurement development. Lewis P. Lipsitt, PhD, is professor emeritus of psychology, medical science, and human development at Brown University. His career-long interests have been in child behavior and development, sensory and learning processes of infants, risk-taking behavior in children and adolescents, and crib death (SIDS). M. Grace Baron is professor of psychology at Wheaton College in Norton, Massachusetts, and a consulting behavioral psychologist at the Groden Center. She is also a member of the Groden Center Research Team, studying biobehavioral aspects of stress in autism. Stefan G. Hofmann, PhD, is an associate professor of psychology at Boston University and editor of Cognitive and Behav- ioral Practice. His current interests include the psychophysiology and treatment of emotion and anxiety disorders. Gerald Groden, PhD, is the cofounder of the Groden Center and is currently on appointment at Brown University and the University of Rhode Island. Address: Matthew S. Goodwin, The Groden Center, Inc., 86 Mt. Hope Ave., Providence, RI 02906; e-mail: msgoodwin@earthlink.net NOTES 1. Small amounts of food were used so that the entire portion of food could be consumed in the time provided. 2. In the analyses, HR data was reduced to 5-second averages to facilitate graphical representation and statistical testing. REFERENCES Althaus, M., Mulder, L. J. M., Mulder, G., Aarnoudse, C. C., & Minderaa, R. B. (1999). Cardiac adaptivity to attention-demanding tasks in children with a pervasive developmental disorder not otherwise specified (PDD-NOS). Biological Psychiatry, 46, 799–809. Amaral, D. G., Bauman, M. D., & Mills Schumann, C. (2003). The amygdala and autism: Implications from non-human primate studies. Genes Brain & Behavior, 2, 295–302. American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., Rev.). Washington, DC: Author. American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author. Angus, Z. (1970). Autonomic and cognitive functions in childhood psychosis. Bulletin of the British Psychological Society, 23, 228–229. Baranek, G. T. (2002). Efficacy of sensory and motor interventions for children with autism. Journal of Autism and Developmental Disorders, 32, 397–422. Barlow, D. H., & Hersen, M. (1984). Single case experimental designs: Strategies for studying behavior change (2nd ed.). New York: Pergamon Press. Baron-Cohen, S., Ring, H. A., Bullmore, E. T., Wheelwright, S., Ashwin, C., & Williams, S. C. R. (2000). The amygdala theory of autism. Neuroscience and Biobehavioral Reviews, 24, 355–364. Bayley, N. (1993). Bayley scales of infant development (2nd ed.). San Antonio, TX: Psychological Corp. Bellini, S. (2004). Social skill deficits and anxiety in high-functioning adolescents with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 19, 78–86. Cautela, J., & Groden, J. (1978). Relaxation: A comprehensive manual for adults, children and children with special needs. Champaign, IL: Research Press. Cohen, D. J., & Johnson, W. T. (1977). Cardiovascular correlates of attention in autistic children: Response times to proximal and distal stimulation. Archives of General Psychiatry, 34, 561–567. Crosbie, J. (1993). Interrupted time series analysis with brief singlesubject data. Journal of Consulting and Clinical Psychology, 61, 966–974. Davis, M., & Whalen, P. J. (2001). The amygdala: Vigilance and emotion. Molecular Psychiatry, 6, 13–34. Dawson, G. (1991). A psychobiological perspective on the early socio-emotional development of children with autism. In D. Cic- FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 112 chetti & S. L. Toth (Eds.), Rochester Symposium on Developmental Psychopathology: Vol. 3. Models and integrations (pp. 207–234). Rochester, NY: University of Rochester Press. Dawson, G., & Lewy, A. (1989). Arousal, attention, and the socioemotional impairments of individuals with autism. In G. Dawson (Ed.), Autism: Nature, diagnosis, and treatment (pp. 49–74). New York: Guilford Press. DesLauriers, A. M., & Carlson, C. F. (1969). Your child is asleep: Early infantile autism. Homewood, IL: Dorsey Press. Evans, D. W., Canavera, K., Kleinpeter, F. L., Maccubbin, E., & Taga, K. (2005). The fears, phobias and anxieties of children with autism spectrum disorders and Down syndrome: Comparisons with developmentally and