Risk of Vaccinia Transfer to the Hands of Vaccinated
advertisement

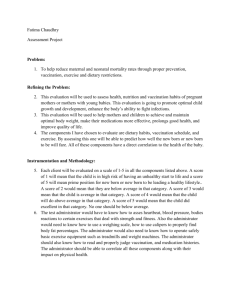
MAJOR ARTICLE Risk of Vaccinia Transfer to the Hands of Vaccinated Persons after Smallpox Immunization Thomas R. Talbot,1 Ellis Ziel,2 Jennifer K. Doersam,2 Bonnie LaFleur,3 Sharon Tollefson,2 and Kathryn M. Edwards2 Departments of 1Medicine, 2Pediatrics, and 3Preventive Medicine, Vanderbilt University School of Medicine, Nashville, Tennessee Transmission of vaccinia virus after smallpox vaccination is a concern. We conducted a prospective examination of the protection afforded by vaccination-site bandages in recently vaccinated individuals. After smallpox vaccination, inoculation sites were covered with 2 occlusive dressings. Site assessment and bandage changes occurred every 3–5 days until the site was healed. At each visit, specimens from the vaccination site, outer dressing surface, and contralateral hand were obtained for vaccinia culture. For 148 vaccinated subjects, vaccinia was detected from vaccination lesions of every subject on several occasions. Only 6 (0.65%) of 918 dressing (95% CI, 0.24%–1.4%) and 2 (0.22%) of 926 hand (95% CI, 0.03%–0.78%) specimens tested positive for vaccinia. The mean number of bandage changes was 9.6 (95% CI, 9.17–10.0). Vaccinia autoinoculation did not occur. The rate of vaccinia recovery outside occlusive bandages covering smallpox vaccination sites was remarkably low, suggesting excellent protection against inadvertent transmission. Routine smallpox vaccination ended in 1972 because of a decreasing incidence of disease and increasing concern about vaccine safety [1]. With the recent bioterrorism attacks involving anthrax and the heightened concern for intentional release of other biologic agents, the United States reinstituted smallpox vaccination in January 2003. In a 3-phase plan for vaccination, military and first-responder teams of selected health care workers were initially vaccinated. The first phase encountered resistance because many health care facilities and providers declined to participate as a result of con- Received 5 September 2003; accepted 16 October 2003; electronically published 28 January 2004. Presented in part: 13th Annual Meeting of the Society of Healthcare Epidemiology of America, Arlington, Virginia, 7 April 2003 (abstract 264). Financial support: National Institute of Allergy and Infectious Diseases Division of Microbiology and Infectious Diseases (study 02-054, contract N01-AI-25462) and Emerging Infections Diseases Cooperative Agreement (salary support for T.R.T.). J.K.D. receives 2% salary support from Aventis Pasteur for work on another study. Reprints or correspondence: Dr. Thomas R. Talbot, A-4103C Medical Center N., 1161-21st Ave. S., Vanderbilt University Medical Center, Nashville, TN 37232 (tom.talbot@vanderbilt.edu). Clinical Infectious Diseases 2004; 38:536–41 2004 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2004/3804-0011$15.00 536 • CID 2004:38 (15 February) • Talbot et al. cerns of possible transmission of vaccinia virus to atrisk patients [2]. Smallpox vaccination entails the induction of a localized skin infection from live vaccinia virus, a related poxvirus, to confer immunity to smallpox (variola). Spread of vaccinia virus occurs predominantly through contact. Individuals may transmit virus from their vaccination sites, potentially leading to substantial morbidity and even mortality in immunocompromised patients or those with eczema [3]. The risk of nosocomial transmission of vaccinia from a vaccinated health care worker has been thought by some to pose a greater risk than the possibility of smallpox release [4]. Precautions to reduce the potential spread of vaccinia from vaccinated individuals include application of an occlusive bioadhesive dressing over the lesion site and careful attention to dressing care and hand hygiene. The recent civilian and military vaccination campaigns reassuringly illustrated the efficacy of this approach: there were rare cases of secondary vaccinia transmission [5, 6]. In a clinical investigation that complements the practical experience seen in these vaccination campaigns, we conducted a prospective surveillance study by using viral culture data to investigate the recovery of vaccinia from vaccination sites covered by occlusive bandages. PATIENTS, MATERIALS, AND METHODS Study subjects. Subjects for this study were recruited from individuals enrolled at a study site (Vanderbilt University; Nashville, TN) participating in a multicenter, double-blind, randomized clinical trial investigating the safety and efficacy of 3 different dilutions of the Aventis Pasteur smallpox vaccine (APSV), a liquid formulation of calf lymph origin smallpox vaccine derived from the New York Board of Health