In Search of the Locus of Information Technology Business Value:
advertisement

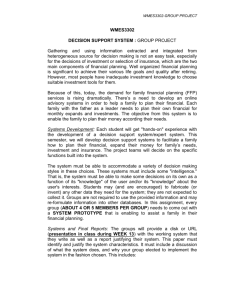
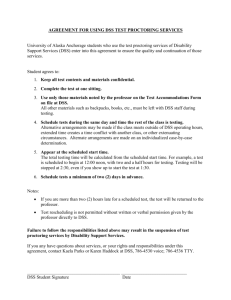
In Search of the Locus of Information Technology Business Value: Do measurement levels make a difference? Rajiv Kohli Mendoza College of Business University of Notre Dame Notre Dame, IN 46556 rkohli@nd.edu http://www.nd.edu/~rkohli Draft: March 21, 2004 Acknowledgements: Preliminary findings of this study were presented at Americas Conference on Information Systems (AMCIS), 2003 in Tampa, Florida. In addition to suggestions from the conference attendees, the paper has benefited from the comments from Sarv Devaraj, Bill Kettinger, Nigel Melville, Ron Ramirez, and Detmar Straub. Please forward comments and suggestions to Rajiv Kohli at rkohli@nd.edu In Search of the Locus of Information Technology Business Value: Do measurement levels make a difference? Abstract The locus of information technology (IT) investments continues to generate interest to identify how and where to examine the payoff. This research study examines the locus of payoff resulting from IT investment in use of a DSS to improve over 30 business processes of a hospital and compares such payoff with the firm-level payoff. We examine the process level payoff through productivity as well as profitability measures. Examination of lagged payoff periods indicates that hospitals are more likely to find appropriate payoff at the process level. Further, viewed through coordination theory’s process interdependence constructs, the results suggest that processes that have reciprocal interdependence are more likely to benefit from the IT investment. In Search of the Locus of Information Technology Business Value: Do measurement levels make a difference? 1. Introduction One would expect a mail order company to invest in information technology (IT) to improve the order-taking and delivery processes and improve firm profitability. What if the IT investment instead led to no improvement in the firm’s performance? What if a hospital invested in an organizational decision support system (ODSS) to cut costs and be more efficient, but instead witnessed declining profitability? What could be the reasons for such unexpected outcome? Does IT investment lead to decline in the firm’s performance? Could it be that the locus of IT benefits lies among the processes, and not at the firm-level? If so, are certain processes more affected by IT investments than others? We explore these questions in the context of healthcare organizations that utilized DSS information and made decisions about operational changes within departments. In doing so, we also examine payoff differences, if any, among the type of processes resulting from the use of DSS information. Our findings indicate that process-level payoffs are indeed manifested differently than firm-level payoffs. We find that the impact of IT payoff is better understood when both efficiency and profitability of processes are examined. However, our findings indicate that processes demonstrate differential temporal improvements from IT investments both in the extent of the impact as well as the lag between investment and payoff. Although business value of IT investments continues to be important for researchers as well as practitioners, there does not appear to be a consensus on what and how to measure the organizational value of technology. The role of IT in enhancing the effectiveness of the organization has been a topic of discussion, and sometimes discord, among academicians. Discord also occurs due to differing measurement beliefs evident in the extant DSS literature and that of organizational studies (OS). The belief that IT leads to organizational effectiveness is especially contentious for DSS which were originally designed to support primarily individual decision making. This raises questions about the aggregation of benefits resulting from individual use in creating organizational effectiveness (Bregman 1995). Similarly, organization theorists raise the question of whether organizational effectiveness can even be measured meaningfully (Mohr 1982). Given that an underlying objective of organizational research is to generate a generalizable theory, measurement of a phenomenon lies at the heart of the theory construction. Nevertheless, Orlikowski and Barley (2001) propose that OS and IT can learn from each other, particularly for studies examining the impact of IT on organizations. In this paper we draw upon the OS literature to frame the issue of measurement of organizational effectiveness resulting from IT investment. Given that in our research setting the organizational DSS has been in place for a number of years, and its use within organizations is deeply entrenched, it is appropriate to reexamine the expectations and assumptions from initial deployment and research at the time DSS were developed. By incorporating findings of the extant literature in IT business value (Brynjolfsson and Yang 1996, Kohli and Devaraj 2003b, Mahmood and Mann 1997) and the research stream of DSS effectiveness (Forgionne and Kohli 2000, Keen 1981, Nault and Benbasat 1990, Sharda, et al. 1988), the goal of this research is to apply the learning of the value of ODSS to the operations of the organization. In doing so, we gather firm level as well as process level data from hospitals and examine ODSS impact on organizational performance. 2 2. Literature Review and Propositions In this section we review the theoretical foundations grounding this study. We draw upon the literature informing the DSS impact on decision-making and the rich literature of organization studies to examine the role of DSS information technology in an organizational context. The success or failure of information technologies largely depends upon its organizational adoption and impact. 2.1 Information Technology: Decision Support Systems DSS are traditionally used by individuals to deal with semi-structured decision scenarios by structuring the problem, generating alternatives and establishing a criteria for choosing the optimal alternative (Simon, et al. 1992). Given the focus on individual decision making and their preference to use or ignore the recommendation, McLean and Riesing (1977) concluded that DSS were discretionary and need not extend beyond the individual decision making needs. Perhaps this conclusion was based upon the narrow definition proposing that DSS were designed to suit an individual’s decision scenario. Nevertheless, contrary to this early view of how DSS can and should be used, DSS were expanded to support group decisions and called Group DSS (GDSS). Later studies developed GDSS evaluation criteria by including voting by group members, conflict resolution, and negotiation (Adkins, et al. 2003, Eden 1995, Tyran, et al. 1992). Hackathorn and Keen (1981) recognized that although DSS originated to support individual decision making, the challenge was in exploiting DSS in an organizational context. They called attention to the fact that most DSS literature had emphasized individual managerial support and future research needed to examine organization-level impact of DSS. 3 Level of Analysis Economy Organization (Firm) Department/ Process Individual Information Technology Business Value Strengths Weaknesses • Any investment should improve • Inherently contain measurement ‘noise’ overall productivity of the economy resulting in mixed results • With enormous investments, the • Poorly performing firms negate the benefits stakes are higher than for any single of higher performance firms organization • Findings result in actionable recommendations • The investment should eventually firm add value to the firm • Intra-firm activities can compete with each other to mitigate organizational benefits • Strategy-IT misalignment can obliterate business value ------- Operational Level ------• Conversion contingencies • DSS do not support a department or process reside at the department or process directly, only through improved individual level decision-making • Process improvements • Processes involve many individuals and contribute to the organizational DSS should take into account potentially improvements conflicting decisions and varying risk criteria • DSS are designed to support • Individuals decision process should be coordinated with decisions in other functional individual decision making by supporting human decision making area processes • For organizations investing in ODSS, • DSS also improve human individual decision making improvements decision making abilities by should eventually translate into organizational supporting creativity and what-if benefits analysis Decision Support Systems Effectiveness Figure 1: Levels of analysis in IT Business Value and DSS Later, another DSS study also found that most past DSS research had examined the influence of DSS capabilities on user behavior (Eierman, et al. 1995). Two decades after Hackathorn and Keen’s call for organization level DSS studies, few have taken on the challenge (Kohli and Devaraj 2003a) and much of the DSS evaluation research still remains at the individual level. Firms that deployed DSS in the early wave of automating decision-making have since extended their use organization-wide and for such organizations the issue is no longer whether DSS is perceived as useful, rather it is to examine how DSS impacts their business processes and 4 the organizations (Devaraj and Kohli 2000a, Devaraj and Kohli 2003, LeBlanc and Kozar 1990, Sainfort, et al. 1990, Tavana, et al. 1998). 