METABOLIC PROBLEMS HYPOGLYCEMIA:incidence of symptomatic hypoglycemia is1-3/1000 live
advertisement

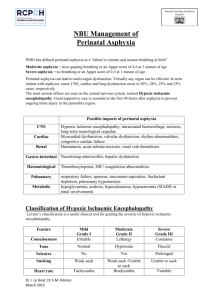
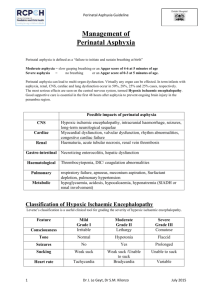
METABOLIC PROBLEMS: HYPOGLYCEMIA:incidence of symptomatic hypoglycemia is1-3/1000 live births,this incidence increases several times in high risk groups. Blood glucose level is maintained if there is: 1-adquate fetal glycogen stores. 2-effective glycogenolysis. 3-effective gluconeogenesis. 4-good nutritional intake. Definition of hypoglycemia:blood glucose level<1.4mmol/L(25mgm/dl) in the first 24 hours of life and 2mmol/L(40mgm/dl) thereafter. Glucose is an essential fuel for the brain, neurons and glial cells are liable to get damaged due to hypoglycemia. CAUSES OF HYPOGLYCEMIA: 1-IGUR, 2-Prematurity. 3-Birth asphyxia. 4-Neonatal sepsis. 5-Hypothermia. 6-Delayed or poor feeding. 7-CHD. 8-Infant of diabetic mother. 9-Rh incompatibility . 10-Beckwith-Wiedman syndrome. 11-Maternal drugs like salbutamol,metochlopramide,valproate,thiazides. 12-Nesidioblastosis. TREATMENT: Asymptomatic hypoglycemia:Treatment is controversial,treatment is by early feeding and if blood sugar drops to <25mgm/dl,start glucose infusion. 10% Dextrose i.v is used to correct hypoglycemia,4mls/kg stat ,then 8mgm/kg/minute.In resistant hypoglycemia due to hyperinsulinemia the following drugs are used: 1-Diasoxide 5-20 mgm/kg/day divided 8 hourly +chlorothiazide to combat water retention,diasoxide inhibit insulin - secretion,increases adrenaline and activates glycogenolysis. 2-Nifedipine(calcium channel blocker)0.25-2.5mgm/kg/day(mode of action is unknown) 3-Glucagon 10Mgm/kg/h by infusion. 4-Hydrocotisone 5mgm/kg/day devided 8 hourly or prednisolone 1-2mgm/kg/day. 5-Surgery. Persistent hypoglycemia:Low blood sugar more than 7 days. Treatment by increasing glucose dose to 16-20mgm/kg/min and investigate for causes. -2- HYPOCALCEMIA Calcium occurs in three forms: 1-Protein bound(30-50%). 2-Bound to citrate or phosphate. 3-Ionised which is the active part. Normal calcium:1.8-2.2mmol/L.The total calcium level does not reflect the actual free calcium level which is the active part. Acidosis increases ionized calcium level and alkalosis decreases it. Types of hypocalcemia: 1-Early hypocalcemia:occurs within 72 hours of life due to poor feeding, it can be seen in prem,RDS,asphyxia,infants of diabetic mothers(because of high calcitonin level which inhibits calcium mobilization from bone ), sepsis,it may be due to transient hypoparathyroidisim,refractory target cells to the effect of parathyroid hormone and lack of transplacentally transmitted hormone.….. 2-Late hypocalcemia:occurs at about 5-7 days, it may continue up to several weeks, it can be regarded as a transitory hypoparathyroidism or due to high phosphorous intake in milk. Hypocalcemia can be caused by alkalosis,repeated blood transfusion Clinical features: It ranges from asymptomatic to jitteriness,tremor of the extremities,tetany,cardiac arrhythmias, convulsions or apnea. TREATMENT: If convulsions are present give calcium gluconate 10%=100-200mg/kg by infusion( 0.20.5 ml/kg). Vit. D 5000 I.U/day orally. In resistant cases of hypocalcemia give I.m Mg sulphate 50% solution, 0.2 ml/kg/dose(100mg/kg),can be repeated 12 hours later. Watch for tissuing of calcium which might cause skin necrosis. . PERINATAL ASPHYXIA Objectives: Define perinatal asphyxia Appreciate the importance of perinatal asphyxia. List infants at risk. List the danger of perinatal asphyxia. Definition of Perinatal Asphyxia: Perinatal asphyxia exist when antepartum,intrapartum,neonatal insult or a combination of these events result in hypoxia and ischemia. Where antenatal services and obstetric care are inadequate and regular monitoring of fetal heart rate is not carried out the incidence of perinatal asphyxia may be expected to be high.. Hypoxic ischemic encephalopathy:Lack of sufficient oxygen to the brain and a diminished amount of blood perfusing the brain,resulting in suppression of electrical activity and cortical depression. Criteria of perinatal asphyxia: The infant is labeled to be asphyxiated if he has the following criteria: 1-Umbilical cord arterial PH<7 2-APGAR Score of 0-3 for more than 5 minutes. 