vaccinia strain and maintained frozen at ⫺20C. In this trial, healthy vaccinia-naive subjects aged 18–32 years were recruited; those who met appropriate screening qualifications and who did not meet any of the exclusion criteria for vaccination (table 1) were enrolled. All vaccinated subjects were eligible for participation in the prospective culture surveillance study, which was conducted under a separate consent process. Both the randomized trial and the surveillance study were approved by the Vanderbilt University Institutional Review Board; all subjects consented to both studies. Human experimentation guidelines of the US Department of Health and Human Services and Vanderbilt University were followed in the conduct of this research. Vaccination methods and follow-up. As a part of the safety and efficacy trial, eligible subjects were randomized to receive 1 of 3 strengths of APSV (undiluted or dilutions of 1:5 or 1: 10). Frozen vaccine was reconstituted with diluent containing glycerin, phenol, and sterile water and was administered in the deltoid area via scarification by 15 punctures with a bifurcated Table 1. needle, as described elsewhere [1]. Vaccination sites were covered with 2 occlusive bandages, an initial waterproof gauzeimpregnated transparent bandage (Opsite Post-Op; Smith & Nephew) and an outer waterproof semipermeable bandage (Tegaderm; 3M HealthCare). Subjects were seen in clinic every 3– 5 days for scheduled dressing changes, assessment of vaccine response, and adverse event evaluation. These dressing changes were performed by the study staff until the vaccination site was well scabbed, which usually occurred several weeks after vaccination. Subjects were taught how to remove old dressings and apply new ones in case an unscheduled dressing change was needed before the next clinic visit. Sterile gloves and clean bandages were provided to each volunteer. Subjects were instructed to place soiled bandages in biohazard bags provided by study staff and to dispose of the bags at the next scheduled clinic visit. Subjects were also repeatedly counseled at each visit to avoid manipulation of the vaccination site and dressing and to use gloves and thoroughly wash hands after any dressing manipulation. There were no restrictions on work activities after vaccination, in accordance with the US Centers for Disease Control and Prevention guidelines [7]. At all follow-up visits, each subject was assessed by history, symptom report, and physical examination for evidence of autoinoculation. Because of study constraints, close contacts of subjects were not actively examined for evidence of secondary transmission. Culture methods. Samples for viral culture were obtained from each subject at each scheduled follow-up visit, beginning with the first visit 3–5 days after vaccination. We used cottontipped swabs to obtain specimens from the palmar surface of the index finger on the hand contralateral to the dressing site Exclusion criteria for vaccinia vaccination. History of autoimmune disease Use of immunosuppressive medications History of HIV infection History of solid-organ or bone marrow transplantation History of malignancy History of or current illegal injection drug use Eczema (active or quiescent) Current exfoliative skin disorders Prior vaccination with any vaccinia-vectored or other pox-vectored experimental vaccine Presence of medical or psychiatric conditions or occupational responsibilities which precluded subject compliance with the protocol Acute febrile illness (temperature, ⭓38.1C) on the day of vaccination Allergies to components of the vaccine Presence of a typical vaccinia scar or history of smallpox vaccination Pregnancy or lactation for women Household or sexual contacts with any of the following conditions or factors: history of or concurrent eczema, history of exfoliative skin disorders, history of the immunosuppressive conditions noted above, ongoing pregnancy, or children aged !12 months Risk of Vaccinia Transfer • CID 2004:38 (15 February) • 537 (hand sample), from the outer surface of the outer dressing before bandage removal (dressing sample), and from the vaccination site lesion (lesion sample) at each visit. Before the hand and dressing samples were obtained, the swabs were moistened with sterile saline. However, a dry swab was used to obtain the lesion sample to avoid disruption of the healing process. Samples were obtained at each clinic visit until the lesion was well scabbed without drainage and no longer required dressing. Study staff changed gloves between the removal of the old bandage and the placement of the new bandage. Samples of the vaccination lesions were obtained at day 28 after vaccination for all subjects, regardless of the lesion status. In those subjects whose sites had not yet