2.2 Business Value of Information Technology Several early studies to measure the business value of IT showed mixed results (Barua, et al. 1995, Byrd and Marshall 1997, Francalanci and Galal 1998) or negative results (Lee and Barua 1999, Loveman 1994) giving rise to much publicized ‘productivity paradox’ (Ahituv and Giladi 1993, Roach 1987). Rigorous follow-up studies that laid to rest the productivity paradox argument also revealed that past economy or industry level studies should have been examining the impacts at the firm-level because at the economy-level or industry-level the IT gains by innovative firms can be offset by firms that did not implement IT successfully (Brynjolfsson 1993, Brynjolfsson and Hitt 1995, Brynjolfsson and Hitt 1998, Devaraj and Kohli 2000a, Hitt and Brynjolfsson 1996, Mooney, et al. 1996). While the DSS literature is facing the challenge of moving from the micro to macro level, the business value of IT or IT payoff literature appears to face challenges to move from the macro level to micro level (See Figure 1). Subsequent to the emergence of firm-level impacts, there are now growing demands that to truly understand how organizations benefit from IT researchers need to examine IT’s role in improving business processes (Chircu and Kauffman 2000, Lillrank, et al. 2002). After all, they contend, it is the aggregated improvements in business processes that eventually lead to organizational impacts. Further, information technologies tend to be closest to the business processes which they aim to support and are less prone to ‘noise’ in their payoff measurement. 5 As illustrated in Figure 1, the IT business value literature calls for measurement at the firm or the process level. However, in the OS literature, Mohr (1982) suggests that organizational, or firm level, benefits are too elusive to be measured; even when they are measured, they may not be generalizable. Further, he argues that it is unlikely that there can be a theory of organizational effectiveness as the two terms are impertinent to each other (pg. 132). Doubts have been cast that aggregation of several optimized functional areas can result in overall organizational effectiveness (Bregman 1995). Although each approach has its strengths and weaknesses, intuitively the operational measurement provides managers with potentially actionable findings. Process or operational level findings are likely to be actionable because managers have greater control over the processes as compared to the firm. Of course, process level data can be aggregated into firm level so that there is no loss of meaningful information. However, it is advisable to gather process-level data because firm-level data cannot be easily broken down in to native processes. Firm level impacts are also susceptible to distortions due to mutually competing processes or misaligned strategies. For instance, in the above example of the mail order firm cited in the Introduction (above), the efficient order-taking process competed with the order-fulfillment process and in the end made the firm inefficient. While the orders were coming in faster, the order fulfillment process did not change and the order fulfillers spent a significant amount of time in sorting incoming orders. The above discussion of the IT business value and the DSS literature demonstrates the tension in measuring the business value of a DSS – a significant organizational IT investment. Thus, further research is needed to closely examine process level measurement of IT value vis-àvis that at the organization level. Organizational DSS provide an opportunity to further an organization’s decision making paradigm and, therefore, render it important to measure their 6 investment. The quality of individual decision making is generally represented by the improvements in the process and the design of decision outcomes (Forgionne and Kohli 2000, Forgionne and Kohli 1996). However, the manifestation of organizational decision making remains scantily explored and few studies have examined ODSS impact at the process level. Poole and Van de Ven (1989) propose that the level of an organization is a legitimate research issue and suggest a multi-level analysis as one of the ways to resolve the equivocal findings in the literature. The method for multi-level analysis begins with a comparative analysis and then proceeds to clarify the findings at the level of analysis. Figure 2 presents such a framework to examine the levels of measurement in IT business value literature, the metrics involved and a sampling of past studies. Macro Level Economy Organization Department/ Process Individual Micro Payoff Objective Quantify the impact of IT spending for welfare of the citizens Assess how the investment in IT helps the organization become more effective Examine the role of IT in improving organizational process outcomes Examine the role of IT in improving an individual’s decision making process, quality of decisions, and productivity Metrics Overall productivity, GDP Sample Past Studies Stiroh, Strassman (1990), ROI, Sales/per employee, Market share, customer satisfaction, overall profitability Throughput rate, Accounts receivable days, Days of cash, Hitt and Brynjolfsson (1996), Kohli and Devaraj (2003), Barua and Mukhopadhyay (1991) Number of alternatives, profitability of decision option Forgionne and Kohli (1996; 2000), Udo, (1992) Mukhopadhyay (1997); Patsko et al. (1994) Figure 2: Level of analysis in Decision Support System (DSS) research 7 3. Research Design Our research analyzes monthly process level data from three1 healthcare organizations. Each process represents a department of the hospital engaged in a specialized function of the hospital. For example, the radiology department represents a process in which a patient undergoes several steps in preparation for diagnostic imaging. Given that a hospital’s profitability is determined by how well it treats the patient, the efficiency of (sub) processes such as the radiology process, is critical. DSS serve a critical role in determining process costs versus reimbursed amount for calculating operational efficiency and profitability of the radiology or other such departments. Findings from such analysis can inform process managers to target areas of operational efficiency improvement e.g. via automation and process redesign. 3.1. Research Setting The research setting is a national health system comprising of several suburban, mid-sized acute care hospitals represented in various geographical regions of the US. With over 4,000 combined beds, 20,000 employees, and annual operating revenue of approximately $1.5 billion, each hospital is an independent legal entity with its own board and financial statements. Productivity and profitability data were collected for 26 monthly periods that were affected by the use of an ODSS to generate the above mentioned analysis. The hospital processes, representing departments, follow the continuum illustrated in Figure 3 in which patients enter the hospital and pass through a series of processes – administrative as well as clinical -- before being discharged. 1 In this paper we report detailed results of one hospital. The findings of two other hospitals (not reported here) were similar to those reported in this paper. 8 Hospital Process-level Radiology Process Patient Ancillary Services Home Health Firm-level Continuum of Patient Care Ob/Gyn Process Pathology Process Pharmacy Managers and Analysts DSS Figure 3: DSS and its impact on Process-level and firm-level measurements in a hospital. A circle represents a measurement point. Clinical as well as financial decision makers analyze operational data to make process improvements, analyze process costs and outcomes, while marketing and corporate development managers utilize DSS to analyze contracts by comparing costs of expected services and expected payments from insurers. The impact of IT investment and hospital clinical and administrative productivity has been examined in several process specific studies of digital technologies as well as enterprise resource planning (ERP) systems (Gell, et al. 2003, Reiner, et al. 2002). Use of data warehouse, as was the case in the organizational DSS reported in this study, to improve performance and reduce costs continues to be studied among hospitals (Wisniewski, et al. 2003, Zhan and Miller 2003). One of the key goals of hospital managers is to identify areas of cost cutting and operational improvements necessary for financial viability of the hospital. 