chronologically age matched children. Child Psychiatry and Human Development, 36, 3–26. Fox, S. (1996). Human physiology (5th ed). Dubuque, IA: W. C. Brown. Gillot, A., Furniss, F., & Walter, A. (2001). Anxiety in highfunctioning children with autism. Autism, 5, 277–286. Glass, G. V., Willson, V. L., & Gottman, J. M. (1975). Design and analysis of time series experiments. Boulder: Colorado Associate University Press. Goodwin, M. S., & Groden, J., Baron, G., Groden, G., Velicer, W. F., Lipsitt, L. P., Hofmann, S., & Hoppner, B. B. (2004, May). Cardiovascular responses to stress in individuals with autism. Poster session presented at the annual meeting of the American Psychological Society, Chicago. Graveling, R. A., & Brooke, J. D. (1978). Hormonal and cardiac response of autistic children to changes in environmental stimulation. Journal of Autism and Childhood Schizophrenia, 8, 441–455. Green, J., Gilchrist, A., Burton, D., & Cox, A. (2000). Social and psychiatric functioning in adolescents with Asperger syndrome compared with conduct disorder. Journal of Autism and Developmental Disorders, 30, 279–293. Groden, J., Cautela, J., Prince, S., & Berryman, J. (1994). The impact of stress and anxiety on individuals with autism and developmental disabilities. In E. Schopler & G. Mesibov (Eds.), Behavioral issues in autism (pp. 178–190). New York: Plenum Press. Groden, J., Diller, A., Bausman, M., Velicer, W., Norman, G., & Cautela, J. (2001). The development of a stress survey schedule for persons with autism and other developmental disabilities. Journal of Autism and Developmental Disorders, 31, 207–217. Groden, J., Goodwin, M. S., Baron, G., Groden, G., Velicer, W. F., Lipsitt, L. P., et al. (2005). Assessing cardiovascular responses to stressors in individuals with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 20, 244–252. Groden, J., LeVasseur, P., Diller, A., & Cautela, J. (2002). Coping with stress through picture rehearsal: A how-to manual for working with individuals with autism and developmental disabilities. Providence, RI: The Groden Center. Harrop, J. W., & Velicer, W. F. (1985). A comparison of three alternative methods of time series model identification. Multivariate Behavioral Research, 20, 27–44. Harrop, J. W., & Velicer, W. F. (1990). Computer programs for interrupted time series analysis: A quantitative evaluation. Multivariate Behavioral Research, 25, 233–248. Hill, E., Berthoz, S., & Frith, U. (2004). Brief report: Cognitive processing of own emotions in individuals with autistic spectrum disorder and in their relatives. Journal of Autism and Developmental Disorders, 34, 229–235. Howlin, P. (1998). Children with autism and Asperger syndrome: A guide for practitioners and careers. Chichester: Wiley. Hutt, C., Forrest, S., & Richer, J. (1975). Cardiac arrhythmia and behaviour in autistic children. Acta Psychiatrica Scandinavica, 51, 361–372. Hutt, C., & Hutt, S. J. (1970). Stereotypies and their relation to arousal: A study of autistic children. In S. J. Hutt & C. Hutt (Eds.), Behaviour studies in psychiatry (pp. 175–204). Oxford: Pergamon Press. Hutt, S. J., & Hutt, C. (1968). Stereotypy, arousal and autism. Human Development, 11, 277–286. Hutt, S. J., Hutt, C., Lee, D., & Ounsted, C. (1964). Arousal and childhood autism. Nature, 204, 908–909. Kim, J. A., Szatmari, P., Bryson, S. E., Streiner, D. L., & Wilson, F. J. (2000). The prevalence of anxiety and mood problems among children with autism and Asperger syndrome. Autism, 4, 117–132. Kinsbourne, M. (1987). Cerebral brainstem relations in infantile autism. In E. Schopler & G. B. Mesibov (Eds.), Neurobiological issues in autism (pp. 107–125). New York: Plenum Press. Knapp, L. G., Barrett, R. P., Groden, G., & Groden, J. (1992). The nature and prevalence of fears in developmentally disabled children and adolescents: A preliminary investigation. Journal of Developmental and Physical Disabilities, 4, 195–203. Kootz, J. P., & Cohen, D. J. (1981). Modulation of sensory intake in autistic children: Cardiovascular and behavioral indices. Journal of the American Academy of Child Psychiatry, 20, 692–701. Kootz, J. P., Marinelli, B., & Cohen, D. J. (1982). Sensory receptor sensitivity in autistic children: Response times to proximal and distal stimulation. Archives of General Psychiatry, 