What Kind of Drug Use Does School-Based Prevention Prevent?
advertisement

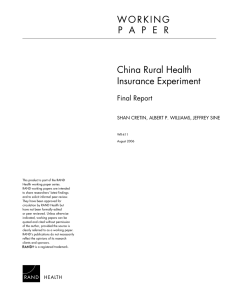
June 2002 What Kind of Drug Use Does School-Based Prevention Prevent? Drug-use prevention programs are now commonplace in the nation’s schools. Their aim is to prevent, or at least delay or diminish, children’s use of a variety of substances, including illicit drugs such as marijuana and cocaine along with legal substances such as alcohol and cigarettes. Most people are instinctively supportive of using such programs to “save our kids” from addiction. But do these programs actually work? Over the last 15 years, compelling evidence from rigorously conducted evaluations has repeatedly shown that the better programs—although by no means all programs—yield tangible effects, often across a variety of substances. But questions remain about the nature of this success. For example, what are the specific benefits of these programs? And which drugs do these programs affect? To frame the issues more provocatively, one might ask whether school-based drug prevention programs are better viewed as a weapon in the war against illegal drugs or as a public health program for decreasing the adverse effects of legal substances. These concerns are central to a study of school-based drug prevention programs recently completed by DPRC researchers. In School-Based Drug Prevention: What Kind of Drug Use Does It Prevent? Jonathan Caulkins, Rosalie Pacula, Susan Paddock, and James Chiesa identify the specific benefits of successful prevention programs—whether in terms of reducing illicit drug use, drinking, or smoking—and discuss whether all these benefits combined exceed the costs of running the prevention programs. Insights into these questions can provide a clearer understanding of the merits of school-based drug prevention programs, and can also shed light on who should be funding drug prevention. The study found that the benefits of model school-based programs do exceed their costs. According to the best estimate, society realizes total quantifiable benefits of $840 from the average student’s participation in drug prevention at this stage of the drug epidemic. This figure is several times the economic cost of one student’s participation in such programs, which averages $150. The researchers derived the amount of the benefit by multiplying together three factors: the amount of substance consumed in an average participant’s lifetime, the percentage reduction in lifetime consumption associated with prevention, and the social cost per unit of substance consumed. Because these factors are themselves the result of many other factors, the value of which can often vary, the researchers also derived a conservative benefit estimate, which was $300. But even with the conservative estimate, the value of prevention is clear relative to the cost of a student’s participation. Both the best and the conservative benefit estimates account for school-based prevention’s effect on use of only four drugs—alcohol, cigarettes, marijuana, and cocaine. These are the only drugs for which data were available to measure prevention’s 4 In This Issue What Kind of Drug Use Does School-Based Prevention Prevent? 1 Director’s Message 2 Leadership 3 New Projects 5 New Publications 6 New People 8 Visiting Scholar: Lisa Kennedy 10 Advisory Board 10 2002 Speaker Series 11 1 D I R E C T O R ’ S M E S S A G E No Progress on Teen Drug Use: What Might Be Done? Remember when teen drug use was news, back in the mid-1990s? The run-up in adolescent drug use in the decade’s early years was big enough news to become an issue in the 1996 presidential election. Since then, the media have moved on to other stories, but the problem remains. The Problem. Use of illicit drugs by adolescents did level off after 1996 (see the figure), and at a percentage that was about half the former peak in 1978. If that sounds comforting, consider that teen drug use over the last five years is almost twice what it had been in the early 1990s. One out of every four 12th-graders and almost as many 10th-graders currently use illicit drugs. Note that is not the proportion responding to the question “Have you ever used . . . ?” It is the proportion just saying “Yes” when asked “Have you used any illicit drug in the past month?” The data on specific drugs provide additional reasons for concern. Marijuana is the illicit drug of choice for teens, so the answers for current marijuana use tend to track those for “any drug.” Marijuana use has almost doubled over the past decade among 12th-graders and more than doubled among 8th- and 10th-graders. The 1975 peak for 12th-grade heroin use has now been surpassed by all three grades. Of course, very few adolescents use heroin, even now. However, the increases potentially represent a big future problem, because of the addictive nature of heroin and the high social and physical costs associated with its use. Stimulant use is another concern. Cocaine is a stimulant. The use of cocaine, both as crack and in other forms, has risen steadily among 8th-, 10th-, and 12th-graders over the last decade. For every thousand adolescents between the Percentage Reporting Use of Any Illicit Drug in the Preceding Month RANDCP201(6/02) 30 25 12th grade 20 10th grade 15 10 8th grade 5 0 1992 2 1993 1994 1995 1996 1997 1998 1999 2000 2001 ages of 12 and 17 who had not previously used cocaine, 14 initiated in 1998 (representing approximately 339,000 new users in this age group); that was the highest such rate in 33 years of data collection. MDMA, also called ecstasy, is a stimulant with hallucinogenic properties. Data on teen use of ecstasy go back only six years, but the percentages reporting use have been steadily increasing for that drug, too. Teen use of the two most common licit drugs, alcohol and tobacco, is also problematic. Some 28 percent of high school students (over all four grades) were current cigarette smokers in 2001. Fortunately, that is down about 8 percentage points from four years