9 CT Cardiac Cath Lab/ Angioplasty Clinical Lab Diagnostic Imaging Echo cardiology EEG, EKG Endoscopies MRI Ultrasound X-ray Sleep Lab Special Procedure Ultrasound Administrative Admissions Transportation Chem Dependency / Detox Rehab Diabetic Care Gastroenterologists Labor and Delivery Nuclear Medicine Oncology Out patient surgery Physical Therapy Psychiatric PACU Renal Medicine Respiratory Care Short-stay / Observation Speech Therapy Surgery Services Ancillary Service Blood Bank Observation (Radiology) Other Ancillary Pathological Lab Pharmacy Routine Services Supportive Diagnostic Acute Care Sub Acute Anesthesiology Cardiac Rehab CCU (Coronary) Emergency Dept ICU Inpatient Surgery Medical / Surgical Neonatal ICU Nursery OB Open Heart Pediatrics Post Acute Behavioral Care Home Care Service Occupational Therapy Pain Therapy Figure 4: Hospital Process Flow The profitability of the firm (hospital) is captured in the Net Operating Income, whereas the departmental process can provide profitability and productivity indicators. Greater detail of the hospital process flow is illustrated in Figure 4. The key phases of the process are in indicated in the diamond-shaped boxes – administrative, diagnostic, acute care, supportive, sub-acute and post acute. Processes are represented in the boxes linked to the phases. The process managers, with support from IT analysts, access the DSS to review process performance and make decisions to ensure that the processes are optimized and costs are under control. DSS clinical and financial project leaders work with departmental managers to identify variations in the departmental costs, 10 productivity and profitability. In doing so, they also monitor quality outcomes. They examine DSS reports and arrange for meetings with department administrators and clinical directors to identify areas of improvement. The steps followed by the decision makers to utilize the DSS for such decision making are demonstrated in Figure 5. A detailed illustration of the steps is illustrated in Figure 6 and also described below (independent variables). Each department has selected a primary statistic to measure the productivity on an on-going basis. In addition, the finance department captures departmental costs and revenue to assess the aggregated hospital costs such as Excess Revenue over Expenses (ER). All the variables used in this study are standard indicators for departmental and hospital activity are routinely reported in the financial statements and are applied for making other managerial and strategic decisions, in addition to mandatory reporting to state and federal agencies. For instance, Primary Statistic (PS) is used by departments to justify resource consumption, budget projections and is a critical input in developing accurate costs. Financial managers utilize Primary Statistic and Excess Revenue over Expenses in projecting revenue targets, contract pricing and recommend process redesign opportunities to departmental managers. Further description of the variables is provided below. In order to avoid over-stating or under-stating IT investment, we used the two variables PS and ER as control variables e.g. when PS was the dependent variable, we utilized ER as one of the explanatory variable; similarly when ER was utilized as the dependent variable, PS was used to control for changes in productivity. Such reciprocity can also account for unexplained changes in departmental activities. 11 1 Outcomes dashboard highlights misaligned processes 6 2 Process managers examine outcomes in ‘Responsibility Reports’ Process, Cost, and Quality outcomes stored in DSS-data warehouse 5 3 Managers, Physicians make changes to patient care processes DSS analysts conduct cost analysis for ‘areas of opportunity’ 4 Process Managers, Physicians, Quality team examine cost analysis Figure 5: The process improvement cycle indicating how data translates into actions among the hospital processes 3.2 Dependent Variables Each process consists of expenses, resources consumed, productivity, and profitability measures. Similar analysis is conducted at the organizational level to compare with the process level outcomes of ODSS use. Following the work of Hitt and Brynjolfsson (Hitt and Brynjolfsson 1996), we rely upon the past literature to examine the productivity and profitability because IT value can manifest in more than one way. 12 Each morning when the VP of Outcomes Management, Bruce arrives at work he studies the ‘outcomes dashboard’ on his computer for a status of hospital processes. Drawing data from the clinical and financial information systems and the decision support data warehouse (DSS), the dashboard presents a color-coded view of key performance metrics such as length-of-stay (LOS), costs, reimbursement, and patient satisfaction for each hospital process. The color codes are green (aligned), yellow (caution) and red (misaligned). The adjacent column has data from the hospital with which he benchmarks his hospital. October 1 (Step 1) Bruce notices that the costs for DRG 209 in the Cardiology process are in ‘yellow’ and on the rise. As he examines these outcomes, he receives a call from a member of the quality council who also viewed the dashboard. They decided to call a meeting of the process managers and physicians. October 10 (Step 2) Bruce and the quality council review a copy of the ‘responsibility report’ that shows budgeted and actual costs, volumes, employee hours for the process. Responsibility reports are periodically sent to process managers to show the status of the resources for which they are administratively responsible. Clare, the DSS analyst assigned to the process, conducts analysis for each severity-adjusted procedure and shows projected vs. actual patient volumes, labor hours, revenues and cost components. Finally, the analysis compares the outcomes data with the benchmarked institution to assess the locus of differences in patient care process and resources consumed. Clare also coordinates with her counterpart at the benchmarked hospital to ensure that the analysis is not confounded due to differences in accounting and measurement practices. October 25 (Step 3) Clare presents the findings and ‘areas of opportunity’ at the meeting of quality council, process managers and physicians. Jointly, the group identifies changes needed to align LOS, quality, and cost outcomes. A subsequent conference call followed by a visit to the benchmarked hospital reveals some innovative ideas for improving process performance e.g. the benchmarked hospital moved the cardiac patients sooner from Cardiac Recovery Unit (CRU) to the Progressive Care Unit (PCU). This is because the ratio of nursing staff-to-patients is significantly higher in the CRU, thus increasing labor costs. These improvements also resulted in process efficiency because more patients could be scheduled for cardiac procedures in the CRU. The patient recovery was faster in PCU perhaps because the patient got more rest, thus reducing the LOS. November 15 (Step 4) Process managers and physicians meet to finalize concrete steps to improve patient outcomes as well as operations relating to use of supplies, job restructuring, and steps to reduce the LOS. Frank and Dave, DSS clinical consultants, now join the team to assist process managers and physicians with the analysis of how changes on the hospital floor can impact the clinical outcomes. They analyze historical data from the decision support-data warehouse and, combined with recent clinical literature, assist physicians in developing best practices, also called clinical pathways. December 10 (Step 5) Process managers begin making changes in staff scheduling, clinical pathways, and dispensing pharmaceuticals and supplies. Physicians also share with their colleagues new practice guidelines including use of diagnostic and pharmacy in their bi-weekly meetings. January – February (Step 6) Data from redesigned processes are gathered in clinical and financial systems, the DSS-data warehouse, and appears in ‘green’ metrics on the dashboard. Bruce and Quality Council send a ‘kudos’ message to the process managers and physicians. On a mid-February morning as Bruce listens to a congratulatory voicemail from the COO, the Dashboard shows that another process metric has changed to ‘yellow.’ Figure 6: Vignette illustrating role of IT investment in hospital processes 13 Table 1: Dependent variables and description Dependent Variable Description Primary Statistic (PSit) Units of productive activity for the processi during timet period (Process Level) Excess of Revenue over Expenses (ERit) Net Income (NIt) Revenue exceeding the expenses of the processi during timet period. (Process Level) Net Income of the hospital during timet periods (Firm-level) References in the Literature Gapenski et al. 1993; Langland-Orban et al. 1996; Shi 1996; Teplensky et al. 1995 (Hay 2003, Mosley 2000) 3.3 Independent Variables IT Expenditure captured expenses booked to the general ledger for IT Labor. As illustrated in the vignette and the Figure 1, the change in the process is a labor intensive process, therefore we included IT Labor as the IT expenditure. Other expenses such as capital and support were not used because these investments in DSS had already been made and no special hardware, software or external consulting support to implement the DSS was used. The DSS is an established tool for the hospital with a long history of support applications to facilitate billing, cost management, claims processing and reimbursement modeling. In the research reported here, the DSS was being used for process evaluation and improvement. Primary statistics represent units of productive activity chosen by a functional process area to track its performance such as number of laboratory tests, number of x-rays, or number of patients registered, while Excess Revenue over Expense (ER) represents the profitability of the process function. Medicaid and Medicare In the US, the state government pays for low income patients’ healthcare expenses through the Medicaid program while the federal government pays for the healthcare expenses of senior 14 citizens through the Medicare program. The two variables represent the percent of services offered by the hospital for patients covered under these programs. We control for these effects because Medicare and Medicaid patients can be more costly to treat and reimbursement for such patients is typically less than that from other payers for similar services. Table 2: Independent variables and description Independent Variable IT Expense ($) (IT_LABOR)it-1-5 Operating Expense $ (OE)it-1-5 Medicaid (MEDICAID t-1-6 ) Medicare (MEDICARE t-1-6 ) HMO (HMO t-1-6 ) Casemix (CASEMIXt-1-6) FTE Hours (FTE t-1-6) Description IT Expense for processi lagged 1to 5 timet periods (Process Level) Operating Expense for processi lagged 1to 5 timet periods (Process Level) Percent of Medicaid admissions at hospital lagged 1 to 6 timet periods (Firm-level) Percent of Medicare admissions at hospital lagged 1 to 6 timet periods (Firm-level) Health Maintenance Organization penetration lagged 1to 6 timet periods(Firm-level) Case mix for hospital lagged 1 to 6 timet periods (Firm-level) Full Time Equivalent Employee hours lagged 1 to 6 timet periods (Firm-level) References in the Literature Devaraj and Kohli 2000, (Menon and Lee 2000) Barker 1999; LeFebvre 1999 (Zarling, et al. 1999) (Landon, et al. 2004) (Bazzoli, et al. 2000) (Challiner, et al. 2003, Hay 2003, Jackson 2001) (Bui, et al. 2004) Health Maintenance Organizations (HMO) We include HMO percentage as a measure of the competition in the market. HMO’s are characterized by their preferences for preventive services and management of patient costs. It can be expected that greater HMO penetration in a market will lead to lower profitability for the hospitals. Therefore, we include HMO as a control variable in our model. Case Mix The Casemix index is a measure of the range of services offered by the hospital. The higher this measure, the more complex the services rendered by the hospital. Revenue and 15 Reimbursement can be affected by higher casemix due to higher resource consumption generally expected for such services. FTE Hours Our operationalization of the FTE Hours variable was through the number of employee hours to provide a measure of the labor intensity. The relationship between the number of employees and organizational performance has been of interest to healthcare management researchers and is accounted for in our model. Lag Effects It is conceivable that impacts of IT investment may be observed at a later time in the process. Thus, longitudinal studies offer the advantage of modeling and testing such time-lagged relationships. Peffers and Dos Santos (1996) concluded that impact of IT on performance in banks occurred after certain time lags and contend that cross-sectional studies conducted soon after an application is installed may fail to find benefits. We employed three criteria to establish the credibility and optimality of the lag effects considered: a. Field interviews with managers to assess their expert opinion on appropriate lags b. Literature review of studies in healthcare that document time-lagged effects of operational changes on hospital performance c. Use of statistical criteria (Akaike’s Information Criteria and Schwarz’s Criteria) (Akaike 1978, Schwarz 1978) to compare models with varying lag effects to select the best-fitting model In contrast to start-up organizations where the infrastructure deployment can take several months or even years, the DSS infrastructure in the hospitals to support clinical and financial initiatives has been in place and the DSS is widely used to identify operational improvement opportunities. Our interviews with managers responsible for implementing the improvement 16 initiatives also supported the view that changes in operations occur soon after a DSS report highlights an opportunity for improvement (See vignette in Figure 6). One manager stated that “[once identified]…the change [in operations] happens within weeks, whereas the financial impact may be felt in a few months.” Therefore the lags were primarily due to the department managers and physicians incorporating the new process into practice, followed by the time involved in compiling medical and billing cycle with the insurance companies. Further detailed interviews with managers suggested that due to the billing cycles involved it takes about 45–60 days for the financial accounting systems to reflect any changes made in the operations. Previous studies in clinical operations have suggested lag effects of less than six months. Relative to other IT impacts, shorter lead times in clinical settings can be ascribed to the implementation of ‘evidence-based practice’ that promotes making early process changes based upon published clinical evidence (Silagy and Lancaster 1995). For example, process changes in the emergency department resulted in a reduction of laboratory utilization with a lag of six months (Dickinson 1987), respiratory infections were reduced significantly after a lag of four months of a redesign initiative (Joiner, et al. 1996). Our analyses of lag effects using all the criteria listed above suggested a 1 or 2-period lag for the efficiency of operations and 4 or 5-period lags before the financial impact was evident. Therefore, we test the impact of technology on operations in time period t- (1-5) on hospital performance in time period t. To test the basic theme of this paper Proposition 1 (P1) proposes that process-level and firmlevel payoffs will be different. To further the above proposition, Proposition 2 (P2) proposes that IT investment will better explain payoff at the process-level than that at the firm-level. In addition to the above captured variables, we code the locus of the process in the overall hospital patient care process. The six steps in the hospital process flow (See Figure 4) are common to all acute care 17 hospitals such as the ones utilized in our research. The need for understanding the healthcare process flow as “….a means to define and manage the events, roles, and information integral to health-care delivery…(Buffone, et al. 1996)” has been suggested to deal with increasing pressures to reduce costs and improve quality. Marrin and colleagues (1997) argue that finding cheaper supplies and reducing patient LOS may serve in short term cost control, [but the] long term success depends upon the reduction of costs by understanding process dependencies and reengineering the processes of care. Similar calls to understand the process flow and linkages of sub-processes have been made in manufacturing systems where workflow dependencies have a significant impact upon firm performance (Albino, et al. 2002, Kim 2000). Albino et al., propose a methodology to describe information flows involved in the coordination of production processes. They suggest that by assessing the process coordination load, i.e., the effort required for resources to address coordination problems, managers can enhance the adopted coordination form, improve the performed process, and support the selection of the coordination technologies that better satisfy the information requirements. Indeed, coordination theory can enhance our understanding of process interdependencies and thus the opportunity for IT to make a