3-Neonatal neurological manifestations(convulsions,coma,hypotonia) 4-Multisystem organ dysfunction. It forms 20% of neonatal deaths and the case fatality rate is around 40%(4-9 million cases/year,more than a million develop cerebral palsy and it’s sequale).Hypoxic ischemic encephalopathy is an evolving process starts from the beginning of the insult and extends into the recovery period when there is neuronal necrosis. Pathophysiology: A combination of hypoxia and ischemia of the brain and other organs. Fetal hypoxia is caused by: 1-Inadequate oxygenation of maternal blood during anesthesia,cyanotic heart disease,respiratory failure. 2-Low maternal BP due to shock,anesthesia,pressure on the inferior vena cava by a gravid uterus. 3-Uterine tetany due to excessive use of oxytocin. 4-Premature separation of the placenta. 5-Compressed umbilical cord. 6-Post maturity and placental infarction. RISK FACTORS FOR HYPOXIC ISCHEMIC BRAIN DAMAGE: 1-Very low APGAR score. 2-Acidotic infants. 3-Those who require cardiopulmonary resuscitation. 50% of infants with perinatal asphyxia have no risk factors so there should be an experienced doctor ready on call at any delivery. Monitoring of heart rate in the second stage of labor is important to detect fetal distress.A bag and mask is very useful in most of the cases ,only 10% need endotracheal intubation. After delivery there are 5 important clinical signs which form the APGAR score(A=appearance i e colour,P=pulse i.e heart rate,G=grimace i.e reponse to suction,A=activity i.e tone,R=respiration. Normal breathing at birth is about 40/minute,heart rate(120-160),you can count for 30 seconds by listening to the heart or palpating the umbilical artery, for color, look at the tongue and extremities .Tone :the infant is usually flexed. APGAR SCORE: Variable Heart rate Respiratory rate 1 minute None <100 >100 Absent Weak or irregular score O 1 2 0 1 Colour Good or cries 2 Central cyanosis 0 Peripheral cyanosis 1 Peripherally pink Muscle tone Limp Some flexion Active,well flexed Response to stimulation None Some response Good response 2 0 1 2 0 1 2 5 minute None <100 >100 Absent Weak or irregular Good or cries Central cyanosis Peripheral cyanosis Peripherally pink Limp Some flexion Active,well flexed None Some response Good response If the APGAR score at one minute is abnormal it should be repeated at 5 minutes.The APGAR at one minute should be 7 or more out of 10. An APGAR at one minute of 4-6 indicates moderate Asphyxia. 0-3 severe Asphyxia. A low 5 minute APGAR score indicates that the infant is not responding well to stimulation and if it continues to be low then the baby is going to have problems of brain damage or death. Causes of low APGAR score: 1-Fetal asphyxia. 2-Maternal GA. 3-Maternal sedation with morphine or pethidine within the last 4 hours. 4-Excessive suctioning of the infant throat. 5-Low birth weight infant. 6-Difficult or traumatic delivery. -4- APGAR results: 1 min >7 No resuscitation. 1 min5-6 Bag and mask. 1 min <4 Intubation. Sequale of Perinatal Asphyxia: 1-Cerebral hypoxia. 2-Convulsions. 3-Periventricular hemorrhage 4-Renal failure. 5-Anoxic cardiomyopathy. -56-DIC. 7-Pulmonary hypertension. 8-NEC. 9-Adrenal hemorrhage. 10-Metabolic disturbances;hypocalcemia,inappropriate ADH secretion,hypoglycemia. TREATMENT: The main point in management is prediction. 1- Treatment of cerebral edema : a-Correct hypoxia and acidosis. b-Control convulsions.it occurs in 20-50% of HIE cases. c-Restrict fluid to 60ml/kg/day. d-Mannitol 5mls/kg/dose over 20 minutes can be repeated four times a day. e-Dexamethasone 1 mg loading dose then 0.3mgm/kg/8 hourly for three days. f-Hyperventilation. g-High dose barbiturate. 2-Maintain tissue perfusion, blood may be given. This is the main step to keep normal (Cerebral perfusion pressure) to prevent neuronal damage which is more important than oedema. 3 -Maintain renal function by ensuring good urine output,furosemide and dopamine may be used. 4- Stop oral feeding for 4-7 days. 5-Treat secondary infection. 6-Thermal regulation. 7-Physiotherapy. 8-Drugs which inhibit oxygen free radicals function or destroy them are useful as a treatment, like dismutase and catalase which are enzymes,allopurinol works on protaglandins,calcium channel blockers like flunarizine blocks the influx of ca into the cell which in high concentration is toxic. 9-Hypothermia. 10-Glutamate is a powerful neurotoxin,Magnesium blocks glutamate receptors. 11-Selective head hypothermia is under investigation.