earlier. About 22 percent of 8th-graders used alcohol in 2001, as did 39 percent of 10th-graders and 50 percent of 12th-graders. For the 8th-graders, the percentage is down somewhat over the past decade, while for the others, it’s changed little. Addressing the Problem. Over the last decade, then, adolescent use of both licit and illicit substances has been quite high, and for some illicit drugs it has been increasing substantially. So what is being done to combat adolescent drug use? Prevention programs are funded mostly through the Safe and Drug-Free Schools and Communities Act (SDFSCA). Funding under the act was $634 million in 2001—up more than a third in the last five years but no more than it was in 1992. Moreover, a sizable portion of the funds is now directed to violence prevention measures, e.g., metal detectors, that are unrelated to drug prevention. Recent DPRC research suggests that, while the amount of money dedicated to the program as a whole might appear large, the average per-pupil expenditure is less than $8 per year. A more significant and perhaps related problem is that most of the drug prevention money has gone to programs whose efficacy has not been demonstrated. Other research shows that the fraction of school districts relying on evidence-based prevention programs is increasing, though at a slow pace, reaching 27 percent in one recent year. That trend is encouraging, but much more can and needs to be done. A recent tobacco control study in Oregon illustrates this point. Since 1997, a Tobacco Prevention and Education Program has been funded from an excise tax on cigarettes. A portion of the program’s funds have been used to implement guidelines from the Centers for Disease Control and Prevention that are intended to help schools and their communities to reduce tobacco use. In the study, it was found that decreases in 8th-grade smoking rates have been greater in schools with medium or high adherence to the guidelines than in those with low adherence or no funding through the Tobacco Prevention and Education Program. These results suggest not only the value of more prevention but also the value of moreeffective prevention. Prevention is not the only tool for lowering adolescent substance abuse. Many adolescents require drug-abuse treatment. Last year, the U.S. Department of Health and Human Services issued a report to the president on drug-abuse treatment, which estimated that, of more than a million persons aged 12 to 17 who needed treatment for illicit drug use, only 11 percent received it. This was a lower percentage than for everyone over 12 (17 percent), suggesting that the treatment gap is wider for youths than it is for adults. And the need is even greater when youths requiring treatment for nicotine and alcohol dependence are taken into account. But as for prevention, it is not simply that treatment needs to be more available but that better treatment models need to be implemented. Most programs deliver treatment developed for adult drug abusers rather than adolescents. Such interventions are not optimally configured for younger drug users and may not address issues relevant to them. Treatments developed specifically for adolescents need to consider developmental issues, peer influences, parental roles and influences, educational needs, and relatively concrete thinking. Also, drug use by adolescents is more often a symptom of general life problems than the cause, and this, too, should be taken into account in treatment program design. Summary. The available data appear to indicate several emerging issues. Drug use by adolescents has been trending upward over the last decade. Cocaine initiation rates are reaching alarming levels, and use of heroin, methamphetamine, and ecstacy have also increased over the past decade. An aggressive response is merited. Much more attention needs to be paid to the use of evidence-based prevention in our schools. More attention needs to be paid to developing ways to detect drug use and intervene early in educational and health care settings so that action can be taken before the adolescent gets involved with the criminal justice system. Finally, we need to aggressively expand and improve the quality of adolescent treatment options, so that more than the current one in ten can be accommodated by the treatment system, and so that treatment is available to adolescents outside the criminal justice system. ■ Adolescent substance-use data reported here are from Monitoring the Future, the National Household Survey on Drug Abuse, and the Youth Risk Behavior Survey. Leadership After 10 years as director or codirector of the DPRC, Audrey Burnam (shown above with Martin Iguchi) returned to full-time research in July 2001. Audrey had provided strong leadership to the Center as a whole, as well as guidance and inspiration to researchers on an individual basis. In fact, Audrey was largely responsible for the DPRC’s institutional emphasis on mentoring and was at one point named mentor of the year by RAND Health, one of the Center’s two organizational homes. Audrey was particularly interested in performing and fostering research on the re- lations among drug abuse, mental health, and HIV status, and her health services orientation helped balance a DPRC research portfolio that has well represented criminal justice issues. As director and codirector, Audrey was tireless in discharging her administrative responsibilities, in helping shape presentations, and in communicating with board members and other advisors. It is largely as a result of her efforts that the Center grew and thrived as it did. Fortunately, she remains an active resource for the Center and its researchers. ■ 3 1 effectiveness and, thereby, to estimate lifetime reductions in use. However, if one were to assume that prevention programs reduce the use of other illicit drugs, such as heroin or methamphetamines, by the same proportion that they reduce cocaine use, the best estimate of benefits per participant would rise to about $1,000. The