difference. Thompson (1967) (pg. 54) cites three basic interdependence mechanisms – pooled, sequential, and reciprocal -- that can be help understand the coordination needs of an organization. In an increasing order of interdependence, pooled process have the least interdependence with other process and usually can be coordinated by process standardization. Sequential processes depend upon inputs from other processes; similarly making process down the chain interdependent upon their output. Process coordination in such situations is executed with an agreed upon plan. Finally, in a reciprocal interdependence the processes improvise their roles and functions and mutually adjust to the 18 changing needs of the other(s). Reciprocal interdependence has high coordination costs resulting from communication and decision making. In Proposition 3 (P3), we propose that due to varying interdependencies and resource requirements, IT will impacts hospital processes in different ways. In other words, some processes will benefit more from IT investment than others. Table 3: Propositions Proposition P1 P2 P3 Description IT investment payoff will manifest differently* at firm-level vs. process-level IT investment will better** explain payoff at the process-level than that at the firm-level IT investment payoff will affect processes differently* with in the organization 4. Data Analysis The analysis involves a regression equation to examine the impact of IT investment upon the process level performance. Similarly, another regression equation measures the impact of IT investment upon the firm i.e. hospital. These two will be compared to examine if the impact of IT is found to be the same at the process and the firm level. The regression equations will include the common variables to control for the complexity and volume of services in the hospitals. A sample set of equations is as follows: Process level Performance: Excess of Revenue over Expenses (ERit) = α + β1 * (lagged value of IT Expenditureit-1-5 ) + β2 Primary Statistic (PSit) Primary Statistic (PSit) = α + β1 * IT Expenditureit-1-5 + β2 Excess of Revenue over Expenses (ERit) Firm level Performance: Net Income (NIt) = α + β1 * IT Expenditure + β2 * Employees + β3 * Casemix index + β4 Medicare + β5 * Medicaid + β6 * HMO 19 We anticipate that our findings will shed light on the relevance of measuring information technology value at the process level. The findings will provide guidance to business organizations as well as researchers on where to examine IT value. The results will suggest conditions under which the organizational or process level of measurement is preferred. Such findings will provide guidance to the organizations as to where and how they are likely to find value for their IT investment which occasionally appears to get lost in the measurement process. 4.1 Specification tests Causality Tests: Longitudinal analysis presents some challenges in the estimation procedure as compared to cross-sectional data because there is an implicit assumption of causality in the analyses. Therefore, a useful specification test is to check for reverse causality. In other words, can the same or similar results be obtained by reversing the dependent and independent variables. A standard statistical procedure to address this issue is the Granger Causality Test. We were unable to reject the null hypothesis that usage ‘granger causes’ performance. Therefore, we believe that it is not performance that drives technology investment but vice versa [to be done]. 4.2 Diagnostic checks on residuals Several diagnostic checks were done on the residuals to insure that the assumptions of time series analyses are not violated. Specifically, tests for serial correlation, normality, and heteroscedascity were performed. An observation of correlograms as well as Q-statistics confirmed that the final models did not exhibit serial correlation. Although the data does not constitute a panel dataset because each process of each hospital is examined separately, given that we study multiple periods, we examined the Durbin-Watson (DW) statistic. Such an examination revealed 20 that the DW statistic was not significantly different from 2 for each process, indicating that serial correlation was not a problem. Normality was tested using Shapiro-Wilk test. The Shapiro-Wilk test is suitable for smaller sample sizes and calculates a W statistic that tests whether a random sample, x1, x2, ..., xn comes from a normal distribution (Shapiro and Wilk 1965). Small values of W are evidence of departure from normality, however, in our case the p-values obtained did not indicate a violation of the normality assumption. White’s test (White 1980) is a test of the null hypothesis of no heteroscedascity against heteroscedascity of some unknown general form. White’s test statistic, as well as the reported F-statistic, did not indicate heteroscedascity to be a problem. 4.3 Results The estimation results for two separate dependent variables for productivity and profitability are presented in Table 4 and Table 5. Firm-level impact of IT investment is shown in Table 62. The results of the estimation model indicate that the hypothesis that IT leads to the firm’s profitability cannot be supported. Process productivity as measured by the IT investment and controlled for increased patient activity as represented by profitability was positively and significantly associated at the .05 significance level in 20 out of 36 processes. Thus, there is strong statistical support for the role of IT in improving process productivity performance. Thus, Proposition 1(P1) is supported. 2 We also utilized another model including primary statistics (PS) = IT Labor + ER (Expenses over Revenues) + AdjOE (Adjusted Operating Expense) but it displayed high multicollinearity. AdjOE and ER are expected to be correlated because profitability is related to costs. We then dropped one and used the other, one at a time with PS=IT_Labor (1-5) + ER; ER = IT_Labor (1-5) + PS. We also examined adjOE for ER in the above two models and the results were similar. 21 The results also indicate that the impact of IT investment appears after a lag of one period. This is consistent with hospital activities to change processes depicted in Figure 6 where the changes begin to take hold within the next two months. In the second set of results, reported in Table 5 corresponding to profitability as a dependent variable, the results indicate that IT investment is associated with 21 out of 39 processes. Further, an examination of the lag period indicates that the lag effects appear later than productivity. This is expected because primary statistics represent IT’s impact on processes, a prerequisite to overall improvement and subsequent increase in profitability. Thus Proposition 2 (P2) is supported. Finally, when mapped upon the locus of the process on the patient care continuum the process results suggest a greater likelihood of IT’s positive impact among the middle processes i.e. acute care, supportive and sub-acute. IT’s impact on the beginning and ending of the patient care process is not as significant as the middle processes. Our discussions with managers suggest that this may be because business process redesign initiatives over the past decade have optimized the workflow for such processes. The middle processes represent high coordination between process personnel and as such are not easy to automate. For instance, while admissions and transportation processes (administrative) have been redesigned and automated, acute care processes such as intensive care unit (ICU), open heart surgery and emergency department are relatively challenging to automate without rigorous analysis of patient outcomes data. Use of DSS data to actively analyze processes and make process changes demonstrates the strategic informating role of IT (See Figure 5). We note exceptions of IT’s role in process productivity and profitability i.e. all processes showing productivity improvement were not the ones that demonstrate profitability improvement. For instance, process BLDBNK showed improvement productivity but not in 22 profitability. Such instances represent areas of future opportunity in which the improved productivity needs to be linked to the profitability. Table 4: Estimation Results: Information Technology investment measured by Dependent Variable: Primary Statistic (Productivity) DEPT ULRSD MRI CLNLB EEG ENDSP CT CCUNT EKG ANSVS PHARM RDLGY BLDBK RTSVS IVDEP DFNOB ICUNT CRDCT ANEST INPSG MDSRG OPHSG OTCRD PACU OB OTPSG RNLMD SGSVS SCHTR ONSVS PHSTR OTANC NCLMD RSPCR CRDRB OCPTR PNTRP Locus 2 2 2 2 2 2 2 2 3 3 3 3 3 3 4 4 4 4 4 4 4 5 5 5 5 5 5 5 5 5 5 5 5 6 6 6 Intercept 582.5545 32.6546 9233.827 20.57862 85.73855 282.4476 12.87872 703.5868 566961.8 486200 2825.262 929.0347 1861.684 738.4311 70.08819 55.44074 113.2817 175.1396 290.9383 