healed, dressing and hand samples were also obtained for culture. By means of methods described elsewhere [8], specimens were directly inoculated into 1 mL of standard Hank viral transport media and frozen at ⫺70C for batch processing. It was expected that vaccinia would be recovered from a majority of the lesion specimens, because these cultures were obtained from direct contact with the vaccinia pustule. All lesion specimens were inoculated undiluted and at dilutions of 1:10, 1:100, and 1:1000 in triplicate directly onto plates coated with BSC-40 cells (African green monkey kidney) and washed with sterile PBS. After incubation, cells were fixed with formalin and stained with crystal violet to visualize the presence of characteristic vaccinia plaques. Plates without plaque formation at 2 days were considered to be negative for vaccinia. Quantitative titers for positive specimens were expressed as the average of the triplicate counts in log10 plaque-forming units (pfu) per milliliter. Specimens with titers that were too high to quantify at initial dilution underwent further dilutions up to 1:100,000. Because vaccinia recovery was expected to be low from the hand and bandage specimens, undiluted specimens were screened for the presence of vaccinia before performing triplicate dilutions. Specifically, 0.2 mL of each hand and dressing specimen was inoculated undiluted into tubes coated with BSC40 cells. The presence of distinctive cytopathic effect (CPE) [9] was assessed every 48–72 h. Tubes without CPE at 10 days were considered to be negative for vaccinia. Positive hand and bandage specimens were then titrated for the lesion specimens, as described above. As the study progressed, it became apparent that all vaccinia-positive hand and bandage specimens that exhibited CPE within 10 days after inoculation also developed viral plaques within 48 h when inoculated on the titration plates. Therefore, to reduce the screening time from 10 to 2 days, midway through the study, undiluted hand and dressing specimens were inoculated directly onto the tissue plates and screened for pfu. Specimens with plaque formation at 48 h were then titrated as described above for the lesion specimens. Clinical data collection. Demographic information (age and sex) was obtained at the start of the study. At each follow538 • CID 2004:38 (15 February) • Talbot et al. up visit, data on the number of dressing changes performed by the subject since the previous clinic visit (unscheduled changes) and on concurrent illnesses were collected. Data were abstracted from charts at study completion for information on adverse local and systemic findings after vaccination, including the development of fever (temperature, ⭓38.4C), local axillary lymphadenopathy, and focal satellite lesions of vaccinia around the initial site. Analysis. Rates of vaccinia retrieval were expressed as the number of positive cultures for each specimen type per total cultures obtained. Clinical characteristics were compared among subjects with ⭓1 positive dressing specimen to those without any positive dressing culture results. Categorical variables were compared by Fisher’s exact test, and continuous variables were compared by Student’s t test for normally distributed data and the Wilcoxon rank sum test for nonparametric data. A similar comparison between those subjects with and without positive hand specimen results was planned as well. RESULTS All 148 volunteers enrolled in the primary clinical trial at Vanderbilt University participated in the surveillance study. The mean age (SD) of the cohort was 23.6 3.65 years; 56% of the subjects were female. The cohort consisted of health care workers, students enrolled in area colleges and universities, and other community members. All subjects completed follow-up. The specific dilution of vaccine received was evenly distributed among the 3 potencies (undiluted vaccine, 51 subjects; 1:5 dilution, 48; 1:10 dilution, 49). Subjects completed an average of 6.9 follow-up visits (95% CI, 6.79–7.10) for a mean duration of follow-up of 27.9 days (95% CI, 27.5–28.2). Bandages were changed an average of 9.6 times (95% CI, 9.17–10.0; mean number of scheduled changes, 6.9 [95% CI, 6.75–7.05]; mean number of unscheduled changes, 2.7 [95% CI, 2.30–3.08]). There was no evidence of autoinoculation of vaccinia in any subject. Table 2. Summary of data for 2843 specimens collected for viral culture and titer results from positive specimens obtained from patients who received smallpox vaccination. No. (%) of a Total no. of specimens Peak titer, Titer range, log10 specimens positive mean log10 Specimen site obtained for vaccinia pfu/mL pfu/mL Lesion 999 5.25 2.7–7.3 Dressing 918 6 (0.65) 1.77 0.5–2.7 Hand 926 2 (0.22) 1.40 1.0–1.8 NOTE. a 773 (77) pfu, Plaque-forming