results of the study suggest that model drug-use prevention programs can be justified on a benefit-cost basis by the reductions in substance use they produce. Drug prevention seems to be a wise use of public funds, at least for those patient enough to value benefits that accrue some years in the future. In terms of specific benefits, the researchers found that most of the benefits of prevention programs are related to reductions in the use of legal substances (see figure). Close to 40 percent of the social value of drug-use prevention is realized through reductions in cigarette use, and over a quarter of the value is in decreased alcohol use. Most of the remaining third is associated with cocaine, while marijuana accounts for a very small fraction of the total. These findings suggest that it makes more sense to view prevention as a program with major benefits to public health—not merely or principally as a weapon in the war on illicit drugs with only incidental public health benefits. Who then should pay for prevention programs? Considering that at least twothirds of prevention’s benefits fall within the public health arena, one might ask whether prevention should be viewed as a public health intervention rather than a criminal justice intervention and thus be funded from health rather than justice (or education) dollars. DPRC researchers find some merit in this notion. If public health funding streams are available to support drug prevention programs, it would be foolish not to use them, particularly if criminal justice dollars are going to support higher-priority law enforcement interventions. At the same time, concerns over the source of budgetary support should not obscure the fact that the dominant costs of running school-based pre- 4 vention programs are not dollar costs but the diversion of scarce class time from traditional academic subjects into drug prevention. The low dollar cost of such programs is central to their value. Prevention is a wise use of public funds mainly because it is relatively cheap while drug use is so Most of School-Based Prevention’s Benefits costly to society—not Are in the Form of Reductions in the Use of because even the Legal Substances model programs eliminate a large proportion of use. On this point, the researchers caution Cocaine that, while the best Alcohol 20% drug-use prevention 28% Marijuana programs do provide 3% benefits, such efforts Opiates should not be under8% taken with the expectation that they will Other illicit Cigarettes result in striking—or substances 39% even noticeable— 2% declines in the rate of overall drug use. According to DPRC researchers’ best estimates, prevention reduces lifetime consumption of cigarettes by 2.1 percent, of alcohol by 2.2 percent, and of cocaine by 3.0 percent. While these numbers may seem relatively low, even small reductions in use can cause large decreases in social costs. And small reductions may be all that anyone should expect from prevention. Visit Our Web Site and With only thirty hours of prevention proJoin Our E-Mail List! gramming, one would be hard-pressed to overpower the many thousands of hours The home page for the Drug Policy youth spend with other influences such Research Center is located at as peers or television. Prevention is thus http://www.rand.org/multi/dprc a cost-effective tool for improving the public health and making incremental The Web site includes a description of the DPRC, its research agenda, and the progress in efforts to manage a mature latest issue of our newsletter, as well as drug epidemic, such as the cocaine epia subject index and abstracts of all demic in the United States. ■ DPRC publications. Send e-mail to DPRC@rand.org and request to be added to the list for research updates and news on upcoming publications. New Projects Partner-Oriented Drug Treatment and HIV Risk Reduction Methadone maintenance is an effective tool for reducing HIV risk and incidence among injection drug users. All too often, however, individuals in methadone treatment continue to use opiates and other drugs, usually with a close friend or family member who is not currently enrolled in treatment. One response to this problem is to encourage at least one member of the methadone client’s personal drugusing network to also enter treatment, thereby reducing the number of individuals offering drug-use opportunities. Under the sponsorship of the National Institute on Drug Abuse, the DPRC is seeking to determine whether treatment outcomes can be improved and HIV risk behaviors reduced by involving at least two network members in drug treatment simultaneously. In the study, researchers are interviewing 268 new methadone treatment entrants, each of whom is encouraged to recruit a drug-using partner for an interview. Half the drug-using partners are selected at random and offered 13 weeks of free methadone maintenance, while the other half is not being offered subsidized treatment. Self-reports, clinic retention rates, urinalysis records, and other data are being collected from study participants at baseline and four months later to assess treatment outcomes, change in HIV risk behaviors, and change in personal drug-using network characteristics for both the initial methadone clients and their partner referrals. Implementation and Impact of California’s Proposition 36 In November 2000, California voters approved Proposition 36, which mandates probation and community-based drug treatment—instead of prison—for nonviolent drug possession offenses. In light of the initiative’s passage into law, some have raised concerns about the ability of the criminal justice and drug treatment systems to form an effective partnership capable of meeting the challenges posed by Proposition 36. DPRC and Orange County, California, have established a collaboration to evaluate the implementation of Proposition 36 at the county level. With a population of 2.8 million, Orange County is larger than many states and thus serves as an ideal model for systemwide implementation of