38, 271–273. Lacey, J. I. (1967). Somatic response patterning and stress: Some revisions of activation theory. In M. H. Appley & R. Trumball (Eds.), Psychological stress: Issues in research (pp. 14–42) New York: Appleton-Century-Crofts. Lake, C. R., Ziegler, M. G., & Murphy, D. L. (1977). Increased norepinephrine levels and decreased dopamine-*b-hydroxylase activity in primary autism. Archives of General Psychiatry, 34, 553–556. Lazarus, R. S., & Folkman, S. (1984) Stress, appraisal, and coping. New York: Springer. Levy, M. N. (1984). Cardiac sympathetic-parasympathetic interactions. Federation Proceedings, 43, 2598–2602. Lord, C., & McGee, J. P. (2001). Educating children with autism. Washington, DC: National Academy Press. Lord, C., & Paul, R. (1997). Language and communication in autism. In D. Cohen & F. Volkmar (Eds.), Handbook of autism and pervasive developmental disorders (pp. 195–225). New York: Wiley. MacCulloch, M. J., & Williams, C. (1971). On the nature of infantile autism. Acta Psychiactrica Scandinavica, 47, 295–314. Matson, J. L., & Love, S. R. (1990). A comparison of parentreported fear for autistic and nonhandicapped age-matched children and youth. Australia & New Zealand Journal of Developmental Disabilities, 16, 349–357. Ming, X., Julu, P. O. O., Brimacombe, M., Connor, S., & Daniels, M. L. (2005). Reduced cardiac parasympathetic activity in children with autism. Brain & Development, 27, 509–516. Molenaar, P. C. M. (2004). A manifesto on psychology as idiographic science: Bringing the person back into scientific psychology, this time forever. Measurement. Interdisciplinary Research and Perspectives, 2, 201–218. Mundy, P., & Stella, J. (2000). Joint attention, social orienting, and communication in autism. In A. M. Wetherby & B. M. Prizant VOLUME 21, NUMBER 2, SUMMER 2006 113 (Eds.), Autism spectrum disorders: A transactional developmental perspective (pp. 55–78). Baltimore: Brookes. Muris, P., Steerneman, P., Merckelbach, H., Holdrinet, I., & Meesters, C. (1998). Comorbid anxiety symptoms in children with pervasive developmental disorders. Journal of Anxiety Disorders, 12, 387–393. Ornitz, E. M. (1989). Autism at the interface between sensory and information processing. In G. Dawson (Ed.), Autism: nature, diagnosis, and treatment (pp. 174–297). New York: Guilford Press. Ornitz, E. M., & Ritvo, E. R. (1968). Perceptual inconstancy in early infantile autism. Archives of General Psychiatry, 18, 76–98. Palkovitz, R. J., & Wiesenfeld, A. R. (1980). Differential autonomic responses of autistic and normal children. Journal of Autism and Developmental Disorders, 10, 347–360. Porges, S. W. (1985). Respiratory sinus arrhythmia: An index of vagal tone. In J. F. Orlebeke, G. Mulder, & L. J. P. Van Dornen (Eds.), Psychophysiology of cardiovascular control: Models, methods, and data (pp. 437–450). New York: Plenum Press. Prior, M., & Ozonoff, S. (1998). Psychological factors in autism. In F. R. Volkmar (Ed.), Autism and pervasive developmental disorders (pp. 64–98). New York: Cambridge University Press. Prizant, B. M., Wetherby, A. M., Rubin, E., & Laurent, A. C. (2003). The SCERTS model: A transactional, family-centered approach to enhancing communication and socioemotional abilities of children with autism spectrum disorder. Infants and Young Children, 16, 296–316. Rogers, S. J., & Bennetto, L. (2000). Intersubjectivity in autism: The roles of imitation and executive function. In A. M. Wetherby & B. M. Prizant (Eds.), Autism spectrum disorders: A transactional developmental perspective (pp. 79–108). Baltimore: Brookes. Roid, G. M., & Miller, L. J. (1997). Leiter international performance scale-Revised: Examiners manual. Wooddale, IL: Stoelting. Sapolsky, R. (1998). Why zebras don’t get ulcers. New York: Freeman. SAS Institute. (1988). SAS/ETS user’s guide, Version 6. Cary, NC: Author. Schopler, E., Reichler, R. J., & Renner, B. R. (1986). The childhood autism rating scale. New York: Irvington. Schultz, R. T., Romanski, L. M., & Tsatsanis, K. D. (2000). Neurofunctional models of autistic disorder and Asperger syndrome: Clues from neuroimaging. In A. Klin, F. R. Volkmar, & S. S. Sparrow (Eds.), Asperger syndrome (pp. 172–209). New York: Guilford Press. Selye, H. (1956). The stress of life. New York: McGraw-Hill. Siegel, B. (2003). When