units. For specimens positive for vaccinia. vaccination. Each sample had a titer of 1.0 log10 pfu/mL; the results of the culture of the dressing sample at this visit were negative. Because of the small number of positive hand culture results, we were unable to perform an analysis of risk factors for retrieval of vaccinia from the hands, such as hand hygiene or number of bandage changes. DISCUSSION Figure 1. Course of vaccinia shedding from the vaccination site of a representative subject. Numbers on the curve correspond to specific virus titers. A total of 2843 specimens (999 lesion samples, 918 dressing samples, and 926 hand samples) were obtained (table 2). Vaccinia was isolated from the vaccination lesions of every subject on multiple occasions (mean total number of positive lesion cultures, 5.22; 95% CI, 5.06–5.39). Peak lesion titers occurred an average 12.8 days after vaccination (95% CI, 12.3–13.3 days), with a mean peak lesion titer of 5.25 log10 pfu/mL (95% CI, 5.13–5.38 log10 pfu/mL; range, 2.7–7.3 log10 pfu/mL). A typical time course of vaccinia shedding is shown in figure 1. Only 6 (0.65%) of 918 dressing samples (95% CI, 0.24%– 1.4%) were positive for vaccinia. The range for dressing specimen titers was 0.5–2.7 log10 pfu/mL, with a mean peak titer of 1.77 log10 pfu/mL (95% CI, 0.82–2.71 log10 pfu/mL). The mean time to a positive dressing culture was 10.2 days (95% CI, 6.47–15.2 days), with 5 of the 6 positive specimens obtained 7–10 days after vaccination (figure 2). Although 6 (4.1%) of 148 subjects (95% CI, 1.5%–8.6%) had 1 positive dressing specimen result, vaccinia was not recovered on a second occasion from any subject. There was no significant difference between individuals with and without a positive dressing specimen result with regard to age, sex, dilution of vaccine received, number of dressing changes (scheduled, unscheduled, and total), time to site healing, occurrence of fever or lymphadenopathy, occurrence of satellite lesions, peak lesion culture titer, mean lesion culture titer, total duration of follow-up, or total number of follow-up visits (table 3). Rarely, subjects presented at followup without a dressing covering the site, and a dressing culture could not be obtained. Vaccinia was recovered from only 2 (0.22%) of 926 hand specimens (95% CI, 0.03%–0.78%), each of which had been obtained from a different subject (figure 2). For one subject, vaccinia was recovered from the hand, dressing, and lesion specimens 10 days after vaccination. Virus titers at this time were 4.6 log10 pfu/mL at the vaccination site, 2.7 log10 pfu/mL on the outer dressing, and 1.8 log10 pfu/mL on the hand. The other subject with a positive hand culture result had vaccinia recovered from both the hand and the lesion at 15 days after Our investigation provides contemporary viral culture surveillance confirming that the risk of inadvertent vaccinia transmission from vaccination sites covered by occlusive bandages to areas outside of the bandage is quite low. Although a direct correlation between the recovery of vaccinia on a vaccinated person’s hands and cases of secondary contact spread has not been established, the extremely low rate of vaccinia recovery outside of the occlusive bandage provides great reassurance that contact transmission is unlikely. The inadvertent transmission of vaccinia to unvaccinated individuals (“contact vaccinia”) has been a particular concern for health care workers as a result of potential transmission to immunosuppressed patients [3]. Precautions to prevent spread of vaccinia include the use of occlusive bandages over the site, careful attention to dressing care, and meticulous hand hygiene. The low incidence of contact vaccinia in the recent civilian and military vaccination campaigns in the United States has provided reassurance regarding the very low risk of vaccinia transmission when proper bandaging and hand hygiene practices are used [5, 6]. There have been no reported cases of contact spread to date in the civilian campaign [5]. In the military experience, only 21 cases of contact vaccinia occurred over 306,673 person-months of contact [6]. Our data, which use viral culture information, provide additional support for these findings. Figure 2. Time line of retrieval of dressing (solid bars) and hand (hatched bars) culture specimens positive for vaccinia in relation to the day of smallpox vaccination. One subject had positive results of both a hand and a dressing culture on day 10 after vaccination; the second subject with a positive hand specimen result did not have vaccinia recovered from any dressing specimen. Risk of Vaccinia Transfer • CID 2004:38 (15 February) • 539 Table 3. Comparison between subjects who had vaccinia recovered from dressing specimens with those who