386.6182 19.12287 235.7398 -108.625 534.1415 297.6899 163.2405 262.6869 377.5415 2933.575 6777.401 5282.416 -155.107 -2649.99 1493.667 -466.262 1124.661 it_labor1 -0.00091 0.000103 -0.00525 -8.1E-05 0.000556 -0.00011 -5.9E-05 0.000284 -1.01092 -0.80504 0.012296 0.003391 0.004492 0.004183 0.001289 0.000248 0.001521 -0.00352 0.001682 0.003246 -6E-06 7.64E-05 0.001503 -0.00212 -0.0009 -0.00027 0.006283 0.001352 0.010597 0.021114 0.038402 -0.00092 -0.03197 0.00162 0.003486 0.009089 it_labor2 -0.00014 -0.00012 0.031459 -0.00011 0.000351 0.000164 -0.00017 -0.00031 -0.49269 -0.28366 -0.00411 0.007362 0.000222 -0.00369 0.001133 0.000694 0.000571 0.0013 -0.00448 0.000785 0.0002 0.000138 0.000638 7.08E-05 0.001166 -0.00037 0.015849 -0.00079 0.010011 0.011321 0.01592 -0.00037 0.010496 0.000283 0.007739 0.00316 it_labor3 0.001031 -3.3E-05 -0.08034 0.000114 -0.00026 -0.00076 7.6E-05 -0.00115 -1.95099 -2.04382 -0.00944 -0.02636 -0.00441 -0.00707 0.000781 -0.00048 -0.00044 0.002376 -0.00373 -0.00159 3.23E-05 0.000182 -0.00087 -0.00107 -0.00178 0.000347 -0.00911 -0.00056 0.000132 -0.02352 -0.01439 -0.00172 0.046758 -0.00175 -0.00161 -0.00888 23 It_labor4 -0.00154 0.000152 -0.02213 -0.0003 -0.00104 0.000402 0.000504 0.00011 0.625562 0.334809 0.001043 -0.01216 0.00121 0.002298 -6.7E-05 -0.00034 -0.00088 0.001193 -0.00028 5.4E-05 -7.7E-05 -0.00029 -0.00087 0.000125 -0.00079 0.000569 -0.02022 -8.2E-05 0.004089 -0.01503 -0.02355 -0.00037 0.010045 -5.9E-05 -0.00752 -0.00616 it_labor5 0.000949 -0.0003 0.08513 -3.9E-05 0.000484 0.000346 -0.00019 0.000546 1.701586 1.285289 0.0008 0.023833 0.002719 -0.00112 -0.00036 -8.4E-05 -0.00111 -2.5E-05 -0.00094 0.000922 -0.00015 -4.5E-05 0.000635 0.001776 0.002186 -0.00016 0.010327 0.000385 0.034231 0.020688 -0.00285 0.000462 0.015864 0.001405 0.009535 0.004054 ER 0.00133 -8E-05 0.02109 0.00674 0.00191 0.00093 0.00104 0.00961 -0.0112 -0.0635 0.00603 0.00308 0.00108 0.01963 0.00105 0.00096 0.00037 0.0019 0.00062 0.00155 9.1E-05 5.4E-05 0.00418 0.00064 4.3E-06 0.00113 0.00124 0.00615 0.01535 0.02118 0.01287 0.00296 0.01195 0.00035 0.01661 0.0134 adjR2 -0.35955 0.066481 0.392241 0.395277 0.684715 0.841752 0.887101 0.914596 -0.23951 -0.17712 0.080851 0.530544 0.551115 0.850732 0.606051 0.675155 0.696058 0.701974 0.787374 0.804765 0.867182 -0.65786 -0.13333 -0.07264 -0.07125 -0.00242 0.28372 0.399277 0.481605 0.665741 0.76602 0.850899 0.889293 -0.6169 0.239066 0.795386 Sig 0.8707 0.4084 0.1145 0.1127 0.0116 0.0009 0.0002 0.0001 0.7595 0.6921 0.3922 0.0481 0.0411 0.0007 0.0259 0.0129 0.0101 0.0094 0.0027 0.0019 0.0004 0.9974 0.6423 0.5711 0.5695 0.4881 0.1923 0.1102 0.0675 0.0143 0.0038 0.0007 0.0002 0.9926 0.2307 0.0023 Table 5: Estimation Results: Information Technology investment measured by Expenses over Revenues (Profitability) DEPT MRI EEG ENDSP CLNLB CT EKG NRSRY ULRSD PHARM ANSVS RDLGY BLDBK RTSVS IVDEP CRDCT DFNOB ICUNT ANEST MDSRG OPHSG CCUNT INPSG OTCRD CRDRB DBTCR PACU RNLMD SGSVS OB SCHTR PHSTR ONSVS OTPSG OTANC NCLMD RSPCR HMECR OCPTR PNTRP Locus 2 2 2 2 2 2 3 3 3 3 3 3 3 3 4 4 4 4 4 4 4 4 5 5 5 5 5 5 5 5 5 5 5 5 5 5 6 6 6 Intercept 27421.73 658.3291 -20427.5 777076.6 -189315 -49234.9 142263 130234.5 2834058 11853645 207796.4 20701.52 547919.6 -9977.69 149020.5 286068.3 143888.5 79199.96 102795.6 -36987.4 3468.553 -130896 53186.57 44886.55 -739.035 164681.8 -16045.3 2195965 236411.9 -31800.2 -134170 -146738 872826.4 -199407 79053.46 512426.5 169.6707 70143.37 -63353.8 it_labor1 0.056622 0.000362 -0.14747 1.803445 0.333149 -0.00268 0.30858 0.19852 5.254199 4.959548 -0.84893 -2.63621 -3.40717 -0.17606 -2.77862 -0.49992 -0.05574 1.823319 -1.48021 0.195272 0.133699 -1.93007 1.215085 0.308575 0.017638 0.272928 0.042468 -0.60435 -0.49142 0.145171 0.152697 0.18527 -0.47292 -2.19726 0.345677 1.09214 -0.00086 0.178839 -0.62316 it_labor2 -0.19 0.009766 -0.14496 -2.60174 -0.10066 -0.00524 -1.55746 0.040976 -1.99377 -21.4127 0.094321 -2.02234 -4.95443 0.150677 -1.65282 -2.06592 -1.18968 -0.59963 -1.16772 -2.95288 0.116499 7.703465 -0.18282 -0.50736 0.012289 -0.03295 -0.02071 -5.74515 0.636945 0.259685 0.266165 1.085065 -2.50358 -1.44637 0.081894 -2.9799 -0.00335 -0.18927 -0.07241 it_labor3 -0.08913 -0.01077 0.173055 1.997837 0.666972 0.105766 -0.83128 -0.03437 -6.21843 -7.6197 0.471274 3.378715 2.286647 0.344689 0.38665 -0.47736 -0.49843 -0.9042 0.984646 -0.55708 -0.18864 7.297787 -0.26664 0.306203 -0.01179 0.095869 0.127207 8.091177 2.46664 0.136117 0.745499 2.401735 -2.0507 0.673462 0.461071 -4.34663 0.002328 0.101239 0.624685 24 it_labor4 0.033419 0.006152 0.503334 2.205602 -0.50149 0.022019 0.543872 -0.22617 1.869128 22.7629 0.790768 2.314297 1.343953 -0.1073 2.228533 1.156357 0.750906 -0.63964 0.207439 1.486902 -0.45523 0.075462 1.080314 0.032193 -0.0104 -0.0739 -0.26552 7.394899 -1.29797 -0.08141 0.030352 1.232702 -2.5301 1.884638 0.114429 1.28398 0.002297 0.311023 0.232078 it_labor5 -0.0569 0.027254 -0.29322 -5.47804 -0.35783 -0.10297 0.112423 -0.30503 -7.10017 -17.4111 -0.56573 -1.2717 -3.93842 0.006369 0.762906 -0.66385 -0.00996 -0.47157 -0.95496 0.843756 0.19066 -0.30525 0.004362 -0.29324 0.002365 -0.34706 0.049911 -11.6574 -1.77637 -0.28186 -1.03789 0.636605 -0.74698 -0.20092 -0.14131 0.120373 -0.00267 -0.52603 -0.27912 PS -206.153 64.41825 402.0404 20.96992 957.1822 92.08355 0 35.13843 -0.9063 -1.00923 46.85904 85.03485 580.8584 45.38173 1824.391 544.9929 702.3875 403.5064 540.9711 9412.256 868.9968 1249.996 213.5373 5.453598 0 67.03194 278.0623 340.5201 223.41 80.07992 27.289 16.70866 2.708278 59.79022 299.8112 66.76272 0 24.86885 60.06104 adjR2 -0.54294 0.290206 0.71322 0.758783 0.844655 0.918464 -0.37137 -0.21702 0.016162 0.050332 0.067696 0.335018 0.642321 0.833986 0.614891 0.730467 0.730536 0.773596 0.81754 0.885543 0.891759 0.89381 -0.23441 -0.20844 -0.19756 -0.0396 -0.03155 0.356224 0.387472 0.50546 0.635507 0.660529 0.719117 0.753935 0.825486 0.900738 -0.11622 0.303286 0.773468 Sig 0.9749 0.1870 0.0082 0.0043 0.0008 <.0001 0.9338 0.7358 0.4663 0.4268 0.4070 0.1527 0.0183 0.0010 0.0239 0.0065 0.0065 0.0034 0.0015 0.0002 0.0002 0.0002 0.7542 0.7266 0.7437 0.5320 0.5225 0.1378 0.1174 0.0575 0.0196 0.0152 0.0076 0.0046 0.0013 0.0001 0.6320 0.1766 0.0034 Table 6: Estimation results: Firm profitability measured by lagged information technology investment3 Intercept 15000104 0.504056 HMOP 265.46 0.6073 CASEMIX 3146552 0.809511 FTE -14515.5 0.522914 it_labor6 -24.3812 0.706834 MEDCARE -264.794 0.887663 MEDCAID 6812.208 0.562199 R2 0.196 adjR2 -0.491 Sig 0.92 A summary of results for the proposed hypotheses is presented in Table 8. Our analyses indicated support for the notion that IT’s impact on performance is more likely to be detected at the process level than at the firm level. This research provides empirical evidence that examining at the firm level alone may not present the complete picture. Table 7: Summary of statistical significant process-level and firm-level findings Productivity Pooled (1,6)4 1 of 3 (33%) PROCESS LEVEL Sequential (2,5) 9 of 20 (45%) Reciprocal (3,4) 10 of 13 (77%) FIRM-LEVEL _ Profitability 1 of 3 (33%) 10 of 20 (50%) 10 of 16 (62%) 0% Table 8: Results of Hypotheses Proposition Description Estimation Results P1 P2 IT investment payoff will manifest differently at firm-level vs. process-level IT investment will better explain payoff at the process-level than that at the firm-level IT investment payoff will affect processes differently within the organization Supported Supported P3 Supported 5. Discussion and Conclusions The results provide general support for the proposition that the firm-level and process-level measurements provide different answers for the impact of IT on hospital performance. Further, we find that process-level analysis is more likely to explain the impact of IT, although IT’s impact on the processes is not the same. 3 We also examined a model with 1-6 periods of IT investment. The R-square and significance were approximately the same as those reported in this model. 4 Pooled, Sequential and Reciprocal represent the three interdependence types (Thompson, 1967). The numbers in parenthesis represent the category of processes in Figure 4 and Table 4. 