Proposition 36. Researchers are focusing on several issues, including the response of law enforcement to Proposition 36; the impact of Proposition 36 on prosecutorial discretion and case filing, the courts, probation, and the treatment delivery system; and the collaborative planning efforts of treatment and criminal justice system actors in the county. The analysis, which is funded by the Robert Wood Johnson Foundation, is taking advantage of Orange County’s sophisticated automated data systems and is also using interviews and focus groups. Quality of Care in the Therapeutic Community The effectiveness of substance abuse treatment is well established. Data show that clients who successfully complete treatment generally decrease both their drug use and criminal behavior while increasing their social functioning. What is lacking, however, is an understanding of the treatment process that is responsible for producing client outcomes. Such an understanding is critical to evaluating and improving the quality of care. In research sponsored by the National Institute on Drug Abuse, DPRC is refining and validating a treatment process monitoring tool and examining how treatment programs make use of information from such a tool within a framework of continuous quality improvement. The tool is based on an instrument previously developed by RAND in collaboration with Phoenix House, the largest therapeutic community for substance abuse treatment in the United States. Input from clients in Phoenix House treatment programs throughout the United States will be used, together with state-of-the-art techniques, to refine and validate the tool. Examining the Consequences of Reducing Afghanistan’s Heroin Production While in power, the Taliban effectively enforced an edict against opium production in most of Afghanistan—the source of two-thirds of the global supply in recent years. The fall of that regime led to a resurgence of opium production. The international community now aims to find programs that will again drastically reduce opium production in Afghanistan. Such a cutback, if sustained for even two years, would have profound and varied effects in many parts of Asia and Europe, where the consumption and/or trafficking of heroin are major problems. DPRC is participating in an international collaborative effort aiming to project the effects of an Afghan cutback, help policymakers identify opportunities for effective interventions, and put in place the capacity to monitor the long-term effects of the ban. RAND is developing a simulation model of the global drug trade, while local researchers in affected areas are being asked to provide data about such issues as prices in key markets and average consumption levels by addicts. The Max-Planck-Institut für Informatik in Germany is responsible for the primary data collection. Resulting data will be used to refine the model and generate results, which will be disseminated to decisionmakers in affected countries, while the model itself will be made available to interested governments. This project is sponsored by the Smith Richardson Foundation with additional funding provided to the Max-PlanckInstitut by the Ministry of Justice of the Netherlands. Drug Prosecutions and Drug Policy Reform: The Hidden Connections Americans have become increasingly concerned about the equity and severity of drug sentencing, particularly for offenders whose only crime is drug possession or use. Recently, ballot initiatives have passed in both California (Proposition 36) and Arizona (Proposition 200) that seek to divert low-level drug offenders from incarceration to treatment. In California, opposition to Proposition 36 was 5 led by prosecutors, who argued that few low-level drug offenders actually receive prison sentences. They said that offenders who appeared to be incarcerated on lowlevel drug offenses either had complicated criminal histories that would have excluded them from Proposition 36 eligibility or had pled down from more serious drug charges in exchange for a certain sentence. Prosecutors claimed that under Proposition 36 they would have no choice but to send the latter type of case to trial, as a sentence of community-based treatment is not appropriate for drug traffickers. DPRC, in partnership with researchers at Arizona State University West, is examining the critical issue of prosecution and, in particular, the extent to which those imprisoned on low-level drug charges have engaged in some form of plea bargaining prior to incarceration. The study will identify the types of pleabargaining activities that occurred and examine the extent to which pleabargaining practices are the same across drug types. The project, which is sponsored by the Robert Wood Johnson Foundation, will look at defendants in both California and Arizona. The Effects of Marijuana Depenalization During the mid-1970s, 11 states in the United States passed laws removing incarceration as a penalty for certain marijuana possession offenses. Between 1980 and 1995, state activity in this area was relatively limited; however, in recent years the debate about marijuana reform has been reignited, in part due to significant increases in marijuana-related arrests, heightened attention to the use of marijuana for medicinal purposes, and policy actions in other nations aimed at depenalizing marijuana offenses. Marijuana has been depenalized in several nations, including Italy, Spain, the Netherlands, Portugal, some regions of Australia, and parts of Germany. DPRC is seeking to inform the debate about marijuana depenalization by analyzing the variety of depenalization systems in the United States and abroad, assessing the variations in 6 implementation and enforcement of these systems, and examining the consequences for marijuana use and other outcomes. The study, which is funded by the Robert Wood Johnson Foundation, will provide a broader understanding of the likely consequences of a range of alternative policy options for cannabis law in the United States, at the