had negative dressing specimen results among subjects who received smallpox vaccination. Characteristic Age, mean years SE No. (%) of male subjects Subjects with a positive dressing culture result (n p 6) Subjects with a negative dressing culture result (n p 142) 21.8 0.72 23.7 0.31 3 (50) 62 (43.7) Undiluted 2 (33) 47 (33.1) 1:5 2 (33) 46 (32.4) 1:10 2 (33) 49 (34.5) Dilution of vaccine, no. (%) of patients No. of dressing changes, mean SE Scheduled 6.83 0.40 6.90 0.08 3.5 0.76 2.65 0.20 10.33 0.92 9.56 0.22 Time to lesion healing, mean days SE 24.0 1.95 24.2 0.37 Lesion titer, mean log10 pfu/mL SE 2.46 0.13 2.56 0.05 Peak lesion titer, log10 pfu/mL, mean SE 5.37 0.42 5.25 0.06 Unscheduled Total Development of fever 1 (16.7) 18 (12.7) Development of lymphadenopathy 3 (50) 87 (61.3) Presence of satellite lesions 1 (16.7) 18 (12.7) Total duration of follow-up, mean days SE Total no. of follow-up visits, mean SE NOTE. 27.3 0.33 27.9 0.19 7.0 0.37 6.94 0.08 There were no significant differences between the 2 groups for any noted variable. Before the recent campaign and our investigation, studies conducted on recombinant HIV-vaccinia virus vaccines had evaluated the infectivity of the vaccination lesions and the protection provided by standard dressings. In one trial, the vaccination site was covered by gauze and 2 occlusive bandages, and outer bandage surfaces were negative for vaccinia and no household or sexual contacts developed clinical or serologic evidence of vaccinia exposure [10]. In a similar trial, Graham et al. [8], who used a single occlusive transparent polyurethane dressing over the site, recovered vaccinia from 12 (18.2%) of 66 cultures of samples from the dressing surface. The addition of a second occlusive dressing and a sterile gauze pad reduced the rate of positive dressing cultures to 3% (3 of 103 cultures). Despite the supporting evidence from these studies, there has been continued skepticism about the protection conferred by occlusive bandages and meticulous infection-control practices. In a recent review article citing historical reports, Sepkowitz [4] commented that nosocomial vaccinia required “relatively minor contact with a source case” (p. 443). Many of the highlighted cases, however, resulted from contact with individuals who had disseminated complications from vaccination, such as eczema vaccinatum and generalized vaccinia— situations with a greater degree of viral shedding and, thus, a higher likelihood of secondary transmission, a distinction not 540 • CID 2004:38 (15 February) • Talbot et al. made in the review. Reflecting these concerns, some conclusions reached in this review have subsequently been questioned by Neff et al. [11]. In our study, vaccinia was recovered from the external surface of the outer bandages in 5 of the 6 subjects during days 7–10 after inoculation. This is the usual time when local symptoms, such as pain and pruritus, reach their peak, and inadvertent touching of the site might be expected to occur. Vaccinated individuals should therefore use particular care to avoid manipulation of the inoculation site during the first weeks after vaccination. We did not see a statistically significant association between vaccinia recovery and the number of unscheduled bandage changes performed by the subjects, measures of high viral shedding, such as peak and mean lesion titers, and surrogate markers of a severe host immune response that may serve as a measure of vaccinia burden (e.g., fever and lymphadenopathy). However, the number of subjects with a positive dressing culture was only 6, limiting the statistical power to detect subtle differences between those with and without positive cultures. There are a few limitations to our study. Subjects received a different smallpox vaccine (APSV) from the currently administered lyophilized vaccine (Dryvax; Wyeth Laboratories) used in the military and civilian campaigns. The degree of vaccinia shedding from vaccination pustules induced from these 2 vaccines has not been directly compared; however, both are derived from the same vaccinia strain. In this study, a systematic evaluation for secondary transmission was not performed, thus potentially limiting any conclusions regarding the risk of vaccinia transmission. However, autoinoculation of vaccinia, which occurred more than twice as often as secondary transmission in the recent military campaign (48 cases vs. 21 cases of secondary spread [6]), also serves as a measure of transmission. In our investigation, surveillance for episodes of autoinoculation of vaccinia was performed, and autoinoculation of vaccinia did not occur. This suggests that there is a low risk of transmission from covered vaccination sites, but definitive conclusions on the risk of all types of vaccinia transmission