25 5.1. Implications Several managerial implications follow from the results of this study. First, there is evidence that investments in technologies have positive payoffs when the technology is considered at the process level. While past studies have proposed and examined process level impact of IT (Davern and Kauffman 2000, Mukhopadhyay, et al. 1997a, Mukhopadhyay, et al. 1997b), our study compares the process-level with the firm level for the same organization to make this case. Consistent with the message of previous studies (Davern and Kauffman 2000, Devaraj and Kohli 2000b), this study highlights the importance of IT investment alongside process redesign to arrive at higher productivity and profitability. Process impacts for productivity and profitability provide confirmation that the impacts were indeed tangible. The longitudinal nature of data enabled us to detect and verify significant lag effects on productivity and profitability measures of hospital performance. The results of this study suggest a temporal impact to technology payoff, i.e., payoffs may not be realized instantaneously but only after certain periods of time. The 1-period and 4-period lag (productivity and profitability, respectively) are consistent with managers’ expectation that hospital managers should expect IT investment to first impact productivity before the improvements in profitability can be noticed. Given that most past studies have assessed the relationship between technology investments and organizational performance directly, we measured the impact of IT investment on the same hospital for the same IT investment and for the same period and found the impact to be statistically not significant. The process-based approach proposed by Soh and Markus (1995) and Weill (1992) suggests that technology’s impact on organizational performance may be mediated through another variable, such as process productivity, in our study. 26 Our findings shed further light upon the IT’s differential impacts upon processes based upon the locus and interdependence of the processes. Managers can utilize these findings to prioritize and allocate IT resources toward processes that provide greater potential for productivity and profitability improvement. For instance, our study found that processes with reciprocal interdependence such as pathology lab, pharmacy and radiology processes which share reciprocal interdependence with inpatient surgery, emergency room and intensive care process can benefit from IT’s use more than other processes in the patient continuum. Yet, in practice these processes are considered crucial and remain human-intensive with little intervention of IT even for support purposes. We recognize that there is a distinction between clinical and information technologies, and that although such reciprocal processes extensively utilize clinical technologies, yet the use of IT in such processes remains relatively low. Contrary to our expectations, the administrative and post-acute processes demonstrated little or no impact of IT on their performance. Upon discussion with managers, we found that there were two possible explanations for this finding. First, the front-end and back-end services have been subjected to business process design (BPR) during the last decade resulting in near optimized processes. Second, IT labor investment, the variable in this study, impacts the administrative and post-acute processes less than other processes in the hospital’s continuum of care. 5.2. Limitations and future research This study employs data from hospitals of one health system, therefore, the principal limitation of this study is in the generalizability of its findings to other healthcare organizations or other industries. This, however, is a limitation of field studies in general. On the other hand, 27 field studies, such as the one reported here, have the advantage of providing access to experienced personnel, richer operationalization of reality, and the ability to capture detailed data over multiple time periods in a consistent format. As such, the findings reported here cannot be generalized to the larger population of hospitals or extended to other types of firms in other industries without further validation. Our use of operating income as a measure of firm-level performance has limitations because it does not take into account the efficiency improvement of the firm. Unlike process level data, e firm-level data do not provide a single measure to capture change in the hospital’s efficiency. Firm-level measures such as number of employees are affected by several variables. Although we used FTE (employees) as a control variable to account for resource consumption, estimation results do not support its statistical significance in the model. To the best our knowledge, this is one of the first studies to compare process-level with firmlevel impacts to identify differential process impacts from IT investment in a longitudinal setting. Future studies can examine how IT leads to improvement in processes by understanding the interaction of IT investment and complementary investments such as training, organizational design, reward mechanisms, in addition to process redesign. Future studies can also use the approach deployed in this study and apply it to other business settings such as manufacturing, financial services and retail. We recognize that previous studies have utilized firm-level data and have found IT impacts. Indeed, process level impacts should, and do, lead to firm-level impacts. Our study clarifies past findings to suggest that for DSS investment when the focus is upon cost management and process improvement, the process may provide a better locus of value than the firm. Although our findings of firm level analysis did not indicate improvement in a single period, we do not 28 imply that there were no IT impacts to the firm. A reason for these findings may be that the noise at the firm-level measurement may drown out the process impacts. Indeed, there are indications that extra-ordinary pressures upon hospitals from rising costs, increased scrutiny from insurance companies, lower reimbursement for services and strained resources in upgrading clinical technologies have affected hospitals’ productivity and profitability (Andrianos 1996, Marrin, et al. 1997, Menon and Lee 2000). Future research may combine process owners and managers’ perceptual variables of IT investment combined with objective productivity and profitability measures of IT impact for a holistic view of how IT leads to process performance improvements. Such comprehensive analysis can also bring to light reasons for discrepancies between process-level and firm-level IT impacts and help identify appropriate metrics for firm-level measurement. After all, IT impacts must eventually impact firm performance. 29 References Adkins, M., M. Burgoon and J. F. Nunamaker, "Using group support systems for strategic planning with the United States Air Force," Decision Support Systems, 34, 3 (2003), 315-337. Ahituv, N. and R. Giladi, "Business Success and Information Technology: Are They Really Related," Tel Aviv University, Israel, (1993), Akaike, H., "Bayesian-Analysis of Minimum Aic Procedure," Annals of the Institute of Statistical Mathematics, 30, 1 (1978), 9-14. Albino, V., P. Pontrandolfo and B. Scozzi, "Analysis of information flows to enhance the coordination of production processes," International Journal of Production Economics, 75, 1-2 (2002), 7-19. Andrianos, James Dykan, Mark, "Using cost accounting data to improve clinical value.," 50, 5 (1996), 44. Barua, A., C.H. Kriebel and T. Mukhopadhyay, "Information Technologies and Business Value an Analytic and Empirical-Investigation," Information Systems Research, 6, 1 (1995), 3-23. Bazzoli, G. J., L. Dynan, L. R. Burns and R. Lindrooth, "Is provider capitation working? Effects on physician-hospital integration and costs of care," Medical Care, 38, 3 (2000), 311-324. Bregman, R. L., "Integrating Marketing, Operations, and Purchasing to Create Value," OmegaInternational Journal of Management Science, 23, 2 (1995), 159-172. Brynjolfsson, E., "The Productivity Paradox of Information Technology," Communications of the ACM, 36, 12 (1993), 67-77. Brynjolfsson, E. and S. Yang, "Information Technology and Productivity: A Review of Literature," Advances in Computers, 43, (1996), 179-214. Brynjolfsson, E. and L. Hitt, "Information Technology as a Factor of Production: the Role of Differences among Firm," Economics of Innovation and New Technology, 3, (1995), 183-199. Brynjolfsson, E. and L. Hitt, "Beyond the productivity paradox," Communications of the ACM, 41, 8 (1998), 49-55. Buffone, G. J., D. Moreau and J. R. Beck, "Workflow computing - Improving management and efficiency of pathology diagnostic services," American Journal of Clinical Pathology, 105, 4 (1996), S17-S24. Bui, A. A. T., R. K. Taira, D. Goldman, J. D. N. Dionisio, D. R. Aberle, S. El-Saden, J. Sayre, T. Rice and H. Kangarloo, "Effect of an imaging-based streamlined electronic healthcare process on quality and costs," Academic Radiology, 11, 1 (2004), 13-20. 