federal, state, and local levels. ■ New Publications ImpacTeen Illicit Drug Team, Illicit Drug Policies: Selected Laws from the 50 States, Berrien Springs, Mich.: Andrews University, 2002. The federal government has attempted to contain illicit drug use and its associated costs in a wide variety of ways, primarily relying on the use of criminal law to influence both the supply and demand for drugs. At the same time, each of the individual states and the District of Columbia has been experimenting with its own laws that influence the implementation of drug policies within these jurisdictions. Although these interstate variations are often overlooked, state law matters because the majority of drug offenders in the United States are tried in state courts. Illicit Drug Policies provides the first comprehensive reference guide to selected drug laws in all 50 states and the District of Columbia. This report, prepared by the ImpacTeen Illicit Drug Team, is designed to serve as a resource guide for policymakers, legislators, and researchers across the country. The report demonstrates that substantial variation exists in state statutory approaches to drug policy, as is indicated by their scheduling of specific drugs, penalties associated with possession and sale of specific drugs, and medical marijuana allowances. While not inclusive of all drugs or laws, Illicit Drug Policies is an essential first step in this process because it documents where variation does and does not exist in several key areas. It provides data that can be used by policy analysts and researchers to examine the association between specific criminal justice approaches and the negative consequences and outcomes associated with illicit drug use. This document forms the foundation for future research on state-level illicit drug policy to be conducted by the ImpacTeen Illicit Drug Team. ImpacTeen is an interdisciplinary partnership between DPRC researchers and other nationally recognized substance abuse experts with specialties in such areas as economics, etiology, epidemiology, law, political science, public policy, psychology, and sociology. It is part of the Bridging the Gap Initiative, a program supported by the Robert Wood Johnson Foundation and administered by the University of Illinois at Chicago. Ricky N. Bluthenthal, Alex H. Kral, Lauren Gee, Jennifer Lorvick, Lisa Moore, Karen Seal, and Brian R. Edlin, “Trends in HIV Seroprevalence and Risk Among Gay and Bisexual Men Who Inject Drugs in San Francisco, 1988 to 2000,” Journal of Acquired Immune Deficiency Syndromes, Vol. 28, 2001, pp. 264–269. This article identifies trends in HIV infection and risk behaviors among streetrecruited self-identified gay and bisexual male injection drug users (IDUs) in San Francisco from 1988 through 2000. The researchers found that HIV seroprevalance decreased among this population from 1988 to 1996, but increased from 1996 to 2000. Injection and sexrelated HIV risk behaviors declined modestly during this period. The authors conclude that gay/bisexual men who inject drugs continue to be at elevated risk for HIV, suggesting the need for interventions targeted at this population. Jonathan P. Caulkins, “Drug Prices and Emergency Department Mentions for Cocaine and Heroin,” American Journal of Public Health, Vol. 91, September 2001, pp. 1446–1448. Most U.S. drug control spending seeks to restrain supply, which—unless it makes drugs physically scarce—affects use primarily through prices. Thus, a key question concerns the extent to which drug prices affect use. In this study, drug price series were correlated with data on emergency department mentions for the Drug Abuse Warning Network for cocaine and heroin. Using a simple model, the author demonstrates that fluctuations in prices are an important determinant of adverse health outcomes associated with drugs, explaining more than 95 percent of the variation in emergency department mentions. Jonathan P. Caulkins, “Law Enforce- ment’s Role in a Harm Reduction Regime,” Crime and Justice Bulletin, No. 64, NSW Bureau of Crime Statistics and Research, Sydney, January 2002. Harm reduction has typically been seen as the province of drug treatment and public health interventions, while use reduction has been considered the province of law enforcement. This paper shows how law enforcement might also play a valuable role within a harm reduction paradigm. This author outlines five specific roles for law enforcement: partnerships with treatment and other interventions, constraining supply, timefocused intervention early in an epidemic, reducing control costs and associated harms, and exploiting drug markets’ inherent adaptability. Phyllis L. Ellickson, Joan S. Tucker, David J. Klein, and Kimberly McGuigan, “Prospective Risk Factors for Alcohol Misuse in Late Adolescence,” Journal of Studies on Alcohol, Vol. 62, November 2001, pp. 773–782. This study identified Grade-7 and Grade-10 risk factors for alcohol misuse at Grade 12. Alcohol misuse was conceptualized as problem-related drinking (e.g., missing school), high-risk drinking (e.g., drunk driving), and high consumption. The results of the study indicate that predictors of misuse in late adolescence can be identified by Grade 7 and are generally visible and modifiable. While the high social acceptability of alcohol use makes prevention difficult, curbing alcohol misuse may be a more attainable goal. The authors make recommendations for more effective prevention efforts. R. MacCoun, B. Kilmer, and P. Reuter, “Research on Drug-Crime Linkages: The Next Generation,” in H. Brownstein (ed.), Drugs and Crime: A Research Agenda for the 21st Century, Washington, D.C.: U.S. Department of Justice, 2002 (in press). This literature review begins with Paul Goldstein’s three-part taxonomy of the connections between drugs and violence: psychopharmacological, i.e., violence due to the direct acute effects of a psychoactive drug on the user; economic compulsive, i.e., violence committed in order to generate money to purchase expensive