Volunteer Study for Sensor Calibration
advertisement

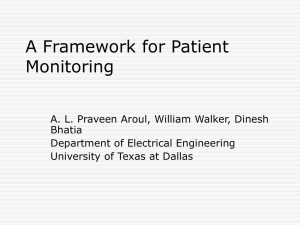
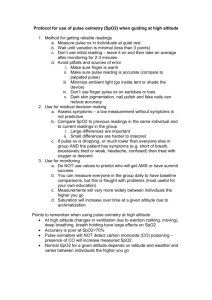
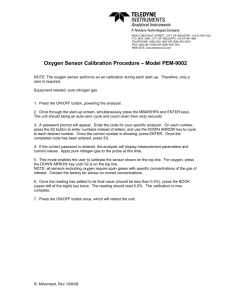
Volunteer Study for Sensor Calibration To calibrate the new SpO2 sensor family it was necessary to adjust the relationship between the ratio measurements and the SpO2 values using data based on real blood samples from volunteers. Fig. 1 shows the measurement environment for the calibration study. The basic instrument is a special HP Component Monitoring System (CMS) with 16 SpO2 channels. Sixteen sensors at different application sites could be used simultaneously. To get SpO2 values over the entire specification range of 70%SpO2100%, the volunteers got air-nitrogen mixtures with lowered oxygen levels—less than 21%. HP Component Monitoring System 16 SpO2 Channels 10% O2 Laptop Computer Regression Analysis Computer Data Files Arterial Blood Sample 21% Nitrogen Oxygen Valve OSM3 Oximeter Fig. 1. Sensor calibration using volunteers and SpO2 data acquisition by a special HP Component Monitoring System (CMS) with a maximum of 16 channels. Different SpO2 values are achieved by supplying different mixtures of oxygen and nitrogen. Arterial blood samples are analyzed by a Radiometer OSM3 oximeter. For each sensor and application site, regression analysis is done, and calibrating tables are derived from the results. Because of his great experience with such studies we used the method developed by Dr. J.W. Severinghaus of the University of California in San Francisco. For each volunteer a maximum of 16 sensors were applied at the fingers, earlobes, and nostrils. A catheter was placed in the left radial artery. Arterial O2 saturation was reduced rapidly by a few breaths of 100% N2. This was followed by a mixture of air and N2 with about 4% CO2 added while the subject voluntarily hyperventilated to speed the attainment of an alveolar gas hypoxic plateau and to provide end tidal samples for regression analysis. FiO2 was adjusted to obtain plateaus for 30 to 60 seconds at different SpO2 levels (Fig. 2). At the end of each plateau a 2-ml arterial blood sample was obtained and analyzed by a Radiometer OSM3 multiwavelength oximeter. The regression analysis yielded three SpO2-versus-ratio calibration curves: one for the HP M1190A adult sensor, a second for the HP M1191A adult sensor, the HP M1192A pediatric sensor, and the HP M1193A neonatal sensor, and a third for the HP M1194A ear sensor. The curves for the HP M1190A and M1191A are different because of their different LED wavelengths, while for the ear sensor the application site is different— the tissue constitution of the earlobe and nostril seems to be optically very different from the other application sites. Each calibration curve is the best least squares fit to the data points of a second-order polynomial. Fig. 3 shows the good correlation with the reference (R2 0.95) in the case of the HP M1191A adult sensor. Fig. 4 shows that the specified SpO2 accuracy is reached within the range of 70%SpO2100%. Fig. 5 shows that the correlation for the HP M1194A ear sensor is not as good as for the HP M1191A. The data point distribution is also wider (Fig. 6). This is caused by a much poorer signal quality at the earlobe than at the finger. In general the perfusion index for the ear is only about a tenth of that for the finger. Therefore, in normal circumstances the preferred application site is the finger. In some cases, such as centralization (i.e., shock patients), the earlobe sometimes gives better results. Subarticle 7a February 1997 Hewlett-Packard Journal 1 100 20 FiO2 SpO2 15 80 10 60 5 40 0 0 t1 1 t2 2 t3 3 t4 Time t (min) 4 5 6 80 HP M1191A SpO 2 Reading (%) Blood Samples Arterial Blood Oxygen Saturation Measured Noninvasively with a Pulse Oximeter SpO 2 (%) Fractional Inspired Oxygen Concentration in Breathing Air FiO2 (%) 100 60 40 20 Fig. 2. Stepwise desaturation by lowering oxygen levels leads to quasistable SpO2 levels. This condition gives blood samples with correct blood gas values. The delay for the SpO2 values compared to the oxygen values comes from the circulation time for the arterial blood from the lungs to the arm. Calibration tables are compiled by comparing the known SpO2 values with the ratio data measured by the CMS. 20 40 60 OSM3 SaO2 Reading (%) 80 Fig. 3. Regression analysis for HP M1191A adult sensor SpO2 measurements after calibration. The measurements are plotted against arterial blood SaO2 measurements from the OSM3 oximeter. The data (206 points) is from 12 volunteers with different oxygen saturation levels. 100 HP M1194A SpO 2 Reading (%) 20 Bias SpO 2 SaO 2 (%) 15 10 5 0 –5 80 60 40 –10 –15 –20 50 60 80 70 OSM3 SaO2 Reading (%) 90 Fig. 4. Bias and standard deviation for the HP M1191A over the specified range of 70%SpO2 100%. Subarticle 7a 100 20 20 40 60 OSM3 SaO2 Reading (%) 80 100 Fig. 5. Regression analysis for HP M1194A ear sensor SpO2 measurements after calibration. The measurements are plotted against arterial blood SaO2 measurements from the OSM3 oximeter for 12 volunteers. February 1997 Hewlett-Packard Journal 2 20 SaO 2 (%) 10 SpO 2 15 0 5 Bias –5 –10 –15 –20 50 60 70 80 OSM3 SaO2 Reading (%) 90 100 Fig. 6. Bias and standard deviation for the HP M1194A. The standard deviation is larger than for the HP M1191A because of the smaller perfusion values in the ear. Subarticle 7a Go to Subarticle 7b Return to Article 7 Go to Next Article Go to Journal Home Page February 1997 Hewlett-Packard Journal 3