Date Title: Problem
advertisement

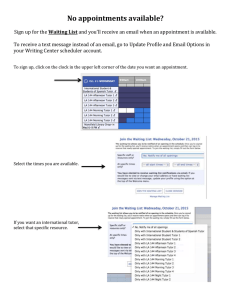
Title: Lengthy Patient Waiting Times for Treatment Appointments Date: December 2014 Problem Waiting times for patients booking treatment appointments is lengthy This results in delay in providing treatment which potentially leads to less favourable outcomes or pain and infection occurring prior to treatment being carried out or completed. Has also led to patient complaints Furthermore, this has led to increased levels of stress for all members of the dental team This is a service wide problem and not specific to Leighton Buzzard Clinic Current Condition Time for treatment appointments currently varies from 1-16 weeks depending on the type of treatment required. This has led to clinicians “fitting in” treatment they consider to be more urgent resulting in: Working extended hours Loss of dedicated time for additional tasks eg admin, FD tutorials and supervision Overbooked clinical sessions Time spent explaining and apologising to patients Additional stress for all members of the dental team Analysis of all appointments booked to return for treatment during November 2014 was carried out. A total of 69 treatment appointments were booked during the month with an average waiting time of 8.45 weeks and 68% of patients waiting more than 6 weeks to return for treatment. Waiting times for treatment appointments 40 30 % 20 10 0 6 or less 4 - 10 11 - 14 Number of weeks 15 or more Only 32% of patients received appointments in 6 weeks or less. Of these 22 patients, 7 were given appointments in emergency/admin or other protected time slots leading to additional stress or workload on staff. Others in this group were allocated cancellation slots or an additional session that was added by one dentist. One patient waited 16 weeks for an appointment. However, this was in part due to a request for a specific time. Target Condition By December 2015, patients at Leighton Buzzard Clinic should be offered treatment appointments within 6 weeks, with their chosen clinician, in order to improve outcomes of care for patients and reduce additional demands and stress on staff. Root Cause Analysis Proposed Changes: As appointment books are currently booked up to 6 months in advance it is understood that any changes will take some time to implement and be evident. Clinic Changes : Appointment books to be amended to have treatment slots and/or dedicated sessions for specific activities eg sedation sessions/GDP referral sessions/IC appointments/treatment appointments etc Consider possibility of dental nurse led clinics to carry out IC appointments as part of DOH pilot Dedicated time to effectively triage referrals to ensure those not meeting current referral criteria are returned to GDP Service Changes: As this is a service wide problem it is felt that changes need to be considered at a “grass roots” level. This has been a discussion at recent staff meetings but no progress has been made at this time. Some changes to consider: Development of more robust referral and discharge criteria Stopping self –referral and consideration to becoming “referral only” service Extension of working hours to potentially include evenings and week-ends Plan Clinic Changes: At next staff clinic meeting to agree: No new patients to be accepted other than GDP referrals meeting current referral criteria Changes in appointment booking to ensure adequate slots available to allow treatments to be allocated appointments within agreed time o Dedicated sessions for examinations, GDP referrals, treatments and sedation to be allocated in individual clinicians appointment books from immediate effect Staff triaging referrals to ensure “protected” admin time to allow more robust triaging of referrals and time to respond to GDP’s having referred inappropriately – admin slots to be placed in appointment book from immediate effect Ensure that all GDP referrals are discharged back to referring GDP at end of treatment Approach senior management to discuss possibility of nurse led-clinic by current senior dental nurse in the free surgery one day/week Service Changes: Approach Operations Director with data collected examining the problem and propose the following: Set up focus group including a mix of staff groups from each clinic to consider the problem and possible solutions – to include the following: Consider whether change to “referral only” service would be appropriate and possibly initiate discussions with commissioners Develop robust referral and discharge criteria for GDP’s Develop a plan for discharge of current patients who no longer require the services of CDS and are appropriate for care to continue within GDS Follow-Up Clinic Level : Ensure dedicated timeslots in appointment book for different clinical sessions, admin and triaging. Re-audit waiting times for patients at 3 monthly intervals to see if improvements are being made with a view to target being met within proposed time frame Service Level: Feedback effect of local changes to Operations Director Continue discussions with Operations Director to initiate and follow progress of service wide changes