drugs; or systemic, i.e., violence associated with the marketing of illicit drugs. The review points to the need for further analyses in several areas, including the role of drug use in criminal victimization; longterm trends in drug use, drug arrests, and drug-related crime; the effects of drug price changes on drug-related criminality; and heterogeneity in drug-crime relationships. Maria Orlando, Phyllis L. Ellickson, and Kimberly Jinnett, “The Temporal Relationship Between Emotional Distress and Cigarette Smoking During Adolescence and Young Adulthood,” Journal of Consulting and Clinical Psychology, Vol. 69, 2001, pp. 959–970. There are three competing hypotheses regarding the relationship between tobacco use and emotional distress among adolescents and young adults: Emotional distress leads to tobacco use, tobacco use leads to emotional distress, or the presence of a third factor leads to both. Using a model with three waves of data from 2,961 adolescents followed into young adulthood, the authors demonstrate that the relationship between tobacco use and emotional distress is a dynamic one in which distress initially leads to use but then becomes exacerbated by it over time. The addition of third factors as predictors of distress and smoking did not alter this pattern of results. Peter Reuter, “The Limits of Supply Side Drug Control,” The Milken Institute Review, Vol. 3, No. 1, 2001, pp. 14–23. U.S. drug policies are heavily supplyside oriented—that is, they aim primarily to restrict the availability of illegal drugs. These enforcement policies have provided mixed results. The author discusses how the nature of the market limits the effectiveness of supply-side policies such as attacking production in source countries, seizing drug shipments, or locking up dealers. He concludes that policymakers will need to focus less on eliminating the drug problem than on finding ways to manage it better. Peter Reuter and Victoria Greenfield, “Measuring Global Drug Markets: How Good Are the Numbers and Why Should We Care About Them?” World Economics, Vol. 2, No. 4, 2001, pp. 159–173. The continuing demand for measures of the size of global drug revenues has produced a supply of numbers that consistently overstate international financial flows. As with many refined agricultural products, most drug revenues go to the distributors rather than to primary producing countries. The authors explore the need for estimates of the global drug markets, address the difficulties of obtaining “good” numbers, and describe opportunities for developing better estimates of flows and revenues. I. Van Beusekom and Martin Y. Iguchi, A Review of Recent Advances in Knowledge About Methadone Maintenance Treatment, 2001, Santa Monica, Calif.: RAND. Since the early 1970s, methadone maintenance treatment has been used in Switzerland as a substitute for heroin addiction. In order to improve the uniformity and quality of methadone maintenance practices, the Swiss Federal Office of Public Health plans to develop clinical guidelines and asked RAND Europe to review the recent literature (1995–2000) on methadone treatment. This review describes the advances in knowledge that have been achieved in understanding the interactions of methadone and other drugs, treatment outcomes associated with methadone maintenance, the use of methadone by special populations (e.g., 7 people with HIV infection or tuberculosis), psychosocial treatment and motivational interventions, addicts’ perceptions of treatment, and the use of other substitution drugs. New People Katherine Watkins, Harold Alan Pin- cus, and Terri L. Tanielan, Evidence-Based Care Models for Recognizing and Treating Alcohol Problems in Primary Care Settings, 2001, RAND MR-1491-SAMHSA. Although primary care physicians (PCPs) are in an ideal position to screen for alcohol problems, begin treatment, and monitor progress, primary care systems are not set up to support PCPs in recognizing and treating such disorders. The authors discuss a chronic disease management model that can be adapted to improve the detection, treatment, and management of alcohol-related problems in primary care settings. The model has four essential components: practice/ delivery system redesign, collaborative management, decision support for providers, and clinical information systems. Suzanne L. Wenzel, M. Audrey Bur- nam, Paul Koegel, Sally C. Morton, Angela Miu, Kimberly J. Jinnett, and J. Greer Sullivan, “Access to Inpatient or Residential Substance Abuse Treatment Among Homeless Adults with Alcohol or Other Drug Use Disorders,” Medical Care, Vol. 39, No. 11, 2001, pp. 1158–1169. This study examines access to in patient or residential treatment among homeless adults with alcohol or drug use disorders. Using data collected from a random sample of 797 homeless adults in Houston, Texas, the researchers found that persons with public health insurance and a history of treatment for substance problems had greater odds of receiving at least one night of treatment, while contact with service sectors was not predictive of treatment access. Schizophrenia and having a partner appeared to hinder access. Greater need for treatment was associated with fewer nights of treatment. The authors conclude that enhancing access to care may require a strengthening of referral relationships across different service sectors. ■ 8 Jeremy Arkes is an associate economist at RAND. His primary interest in drug policy concerns the determinants and consequences of adolescent drug use. Jeremy has recently contributed to several proposals on drug-use research, including one to study how changes in local economies affect adolescent drug use. He has also conducted research in many other areas, including workplace injuries, school accountability, employer training, and military retention and recruiting. Jeremy was previously a research analyst at the Center for Naval Analyses. He has published in such journals as the Review of Income and Wealth and the Economics of Education Review. Jeremy received