cannot be made. There was also no comparison group to determine the rate of vaccinia transmission to the hands of individuals without bandages covering the vaccination site. Although this would allow direct comparison of the recovery of vaccinia from sites covered by occlusive bandages to the recovery from unbandaged sites, we were unable to perform such an investigation, because current US Centers for Disease Control and Prevention guidelines do not recommend leaving vaccination sites uncovered [7]. The generalizability of our results to a broader population could be questioned, because subjects in our trial were monitored intensively, and meticulous dressing care and hand hygiene were emphasized on many occasions. Present plans for vaccinated civilians involve monitoring and education of vaccinees [12], but not to the extent seen in this trial. Whether such differences lead to higher rates of recovery of vaccinia from site bandages requires additional study. Finally, this investigation only examined 1 type of vaccination site dressing. Other bandages, such as the gauze bandage currently used for vaccinated non–health care workers, may not be as protective as the occlusive bandages used in our study. A trial comparing vaccinia retrieval from sites covered by several bandage types is currently under way at our institution. With hope, this will provide additional contemporary data regarding the protection provided by vaccination-site bandages. The reinstitution of smallpox vaccination has evoked many new questions about an old, nearly forgotten vaccine. Although experience is quite extensive, current vaccinia administration is being introduced into a very different environment, which has led many to question the vaccine’s safety [4]. Although no infection-control measure can be absolutely effective, our study reinforces the recent civilian and military vaccination experi- ence that intensive education and proper infection-control procedures limit the potential for secondary transmission of vaccinia from sites covered with 2 occlusive bandages. This will, we hope, allay many of the concerns regarding the risk of contact vaccinia and allow a wider acceptance of the vaccine. Acknowledgments We thank the members of the Vanderbilt Pediatric Clinical Research Office (particularly Jennifer Hicks, Jennifer Kissner, Diane Anders, Karen Adkins, and Frankie Motley), William Schaffner, Peter F. Wright, the Vanderbilt General Clinical Research Center, Aventis Pasteur, and colleagues at the National Institute of Allergy and Infectious Diseases Division of Microbiology and Infectious Diseases (particularly Stephen Heyse, Mamodikoe Makhene, Walla Dempsey, and Holli Hamilton), for their support of and guidance with this project. References 1. Henderson DA, Inglesby TV, Bartlett JG, et al. Smallpox as a biological weapon. JAMA 1999; 281:2127–37. 2. Bartlett J, Borio L, Radonovich L, et al. Smallpox vaccination in 2003: key information for clinicians. Clin Infect Dis 2003; 36:883–902. 3. Neff JM, Lane JM, Fulginiti VA, Henderson DA. Contact vaccinia— transmission of vaccinia from smallpox vaccination. JAMA 2002; 288: 1901–5. 4. Sepkowitz KA. How contagious is vaccinia? N Engl J Med 2003; 348: 439–46. 5. Centers for Disease Control and Prevention. Update: cardiac and other adverse events following civilian smallpox vaccination—United States, 2003. MMWR Morb Mortal Wkly Rep 2003; 52:639–42. 6. Grabenstein JD, Winkenwerder W Jr. US military smallpox vaccination program experience. JAMA 2003; 289:3278–82. 7. Centers for Disease Control and Prevention. Questions and answers: smallpox vaccination program implementation—vaccination site care and precautions for recipients. 10 January 2003. Available at: http:// www.bt.cdc.gov/agents/smallpox/vaccination/vaccination-program-qa. asp?typepcat&catpSmallpox+Vaccine&subCat1pVaccination+Site+ Care+and+Precautions+for+Recipients. Accessed 22 July 2003. 8. Graham BS, Belshe RB, Clements ML, et al. Vaccination of vaccinianaı̈ve adults with human immunodeficiency virus type 1 gp160 recombinant vaccinia virus in a blinded, controlled, randomized clinical trial. J Infect Dis 1992; 166:244–52. 9. Hsiung GD. Diagnostic virology. New Haven, CT: Yale University Press, 1982. 10. Cooney EL, Collier AC, Greenberg PD, et al. Safety and immunological response to a recombinant vaccinia virus vaccine expressing HIV envelop glycoprotein. Lancet 1991; 337:567–72. 11. Neff JM, Lane JM, Fulginiti VA. Smallpox and smallpox vaccination. N Engl J Med 2003; 348:1920–5. 12. Centers for Disease Control and Prevention. Smallpox pre-vaccination information packet. Available at: http://www.bt.cdc.gov/agent/small pox/vaccination/infopacket.asp. Accessed 26 November 2003. Risk of Vaccinia Transfer • CID 2004:38 (15 February) • 541