30 Byrd, T. A. and T. E. Marshall, "Relating information technology investment to organizational performance: A causal model analysis," Omega-International Journal of Management Science, 25, 1 (1997), 43-56. Challiner, Y., G. I. Carpenter, J. Potter and C. Maxwell, "Performance indicators for hospital services for older people," Age and Ageing, 32, 3 (2003), 343-346. Chircu, A. M. and R. J. Kauffman, "Limits to value in electronic commerce-related IT investments," Journal of Management Information Systems, 17, 2 (2000), 59-80. Davern, M. J. and R. J. Kauffman, "Discovering potential and realizing value from information technology investments," Journal of Management Information Systems, 16, 4 (2000), 121-143. Devaraj, S. and R. Kohli, "Information Technology Payoff in the Healthcare Industry: A Longitudinal Study," Journal of Management Information Systems, 16, 4 (2000b), 41-67. Devaraj, S. and R. Kohli, "Performance impacts of information technology: Is actual usage the missing link?," Management Science, 49, 3 (2003), 273-289. Dickinson, J. C., "From process to policy: a generic prescription for test over-utilization in the emergency department," Fam Pract Res J, 7, 1 (1987), 12-21. Eden, C., "On Evaluating the Performance of Wide-Band GDSSs," European Journal of Operational Research, 81, 2 (1995), 302-311. Eierman, M. A., F. Niederman and C. Adams, "DSS Theory - a Model of Constructs and Relationships," Decision Support Systems, 14, 1 (1995), 1-26. Forgionne, Guisseppi A. and Rajiv Kohli, "Management Support Systems Effectiveness: Further Empirical Evidence," Journal of Association for Information Systems, 1, 3 (2000), 1-39. Forgionne, Guisseppi and Rajiv Kohli, "HMSS: A Management Support System for Concurrent Hospital Decision-Making," Decision Support Systems, 16, 3 (1996), 209-229. Francalanci, C. and H. Galal, "Information technology and worker composition: Determinants of productivity in the life insurance industry," MIS Quarterly, 22, 2 (1998), 227-241. Gell, G., P. Schmucker, M. Pedevilla, H. Leitner, J. Naumann, H. Fuchs, H. Pitz and W. Kole, "SAP and partners: IS-H (TM) and IS-H*MED (TM)," Methods of Information in Medicine, 42, 1 (2003), 16-24. Hackathorn, R.D. and P. G. W. Keen, "Organization Strategies for Personal Computing in Decision Support Systems," MIS Quarterly, 5, 3 (1981), 21-27. 31 Hay, J. W., "Hospital cost drivers: An evaluation of 1998-2001 state-level data," American Journal of Managed Care, 9, (2003), SP13-SP24. Hitt, L. M. and E. Brynjolfsson, "Productivity, business profitability, and consumer surplus: Three different measures of information technology value," MIS Quarterly, 20, 2 (1996), 121142. Jackson, T., "Using computerised patient-level costing data for setting DRG weights: the Victorian (Australia) cost weight studies," Health Policy, 56, 2 (2001), 149-163. Joiner, G. A., D. Salisbury and G. E. Bollin, "Utilizing quality assurance as a tool for reducing the risk of nosocomial ventilator-associated pneumonia," Am J Med Qual, 11, 2 (1996), 100-3. Keen, P.G.W., "Value Analysis: Justifying Decision Support Systems," MIS Quarterly, 5, 1 (1981), 57-73. Kim, H. W., "Business process versus coordination process in organizational change," International Journal of Flexible Manufacturing Systems, 12, 4 (2000), 275-290. Kohli, R. and S. Devaraj, "Contribution of Decision Support Systems to Organizational Performance: Evidence from a Longitudinal Study," Decision Support Systems, Forthcoming, (2003a), Kohli, R. and S. Devaraj, "Measuring Information Technology Payoff: A Meta-Analysis of Structural Variables in Firm Level Empirical Research," Information Systems Research, 14, 2 (2003b), 127-145. Landon, B. E., J. D. Reschovsky and D. Blumenthal, "Physicians' views of formularies: Implications for Medicare drug benefit design," Health Affairs, 23, 1 (2004), 218-226. LeBlanc, L. A. and K. A. Kozar, "An Empirical-Investigation of the Relationship Between DSS Usage and System Performance - a Case-Study of a Navigation Support System," MIS Quarterly, 14, 3 (1990), 263-277. Lee, B. and A. Barua, "An integrated assessment of productivity and efficiency impacts of information technology investments: Old data, new analysis and evidence," Journal of Productivity Analysis, 12, 1 (1999), 21-43. Lillrank, P., S. Holopainen and T. Paavola, "Analyzing productivity with the enabler-effect map," International Journal of Production Economics, 78, 1 (2002), 69-78. Loveman, Gary W., An Assessment of the Productivity Impact of the Information Technologies, Oxford University Press, New York, 1994. Mahmood, M. and G. J. Mann, "How Information Technology Investments Affect Organizational Productivity and Performance: A Longitudinal Study," (1997), 187-191. 32 Marrin, C. A., L. C. Johnson, V. L. Beggs and P. B. Batalden, "Clinical process cost analysis," Ann Thorac Surg, 64, 3 (1997), 690-4. McLean, E. and G. Riesing, "The MAPP System: A Decision Support System for Financial Planning and Budgeting," Data Base, 8, 3 (1977), 9-14. Menon, N. M. and B. Lee, "Cost control and production performance enhancement by IT investment and regulation changes: evidence from the healthcare industry," Decision Support Systems, 30, 2 (2000), 153-169. Mohr, Lawrence B., Explaining organizational behavior, Jossey-Bass, San Francisco, 1982. Mooney, J., V. Gurbaxani and K. Kraemer, " A Process Oriented Framework for Assessing the Business Value of Information Technology," Database Advances in Information Systems, 27, 2 (1996), 68-8. Mosley, C., "Coordination of care in disease management: Opportunities and financial issues," Seminars in Dialysis, 13, 6 (2000), 346-350. Mukhopadhyay, T., F. J. Lerch and V. Mangal, "Assessing the impact of information technology on labor productivity - A field study," Decision Support Systems, 19, 2 (1997a), 109-122. Mukhopadhyay, T., S. Rajiv and K. Srinivasan, "Information technology impact on process output and quality," Management Science, 43, 12 (1997b), 1645-1659. Nault, B. and I. Benbasat, "An Evaluation of Empirical Research in Managerial Support Systems," Decision Support Systems, 6, (1990), 203-226. Orlikowski, W. J. and S. R. Barley, "Technology and institutions: What can research on information technology and research on organizations learn from each other?," MIS Quarterly, 25, 2 (2001), 145-165. Peffers, K. and B. L. Dos Sontos, "Performance effects of innovative IT applications over time," IEEE Transactions on Engineering Management, 43, 4 (1996), 381-392. Poole, M. S. and A. H. Vandeven, "Using Paradox to Build Management and Organization Theories," Academy of Management Review, 14, 4 (1989), 562-578. Reiner, B. I., E. L. Siegel, J. A. Carrino and M. M. Goldburgh, "SCAR radiologic technologist survey: Analysis of the impact of digital technologies on productivity," Journal of Digital Imaging, 15, 3 (2002), 132-140. Roach, S., "America's Technology Dilemma: A Profile of the Information Economy," Special Economic Study Morgan Stanley, 22. April 1987. 33 Sainfort, F. C., D. H. Gustafson, K. Bosworth and R. P. Hawkins, "Decision Support Systems Effectiveness - Conceptual-Framework and Empirical-Evaluation," Organizational Behavior and Human Decision Processes, 45, 2 (1990), 232-252. Schwarz, G., "Estimating Dimension of a Model," Annals of Statistics, 6, 2 (1978), 461-464. Shapiro, S. S. and M. B. Wilk, "An analysis of variance test for normality (complete samples)," Biometrika, 52, 3 and 4 (1965), 591-611. Sharda, R. M., S.H. Barr and J.C McDonnell, "Decision Support System Effectiveness: A review and empirical test," Management Science, 34, 1 (1988), 139-159. Silagy, C. and T. Lancaster, "The Cochrane Collaboration in Primary Care: an international resource for evidence-based practice of family medicine," Fam Med, 27, 5 (1995), 302-5. Simon, Herbert Alexander, Massimo Egidi and Robin Lapthorn Marris, Economics, bounded rationality and the cognitive revolution, E. Elgar Pub. Co., Brookfield, VT, 1992. Soh, C. and M. Markus, "How IT Creates Business Value: A Process Theory Synthesis," Amsterdam, The Netherlands, (1995), 29-41. Tavana, M., Q. B. Chung and D. T. Kennedy, "Rho: A Decision Support System for Pricing in Law Firms," Information & Management, 33, 3 (1998), 155-165. Thompson, James D., Organizations in action; social science bases of administrative theory, McGraw-Hill, New York,, 1967. Tyran, C. K., A. R. Dennis, D. R. Vogel and J. F. Nunamaker, "The Application of Electronic Meeting Technology to Support Strategic Management," MIS Quarterly, 16, 3 (1992), 313-334. Weill, Peter, "The Relationship Between Investment in Information Technology and Firm Performance: A Study of the Valve Manufacturing Sector," Information Systems Research, 3, 4 (1992), 307-333. Wisniewski, M. F., P. Kieszkowski, B. M. Zagorski, W. E. Trick, M. Sommers and R. A. Weinstein, "Development of a clinical data warehouse for hospital infection control," Journal of the American Medical Informatics Association, 10, 5 (2003), 454-462. Zarling, E. J., F. A. Piontek and R. Kohli, "The utility of hospital administrative data for generating a screening program to predict adverse outcomes," Am J Med Qual, 14, 6 (1999), 242-7. Zhan, C. L. and M. R. Miller, "Excess length of stay, charges, and morality attributable to medical injuries during hospitalization," Jama-Journal of the American Medical Association, 290, 14 (2003), 1868-1874. 34