his Ph.D. in economics from the University of Wisconsin. Deborah Cohen is a senior natural scientist at RAND with expertise in behavioral research and public health program development. She is interested in the role of structural factors on health, including housing, parks, alcohol policies, supervision of youth, and school quality. Deborah was previously chief of the Section of Public Health and Behavioral Medicine in the Department of Public Health and Pre- ventive Medicine at the Louisiana State University Health Sciences Center. There, she led several alcohol-related studies, including two funded by the Robert Wood Johnson Foundation to study the relationship between alcohol policy and alcohol-related mortality. She also led a community intervention, funded by the Center for Substance Abuse Prevention, to increase enforcement of existing alcohol control polices, a project that involved undercover compliance checks and a billboard campaign to reduce alcohol sales to underage youth. Deborah holds an M.D. from the University of Pennsylvania School of Medicine and an M.P.H. from the University of California, Los Angeles, School of Public Health. She was a Fulbright senior scholar in Salvador, Brazil, and completed a postdoctoral fellowship in health behavior at the University of Southern California. Sarah Hunter is an associate behavioral scientist at RAND. Since coming to RAND, Sarah has worked on an evaluation of a mental health intervention tool for substance abuse treatment providers in Los Angeles. She is also collaborating with the Oakland Police Department to conduct a community survey about racial profiling. Sarah’s interests include race and ethnicity, program evaluation, and the social psychological factors that influence health and behavior. She has experience with experimental, quasiexperimental, and qualitative methods. Sarah received a Ph.D. in social psychology from the University of California, Santa Barbara, in 2000. Jerry Jacobson is a doctoral fellow at the RAND Graduate School for Policy Studies (RGS). He specializes in spatial analysis and geographic methods, as well as urban service delivery. Jerry is currently developing statistical methods for evaluating claims of environmental injustice and is also evaluating the impact of California’s Proposition 36 on drug offenders in Orange County. His doctoral research examines the impact of patient and facility location on substance abuse treatment outcomes. Jerry has also collaborated on an analysis of the Indonesia Family Life Survey and in the design, fielding, and analysis of a nationwide survey of emergency response organizations. He is a recipient of the Rotary Ambassadorial Scholarship for 2002–03. Jerry holds an M.Phil. in policy analysis from RGS and a B.S. in industrial engineering and operations research from the University of California, Berkeley. Nelson Lim is an associate social scientist at RAND and research director of the Los Angeles Family and Neighborhood Survey (L.A.FANS). He is the primary investigator on a pending proposal to examine how the likelihood of drug use among Asian American youths is influenced by the effects of acculturation and selfidentity, parental characteristics and familial relationships, and environmental factors. Nelson is also the leader of a proposed study to investigate the impact of neighborhood characteristics on the risktaking behaviors of immigrant children. As research director of L.A.FANS, Nelson has taken the lead on the neighborhood key-informant survey and in constructing a contextual data file to be used with the statistical models that estimate qualities of community and neighborhood on individual life chances. He has extensive training in spatial statistics and in geographic information systems. Nelson holds a Ph.D. in sociology from the University of California, Los Angeles. Jennifer Magnabosco Bower is currently an associate policy researcher in management sciences and health at RAND. She has more than a decade of experience as a researcher, administrator, and clinical practitioner in public and private human service organizations. Jennifer is currently working with other DPRC staff to develop new grant proposals that will continue RAND’s collaborative working relationship with Phoenix House. She is applying her clinical experience with children and families and her research experience in designing and conducting child and adult decisionmaking experiments to explore the behavioral contingencies that are associated with successful adolescent drug interventions and programs. Jennifer is also involved in studies of managed behavioral health care patterns in state Medicaid programs, geographic and racial disparities and children’s mental health needs, and best practices in mental health and public administration. Jennifer is coeditor, with Ed J. Mullen, of the best-selling volume Outcome Measurement in the Human Services: Cross-Cutting Issues and Methods (NASW Press, 1997). She received a Ph.D. in social policy and administration from Columbia University. Steven Martino is an associate behavioral scientist at RAND. His research interests include health cognition and decisionmaking; developmental patterns of substance use and their associated causes and consequences; and adolescent health behavior. Steve has experience with a variety of research approaches, including survey methods, latent variable modeling, growth modeling, regression techniques, cluster analysis, and multilevel modeling. He received a Ph.D. in psychology from the University of Minnesota in 2001. Julie Straus is working with DPRC as a research assistant. Julie has participated on a variety of studies on such topics as partner-oriented drug treatment and HIV risk reduction, the evaluation of chronic illness care, and the impact of changing health care markets on vulnerable populations. She is particularly interested in the impact of drug policy on the homeless. Julie holds B.A. degrees from the University of Pennsylvania in both economics and psychology. ■ 