atypical development and typical development cross paths. In B. Siegel (Ed.), Helping children with autism learn (pp. 40–76). New York: Oxford University Press. Sigman, M., Dissanayake, C., Corona, R., & Espinosa, M. (2003). Social and cardiac responses of young children with autism. Autism, 7, 205–216. Steingard, R. J., Zimnitzky, B., DeMaso, D. R., Bauman, M. L., & Bucci, J. P. (1997). Sertraline treatment of transition-associated anxiety and agitation in children with autistic disorder. Journal of Child and Adolescent Psychopharmacology, 7, 9–15. Stern, R. M., Ray, W. J., & Quigley, K. S. (2001). Some basic principles of psychophysiology. In R. M. Stern, W. J. Ray, & K. S. Quigley (Eds.), Psychophysiological recording (2nd ed., pp. 52–78). Oxford: Oxford University Press. Stevens, S., & Gruzelier, J. (1984). Electrodermal activity to auditory stimuli in autistic, retarded, and normal children. Journal of Autism and Developmental Disorders, 14, 245–260. Sweeten, T. L., Posey, D. J., Shekhar, A., & McDougle, C. J. (2002). The amygdala and related structures in the pathophysiology of autism. Pharmacology, Biochemistry, and Behavior, 71, 449–455. Toichi, M., & Kamio, Y. (2003). Paradoxical autonomic response to mental tasks in autism. Journal of Autism and Developmental Disorders, 33, 417–426. Thorndike, R. L., Hagen, E. P., & Sattler, J. M. (1986). The StanfordBinet intelligence scale (4th ed.). Chicago: Riverside. van Engeland, H. (1984). The electrodermal orienting response to auditive stimuli in autistic children, normal children, mentally retarded children, and child psychiatric patients. Journal of Autism and Developmental Disorders, 14, 261–278. Velicer, W. F., & Colby, S. M. (1997). Time series analysis for prevention and treatment research. In K. J. Bryant, M. Windle, & S. G. West (Eds.), The science of prevention: Methodological advances from alcohol and substance abuse research (pp. 211–249). Washington, DC: American Psychological Association. Velicer, W. F., & Colby, S. M. (2005). Missing data and the general transformation approach to time series analysis. In A. MaydeuOlivares & J. J. McArdle (Eds.), Contemporary psychometrics. A Festschrift to Roderick P. McDonald (pp. 509–535). Hillsdale, NJ: Erlbaum. Velicer, W. F., & Fava, J. (2003). Time series analysis. In J. A. Schinka & W. F. Velicer (Eds.), Handbook of psychology: Research methods in psychology (Vol. 2, pp. 581–606). New York: Wiley. Velicer, W. F., & McDonald, R. P. (1991). Cross-sectional time series designs: A general transformation approach. Multivariate Behavioral Research, 26, 247–254. Wilhelm, F. H., Roth, W. T., & Sackner, M. A. (2003). The Lifeshirt: An advanced system for ambulatory measurement of respiratory and cardiac function. Behavior Modification, 27, 671–691. World Health Organization. (1992). Tenth revision of the international classification of disease. Geneva: Author. Zahn, T. P. (1986). Psychophysiological approaches to psychopathology. In M. Coles, E. Donchin, & S. Porges (Eds.), Psychophysiology: Systems, processes, and applications (pp. 508–610). New York: Guilford Press. Zahn, T. P., Rumsey, J. M., & van Kammen, D. P. (1987). Autonomic nervous system activity in autistic, schizophrenic, and normal men: Effects of stimulus significance. Journal of Abnormal Psychology, 2, 135–144. FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 114 APPENDIX A Mean Heart Rate Level by Phase for M.L. VOLUME 21, NUMBER 2, SUMMER 2006 115 APPENDIX B Mean Heart Rate Level by Phase for J.L. FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 116 APPENDIX C Mean Heart Rate Level by Phase for S.E. VOLUME 21, NUMBER 2, SUMMER 2006 117 APPENDIX D Mean Heart Rate Level by Phase for M.C. FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 118 APPENDIX E Mean Heart Rate Level by Phase for A.F. VOLUME 21, NUMBER 2, SUMMER 2006 119 APPENDIX F Mean Heart Rate Level by Phase for B.A. FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 120 APPENDIX G Mean Heart Rate Level by Phase for C.N. VOLUME 21, NUMBER 2, SUMMER 2006 121 APPENDIX H Mean Heart Rate Level by Phase for D.P. FOCUS ON AUTISM AND OTHER DEVELOPMENTAL DISABILITIES 122 APPENDIX I Mean Heart Rate Level by Phase for D.V. VOLUME 21, NUMBER 2, SUMMER 2006 123 APPENDIX J Mean Heart Rate Level by Phase for S.M.