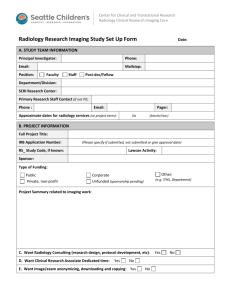
Research Procedure Request form Radiological Services Request
advertisement

Research Procedure Request form Radiological Services Request Requesting Department Information Department Name: Principal PI Name: Additional information: Contact Person (CRC, etc.): Contact Person Phone #: Project Information Project start date: Study Title (per Protocol): Project end date: IRB# Project name (assigned): Study sponsor: DaFIS account number: Study MRN# (Bridge/EMR): Technical Procedures Being Requested (radiological exams, etc. – please describe) 1) 2) 3) 4) 5) Special notes/requests: Imaging location: Main Hospital Imaging time preferences/needs: Modality/cost center: Ambulatory Care Ctr AM PM Weekend CT Diagnostic Nuclear PET Ultrasound Mammo DEXA Who supplies the tracer (PET): UCDHS Who supplies the contrast (CT/MRI): Sponsor Imaging Research Ctr Other Vascular Lab MRI Interventional Radiology Not Applicable Not applicable UCDHS Professional services – do you need the images read by a radiologist? Sponsor Yes No Data/Imaging Transfer Information Image storage requested: Standard (Stentor) Is an image transfer being requested? Yes Disc Videotape Special Formatting No (Transfer requests are completed through the Film Library) For Radiology Internal Use Only Radiology Research Vice Chairman: Radiology Modality Reviewer: Signature Signature Date Date Internally assigned project name: Please submit research protocol, imaging acquisition guidelines, IRB approval and this form to: research-radiology-som@ucdavis.edu