9 Visiting Scholar: Lisa Kennedy Advisory Board Lovida H. Coleman, Jr. (Chair) Partner, Sutherland, Asbill & Brennan The Drug Policy Research Center hosts scholars from other institutions to take advantage of different experiences and outlooks and to provide a means of sharing RAND research with others. The visitor for 2001–02 was Lisa Kennedy, a Ph.D. student at the University of Queensland in Australia, who came to RAND to learn more about cost-effective responses to crime and illicit drug use. Her reflections on her experience at RAND follow: As Thoreau said, “Be not merely good; be good for something.” That’s the difference between the Drug Policy Research Center and institutions with a more theoretical orientation and thus, necessarily, less importance to people in the community. Illicit drug use pervades communities all over the world and while many policy responses are driven by ideology and values, the notion that evidence can, and should, drive policy is gaining currency. The DPRC is at the forefront of providing policy-relevant research. I came to the DPRC to develop my understanding of cost-effective responses to crime and illicit drug use. While I learned about cost-effectiveness research I also learned about the energy that drives the agenda at RAND. It’s hard to explain how the energy at RAND is generated. It must have something to do with recruiting a group of educated, bright people from diverse profes- Stephen M. Duncan Tone N. Grant President, Refco Group, Ltd. Pedro José Greer, Jr. Assistant Dean, Homeless and Poverty Education, University of Miami School of Medicine Calvin Hill Fred C. Iklé Distinguished Scholar, Center for Strategic and International Studies David J. Mactas Norval Morris Julius Kreeger Professor of Law and Criminology School of Law, University of Chicago sional and cultural backgrounds, putting them in a rabbit-warren of a building, and telling them to work really hard. And to collaborate—mostly collaborate. It also helps to have mavens (people who love to teach) such as Martin Iguchi and connectors (people who know everyone), to use terms coined by Malcolm Gladwell. The mavens and connectors at the DPRC have a collective understanding that their research can influence policy, hence their emphasis on getting research into the public domain. For more insight, a social network analysis could help uncover what it is that distinguishes the DPRC—what drives policy-relevant research and collaboration and how the DPRC has harnessed these elusive elements. ■ Amy Pascal Chairman, Columbia Pictures Janet L. Robbie Former Executive Vice President Miami Dolphins and Joe Robbie Stadium Cynthia Telles Director, Spanish Speaking Psychosocial Clinic Department of Psychiatry, University of California, Los Angeles Barbara R. Williams Vice President Emeritus, RAND Hubert Williams President, Police Foundation Judith B. Willis Health Care Consultant Richard B. Wolf James H. Woods Professor of Pharmacology and Psychology Department of Pharmacology, University of Michigan Former Advisory Board Members James E. Burke Chairman, Partnership for a Drug-Free America Norman A. Carlson Senior Lecturer, Department of Sociology University of Minnesota Mathea Falco President, Drug Strategies Daniel P. Garcia Herbert D. Kleber Professor, Department of Psychiatry Columbia University P. Michael Timpane Senior Advisor for Education Policy, RAND The Honorable John P. White Lecturer in Public Policy, John F. Kennedy School of Government; Senior Partner, Global Technologies Partners James Q. Wilson Collins Professor of Management The John E. Anderson Graduate School of Management, University of California, Los Angeles 10 2002 Grant Hill Speaker Series Science and Drug Policy This series provides a forum for decisionmakers and scientists to discuss policies concerning drug supply demand and control. The series is supported by a gift from Houghton Mifflin Company on behalf of Janet and Calvin Hill. February 6 12:00 pm The Iowa Managed Substance Abuse Care Plan (IMSACP): Access, Utilization, and Expenditures for Medicaid Recipients Dennis McCarty, Department of Public Health and Preventive Medicine, Oregon Health Sciences University February 27 3:00 pm Tobacco: Pros, Cons, and Approaches to Harm Reduction Jerome Jaffe, University of Maryland School of Medicine April 8 12:00 pm From Mountains to Molehills: Reducing the Harms Associated with Injection Drug Use in America Stephanie Strathdee, Johns Hopkins School of Public Health May 31 4:00 pm Forces of Habit: Why We Make War on Some Drugs but Not on Others David Courtwright, University of North Florida June 21 12:00 pm The Ethical and Policy Implications of Vaccines Against Cocaine and Nicotine Wayne Hall, Institute for Molecular Bioscience, University of Queensland September 24 12:00 pm Punishment and Prejudice: Judging Drug-Using Pregnant Women Lynn Paltrow, National Advocates for Pregnant Women October 10 12:00 pm Describing Illicit Drug Use in America: Design and Findings of the National Survey on Drug Use and Health Don Goldstone, Office of Applied Studies, SAMHSA November 22 12:00 pm Networks and the Population Dynamics of HIV Martina Morris, Department of Sociology, University Of Washington December 2 12:00 pm Powder Brokers: The Art of Survival in Colombian Cocaine Trafficking Organizations Rick Fuentes, New Jersey State Police The 2002 Speaker Series is held at RAND, 1700 Main Street, Santa Monica, California. For more information, call Nelie Gill at (310) 393-0411, ext. 6330. ■ RAND is a nonprofit institution that helps improve policy and decisionmaking through research and analysis. RAND® is a registered trademark. RAND’s publications do not necessarily reflect the opinions or policies of its research sponsors. The Drug Policy Research Center, established in 1989, is supported by The Ford Foundation, other foundations, government agencies, corporations, and individuals. THE RAND DRUG POLICY RESEARCH CENTER • 1700 MAIN STREET, P.O. BOX 2138, SANTA MONICA, CA 90407-2138 CP-201 (6/02)